


Article Figures & Data
Figures
- FIGURE 1.
Patient with melanoma on vertex of scalp just to left of midline and lymphatic drainage down to left level V node at base of neck. (A) Lymphoscintigraphy findings on delayed imaging 2 h after injection of 7 MBq of 99mTc-antimony sulfide colloid intradermally at 4 points around excision biopsy site. Anterior and left lateral views are shown, and lymphatic vessel can be faintly seen passing directly to sentinel node in left lateral view. Lt = left; Rt = right. (B) Patient at end of study. Sentinel node (SN) location is marked on skin with “X.” Injection site on scalp is indicated by thick arrow.
- FIGURE 2.
Lymphoscintigraphy of patient with excision biopsy site on anterior left thigh above knee. Two lymphatic collecting vessels can be seen passing to left groin in 10-min summed dynamic image (top left). Medial channel can be seen draining to sentinel node in femoral area, whereas more lateral channel bypasses this node to reach another sentinel node higher in groin. Delayed images show these 2 bright sentinel nodes with faint second-tier activity between them. Depth of sentinel nodes beneath skin is shown in left lateral view with point source on skin marks (bottom right). Lt = left; Rt = right.
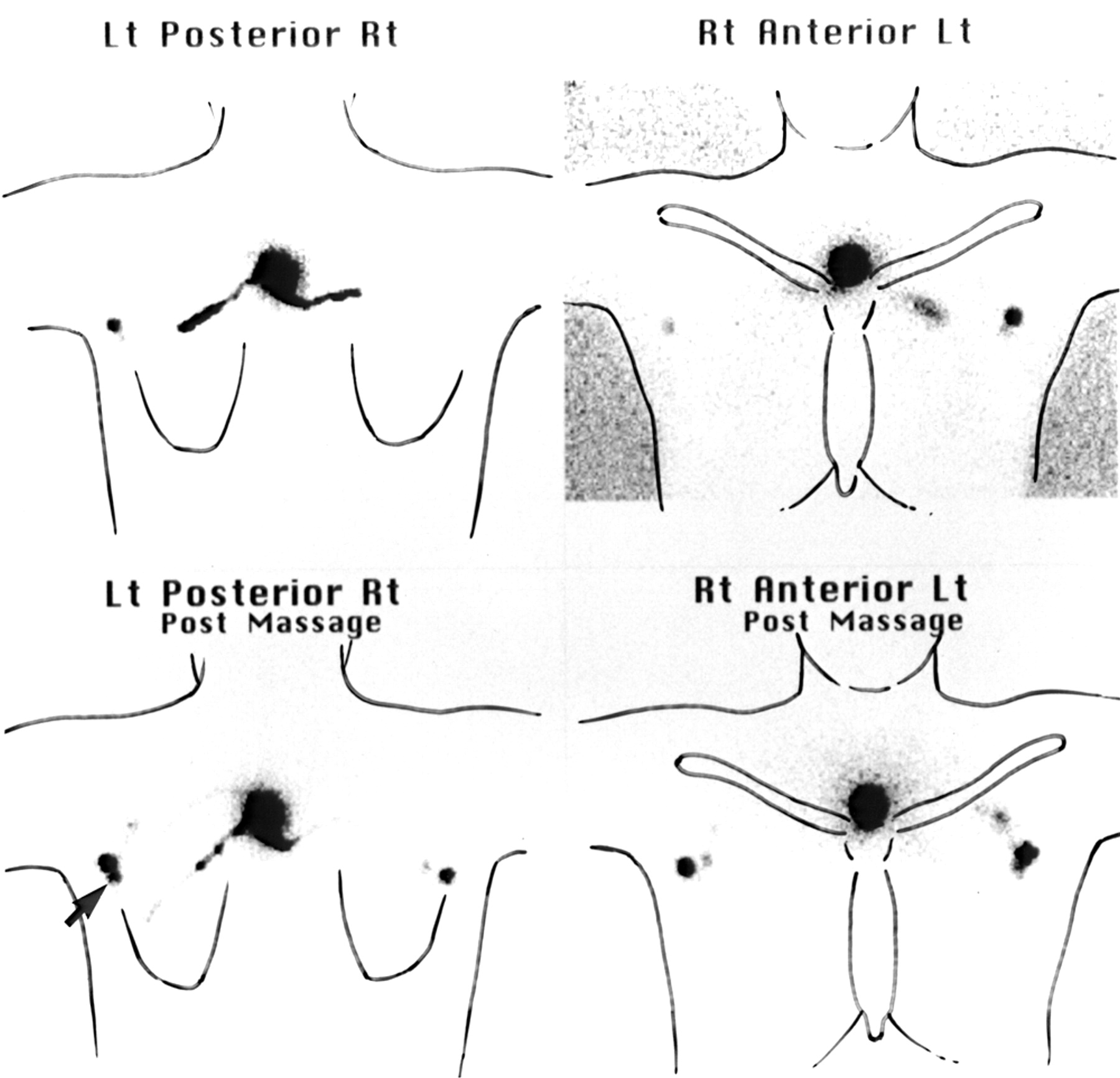
- FIGURE 3.
Lymphoscintigraphy of patient with excision biopsy site on upper back close to midline. (Top row) Delayed images, obtained 2 h after injection of tracer, show faint right axillary sentinel node and brighter left axillary sentinel node. (Bottom row) Images taken immediately after 2 min of massage show that tracer has moved to second sentinel node in left axilla (arrow) and that right axillary sentinel node is much brighter. Even light external pressure significantly decreased lymph flow. Lt = left; Rt = right.
- FIGURE 4.
Dynamic-phase lymphoscintigraphy of patient with melanoma excision biopsy site (open straight arrow) on right heel. Multiple lymphatic collecting vessels can be seen passing up leg to right groin. These vessels reach multiple sentinel nodes (curved arrow). Note tortuous path followed by 1 lymph vessel to faint sentinel node high in groin (solid straight arrow). LT = left; RT = right.
- FIGURE 5.
Lymphoscintigraphy of patient with excision biopsy site on posterior left calf. (Top row) Summed dynamic images show 3 lymphatic collecting vessels converging to single sentinel node in left groin. (Bottom row) Delayed images, obtained 2 h later, show single left groin sentinel node. Note that there are no second-tier nodes and that all tracer is retained in sentinel node. Lt = left; Rt = right.
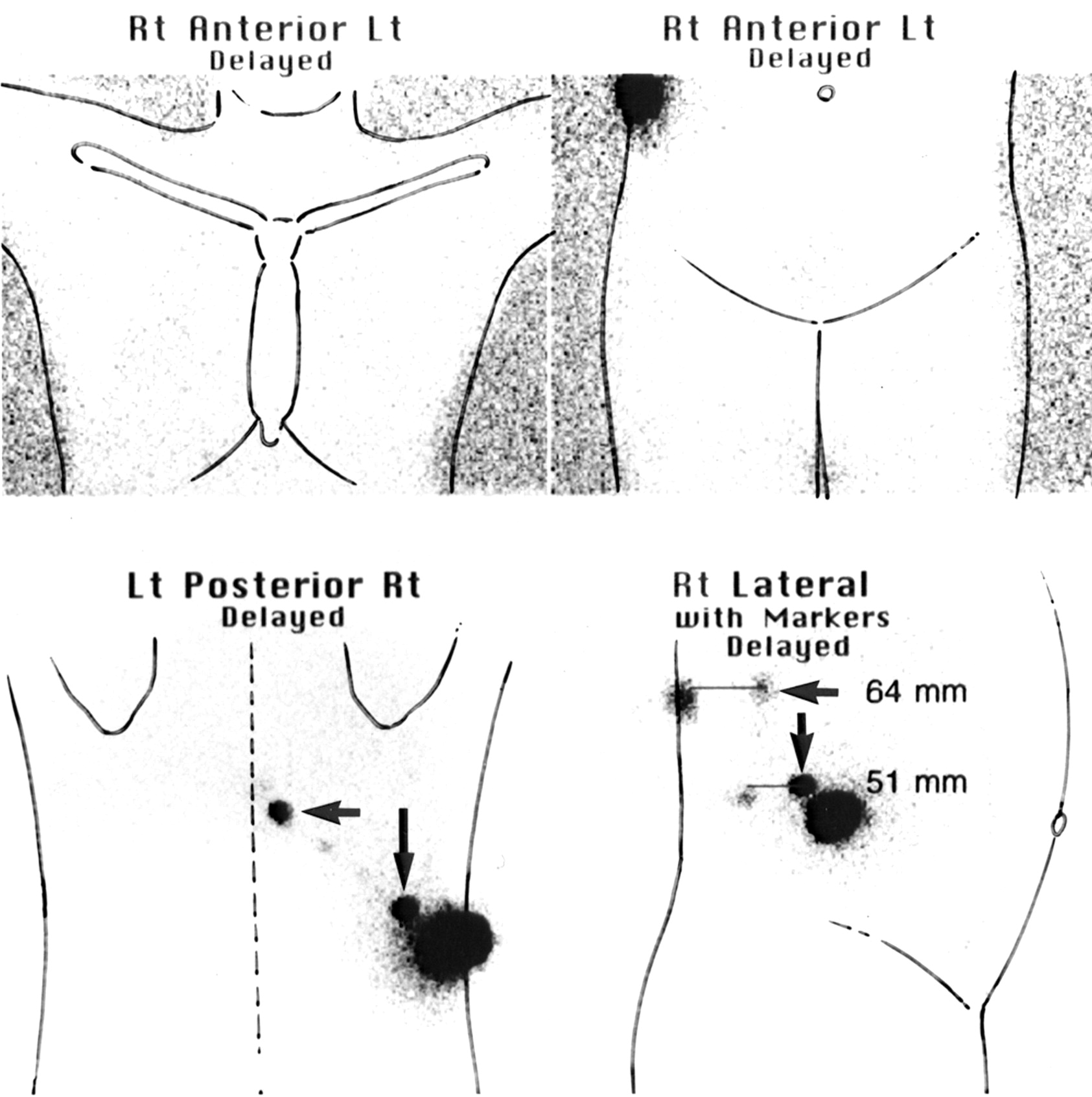
- FIGURE 6.
Lymphoscintigrams of 2 patients with excision biopsy sites on upper back close to midline. Each had sentinel node in left axilla, and summed dynamic image for each (top left) shows lymphatic collecting vessels reaching these sentinel nodes. (A) Faint sentinel node can be seen in right triangular intermuscular space (TIS) on dynamic image (arrow). (B) No TIS sentinel node can be seen on dynamic image. Delayed images show sentinel node in right TIS in both patients (arrows). This node is clearly seen in posterior and lateral views but is not seen in standard anterior views of axillae. Lt = left; Rt = right; RTIM = right triangular intermuscular space.
- FIGURE 7.
Delayed lymphoscintigraphy images of patient with melanoma excision biopsy site in posterolateral right loin area. Lymphatic channels passed directly through body wall to sentinel node in retroperitoneal area (vertical arrow) and sentinel node in right para-aortic region (horizontal arrow). There was no drainage to sentinel nodes in either axilla or groin. Depth of sentinel nodes is shown in right lateral view with point source on posterior skin mark. Nodes lay 5 and 6.5 cm deep relative to skin of back. Lt = left; Rt = right.
- FIGURE 8.
Lymphoscintigraphy of patient with excision biopsy site on upper back to right of midline. (Left) Two lymph vessels can be seen on posterior summed dynamic image, 1 passing over shoulder to sentinel node in right supraclavicular fossa and 1 passing to sentinel node in right axilla. (Right) Both of these sentinel nodes are visible on anterior delayed image. However, sometimes neck nodes are obscured by activity at injection site in such patients, and vertical oblique views are then required to clarify situation. Lt = left; Rt = right.
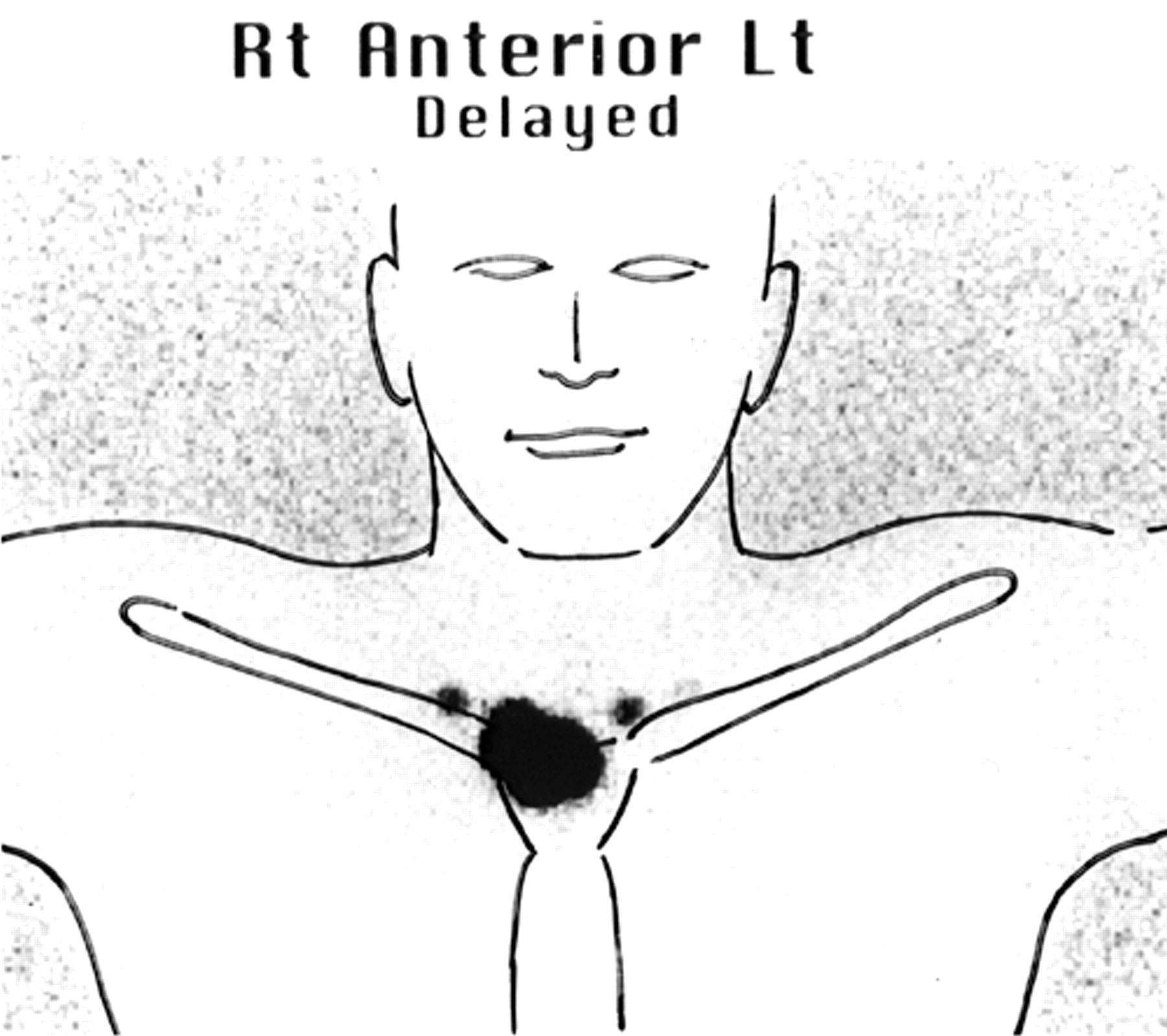
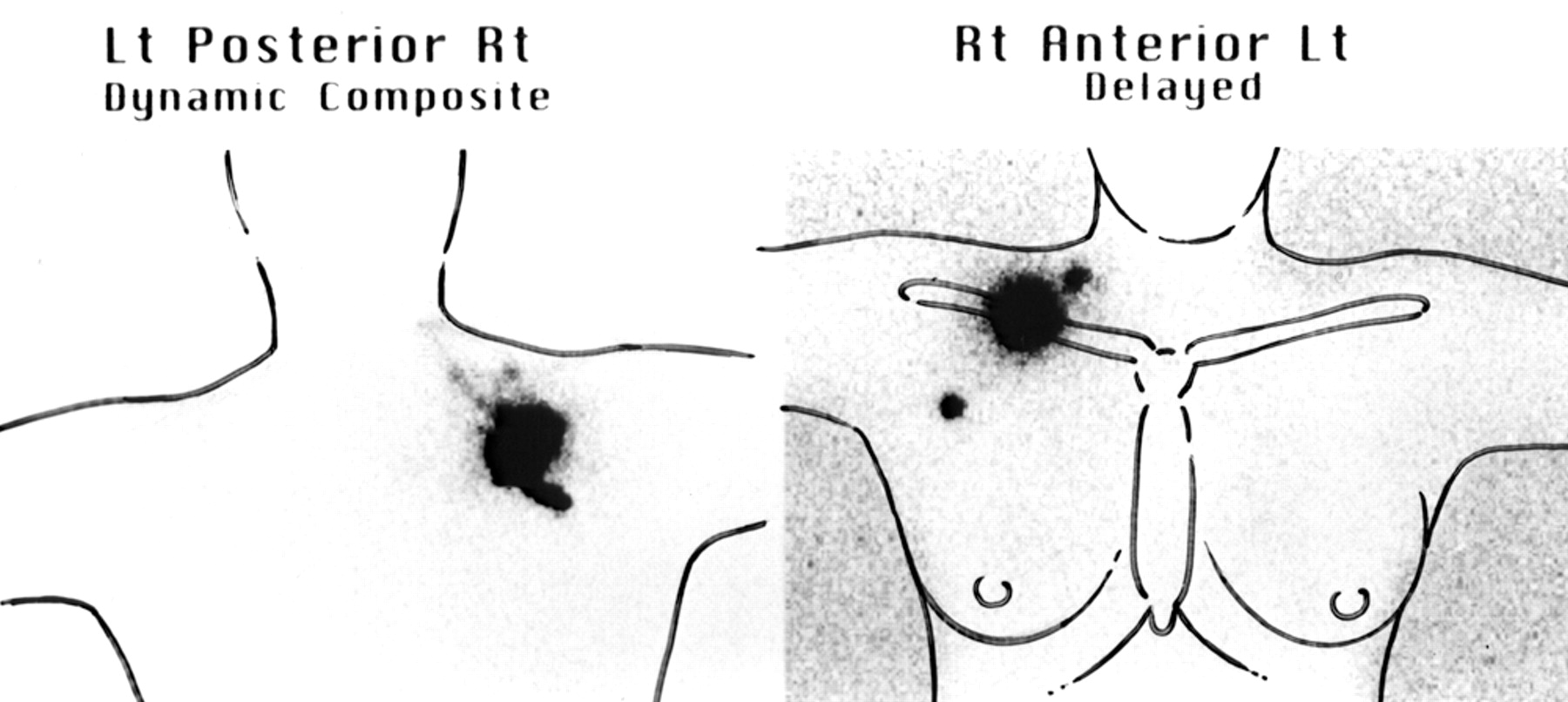
- FIGURE 9.
Delayed lymphoscintigraphy of patient with excision biopsy site over manubrium. Drainage to sentinel node in supraclavicular fossa on each side can be seen; there is no drainage to either axilla. Lt = left; Rt = right.
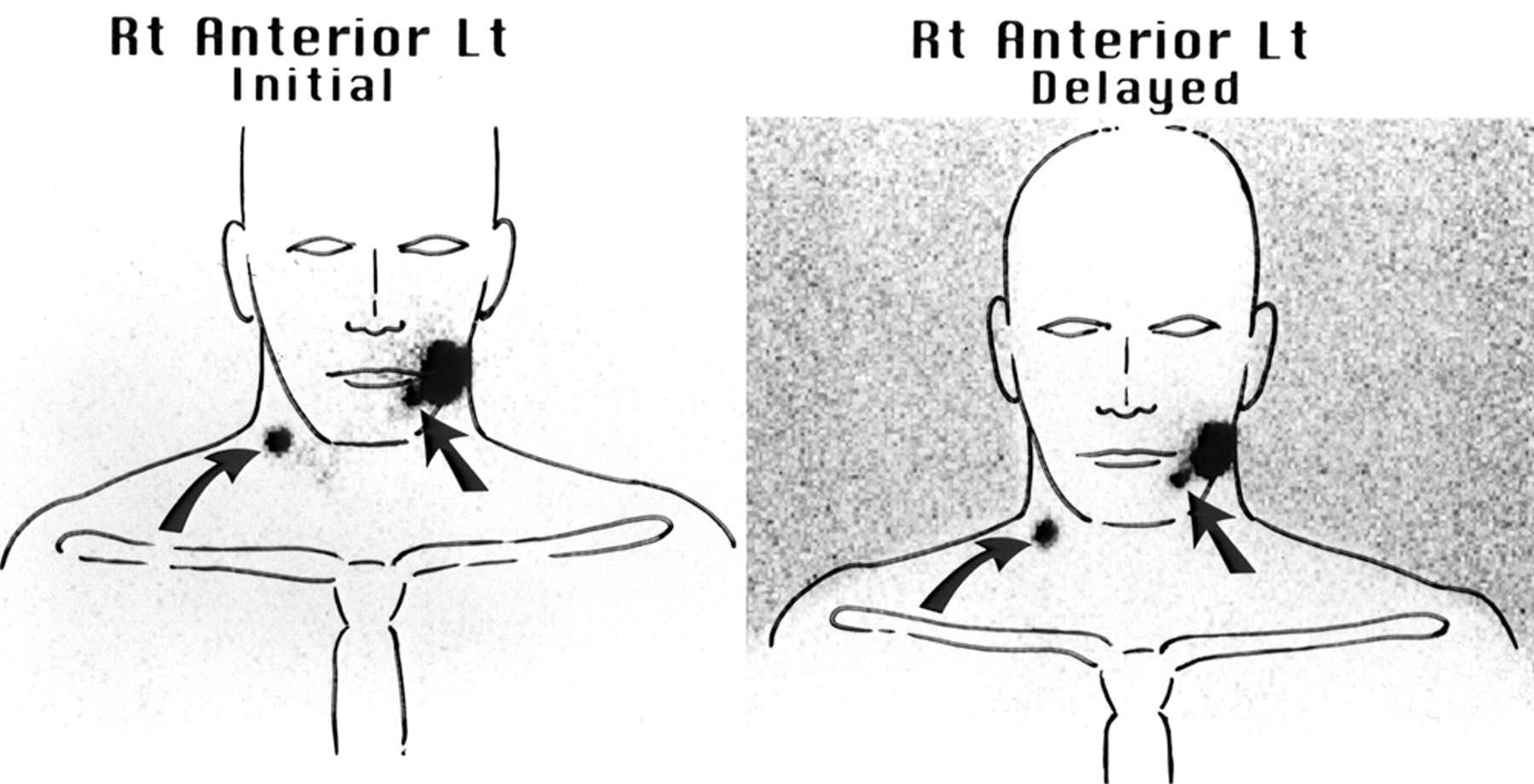
- FIGURE 10.
Dynamic and delayed lymphoscintigraphy of patient with excision biopsy site on left cheek. Sentinel node can be seen in left submandibular region (level I) (straight arrow). Another sentinel node can be seen in right midcervical area (level III) (curved arrow). Such contralateral drainage is not uncommon in head and neck. Lt = left; Rt = right.
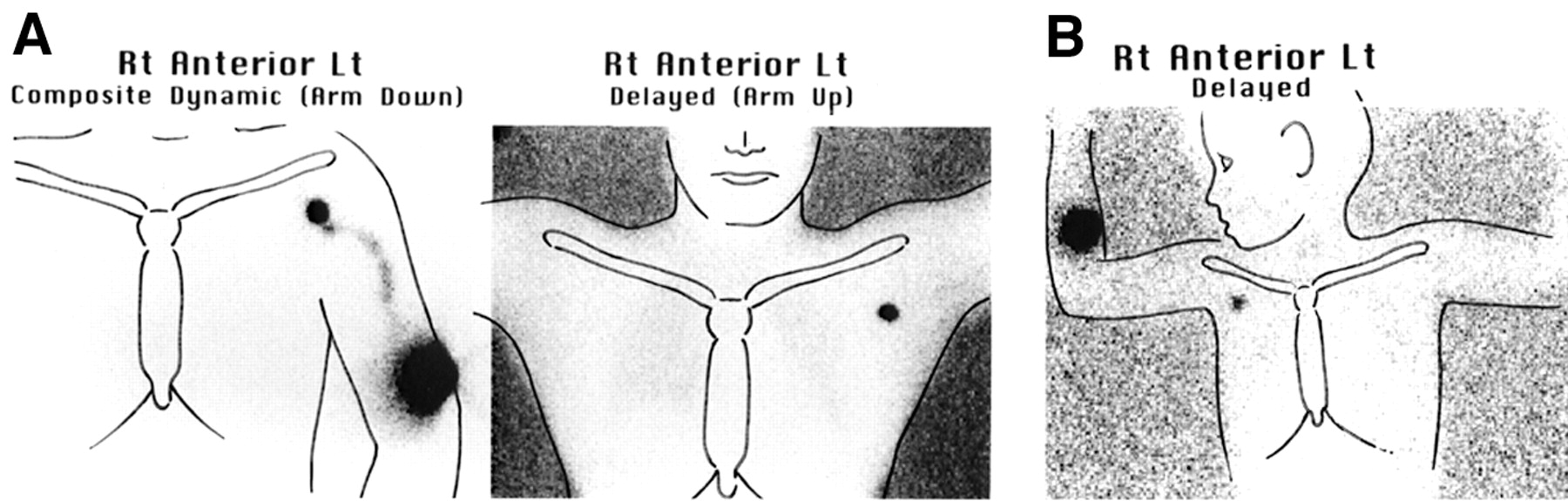
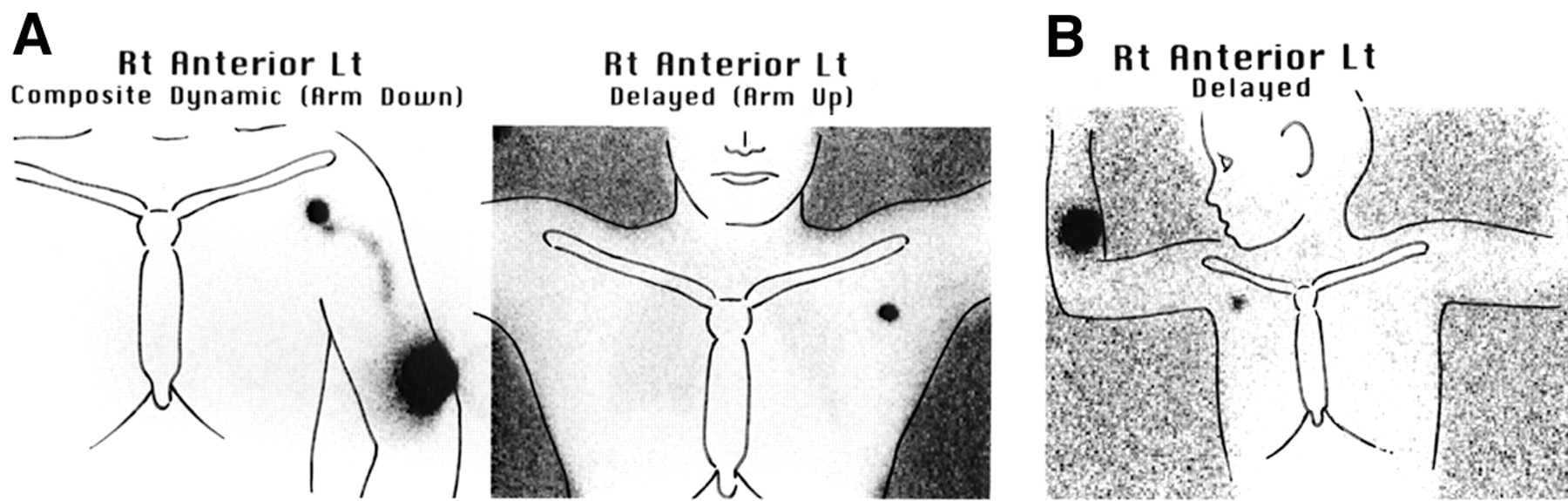
- FIGURE 11.
(A) Adult with left-arm melanoma shows single channel on dynamic lymphoscintigraphy passing to single left axillary sentinel node, also seen on delayed scan. (B) Two-year-old child with melanoma on right forearm shows single right axillary sentinel node on delayed lymphoscintigraphy. Most upper limb melanomas include axillary sentinel node. Lt = left; Rt = right.
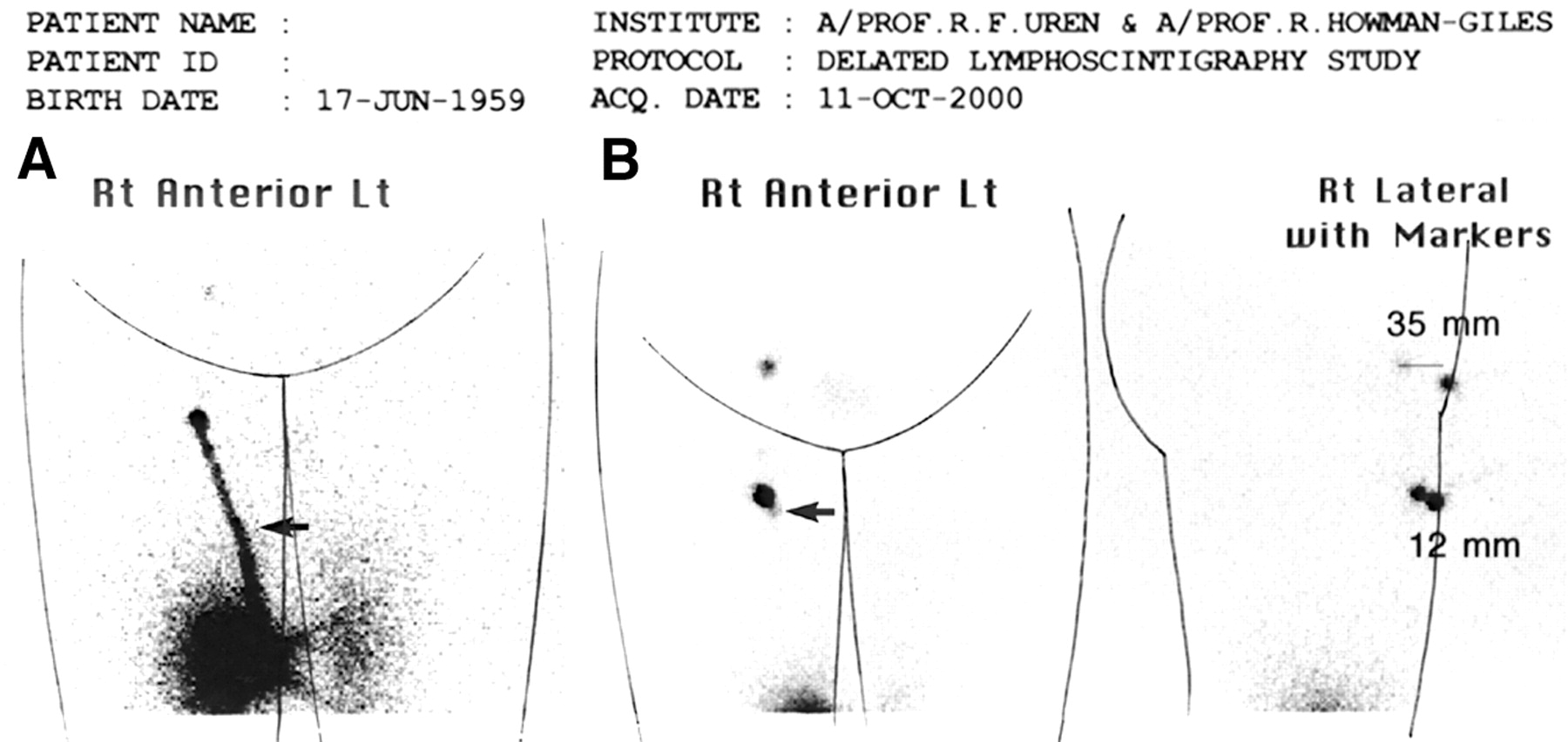
- FIGURE 12.
Lymphoscintigraphy of patient with excision biopsy site on medial right thigh anteriorly. (A) Summed dynamic image shows bright lymphatic collecting vessel passing to right groin sentinel node. Very faint second vessel can be seen medial to this vessel (arrow). (B) Delayed image shows bright sentinel node and second faint sentinel node just medial to this node (arrow). Second-tier node higher in groin receives tracer from bright sentinel node and is actually “hotter” than faint sentinel node. At histologic examination, bright sentinel node was normal, but faint sentinel node contained micrometastasis. Lt = left; Rt = right.
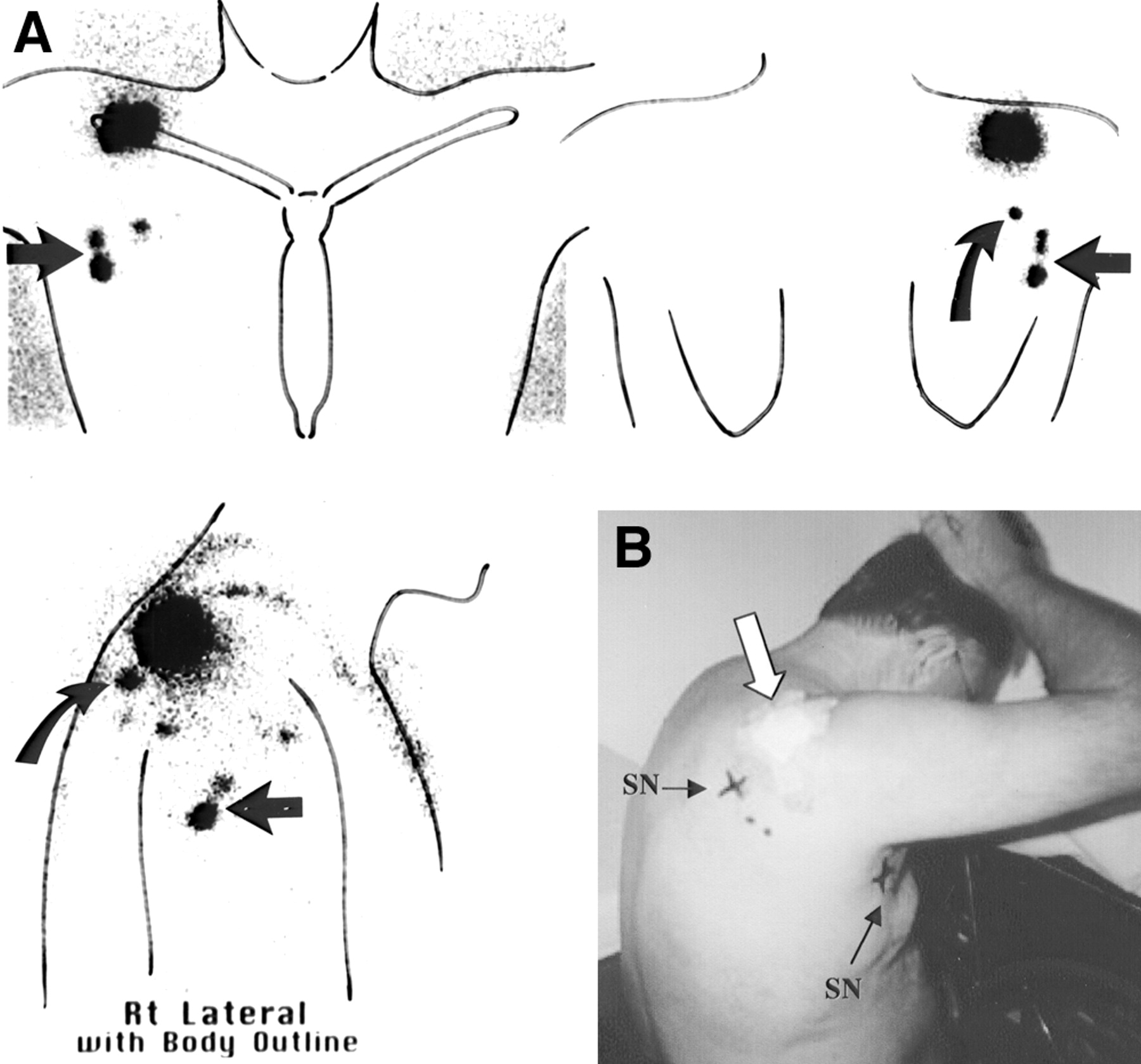
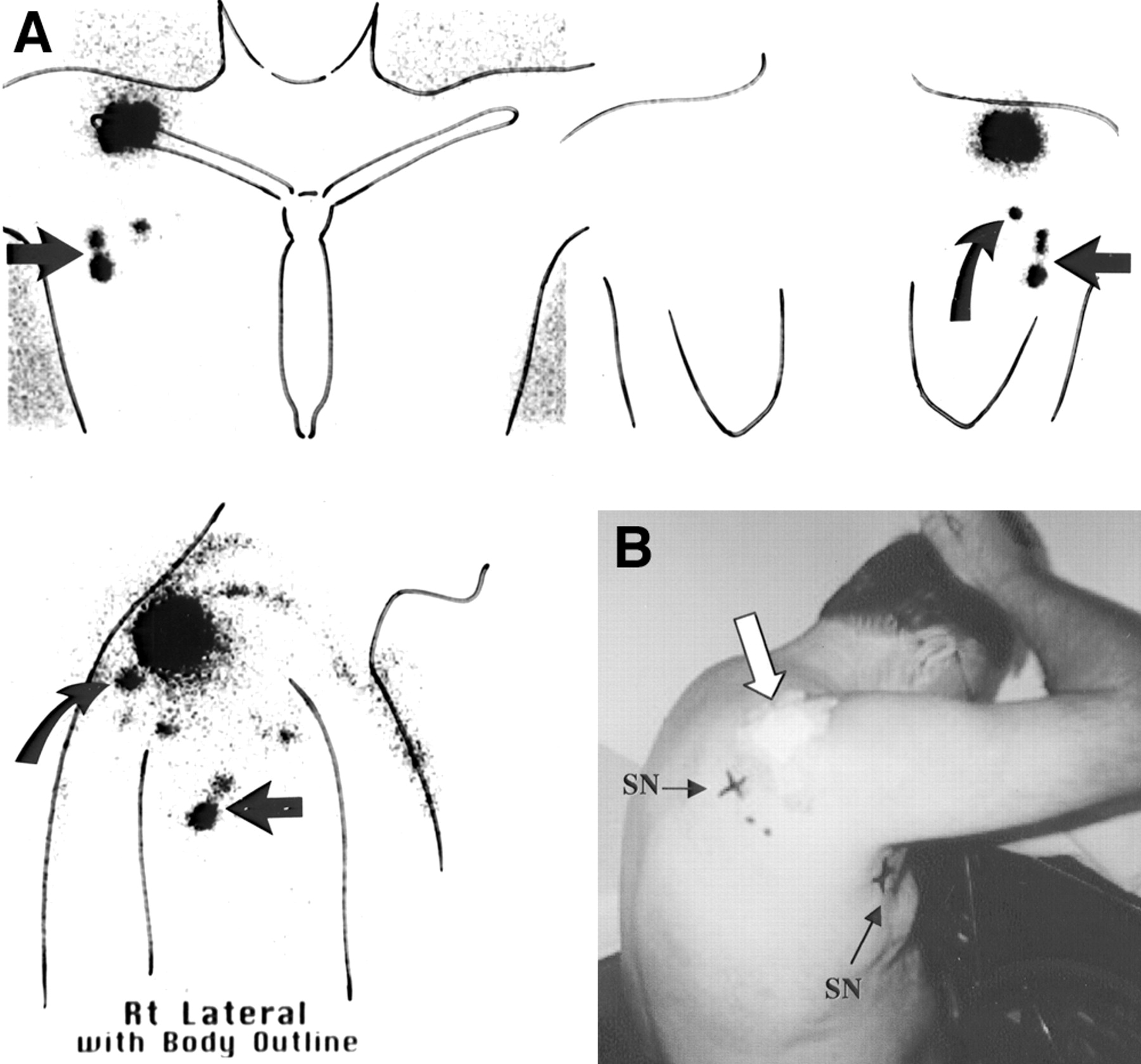
- FIGURE 13.
Patient with melanoma behind right shoulder. (A) Delayed lymphoscintigraphy images show 2 sentinel nodes in right axilla (straight arrow) and second-tier node in right axilla as well as sentinel node in right triangular intermuscular space (curved arrow). Lt = left; Rt = right. (B) Patient at end of study. “X” marks surface locations of right triangular intermuscular space sentinel node (SN) and 1 right axillary sentinel node. Melanoma site is indicated by thick arrow.
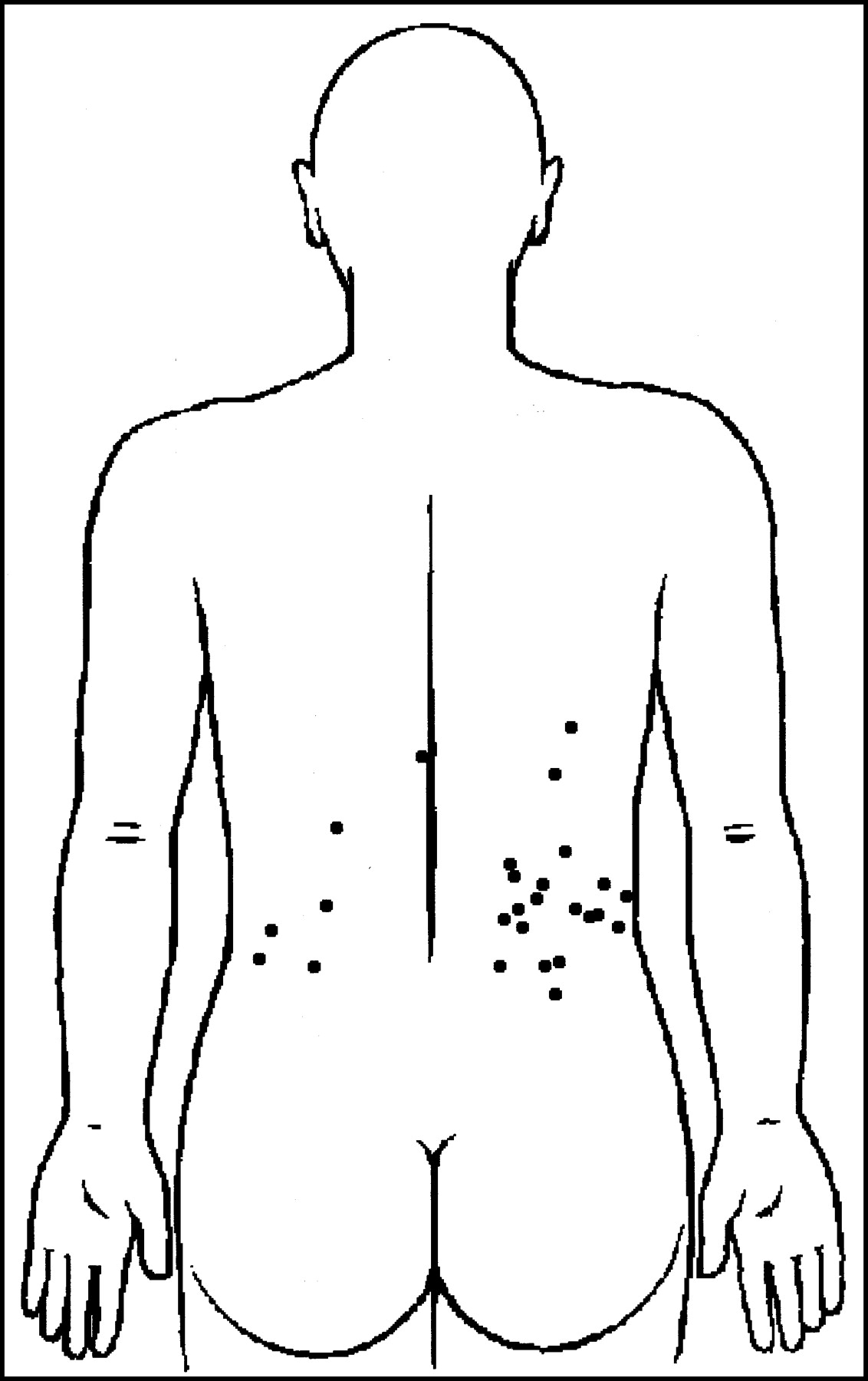
- FIGURE 14.
Locations of all skin sites draining to sentinel node in right or left triangular intermuscular space.
- FIGURE 15.
Location of skin sites draining directly through body wall to sentinel nodes in paravertebral, para-aortic, and retroperitoneal areas.
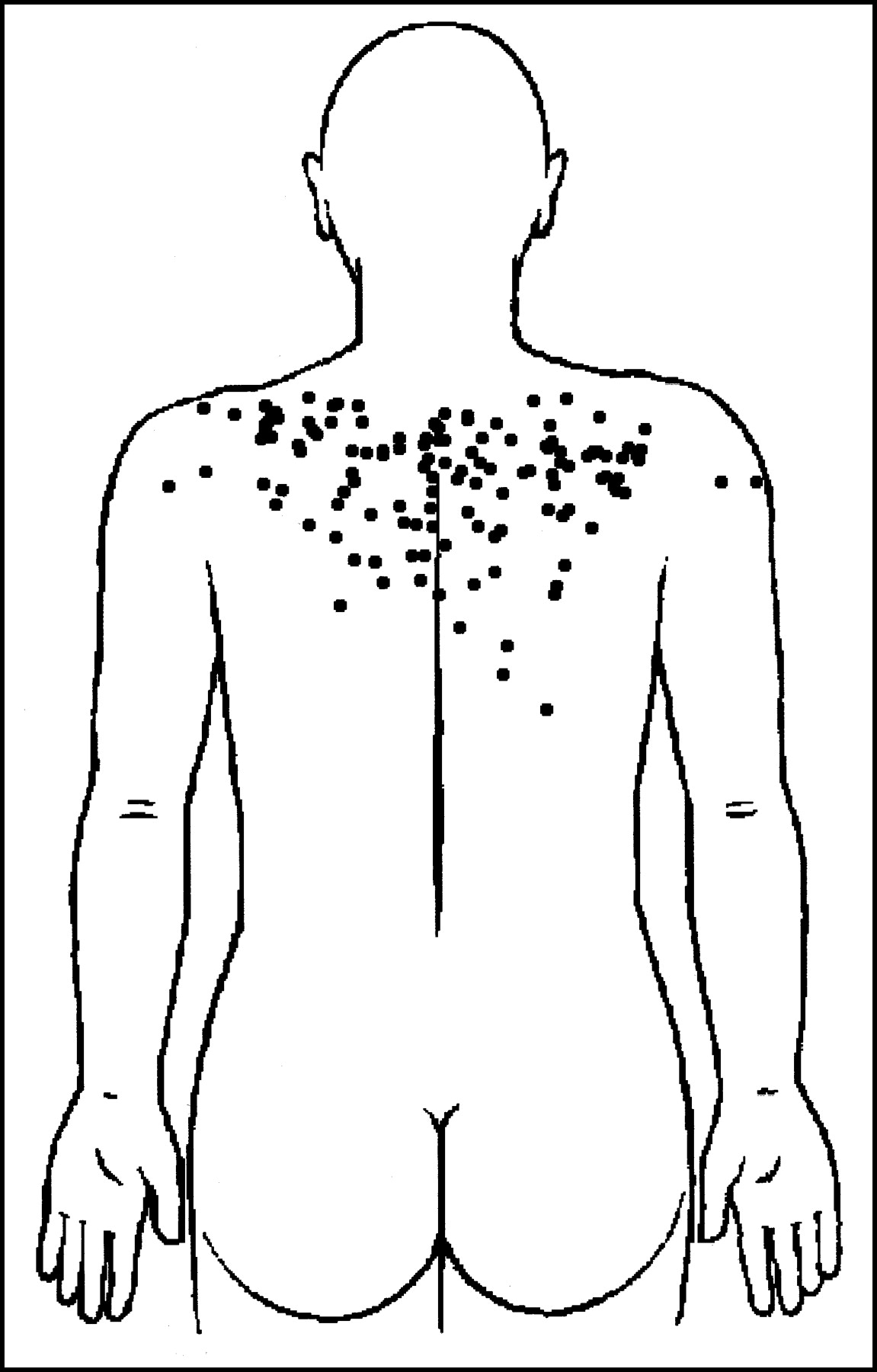
- FIGURE 16.
Locations of skin sites on back draining to sentinel nodes in supraclavicular fossa.
- FIGURE 17.
Locations of skin sites on back draining to right axilla (A) and left supraclavicular fossa (B). Note that drainage from contralateral side of back is common in each case.
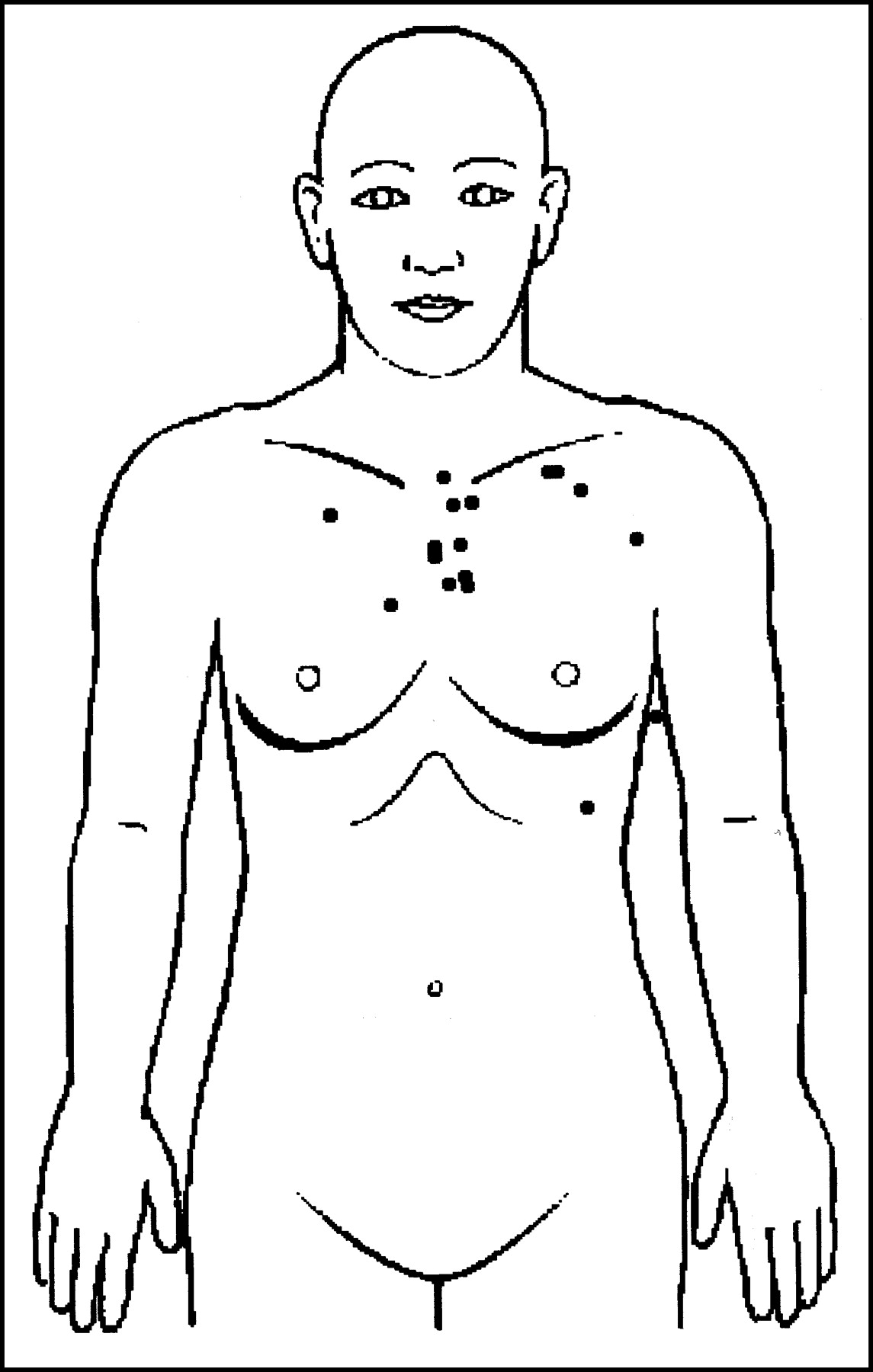
- FIGURE 18.
Locations of skin sites on anterior trunk draining to right or left supraclavicular fossa. This drainage occurs from more restricted area than on back, but some patients do show such drainage from low in anterior chest.
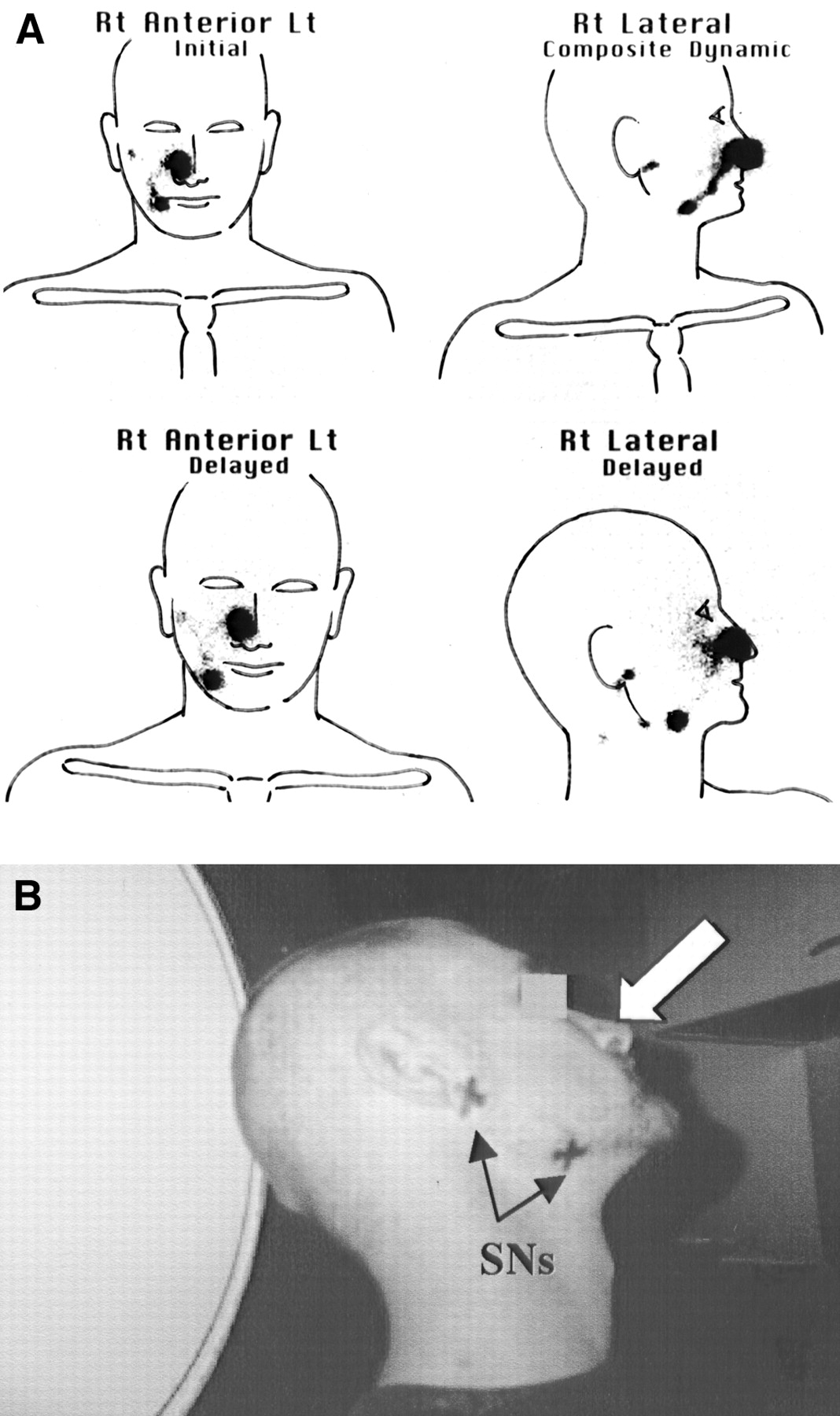
- FIGURE 19.
Patient with excision biopsy site on right side of nose. (A) (Top row) Summed dynamic lymphoscintigraphy images. (Bottom row) Delayed lymphoscintigraphy images. Two separate lymphatic vessels reach 2 sentinel nodes, 1 in parotid region and 1 in right submandibular region. Lt = left; Rt = right. (B) Patient at end of study. Sentinel node (SNs) are marked on skin with “X.” Melanoma site on nose is indicated by thick arrow. Multiple draining node fields are common in head and neck.
- FIGURE 20.
Patient with excision biopsy site on left arm above and behind elbow. (A) Lymphoscintigraphy shows that channels pass to interval node (1 of the sentinel nodes in this patient) in medial arm (curved arrow) and to 2 sentinel nodes in left axilla. Lt = left; Rt = right. (B) Patient at end of study. Melanoma site is indicated by thick arrow. Sentinel nodes (SNs) are marked on skin with “X.”
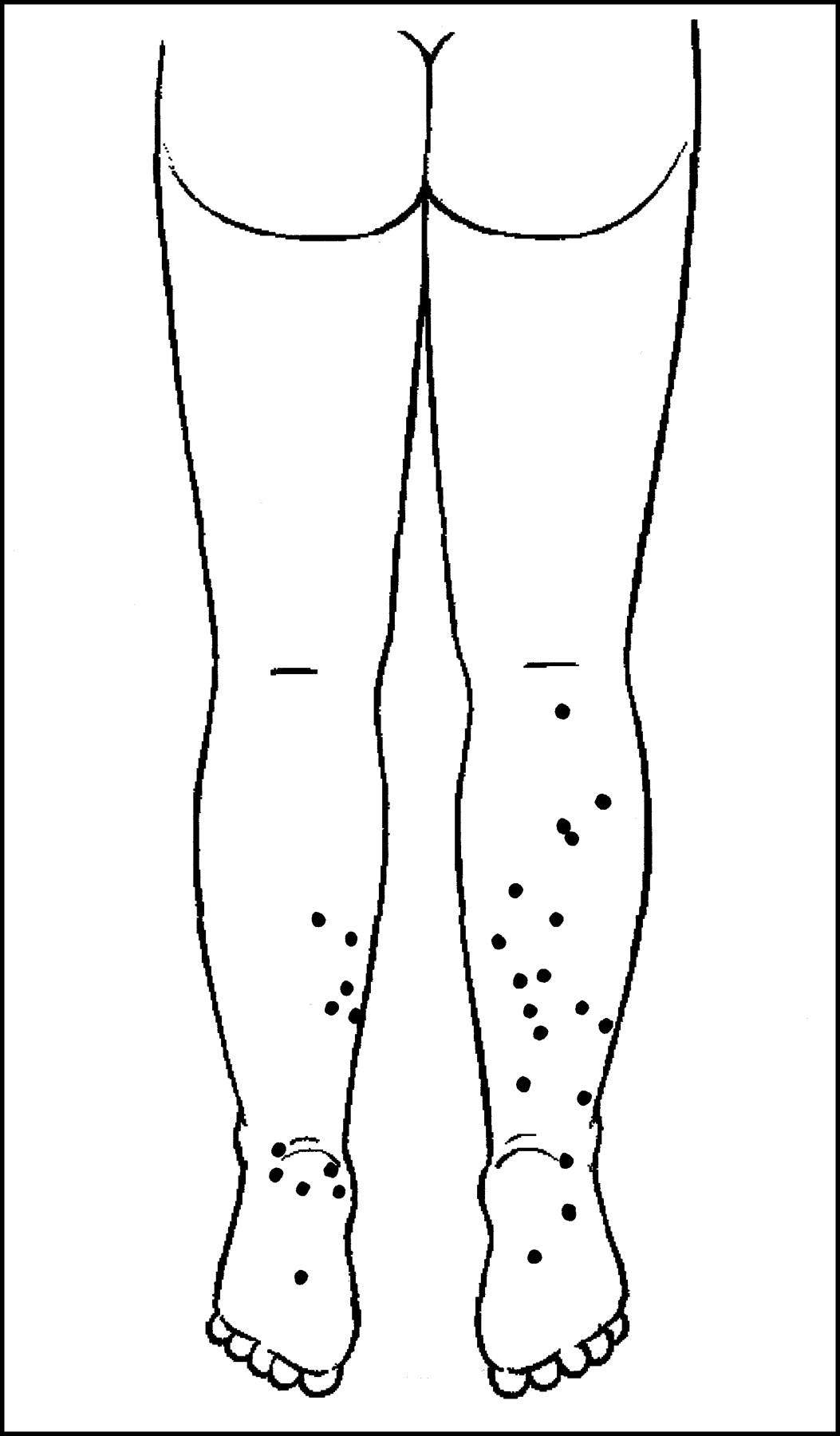
- FIGURE 21.
Locations of skin sites draining from posterior legs and feet to sentinel nodes in popliteal fossae.












Tables
Region Average flow (cm/min) Head and neck 1.5 Anterior trunk 2.8 Posterior trunk 3.9 Arm and shoulder 2.0 Forearm and hand 5.5 Thigh 4.2 Leg and foot 10.2 Melanoma site SN site n % Area Location Anterior trunk (n = 211) Above umbilicus (n = 199) Axilla Ipsilateral 180 90 Contralateral 31 16 Bilateral 30 16 Groin Ipsilateral 19 9 Contralateral 7 4 Bilateral 3 1.5 Cervical Level II 1 0.5 Level III 3 1.5 Level IV 3 1.5 Level V 6 3 Supraclavicular 27 14 Costal margin 6 3 Internal mammary 2 1 Interval node 17 8 Below umbilicus (n = 12) Axilla Ipsilateral 4 33 Contralateral 0 0 Groin Ipsilateral 12 100 Contralateral 2 16 Bilateral 3 25 Interval node 1 8 Posterior trunk (n = 1,057) Above waist (n = 965) Axilla Ipsilateral 875 91 Contralateral 292 30 Bilateral 264 27 Groin Ipsilateral 34 3 Contralateral 10 1 Bilateral 4 0.5 Triangular intermuscular space Ipsilateral 88 9 Contralateral 35 3 Bilateral 11 1 Cervical Level II 1 Level III 4 0.5 Level IV 15 1.5 Level V 108 11 Supraclavicular Ipsilateral 104 11 Contralateral 34 3 Bilateral 15 1.5 Postauricular 1 Occipital 4 0.5 Paravertebral or para-aortic 21 2 Retroperitoneal 8 1 Interval node 118 12 Below waist (n = 92) Axilla Ipsilateral 38 41 Contralateral 15 16 Bilateral 9 10 Groin Ipsilateral 71 77 Contralateral 24 26 Bilateral 21 23 Paravertebral or para-aortic 1 1 Retroperitoneal 1 1 Interval node 12 13 SN Site n (total, 508) % Area Location Parotid Ipsilateral 171 34 Contralateral 7 1 Ipsilateral cervical Level I 84 16 Level II 295 58 Level III 62 12 Level IV 47 9 Level V 97 19 Supraclavicular Ipsilateral 49 9 Contralateral cervical Level I 19 4 Level II 16 3 Level III 17 3 Level IV 9 2 Level V 16 3 Supraclavicular Contralateral 4 1 Occipital Ipsilateral 47 9 Contralateral 15 3 Postauricular Ipsilateral 83 16 Contralateral 5 1 Axillary Ipsilateral 7 1 Contralateral 2 0.3 Interval node 25 5 Melanoma site SN Site n % Upper limb (n = 571) Axilla 563 99 Epitrochlear 36 6 Cervical (Level V) 3 0.5 Supraclavicular 36 6 Triangular intermuscular space 3 0.5 Interpectoral 2 0.3 Infraclavicular 1 0.2 Interval node 23 4 Lower limb (n = 712) Groin 712 100 Popliteal 38 5 Interval 4 0.5
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Intramammary melanoma micrometastasis within a silicone-implanted breast
- Radioguided Surgery
- Lymphoedema of the upper limb: a rare complication of thyroid surgery?
- Lymphoscintigraphy and Sentinel Nodes
- Does the Preparation and Utilization of 99mTc-Sulfur Colloid Affect the Outcomes of Breast Lymphoscintigraphy?
- Management of Regional Lymph Node Basins in Melanoma
- Pearls and pitfalls of radionuclide imaging of the lymphatic system. Part 1: sentinel node lymphoscintigraphy in malignant melanoma
- Role of Nuclear Medicine in the Management of Cutaneous Malignant Melanoma
- The Impact of Lymphoscintigraphy Technique on the Outcome of Sentinel Node Biopsy in 1,313 Patients with Cutaneous Melanoma: An Italian Multicentric Study (SOLISM-IMI)
- Reconfirmation of Clinical Unpredictability of Lymphatic Drainage in Cutaneous Melanoma and New Developments in Sentinel Lymph Node Diagnostics