


Abstract
The clinical value of a novel technology of combined transmission and emission tomography (TET) was assessed in patients with endocrine tumors. Methods: TET technology, which combines simultaneous acquisition of SPECT and CT images, using the same imaging device, allows correct fusion of images of both modalities. TET was performed on 27 patients with known or suspected endocrine tumors. The radiopharmaceuticals used for the emission part of the study were chosen according to the tumor type: 111In-octreotide for patients with neuroendocrine tumors (n = 10), 99mTc-sestamibi for patients with primary hyperparathyroidism (n = 8), 131I for patients with thyroid cancer (n = 4), and 123I-metaiodobenzylguanidine and 75Se-cholesterol for patients with adrenal masses (n = 3 and n = 2, respectively). The additional information provided by TET compared with scintigraphy was assessed for both image interpretation and clinical utility. Results: TET did not provide any additional data in 16 patients (59%), including 5 patients with normal scintigraphy. In 11 patients (41%) with abnormal SPECT findings, TET improved image interpretation by providing a better anatomic localization of SPECT-detected lesions. It showed unsuspected bone involvement in 4 patients, it identified the organs involved and the relationship of the lesions to neighboring structures in 5 patients, and it differentiated physiologic uptake from tumor uptake in 2 patients. TET provided additional information of clinical value in 9 patients (33%). It assisted in better planning of surgery in 2 patients with neuroendocrine tumors and in 2 patients with ectopic parathyroid adenomas. It changed the treatment approach in 2 patients with neuroendocrine tumors and 1 patient with thyroid carcinoma, and it altered prognosis in 2 patients with thyroid malignancy. Conclusion: TET enhances the already unique role of nuclear medicine procedures in the assessment and management of patients with endocrine neoplasms.
Nuclear medicine plays an important role in the management of patients with endocrine and neuroendocrine tumors. It provides information on functional status, tissue viability, metabolism, and receptor expression. Scintigraphic procedures have a higher sensitivity for the detection of endocrine tumors than anatomic imaging modalities. Nuclear medicine contributes to clinical decision making, such as establishing resectability, planning the surgical approach, and choosing the optimal treatment strategy for advanced disease. For example, recent studies indicate that somatostatin receptor scintigraphy (SRS) is more sensitive than anatomic imaging modalities, including sonography, CT, MRI, and angiography, for identifying tumors such as gastrinoma or carcinoid and their metastases (1–3). A recent study on 160 patients with gastroenteropancreatic tumors reported that SRS led to a change in classification of 24% and a change in the surgical strategy in 25% of the study population (4). However, nuclear medicine procedures are limited by their lack of ability to define the precise anatomic localization of suspected lesions and, therefore, often require correlation with anatomic imaging techniques such as CT or MRI.
Structural and functional imaging modalities have a complementary role in the evaluation of endocrine and neuroendocrine neoplasms. However, their correct alignment can be difficult. Previous attempts to integrate nuclear medicine and CT or MRI studies of the torso have used either external or internal landmarks or a combination of both (5,6). Errors in realignment of functional and anatomic data obtained separately on different devices, on different days, may occur as a result of variations in positioning, in bowel gas or urine content, or may be associated with respiration and motion. Minimizing registration errors is a challenging task and depends on recognition of correct corresponding target landmarks.
A novel imaging device combining a dual-head, variable-angle gamma camera with coincidence acquisition capabilities with a low-dose x-ray tube has been introduced recently (7–9). Transmission and emission tomography (TET) is performed in the same setting, without changing the patient’s position, thereby allowing correct fusion of images of both modalities. The purpose of this study was to assess whether fused images of SPECT and low-dose CT have an impact on image interpretation of both, nuclear medicine and conventional CT studies, and whether TET provides information of added clinical value in patients with endocrine tumors.
MATERIALS AND METHODS
Patient Population
TET was performed on 27 consecutive patients (15 male, 12 female; mean age, 52 y; age range, 5–81 y) with known or suspected endocrine or neuroendocrine tumors. The study was approved by the institutional ethics committee. Table 1 summarizes the clinical data of the study population.
Clinical Data on 27 Patients with Endocrine Neoplasms Evaluated by TET
Selection of the appropriate radiopharmaceutical for the emission (nuclear medicine) part of the procedure was based on the type of tumor. Ten patients with known or suspected neuroendocrine tumors were imaged 4 and 24 h after intravenous injection of 148 MBq (4 mCi) 111In-octreotide (SRS-TET; n = 10), 8 patients with suspected primary hyperparathyroidism were imaged 1 h after intravenous injection of 888 MBq (24 mCi) 99mTc-sestamibi (sestamibi-TET; n = 8), 4 patients with well-differentiated thyroid carcinoma were imaged 48 h after administration of 185 MBq (5 mCi) 131I (131I-TET; n = 4), 3 patients with known or suspected adrenal tumors were imaged 4 h after intravenous injection of 148 MBq (4 mCi) 123I-metaiodobenzylguanidine (MIBG-TET; n = 3), and 2 patients with suspected adrenocortical tumors were imaged 48 h after intravenous injection of 9.25 MBq (0.25 mCi) 75Se-cholesterol (cholesterol-TET; n = 2).
TET Technology
TET was performed using a dual-head, variable-angle, gamma camera equipped with a low-power x-ray system (Millennium VG & Hawkeye; General Electric Medical Systems, Milwaukee, WI). The imaging system is composed of an x-ray tube and a set of detectors fixed on opposite sides of the gamma-camera gantry. This system rotates around the patient along with the γ-detectors. Transmission and emission acquisition can follow an interchangeable sequence. For transmission data, “half-scan” acquisition is performed over 220° in 16 s for each transaxial slice. Multiple slices are obtained by moving the table by a slice step before acquiring the next slice. The full field of view consisting of 40 slices is completed in 10 min. Transmission data of the patient are corrected and reconstructed using filtered backprojection to produce cross-sectional attenuation images in which each pixel represents the attenuation of the imaged tissue. Resolution of radiographic scans is 1 mm, but localization images are produced on a 4-mm pixel size, similar to the nuclear medicine images. The radiographic images are reconstructed into a 256 × 256 matrix. Radiation doses for a transmission scan, calculated on the basis of phantom studies, range from 1.3 mGy at the center to 5 mGy at the surface (7,8).
Planar and SPECT acquisition protocols depend on the administered radiopharmaceutical and were similar to those used routinely in nuclear medicine procedures. For 99mTc- and 123I-labeled radiopharmaceuticals, high-resolution, low-energy collimators were used and 360° SPECT images were acquired in a matrix size of 128 × 128, a zoom of 1.28, a 3° angle step, and a time of 20 s per frame. For 111In- or 75Se-labeled radiopharmaceuticals and 131I, medium-energy collimators were used, with a 6° angle step and a time of 30 s per frame. The collected data were reconstructed using the filtered backprojection technique.
X-ray images were reconstructed using the nuclear medicine workstation (eNTEGRA; General Electric Medical Systems), and transmission data were integrated into the nuclear medicine database. Matching pairs of x-ray and nuclear medicine images were fused using the eNTEGRA software, and images overlying the transmission (CT) and emission (SPECT) data were generated.
Interpretation and Analysis of TET Images
The nuclear medicine and high-resolution conventional CT studies were initially interpreted independently, without prior knowledge of findings on other imaging modalities. Data from both planar and SPECT images were used for scintigraphic assessment. Thereafter, a team of specialists of both modalities interpreted the fused TET images. Scintigraphy was compared with TET-fused images. Transmission data acquired during TET, being inferior in quality to conventional contrast-enhanced CT images, were used for anatomic localization of scintigraphic findings and guided retrospective evaluation of high-resolution CT.
TET was considered to improve image interpretation when it provided a better definition of sites of increased radiopharmaceutical uptake such as determination of the involved organs, the accurate relationship between lesions and neighboring structures, or the exclusion of disease in sites of physiologic radiopharmaceutical uptake, or when it allowed for retrospective detection of lesions missed previously on conventional CT. TET findings were compared with the results of surgery and with clinical and radiologic follow-up. TET was considered to provide additional information of clinical value when the improved accuracy of image interpretation led to a change in prognosis or in treatment approach.
RESULTS
Of the 27 patients who were evaluated in this study, 5 patients had scintigraphic studies with normal findings and 22 patients had abnormal findings. In 16 patients (59%), including the 5 patients with normal scans and 11 patients with abnormal scans, TET did not add any significant information to image interpretation and clinical decision making.
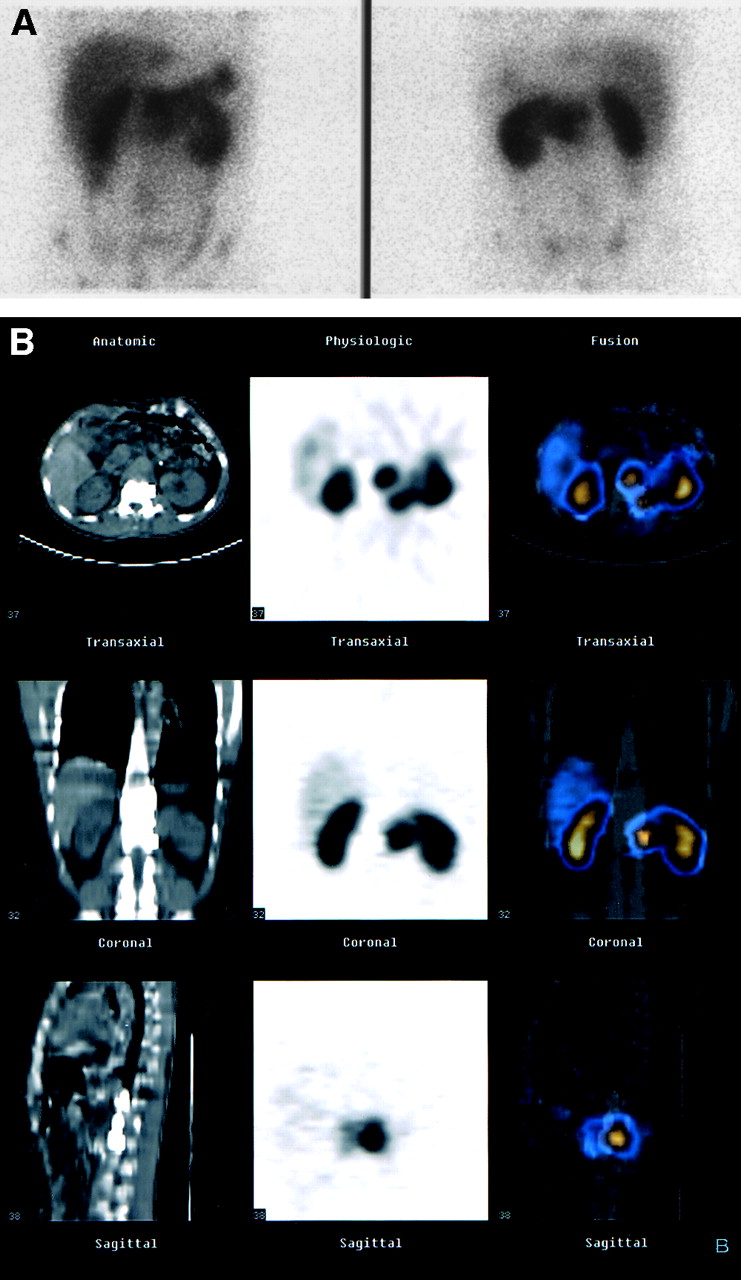
Ten patients with suspected or known neuroendocrine tumors were evaluated by SRS-TET. Eight of these patients had abnormal SPECT findings. In 5 of 8 patients with abnormal SRS, SRS-TET improved lesion localization. In 1 patient with suspected recurrent gastrinoma, a focus of abnormal uptake seen in the abdomen was localized by TET in a normal-sized retroperitoneal lymph node. This patient had a history of adhesions and multiple episodes of small bowel obstruction, and correct localization allowed for minimizing the surgical field, thus avoiding unnecessary adhesiolysis. In a second patient with a recurrent nonsecreting tumor, TET showed that the soft-tissue tumor seen on scintigraphy had penetrated to the adjacent vertebra (Fig. 1). Therefore, the planned curative surgical procedure was canceled. In a third patient with a known pancreatic tumor, SPECT detected a second uptake site localized by TET to the pancreas. This lesion had been missed previously on CT and was detected only retrospectively. The surgical approach was changed to allow removal of both tumor sites. A fourth patient with a carcinoid and extensive liver involvement diagnosed by CT showed multiple abdominal sites of uptake on SPECT. TET excluded extrahepatic disease, and the patient was referred for chemoembolization. In a fifth patient with medullary thyroid carcinoma, TET showed an extension of a known mediastinal tumor to the clavicle, leading to a change in the patient’s prognosis.

SRS-TET in patient with neuroendocrine tumor. (A) Scintigrams show 2 foci of increased 111In-octreotide uptake in midabdomen. (B) TET images (CT, left column; SPECT, center column; fusion, right column) show precise localization of 2 sites of uptake in retroperitoneal, paravertebral region and show involvement of T12 and L1 vertebrae. MRI confirmed findings, and surgery for resection was canceled.
Sestamibi-TET was performed on 8 patients with suspected primary hyperparathyroidism. Five of these patients had an abnormal study. TET added no information in 3 patients with adenoma in the neck that had been detected on scintigraphy. In 2 patients with ectopic thoracic adenoma, TET was the only imaging procedure to provide precise anatomic localization of the lesion for planning of the surgical approach (Fig. 2).

Sestamibi-TET in patient with ectopic parathyroid adenoma. (A) 99mTc-sestamibi scintigrams (early phase, left; late phase, right) show parathyroid adenoma located inferior to right lobe of thyroid, extending into right thorax. (B) TET images (CT, left column; SPECT, center column; fusion, right column) show precise posterior localization of adenoma in right paratracheal region. Surgical approach was planned according to these findings, and adenoma was removed.
131I-TET was performed on 4 patients with thyroid carcinoma. All had abnormal sites of 131I uptake. TET detected the presence of unsuspected bone involvement in 2 patients. One of these lesions was refractory to high-dose 131I treatment. The patient was referred for surgery.
Five patients were evaluated for suspected adrenal tumors, 3 with MIBG-TET and 2 with cholesterol-TET. Four of these patients had abnormal SPECT studies. In 2 patients, TET excluded a tumor as the cause of uptake by localizing the suspected focus in physiologic sites of increased activity, the bowel in 1 patient and the ureter in the second patient. The same final reading could also have been reached by rescheduling the patients for repeated delayed scans. Therefore, these findings improved image interpretation but were not considered to be of clinical value in further analysis of the results.
TET improved image interpretation in 11 of the 27 patients (41%). In 5 patients, it allowed precise localization of disease sites and determination of their relationship with neighboring organs and structures. Anatomic localization provided by TET was confirmed by surgery in all 5 patients. In 4 patients, TET detected previously unsuspected bone involvement. In 2 of these patients, bone involvement was confirmed by MRI after scintigraphy. One patient, in whom MIBG-TET excluded the presence of an adrenal tumor, had a disease-free follow-up at 14 mo. In 1 patient with a carcinoid, clinical and CT follow-up at 8 mo confirmed the absence of extrahepatic involvement. In 1 patient, repeated evaluation of high-resolution, contrast-enhanced CT studies after TET allowed the retrospective detection of a second pancreatic tumor confirmed by surgery. Conventional CT did not detect the scintigraphic findings of bone lesions in 3 patients, 2 ectopic parathyroid adenomas, and 1 metastatic normal-sized retroperitoneal lymph node with gastrinoma. In these 6 patients, TET provided the only imaging evidence of disease before surgery.
TET provided information of additional clinical value in 9 of the 27 patients (33%). It altered the prognosis in 2 patients with thyroid malignancy. It changed the therapeutic approach in 3 patients; on the basis of TET results, 1 patient was referred for surgery, 1 patient was spared unnecessary surgery, and in 1 patient chemoembolization was chosen as the appropriate mode of treatment. TET also assisted in surgery planning in 4 patients, 2 with neuroendocrine tumors and 2 with ectopic parathyroid adenoma (Table 2).
Added Value of TET for Image Interpretation and Clinical Management of 11 Patients with Endocrine Neoplasms
DISCUSSION
Nuclear medicine procedures are sensitive and independent delineators of the functional characteristics of tumors and are used routinely for diagnosis and follow-up of endocrine tumors. However, scintigraphy is limited in its ability to determine the precise anatomic localization of detected foci of increased uptake and often requires correlation with high-resolution imaging modalities for better topographic definition (4,10). Precise tumor localization, correct determination of disease extent, and diagnosis of metastatic spread are important factors affecting outcome in patients with endocrine tumors.
A novel technology of combined SPECT and low-dose CT acquisition using the same imaging device has been introduced recently (7–9). Acquisition of transmission (CT) and emission (SPECT) data is performed during the same session without a change in patient positioning, thereby allowing correct registration of both imaging modalities.
In our study, TET improved image interpretation compared with scintigraphy alone in 11 of the 27 study patients (41%). It provided better definition of the organs involved and determined the precise relationship of the detected lesions with neighboring structures. False-positive results have been described with different radiopharmaceuticals because of their physiologic excretion in the urinary and gastrointestinal tracts (11). TET allowed for exclusion of disease in sites of physiologic radiopharmaceutical uptake, thus improving the specificity of scintigraphy, as was the case in 2 of our patients. Rescheduling for delayed images on different days was unnecessary. After TET, retrospective interpretation of conventional CT detected a pancreatic tumor that was missed on independent reading. TET results indicated the need for a further assessment of unsuspected bone lesions on MRI. In 6 patients, fused TET images provided important topographic data before surgery in the precise definition of lesions detected only on scintigraphy. The low-dose CT used for fused TET imaging is not optimized because of its low resolution and the absence of contrast use. Therefore, it is not meant to replace high-resolution, contrast-enhanced, conventional CT, which maintains its complementary role to nuclear medicine in the evaluation of patients with endocrine tumors.
TET provided additional information of clinical value in 9 of the 27 study patients (33%). Similar results on the clinical contribution of combined imaging have been reported recently (9,12). Using the same imaging device with 18F-fluorodeoxyglucose, Delbeke et al. (9) found that the fused images were clinically relevant in 31% of 35 cancer patients. Charron et al. (12) used a combined dedicated PET–CT device and found fused images to be more precise than PET alone for tumor localization in 24% of cases.
The results of TET imaging in this study allowed a change or optimization of the therapeutic approach and determination of the correct prognosis. Surgery remains the optimal treatment modality for patients with localized neuroendocrine tumors (13). Correct preoperative detection of all tumor sites minimizes the chances for overlooking lesions during surgery. TET assisted in the surgical planning of 2 patients with neuroendocrine tumors. Fused images targeted the surgical field in 1 patient with a recurrent gastrinoma and multiple abdominal adhesions and enabled the planning of the appropriate surgical strategy in a second patient with 2 sites of nonsecreting pancreatic tumor. Accurate localization is particularly important but is difficult to achieve in ectopic parathyroid adenomas. In the absence of correct preoperative localization, the reported rate of surgical failure varies between 33% and 40% and the complication rate is as high as 21% (14,15). In both patients with ectopic parathyroid adenoma evaluated in the current study, TET was the only imaging modality that provided relevant functional and topographic data for surgery planning.
The incidence of multiple organ involvement in patients with neuroendocrine tumors is high. Knowledge of the precise extent of disease plays a major role in determining the appropriate treatment option and choice of treatment procedures such as chemotherapy, cytoreductive surgery, embolization, or liver transplantation (16–20). In 1 patient, TET showed that the metastatic involvement of a carcinoid was limited to the liver, suggesting the use of a local rather than a systemic mode of treatment.
TET identified the presence of unsuspected bone involvement in 4 patients. Diagnosis of bone metastases is of prognostic significance, indicating short survival. In addition, in the presence of bone metastases, patients may be spared unnecessary surgery, insofar as operative removal of a primary tumor is not a curative option (21–26).
CONCLUSION
The results of this study indicate that TET improves image interpretation and provides correct anatomic localization of scintigraphic findings in patients with endocrine neoplasms. TET enhances the already unique role of nuclear medicine procedures in the assessment of these tumors. This accurate, simply achieved method of registration of functional and anatomic data is of importance particularly when lesions are detected only on scintigraphy. It allows a more precise staging and determination of prognosis and leads to better therapeutic management.
Acknowledgments
The authors thank Drs. Rachel Bar-Shalom and Gerald M. Kolodny for their many useful suggestions in reviewing the manuscript and also thank Esther Eshkol for editorial assistance. This research was supported in part by a grant from the L. Rosenblatt Fund of the Technion Foundation for Research in Cancer and by a Research grant from Elgems, Ltd., Haifa, Israel.
Footnotes
Received Nov. 9, 2000; revision accepted Mar. 9, 2001.
For correspondence or reprints contact: Ora Israel, MD, Department of Nuclear Medicine, Rambam Medical Center, Haifa, Israel.
REFERENCES
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- SPECT/CT: Standing on the Shoulders of Giants, It Is Time to Reach for the Sky!
- 131I SPECT/CT in the Follow-up of Differentiated Thyroid Carcinoma: Incremental Value Versus Planar Imaging
- SPECT/CT
- SPECT/Multislice Low-Dose CT: A Clinically Relevant Constituent in the Imaging Algorithm of Nononcologic Patients Referred for Bone Scintigraphy
- SPECT/CT Using 67Ga and 111In-Labeled Leukocyte Scintigraphy for Diagnosis of Infection
- Coincidence Imaging Using 2 Dual-Head {gamma}-Camera Systems, With and Without Attenuation Correction
- In Vivo Prediction of Response to Antiestrogen Treatment in Estrogen Receptor-Positive Breast Cancer
- Clinical Usefulness of Fusion of 131I SPECT and CT Images in Patients with Differentiated Thyroid Carcinoma