


Abstract
Precise localization of the foci of 131I uptake for management of patients with differentiated thyroid carcinoma can be difficult because of a lack of anatomic landmarks. The objective of the present study was to demonstrate the clinical usefulness of 131I SPECT/CT fusion images in patients with differentiated thyroid carcinoma. Methods: CT and SPECT were performed 7 d after administration of a therapeutic dose of 131I to 17 patients with differentiated thyroid carcinoma. External markers were placed at 3 locations on the skin of the patient to adjust the sections of CT and SPECT in the same geometric plane. Fusion images were constructed by combining the digital CT and SPECT images on a computer workstation. The data from both planar and SPECT 131I images and CT images were first separately assessed by 2 nuclear medicine physicians. 131I SPECT/CT fusion images were then interpreted. Fusion images were considered to improve image interpretation in comparison with CT and scintigraphy separately when they provided better localization of sites of increased radiopharmaceutical uptake. Results: Both CT and 131I SPECT showed the pathologic sites in 5 of 17 patients (29%). Fusion images were considered to be of benefit in 15 of 17 patients (88%). In 4 patients, CT showed normal-sized lymph nodes, whereas 131I SPECT showed abnormal findings. In 3 patients with bone metastasis, fusion images confirmed the precision of the localization of abnormal 131I uptake. Five bone metastases and 1 muscle metastasis were occult and were not seen on the CT images. Finally, 131I scintigraphy findings were abnormal for 2 patients for whom the CT findings were initially considered normal. Fusion images confirmed the precision of the localization of physiologic 131I uptake. Conclusion: For registration of anatomic and functional images in fusion imaging, the method using external markers was simple and practical. 131I SPECT/CT fusion images using this technique may improve anatomically limited interpretation of 131I scintigraphy alone in patients with differentiated thyroid carcinoma.
Nuclear medicine imaging provides excellent information on functional biology. However, the anatomic information obtained from this technique is generally quite limited. In contrast, CT and MRI are excellent anatomic imaging modalities. Combination of the functional information from nuclear medicine imaging and the anatomic information from CT and MRI can improve diagnostic capability and facilitate image interpretation (1,2).
131I scanning is indispensable for the management of patients with differentiated thyroid carcinoma (3). However, precise localization of the foci of 131I uptake can be difficult because of a lack of anatomic landmarks. In addition, there are many other potential sites of physiologic uptake, such as the salivary glands, urinary bladder, gastrointestinal tract, and liver (4). Precise tumor localization for correct diagnosis and assessment of disease extent and metastatic spread is important for determining outcome in patients with thyroid carcinoma. SPECT should be performed to improve the sensitivity of 131I imaging and to allow better localization of the tumor site. However, precise localization of tumor foci can still remain difficult despite optimal technical conditions and careful correlation with morphologic imaging. These difficulties may be related to various factors including lack of anatomic landmarks and physiologic distribution of the tracer.
Multimodality image coregistration can be achieved by several techniques using external markers or internal landmarks. Recently, CT combined with SPECT or PET has been developed (5–7). However, because of high cost, these systems are available in few centers and are limited to the combination of the above 3 modalities. The purpose of the present study was to demonstrate the clinical usefulness of 131I SPECT/CT fusion images using external markers in patients with differentiated thyroid carcinoma.
MATERIALS AND METHODS
The study had 2 parts: a preclinical phantom study to validate the image fusion technique using CT and SPECT imaging systems, and a clinical feasibility study with 17 patients to assess the value of CT and 131I SPECT image fusion.
Preclinical Phantom Study
A cylindric phantom was prepared to check the accuracy and reproducibility of the methodology for registering CT and SPECT images. The phantom consisted of 5 ellipsis-shaped sources (5 cm long and 2 cm in maximum diameter) as internal landmarks filled with normal water and a 131I solution with an activity of 25 kBq/mL for the CT and SPECT studies, respectively. The rest of the phantom was filled with normal water and a 131I solution with an activity of 5 kBq/mL for the CT and SPECT studies, respectively. Three external markers (multimodality radiographic marker MM3003; IZI Medical Products) suitable for CT and SPECT scans were defined on the surface of the phantom. The MM3003 marker is disk shaped, with a sealant covering the top and forming a well in the center. For SPECT, 99mTc-pertechnetate (approximately 185 Bq per marker) was placed in the well of the external markers.
SPECT images were obtained using a dual-head γ-camera (Picker Prism 2000; Marconi Medical Systems) equipped with high-energy parallel-hole collimators. Acquisitions were performed with dual-energy windows: a 20% energy window centered at 364 keV for the 131I images and a 20% window centered at 141 keV for the markers (99mTc). The data acquisition included a 360° rotation with 72 projections and a matrix of 64 × 64. CT images were obtained using multislice spiral CT scanning (Aquilion; Toshiba).
Clinical Feasibility Study
Patients.
131I SPECT/CT fusion images after an oral therapeutic dose of 131I (3.7–7.4 GBq) were obtained for 17 consecutive patients whose 131I planar images showed an abnormality. The patients (8 male, 9 female; age range, 15–79 y; mean age, 49.5 y) had differentiated thyroid carcinoma (13 with papillary carcinoma, 4 with follicular carcinoma) and had undergone total thyroidectomy. Each patient gave informed consent for participation in the study.
CT.
CT was performed 7 d after administration of a therapeutic dose of 131I. Before CT acquisition, 3 external markers were placed at 3 locations: on the glabella and left and right axillary areas for neck SPECT; on the manubrium and left and right axillary areas for thoracic SPECT; around the umbilicus and the iliac crests for abdomen/pelvis SPECT; and on the pubic bone and left and right thighs for leg SPECT. While the patient was breathing naturally, multislice spiral CT (Aquilion) was performed on the lesion site that was suspected on the basis of 131I planar images. The patients had their arms beside the body for neck imaging and behind the head for imaging of the thorax-to-leg region. The imaging protocol consisted of a 5- to 10-mm section thickness and a matrix size of 512 × 512.
131I SPECT.
131I SPECT was performed on the same day as CT. Images were obtained using a dual-head γ-camera (Picker Prism 2000; Marconi Medical Systems) equipped with high-energy parallel-hole collimators. Anterior and posterior spot imaging for 5 min and whole-body imaging at a speed of 9 cm/min were performed. SPECT was performed on the same day with the patient in a similar position, including arm position, as during the CT study and was focused on the suspected area of the lesion as seen on 131I planar images. Before SPECT, 99mTc-pertechnetate (approximately 185 Bq per marker) was injected in each of the 3 markers on the skin. Acquisitions were performed with dual-energy windows: a 20% energy window centered at 364 keV for the 131I images and a 20% window centered at 141 keV for the markers (99mTc). This yielded 2 simultaneously acquired sets of images: one showing the 131I distribution and the other, the radioactive markers. The data acquisition included a 360° rotation with 72 projections and a matrix of 64 × 64. Iterative reconstruction was performed.
131I SPECT/CT Fusion
Fusion images were constructed by combining morphologic CT and functional SPECT images on a computer workstation (Odyssey FX; Shimadzu). CT and SPECT data were transferred to the workstation by a DICOM network. The 2 sets of data were arranged to obtain a common matrix of 256 × 256. Datasets of CT and SPECT were fused using external landmarks and commercial software (Volume Registration; Shimadzu). The fusion algorithm of this program is based on the point-match method. With this method, up to 10 points in space can be marked manually as corresponding point pairs, within the CT volume data as well as within the SPECT volume data. If at least 3 point pairs are set, the coordinate system of the volume dataset of the SPECT image is translated and rotated in space in such a way that the sum of the squared distances of the point pairs is a minimum. After image fusion of the CT data and the resampled SPECT data, corresponding 5.6-mm-thick transaxial, coronal, and sagittal slices were obtained and simultaneously displayed, using a linked cursor. For fusion image display, an interlaced pixel approach was used, with CT images in gray scale and superimposed SPECT images in a bright color scale.
To quantitatively determine the accuracy of superimposition in the preclinical phantom study, the error of the point matching was shown as a root mean square (rms) of the point-pair distances in millimeters.
In the clinical study, data from both planar and SPECT 131I images and CT images were first separately assessed by 2 nuclear medicine physicians. Tumor uptake of 131I was defined as any focal or diffuse activity at sites incompatible with normal activity. A lymph node size of 10 mm in the short axis was used as a criterion for the presence of metastatic nodal involvement on CT. The 131I SPECT/CT fusion images were then interpreted by the 2 physicians. Briefly, each individual CT abnormality was examined for pathologic 131I uptake, and, conversely, suspected 131I foci were compared with CT findings. Fusion images were considered to improve image interpretation in comparison with CT and scintigraphy separately when they better localized sites of increased radiopharmaceutical uptake. The gold standard for confirming the presence or absence of malignancy was surgery or clinical and radiologic follow-up of at least 6 mo.
RESULTS
Preclinical Phantom Study
Using the 3 external markers, the mean deviation expressed as rms in millimeters for CT/SPECT fusions was 2.65 ± 0.74 (±SD). This deviation was less than the intrinsic resolution of the SPECT image (7 mm).
Clinical Feasibility Study
All lesions in the present study could not be confirmed by surgery and were validated by radiologic and clinical follow-up of at least 6 mo.
CT and 131I Scintigraphy Analysis Before Image Fusion.
Both CT and 131I scintigraphy showed the same pathologic sites in 5 of 17 patients (29%). However, it was difficult to determine the precise location of the foci from SPECT images alone in 3 patients. In 2 patients, both imaging modalities showed abnormality in the mediastinal lymph node. In the remaining 12 patients, CT showed normal findings, whereas 131I scintigraphy showed abnormal findings.
131I SPECT/CT Fusion Data.
Additional information for image interpretation was provided by 131I SPECT/CT fusion images in comparison with CT and 131I scintigraphy separately in 15 of 17 patients (88%). The details of imaging data are listed in Table 1. In 4 patients, CT showed normal-sized lymph nodes, smaller than 1 cm in diameter, whereas 131I scintigraphy showed abnormal findings. In 3 patients with bone metastasis, fusion images confirmed the precision of the localization of abnormal 131I uptake. Five bone metastases (Fig. 1) and 1 muscle metastasis (Fig. 2) were occult metastases and were not seen on the CT images. Finally, 131I scintigraphy showed abnormal findings for 2 patients for whom the CT findings were initially considered normal. Fusion images confirmed the precision of the localization of physiologic 131I uptake.

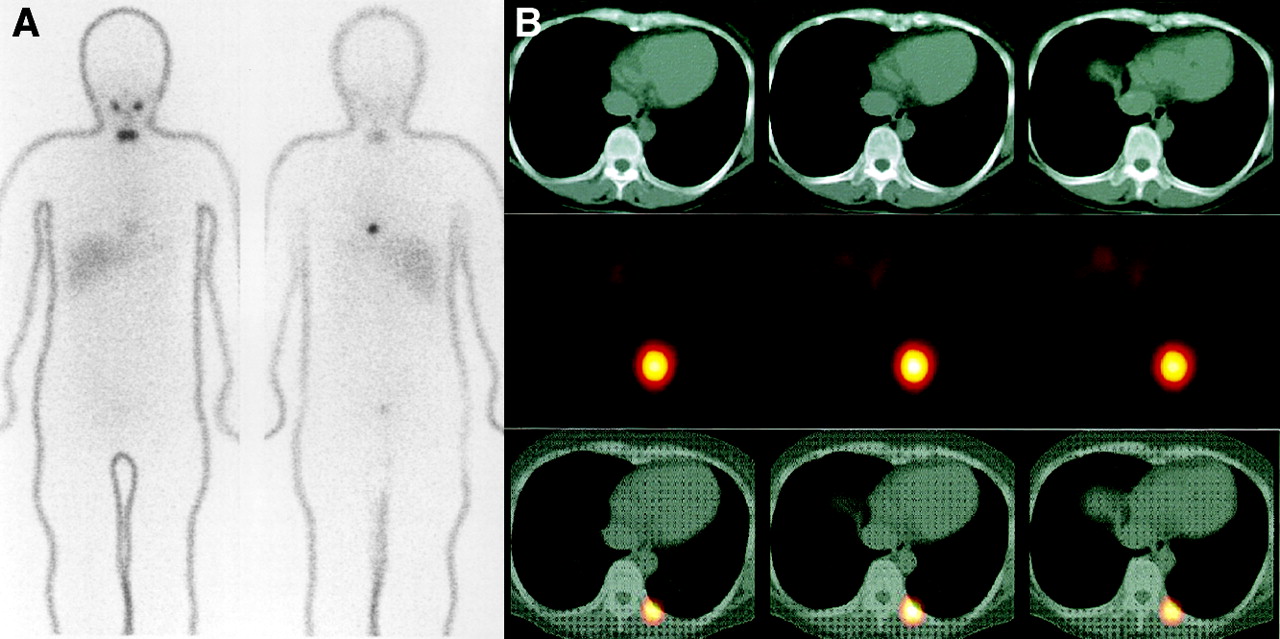
A 47-y-old woman (patient 5) with differentiated papillary thyroid carcinoma underwent total thyroidectomy. (A) 131I whole-body images (left, anterior view; right, posterior view). (B) CT images (first row), 131I transaxial SPECT images (second row), and 131I SPECT/CT fusion images (third row). 131I planar and SPECT images show intense focal uptake in posteromedial region, but slightly on left side of chest, suggesting thoracic spine involvement. Uptake in neck is thyroid bed. Bone appears normal on diagnostic CT scan. 131I SPECT/CT fusion images show that intense tracer uptake is in posterior portion of 9th rib and not in thoracic vertebra. In this patient, final diagnosis was made on basis of follow-up; follow-up period was 12 mo, and clinically, fusion images confirmed precision of localization of abnormal 131I uptake.

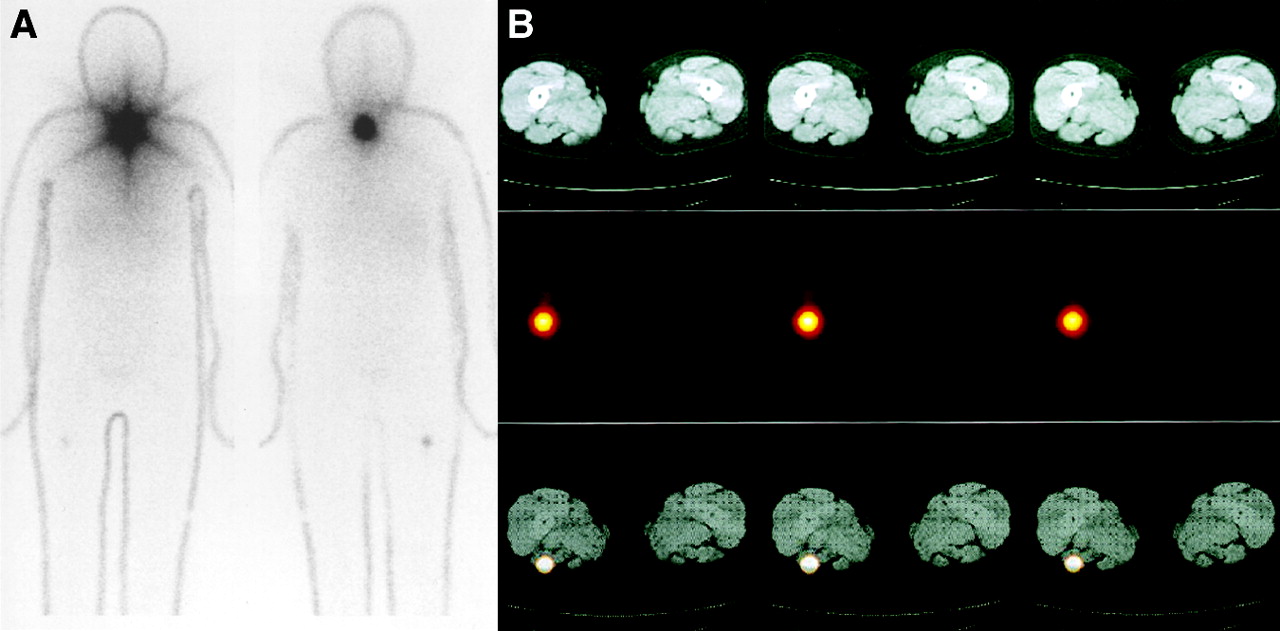
A 72-y-old woman (patient 13) with differentiated papillary thyroid carcinoma underwent total thyroidectomy. (A) 131I whole-body images (left, anterior view; right, posterior view). (B) CT images (first row), 131I transaxial SPECT images (second row), and 131I SPECT/CT fusion images (third row). 131I planar and SPECT images show focal uptake in posterior part of right thigh, suggestive of right femoral bone or muscle involvement. Intense uptake in neck is thyroid bed. Bone appears normal on diagnostic CT scan. 131I SPECT/CT fusion images show that intense tracer uptake is located in biceps of right thigh and not in femoral bone. In this patient, final diagnosis was made on basis of follow-up; follow-up period was 9 mo, and clinically, fusion images confirmed precision of localization of abnormal 131I uptake.
Detailed Data for Patients for Whom Additional Information Was Provided by Fusion Imaging
In 2 patients—patients 6 and 8 in Table 1—in whom bone metastasis with suspected nonosseous metastasis was detected separately on CT and SPECT, fusion images did not change the decision regarding the use of 131I treatment but did influence the therapeutic dose of 131I. In patients 14 and 15, on the other hand, fusion images excluded the tumor as the cause of uptake by showing the suspected focus to be in physiologic sites. These 2 patients were spared unnecessary treatment.
DISCUSSION
Using external markers, we have demonstrated the clinical usefulness of 131I SPECT/CT fusion images in patients with differentiated thyroid carcinoma. Different imaging modalities provide different but complementary information. Both CT and MRI are used primarily for imaging anatomic changes associated with an underlying pathology, whereas the molecular imaging techniques of PET and SPECT capture functional or metabolic changes associated with the pathology. The use of anatomic and functional image fusion is increasing in nuclear medicine, and especially in oncology (1,2,5–15). Anatomic and functional information are combined to aid diagnosis, allow accurate tumor localization, and improve the outcome of treatment planning (12).
Whole-body imaging after an oral dose of 131I is commonly performed to identify residual or metastatic tumor during the treatment of differentiated thyroid carcinoma. Scintigraphic procedures after administration of 131I have a higher sensitivity for the detection of metastases from thyroid carcinoma than do anatomic imaging modalities. However, interpretation of 131I images is difficult because of the absence of readily identifiable anatomic structures. Therefore, precise lesion localization is often not possible. In addition, knowledge about 131I physiologic uptake is essential to avoid false-positive results in the interpretation of 131I SPECT. It is also important for assessing additional 131I treatment and monitoring the response to therapy. Correlation of anatomic and metabolic images is usually done visually by separate readings of CT/MRI and SPECT images. Misinterpretations can result, especially for small lesions. In the present study, 131I SPECT/CT fusion imaging allowed precise localization of 131I uptake in patients with differentiated thyroid carcinoma and, in comparison with separate analysis of CT and scintigraphy, improved the diagnosis in 15 of 17 patients (88%). In the abdominal and pelvic areas, 131I SPECT/CT fusion imaging helped in differentiating physiologic urinary bladder elimination of 131I from its abnormal uptake. The therapeutic dose of 131I was changed in 2 patients because of the findings of fusion imaging. Two other patients were spared unnecessary treatment because of the fusion findings. For these 4 patients, the information provided by the image registration technique had an impact on management.
Perault et al. assessed the feasibility of registration with CT in 13 patients with endocrine carcinoma evaluated with 131I, 131I-MIBG, and 111In-pentetreotide (14). The investigators obtained simultaneous dual-isotope acquisitions using these agents and 99mTc-methylene diphosphonate to get information on skeletal structures that could subsequently be correlated with anatomic data provided by CT. In their study, fused images allowed the detection and correct localization of 6 unsuspected sites of disease. At 2 sites, fusion led to better localization of known lesions; at 2 other sites, disease uptake was related to inflammatory changes seen on CT scans. The clinical value of combined transmission and emission tomography imaging was assessed using 131I, 123I-MIBG, 75Se-cholesterol, 111In-pentetreotide, and 99mTc-MIBI in 27 patients with endocrine tumors (15). For 41% of the patients, fused images improved the accuracy of nuclear medicine studies by providing better localization of SPECT-detected lesions. For one third of the patients, image fusion had a clinical impact on management.
Multimodality image coregistration can be achieved by several techniques using external markers or internal landmarks. Most fusion algorithms have been developed for brain imaging. The brain, being a rigid body, allows accurate registration (16). Internal landmarks relating to well-known sites of physiologic uptake have not been used with 131I SPECT, probably because of the lack of reliable potential internal markers. In the present study, the method used external markers placed at specific positions on the patient’s body. This method requires that CT and SPECT be performed on the same day, that the patient be imaged in the same position for both CT and SPECT, and that external markers be carefully matched. Respiration might affect that relationship, thus affecting the reliability and usefulness of the registration process. In our study, CT and SPECT were both performed while the patients were breathing freely. This was possible even in moderately cooperative patients, because of the short scanning time of helical CT. In point matching, the transformation parameters were determined by establishing a correspondence between a set of landmarks visible in both imaging modalities and minimizing the mismatch between these points. The rms error of 2.65 mm obtained in this study appears to be sufficient in view of the SPECT resolution. The accuracy obtained with the markers described here should be sufficient for image fusion of CT and SPECT. One partial solution to positioning problems is provided by integrated SPECT/CT or PET/CT systems that acquire both anatomic and functional information in the same examination (5–7). These systems allow the patient to be imaged in exactly the same position, reducing the artifacts that occur because of unavoidable minimal differences in positioning when CT and SPECT are performed successively. However, combination of the 2 modalities in the clinical setting is associated with many practical problems, such as high cost and lack of availability.
Realignment is fast when external markers are used, and a technologist trained to work with the realignment software can perform the entire procedure in less than 10 min. For clinically oriented settings, establishing such a method may be a cost-effective alternative to investment in a combined SPECT/CT device. However, it is difficult to overlap images on the correct plane because SPECT images are not sharp. In addition, because the marker definition was done manually, a small intra- and interobserver variability was possible. In the future, automated landmark selection will replace most of the manual landmark selection used in this study and should decrease the time required for fusion. Overall, the present study had some limitations. First, no lesions could be validated by histologic examination. All were validated by radiologic and clinical follow-up. This limitation was due to a selection bias toward patients presenting with occult metastasis not shown on conventional imaging or advanced disease without the need for lesion biopsy or surgery. Second, choosing the CT-scanning area on the basis of 131I planar images and not on SPECT images might have led to missed lesions. Third, only 3 external markers were used. Further studies on the clinical usefulness of fusion images are needed, using more than 3 external markers and with precise coordination between anatomic and functional images.
CONCLUSION
For registration of anatomic and functional images in fusion imaging, the external-marker method of the present study was simple and practical. 131I SPECT/CT fusion images obtained with this technique may improve the anatomically limited interpretation of 131I scintigraphy alone for patients with differentiated thyroid carcinoma.
Footnotes
Received Mar. 26, 2003; revision accepted Sep. 8, 2003.
For correspondence or reprints contact: Yuka Yamamoto, MD, Department of Radiology, Kagawa Medical University, 1750-1 Ikenobe, Miki-cho, Kita-gun, Kagawa 761-0793, Japan.
E-mail: yuka{at}kms.ac.jp
REFERENCES
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- I-131 Postablation SPECT/CT Predicts Relapse of Papillary Thyroid Carcinoma more Accurately than Whole Body Scan
- Radioiodine Scintigraphy with SPECT/CT: An Important Diagnostic Tool for Thyroid Cancer Staging and Risk Stratification
- Radioiodine Scintigraphy with SPECT/CT: An Important Diagnostic Tool for Thyroid Cancer Staging and Risk Stratification
- The Effect of Posttherapy 131I SPECT/CT on Risk Classification and Management of Patients with Differentiated Thyroid Cancer
- Hybrid SPECT/CT: the end of "unclear" medicine
- 131I SPECT/CT in the Follow-up of Differentiated Thyroid Carcinoma: Incremental Value Versus Planar Imaging
- A Proposition for the Use of Radioiodine in WDTC Management
- Incremental Value of 131I SPECT/CT in the Management of Patients with Differentiated Thyroid Carcinoma
- Localization of Metastases from Malignant Pheochromocytoma in Patients Undergoing 131I-MIBG Therapy with Manually Fused 123I-MIBG SPECT and CT Images
- SPECT/CT
- SPECT/Multislice Low-Dose CT: A Clinically Relevant Constituent in the Imaging Algorithm of Nononcologic Patients Referred for Bone Scintigraphy