


Abstract
In metastatic breast cancer, the estrogen receptor (ER) is a well-known prognostic factor predictive of response to hormonal treatment in most, but not all, patients. Recently, a receptor-specific radioligand for in vivo imaging of the ER in breast cancer patients was developed: 123I-labeled cis-11β-methoxy-17α-iodovinyl-estradiol (Z-123I-MIVE). It showed high sensitivity and specificity for the in vivo detection of ER-positive breast cancer. The aim of this study was to determine whether Z-123I-MIVE scintigraphy is able to predict response or resistance to antiestrogen therapy in patients with metastatic ER-positive breast carcinoma. Methods: Twenty-three patients with first metastases of their breast cancer and positive Z-123I-MIVE scintigraphy were included and treated with tamoxifen, 40 mg/d. Scintigraphy was repeated, on average, 4 wk later. The results of these scintigraphies were compared with the clinical outcome. Results: On baseline scintigraphy, 21 of 23 patients had clear uptake and 2 of 23 patients had faint uptake of Z-123I-MIVE. After initiation of antiestrogen treatment, 17 of 21 patients with clear uptake on baseline scintigraphy showed complete blockade of ER activity on the Z-123I-MIVE scintigraphy. Four of 21 patients showed mixed or no ER blockade. All patients with faint baseline uptake or mixed or no ER blockade after tamoxifen showed progressive disease despite antiestrogen treatment. Patients with clear baseline uptake and complete ER blockade after tamoxifen had a significantly longer progression-free interval (mean ± SEM, 14.4 ± 1.6 vs. 1.8 ± 0.8 mo; P < 0.01). Conclusion: Z-123I-MIVE scintigraphy seems to be a useful tool to predict response or resistance to antiestrogen treatment in ER-positive metastatic breast cancer patients and to depict nonresponders before the clinical manifestation of progression.
Breast cancer remains a leading cause of cancer mortality among women in Western Europe and the United States (1). Knowledge of the estrogen receptor (ER) status of breast tumors is of known value to predict patient prognosis and to determine proper patient management (2–4). Until now, the presence of the ER is measured in vitro on a biopsy sample or after resection of the tumor. Of all primary breast carcinomas, about two thirds are ER positive (5). However, in terms of clinical remission, the response to hormonal therapy, which commonly involves treatment with antiestrogens, is variable. Only 50%–60% of these patients with ER-positive tumors show response to hormonal therapy, whereas lack of detectable ERs is usually associated with 5%–10% response (6–8). Furthermore, ER distribution within the primary tumor is often heterogeneous, which might result in a false-negative ER status determined on a random biopsy or tumor cross-section microsample (9). Moreover, it is known that the ER status of metastases, often unreachable for biopsy in clinical practice, may differ from that of the primary tumor (10,11). Finally, the ER status can change during the course of the disease, either spontaneously or induced by therapy (12).
Given the inaccurate predictive value of current ER measurements and the application of Union International Contre le Cancer (UICC) criteria, roughly 40%–50% of patients on first-line hormonal treatment are deprived for at least 2–3 mo of a potentially beneficial alternative treatment option. Accordingly, better methods for predicting clinical response to antiestrogen therapy are needed (13). Several studies have been performed to investigate the possibility of in vivo imaging of the ER with receptor-specific radioligands by PET or SPECT (14–23). The functional status of tumor ERs have been characterized in vivo by PET with FDG and 18F-fluoroestradiol (18F-FES) (23). This study showed that baseline 18F-FES uptake and a flare reaction resulting in increased FDG uptake after tamoxifen are important single predictors of response to tamoxifen treatment. However, this technique requires multiple PET scans where there is limited availability. Recently, we reported on an 123I-labeled ER ligand, cis-11β-methoxy-17α-iodovinyl estradiol (Z-123I-MIVE), which showed high ER binding affinity in both rat and human mammary tumor tissue preparations (24,25). A biodistribution study showed an acceptable effective dose equivalent for the amount of Z-123I-MIVE required for imaging of ERs in primary and metastatic breast carcinoma (26). In a clinical pilot study, focusing on feasibility of Z-123I-MIVE scintigraphy, the preliminary results indicated that Z-123I-MIVE shows good agreement with ER immunohistochemistry (27). A subsequent study confirmed the high sensitivity of Z-123I-MIVE scintigraphy in primary breast carcinoma (28).
This study was undertaken to investigate whether Z-123I-MIVE scintigraphy can predict the response to antiestrogen treatment in metastasized breast cancer and whether it can predict resistance to antiestrogen treatment before clinical progression.
MATERIALS AND METHODS
Patients
In total, 59 patients with metastasized breast cancer have been screened for Z-123I-MIVE uptake. Thirty-five patients (59%) had Z-123I-MIVE-positive lesions. Of this group, 5 patients refused further participation, 7 patients were treated by other means, and 23 patients were included in this trial. Table 1 summarizes the patient characteristics. Twenty-three patients (22 women, 1 man; mean age, 58 y) were included in the study during a 2-y period. All patients had a histologically proven breast cancer and had developed distant metastases, either proven by biopsy (16/23) or strongly suggested by clinical or radiologic (echography, CT) findings (7/23). Upon inclusion, 3 of 23 patients (13%) had a first diagnosis of metastatic breast cancer and 20 of 23 patients (87%) had a diagnosis of relapse or progression of a previously treated breast cancer eligible for antiestrogen treatment. Of the latter group, none of the patients received prior chemotherapy. Ten of 20 patients were treated with surgery and radiotherapy (RT), 4 of 20 patients were treated with ovarian ablation RT, 4 of 20 patients were treated with either surgery or RT, and 2 of 20 patients refused prior therapy. The study was approved by the Medical Ethics Committee of the Academic Medical Center at the University of Amsterdam. Each patient gave written informed consent before participation in the study.
Patient Characteristics and Results
All patients had positive baseline Z-123I-MIVE scintigraphy. Whenever possible, the ER status was confirmed by immunohistochemistry. All patients were treated with tamoxifen, 40 mg/d, and scintigraphy was repeated 4 wk after starting antiestrogen therapy. This timing was chosen since steady-state serum concentrations of tamoxifen are usually achieved within 3–4 wk of daily tamoxifen administration (29). Patients were followed clinically 3, 6, 12, 18, and 24 mo after initiation of therapy or sooner if symptoms occurred. The physician responsible for categorizing disease response or progression was unaware of the scintigraphy findings after therapy. Disease activity was assessed according to UICC criteria (30). Disease progression was assessed by clinical follow-up, echography, CT, and biochemistry including tumor markers. A bone scan was performed on clinical indication. Disease progression was defined as worsened disease on imaging or worsened pain. If a patient returned in emergency before the first 3-mo visit, the patient was reviewed on the next scheduled visit to exclude a flare reaction being mistaken for progression. The endpoint of the study was progression of disease or 24-mo follow-up.
Radiopharmaceutical Synthesis
Z-123I-MIVE was prepared by oxidative radio-iododestannylation of its corresponding stereoisomeric 17α-tri-n-butylstannylvinylestradiol precursor by Amersham Health as described (25). The specific activity of 123I was ≥185 TBq/mmol and the radionuclidic purity was >99.9%. The radiochemical yield was approximately 80%. The specific activity of Z-123I-MIVE amounted to ≥185 TBq/mmol and the radiochemical purity was >98%. The radiolabeled product, which was dissolved in ethanol, was diluted with 0.9% saline to a maximal ethanol concentration of 10%. Before use, thin-layer chromatography was performed to check the absence of free radioiodide. The amount of free iodide was ≤2%. The final product was filtered through a sterile Millex GV 0.22-μm membrane (Millipore).
Imaging Studies
All patients received approximately 300 mg potassium iodide orally—3 doses daily over 2 d—to block thyroid uptake of free radioactive iodide.
Imaging was performed after a single intravenous injection of approximately 185 MBq Z-123I-MIVE in the arm opposite to the known breast lesion to avoid any false-positive uptake in the axillary lymph nodes. Patients were positioned supine and at times of imaging of the thoracic region with the arms alongside of the head. Planar and whole-body acquisitions were performed using a dual-head γ-camera (Siemens Body Scan; Siemens Medical Systems, Inc.), interfaced to a Sun workstation (Hermes; Nuclear Diagnostics). SPECT was performed on a Siemens 3-head SPECT camera. For both, a medium-energy collimator was used, and the energy peak centered at 159 keV with a 15% window.
For all patients, whole-body images were made 4 h after injection. Whole-body acquisition was performed simultaneously in anterior and posterior view (scan speed, 10 cm/min; matrix, 256 × 512 pixels). If necessary, additional spot planar images were acquired for 10 min in a 256 × 256 pixel matrix.
Data Analysis
Scintigraphy.
All images were evaluated independently by 2 experienced nuclear medicine physicians based on the knowledge of the normal distribution of Z-123I-MIVE in healthy volunteers (26). Images were reviewed in cohort for the presence or absence of focally increased uptake at sites of tumors known from clinical findings or other imaging modalities and for possible additional spots of uptake. Posttherapeutic scans were reviewed without knowledge of the clinical outcome. Sites of pathologic uptake were scored semiquantitatively: no uptake (−), faint uptake (±), and clear uptake (+) of tracer. Disagreements were resolved by consensus. Response was defined as complete blockade of uptake on the posttherapeutic scintigram in all clearly positive lesions detected on the baseline scintigraphy.
In Vitro ER Determination.
ER immunohistochemistry was essentially performed on paraffin-embedded material of the metastasis or of the initial primary tumor, if this was available, as described by Sannino and Shousha (31). Material was available in 13 patients (Table 1). Staining intensity was assessed as positive or negative.
Statistical Analysis
Values are reported as mean ± SEM. A log rank test was used to compare differences between activity scores of responders and nonresponders. The agreement between observers was assessed with the κ-test (κ). Kaplan-Meier survival analysis was used to compare the progression-free survival between responders and nonresponders. A possible relation between the progression-free interval and the timing of the repeat study was assessed by rank correlation. All statistical tests were 2-tailed and differences were evaluated at the 5% level of significance.
RESULTS
The results of the study are summarized in Table 1. In 13 of 23 patients (57%), immunohistochemical staining on formalin-fixed paraffin-embedded tissue sections of the tumor could be performed. Twelve of 13 patients (92%) had an ER-positive and 1 of 13 patients (8%) had an ER-negative primary breast carcinoma. In 10 of 23 patients (43%), there was not enough tissue available for immunohistologic staining. All patients had positive Z-123I-MIVE scintigraphy on inclusion. Physiologic distribution of Z-123I-MIVE is seen in the liver, gallbladder, and intestine, reflecting the known hepatobiliary excretion of steroids (26). Visual scoring of pathologic uptake on whole-body scintigraphy resulted in 21 of 23 (91%) patients with 60 clear ER-positive lesions (Fig. 1) and 2 of 23 (9%) patients with 3 faint ER-positive lesions. The second Z-123I-MIVE scintigraphy was performed 4.7 wk (range, 3–8 wk) after starting antiestrogen therapy. Of the initial clear Z-123I-MIVE scintigraphy positive patients, 17 of 21 (81%) showed complete blockade of uptake in all lesions (Fig. 1) and 4 of 21 (19%) showed remaining (3/4) or unchanged (1/4) uptake (Fig. 2). Of the initial faint ER scintigraphy-positive patients, one showed no uptake and the other showed unchanged uptake on the second scintigraphy. For the evaluation of 63 lesions before and after treatment with tamoxifen, there was an excellent agreement between observers (κ = 0.89). There was no relation between the timing of the posttherapeutic scan and progression-free interval.

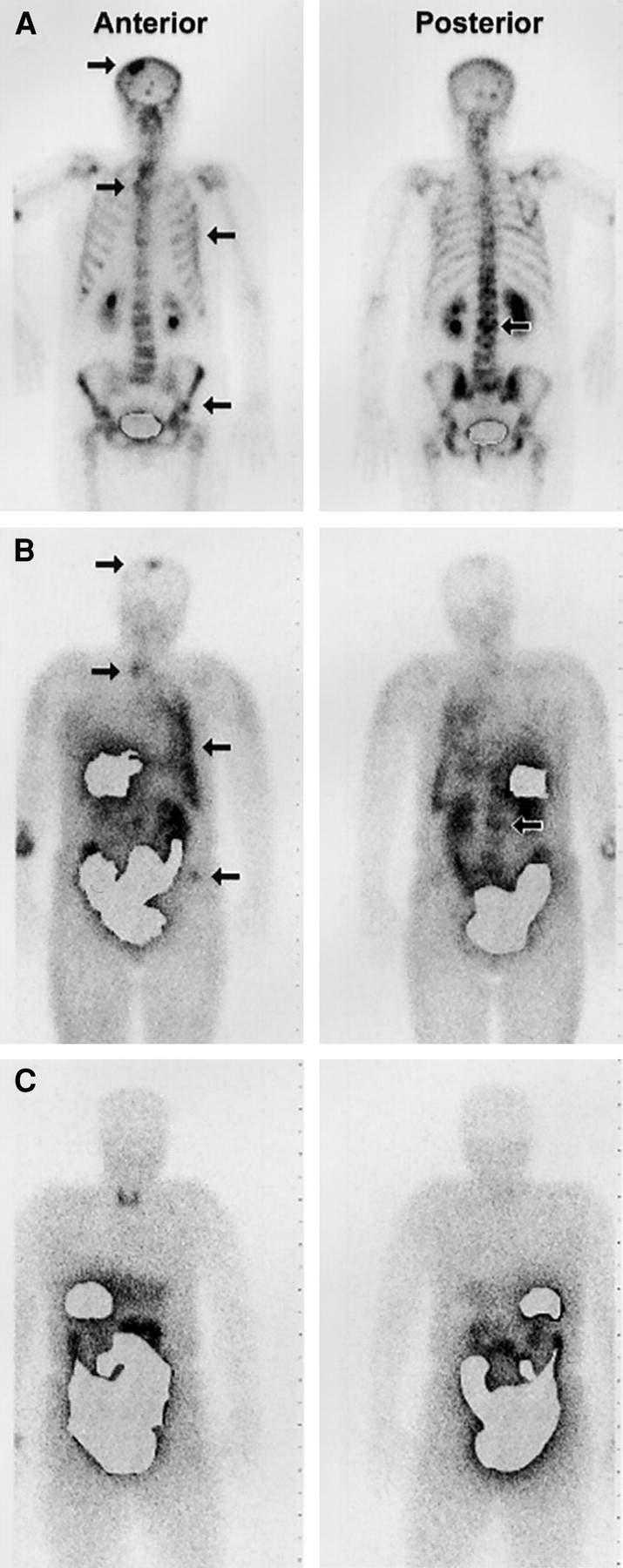
Anterior (left) and posterior (right) whole-body scintigraphy of patient 1. (A) Correlating bone scintigraphy shows multiple sites of pathologic uptake (arrow). (B) Baseline Z-123I-MIVE scintigraphy shows multiple sites of pathologic uptake (arrow) in axial skeleton, skull, and left pleura. (C) Z-123I-MIVE scintigraphy 4 wk after starting tamoxifen shows complete blocking of pathologic uptake in lesions visible on baseline scintigraphy. Thyroid uptake (C) is due to suboptimal blocking of free 123I uptake. Masking of intestinal and hepatic activity was done by computer processing after acquisition.

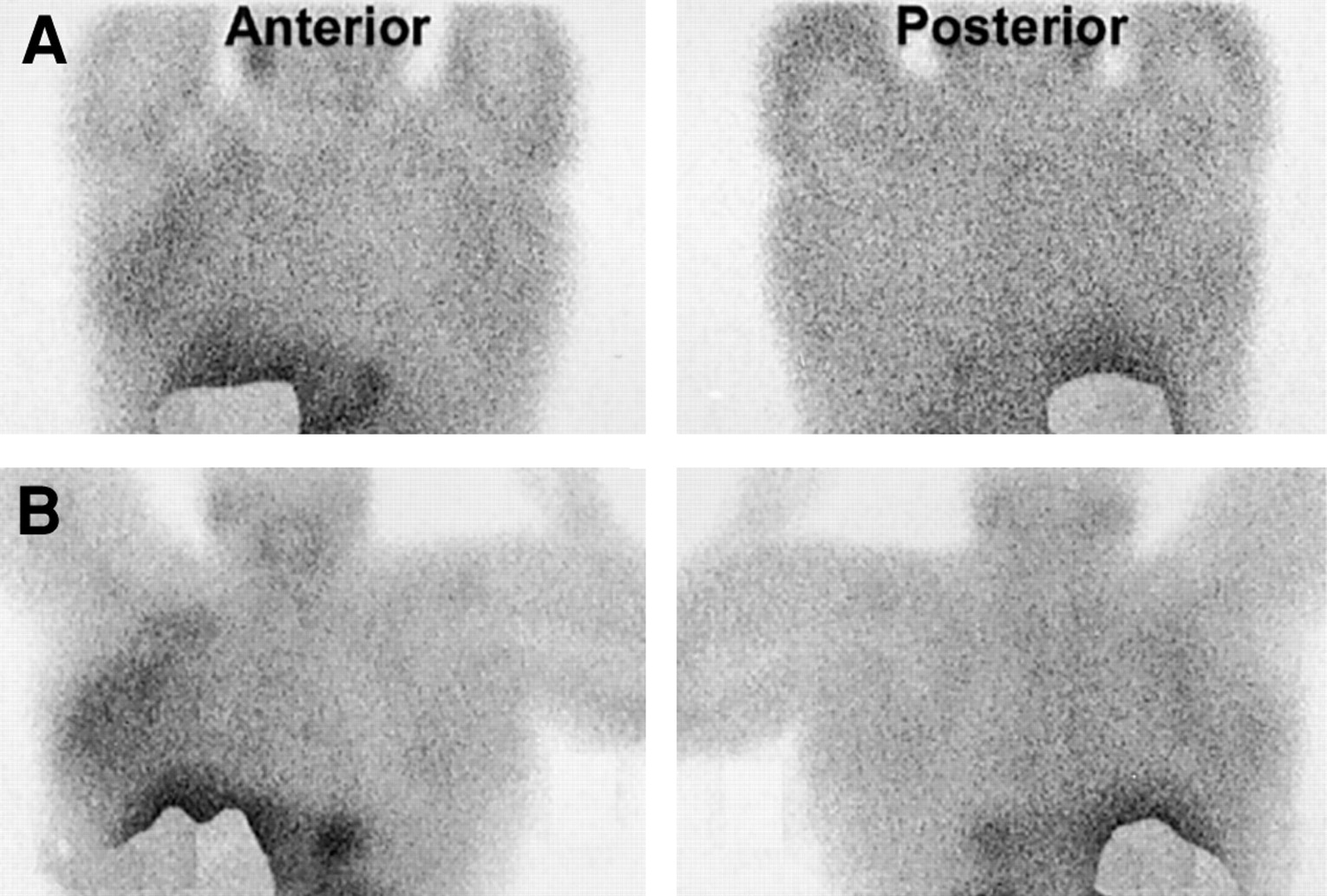
Anterior (left) and posterior (right) planar Z-123I-MIVE scintigraphy of patient 8 before (A) and 3 wk after (B) starting tamoxifen. Baseline Z-123I-MIVE scintigraphy (A) shows diffuse increased uptake in right breast (T4 tumor) with persisting uptake after therapy (B). Masking of intestinal and hepatic activity was done by computer processing after acquisition.
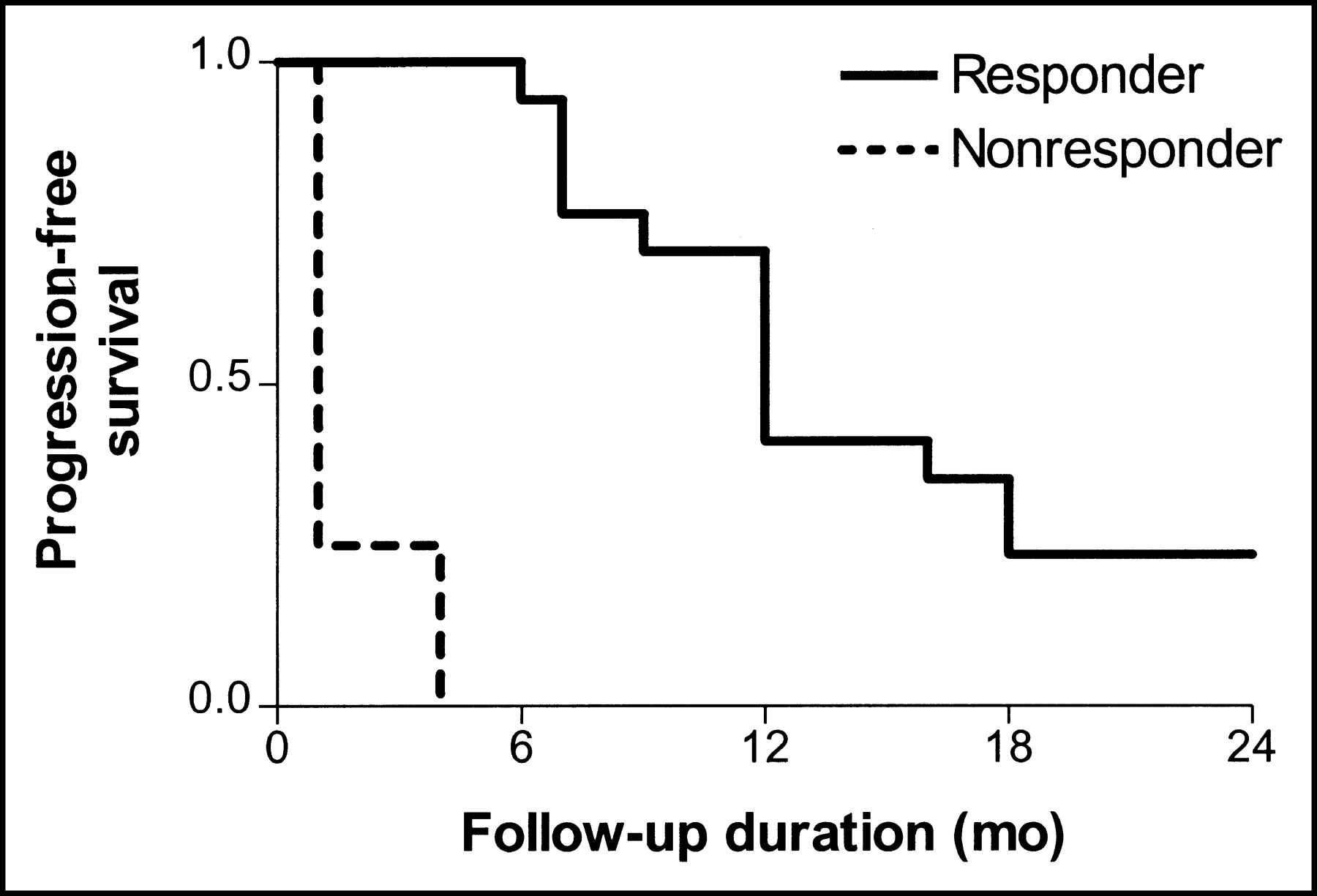
Based on the criteria of total receptor blockade in patients with clear ER-positive lesions on baseline scintigraphy (n = 21), there were 17 responders and 4 nonresponders. Patients with faint uptake on baseline scintigraphy (patients 6 and 11) were excluded from the progression-free survival analysis. Comparing the progression-free interval of responders and nonresponder shows a significant longer (P < 0.01) progression-free interval in the former group, 14.35 ± 1.59 mo and 1.75 ± 0.75 mo (mean ± SEM), respectively (Fig. 3).
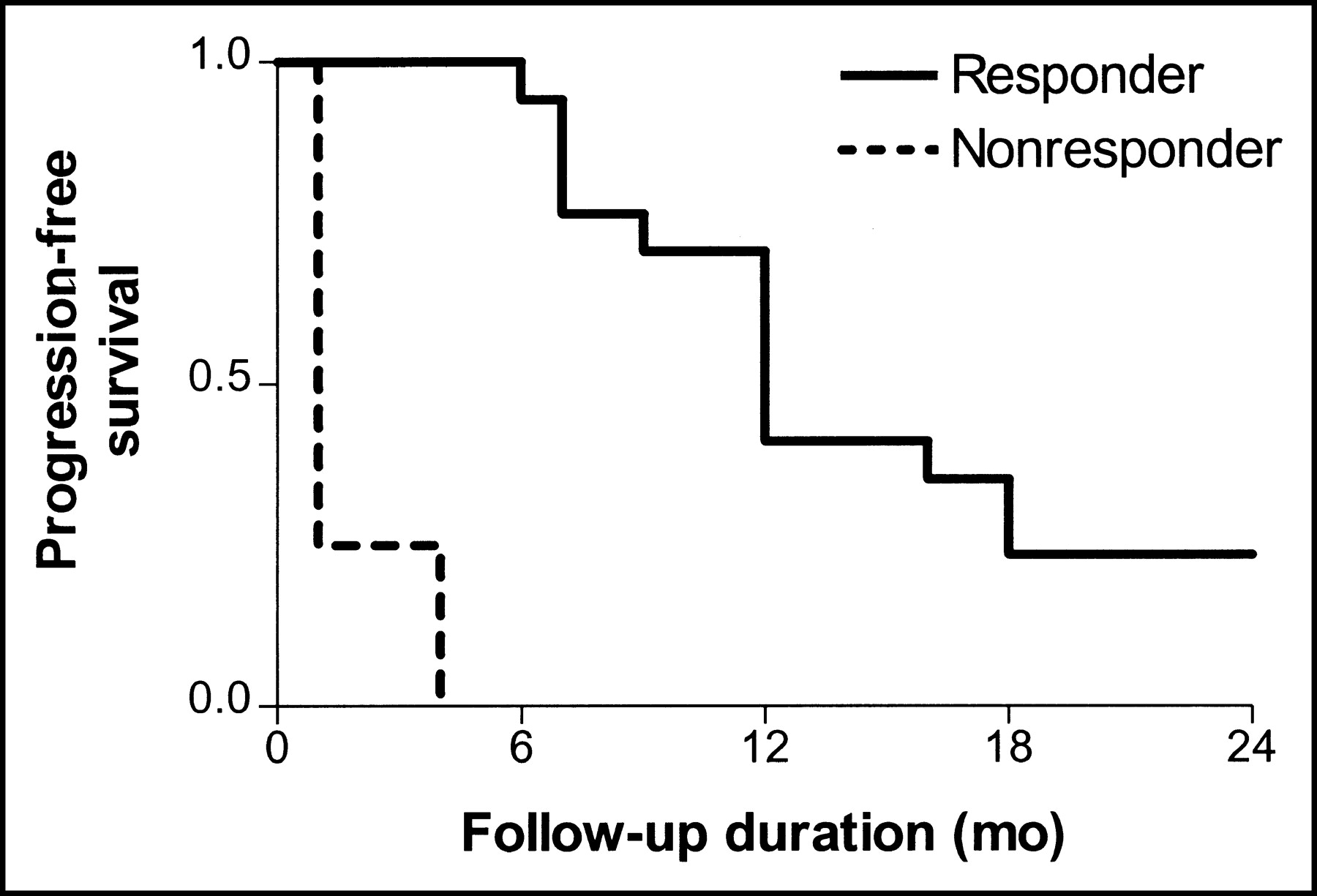
Progression-free survival in ER-positive breast carcinoma in responders and nonresponders after starting tamoxifen, with exclusion of patients with faint uptake on baseline scintigraphy. There is significant difference (P < 0.01) in progression-free survival between responders and nonresponders.
DISCUSSION
Absence or presence of the ER is an important predictor of breast cancer prognosis. When combined with other prognostic information, the ER status is predictive of disease-free survival (32). Therefore, measurement of the ER status is a useful procedure in the management of patients with breast cancer. The ER status is usually determined by biochemical or immunohistochemical assays on biopsy or resection material of the primary tumor or regional lymph node metastases. If patients develop metastases, knowledge of the ER status is also useful to determine whether an endocrine treatment is the treatment of choice. However, even if the original tumor or its regional metastases were ER positive, the possibility remains that endocrine treatment will fail because of discordance of ER contents of the primary and its metastases or a change during the course of the disease (9–12). In general practice, patients are followed after starting the endocrine treatment and nonresponders are identified only after progression becomes clinically apparent, which may take several months or up to >1 y (13).
A clinical pilot study performed with Z-123I-MIVE showed promising results for noninvasive in vivo imaging of the ER status, both in primary and metastatic breast cancer (27). Recently, high sensitivity of Z-123I-MIVE scintigraphy for primary ER-positive breast cancer was confirmed (28). Based on these results, the aim of this study was to determine if Z-123I-MIVE scintigraphy is able to predict response or resistance to antiestrogen therapy.
In our study, it was demonstrated that presence of ERs in primary tumors, local relapse or metastases, clearly visualized on baseline Z-123I-MIVE scintigraphy but blocked (hence, not longer visualized) after antiestrogen treatment is predictive of a longer progression-free interval as compared with incomplete or nonresponders. Furthermore, we show that with Z-123I-MIVE scintigraphy this response can be assessed as early as 3–4 wk after the start of treatment.
In this series, 17 of 23 (74%) of the patients responded well to tamoxifen treatment. This percentage is somewhat higher than the 40%–70% reported in the literature (33). This can be explained by the fact that patients were included with positive Z-123I-MIVE scintigraphy reflecting the actual positive ER status of the tumor and its metastases and not the ER status of a primary tumor assessed in the past. The relative high percentage (43%) of patients in our study population without immunohistochemical ER confirmation reflects the specific patient group with a high number of patients with progressive disease or relapse several years after initial treatment. Frequently, the ER status was not assessed at that time and there was not enough tissue left for processing. Besides this, known problems of sampling error, tumor heterogeneity, and differences in or changing of ER status of primary tumor and metastases in time or after therapy makes such an assessment less reliable (13). The high sensitivity and specificity of Z-123I-MIVE scintigraphy allows assessment of ER status in these patients with the advantage of identification of possible ER-positive metastases (28). Thus, Z-123I-MIVE scintigraphy might be an elegant noninvasive tool to resolve the aforementioned clinical problem.
One could ague that the some of the decrease in apparent Z-123I-MIVE uptake might be simply a reduction in tumor size, resulting in net tumor uptake inferior to the γ-camera detection limits. However, if an initial ER-positive tumor shrunk that much that Z-123I-MIVE visualization is difficult (though positive) due to size-limited detection limits, a patient is correctly determined as a responder. Since scintigraphy and clinical follow-up were not performed within the same time frame (scintigraphy after 4 wk, clinical follow-up after 3 mo or earlier when symptoms warned of progression), exact data are not known for tumor size change at time of the posttherapeutic scintigraphy. However, most lesions were stable or decreased moderately in size after 3 mo in patients responding to therapy.
Scintigraphic detectability of ER-positive tumors will largely depend, among other factors, on tumor size and receptor density (28). The use of SPECT can further improve contrast and lesion localization (28). However, this has practical and logistic implications. First, it is logistically not feasible to perform a multiple (whole body) SPECT acquisition in every patient presenting for Z-123I-MIVE scintigraphy. Second, SPECT can be difficult to read in the abdomen since abundant physiologic bowel activity affects image quality and might result in false-positive results. Improvement in this field could be obtained by using SPECT with functional anatomic mapping, making it easier to delineate bowel through air content (34). Finally, false-negative cases might be avoided in small metastases exhibiting a weak ER positivity, once the localization is known.
It has been demonstrated that there is a good correlation between the immunohistologic staining of ERs and visual scintigraphic Z-123I-MIVE uptake scores (28). Tumor heterogeneity with respect to the ER distribution is a potential cause of discordance between the ER status and therapy response to antiestrogens (13). This might explain why the patients with faint Z-MIVE uptake in our series (patients 6 and 11) had a short progression-free interval, despite blocked uptake after therapy (patient 11).
For progression-free survival analysis, only patients with clear uptake before therapy were included. Inclusion of patients with faint uptake would improve the statistical significance of Z-123I-MIVE uptake before and after tamoxifen as a predictor of outcome. However, these patients had no chance of being responders no matter what was seen on Z-123I-MIVE scintigraphy after tamoxifen. Including patients with faint uptake before therapy was considered because it could be important to know whether a prediction can be made in this category of patients. We were confident to report that blockade of tumor ER by tamoxifen, manifest as a disappearance of clear Z-123I-MIVE uptake, portends a better outcome than when Z-123I-MIVE uptake persists. Limited data suggest that this is not true for patients with only faint uptake before tamoxifen and suggest that these patients should be considered as Z-123I-MIVE negative.
The assessment of therapy response is usually based on the UICC criteria, using morphologic criteria depending on imaging of volumetric changes with a significant reduction of volume needed for response determination requiring generally at least 2- to 3-mo follow-up (30). In case of nonresponse to antiestrogen therapy, which occurs in 30%–60% of these ER-positive breast cancer patients, potentially beneficial alternative treatment options are delayed unnecessarily. In our series, patients were assessed approximately 1 mo after starting antiestrogen therapy. The data illustrate a significant difference between responders and nonresponders, creating the possibility of predicting the response to hormonal treatment in breast cancer on an individual basis at an early stage of therapy. Whether the interval between start of therapy and assessment of therapy response can be shortened is subject of ongoing investigation.
PET using 18F-FES has also been shown to have a high sensitivity and no false-positive cases for the detection of ER-positive primary as well as metastatic human breast cancer (15–17,35). It has also been shown that the responsiveness to antiestrogen therapy in patients with advanced ER-positive breast cancer can be characterized in vivo by FDG PET in combination with 18F-FES PET and that the flare reaction on FDG PET is predictive of response (23). Although 18F-FES PET is a sensitive imaging method for the detection of ER-positive breast cancer, its application in daily clinical situations is confined by its more limited availability and high costs. Therefore, a conventional nuclear medicine imaging procedure could have a place in the work-up of these breast carcinoma patients.
More recently, aromatase inhibitors have been introduced and proved to be superior to tamoxifen as initial therapy and are being extensively tested in the adjuvant setting after, or instead of, tamoxifen (36). Unlike tamoxifen, aromatase inhibitors are not in competition with Z-123I-MIVE for the ER. Therefore, the effective tumor response after therapy could be monitored using Z-123I-MIVE scintigraphy where tumor regression would be detected as a decrease in radiopharmaceutical uptake.
CONCLUSION
Z-123I-MIVE scintigraphy not only is useful in determining the actual ER status in patients with metastasized breast cancer but also seems a useful, noninvasive tool to predict response or resistance to antiestrogen treatment in ER-positive breast cancer patients within a few weeks after the start of treatment.
Footnotes
Received Mar. 25, 2003; revision accepted Sep. 18, 2003.
For correspondence contact: Roelof J. Bennink, MD, Department of Nuclear Medicine, Academic Medical Center, Meibergdreef 9, 1105 AZ Amsterdam, The Netherlands.
E-mail: r.bennink{at}amc.uva.nl
REFERENCES
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- IMAGING IN ENDOCRINOLOGY: 2-[18F]-fluoro-2-deoxy-D-glucose positron emission tomography/computed tomography in differentiated thyroid carcinoma: clinical indications and controversies in diagnosis and follow-up
- Preclinical Development of a Neutral, Estrogen Receptor-Targeted, Tridentate 99mTc(I)-Estradiol-Pyridin-2-yl Hydrazine Derivative for Imaging of Breast and Endometrial Cancers
- PET/CT imaging: detection of choroidal melanoma
- Receptor Imaging in Oncology by Means of Nuclear Medicine: Current Status