


Abstract
An observational multicentric Italian trial on sentinel node biopsy (SNB) in melanoma patients was performed to diffuse a common SNB protocol nationwide (Italy). We report herein the results of this trial. The influence of some technical aspects on the outcome of SNB was also investigated, because a certain degree of variability was accepted in performing lymphoscintigraphy. Methods: From January 2000 to December 2002, 1,313 consecutive patients with primary cutaneous melanoma (Breslow thickness, >1.0 mm or <1.0 mm but with ulceration, Clark level IV–V, presence of regression) were enrolled by 23 centers. One half to 1 mL of 99mTc-labeled human albumin colloid, at a suggested dosage of 5–15 or 30–70 MBq, was injected intradermally, closely around the scar, the same day or the day before SNB. Intraoperatively, Patent blue was associated when a definitive wide excision of the primary was required. A positive sentinel node (SN) was defined when containing melanoma cells detected by either hematoxylin–eosin or immunohistochemistry (S100 and HMB45 antibodies). All patients underwent regular follow-up. False-negative cases were considered when lymph node metastases occurred in the same lymphatic basin of SN biopsy (SNB) during follow-up. A quality control program has been performed for the surgical procedure and for the histologic diagnosis. Results: The SN identification rate was 99.3%. The axilla was the site of the SN in 52.5% of the cases. The mean number of SNs was 2.0 (range, 1–17) and only 1 node was removed in 45.4%. The positivity and false-negative rates were 16.9% and 14.7%, respectively (median follow-up, 31 mo). On multivariate analysis (logistic and linear regression) only the number of peritumor injections was inversely associated with the number of excised SNs (P = 0.002), whereas none of the technical variables showed an independent impact on SN status when Breslow thickness was included as a control variable. Conclusion: The number of peritumor injections seems to influence the outcome of lymphoscintigrapy in melanoma patients undergoing SNB. If these results are confirmed in a controlled trial, 3 injections at least should be recommended.
Development of the concept of sentinel lymph node (SN) and the association of the SN biopsy (SNB) technique represent a major breakthrough in the management of primary cutaneous melanoma. Since the milestone publication in 1992 by Morton et al. (1), who first applied SNB to melanoma patients, lymphatic mapping has evolved through refinement, clinical experience, and clinical trials, becoming an invaluable technique for identifying patients with subclinical lymph node metastasis (2,3). Surgeons can now identify patients who may benefit from a complete lymph node dissection and possible adjuvant therapy, while sparing patients with negative SN from the morbidity associated with these treatments. SNB is widely accepted as a powerful tool for disease staging, as supported by the evidence that SN status represents the most important single factor determining overall survival for patients with cutaneous melanoma at clinical stage I–II (2,3).
While biologic factors (e.g., Breslow thickness, mitotic rate, ulceration, and so on) predicting SN status have been extensively investigated (4,5), investigators have paid less attention to the impact of SNB technical variables on the SN identification rate and status (6).
In this article we present the results of an observational multicentric Italian trial on SNB, performed on behalf of the Italian Melanoma Intergroup (IMI), which enrolled >1,300 patients affected with primary cutaneous melanoma. This study was conducted with the main aim of diffusing the use of a common SNB protocol nationwide. As some aspects of the SNB technique were—and still are—not standardized worldwide, the protocol has left some room for variability in performing the procedure, such as the timing of lymphoscintigraphy, the number and site of the injections, and the radiotracer dose. This revealed a certain degree of technical heterogeneity among the participating centers, depending on institutional/personal preferences/beliefs, which allowed us to investigate the relative importance of such variability when affecting the outcome variables—that is, the rate of SN identification, the number of excised SNs and the SN status.
To validate the study results, a quality control program (QCP) was conducted for the surgical and the histopathologic procedures.
MATERIALS AND METHODS
Study Design
This was an observational study conducted by 23 Italian centers on behalf of the IMI. The coordinating centers (the University of Padova and the European Institute of Oncology of Milan) formulated a protocol containing the guidelines for patient enrollment, the SNB technique, and the SN pathologic evaluation.
All consecutive patients with lesions with a Breslow thickness of >1.0 mm or <1.0 mm with at least one of the following histopathologic features—ulceration, Clark level IV–V, presence of regression—were considered for lymphatic mapping and SN biopsy. Patients with clinical metastasis detected by palpation or ultrasound examination were excluded.
Patients
From January 2000 to December 2002, 1,313 patients with primary cutaneous melanoma were enrolled. Some variability in patient accrual (range, 7–268 patients) appeared across the clinical centers, with 10 centers enrolling >50 patients.
There were 666 males (50.7%) and 647 females (49.3%), with a median age of 52 y (range, 13–91 y). Tumor characteristics are reported in Table 1.
Baseline Tumor Characteristics
Lymphoscintigraphy and SNB Technique
Patients underwent preoperative lymphoscintigraphy with 99mTc-labeled human albumin colloid (Nanocoll; Amersham Health) either the same day or the day before SNB. In accordance with the lymphoscintigraphy time, a suggested dosage of 5–15 or 30–70 MBq, in a total volume of 0.5–1 mL, was injected intradermally in 1–4 sites closely around the scar of the excisional biopsy to identify the regional lymphatic basins draining that cutaneous region. The number of injections depended on the scar length or the primitive lesion sizes. In scars located on the head, usually 2 injections with a total lower volume (i.e., 0.4 mL) were suggested. Images were acquired immediately after the radiocolloid injection (dynamic phase) to investigate the drainage route, particularly for trunk lesions. When the first SN was clearly evident (15–30 min), a static image was taken using a 57Co flood source with the aim of outlining the body profile. This SN was marked on the skin using a dermographic pen. A delayed image acquisition was recommended to obtain all drainage basins and the total number of lymph nodes visualized. Early and delayed images were attached to the nuclear physician report to provide an easier surgical excision by the surgeon.
Intraoperatively, the SN was located by using a handheld γ-probe and the blue dye–based lymphatic mapping technique. After the induction of satisfactory anesthesia (local or general), Patent blue dye was intradermally injected around the excision biopsy site, and the area was massaged to promote lymphatic flow. When the primary lesion was located on the face or neck areas, vital dye was generally avoided if a wider excision was not indicated. After approximately 5–10 min, a handheld γ-probe was used to identify the hot spots over the SN. A small incision was made directly over the hot spots and carried down through the skin and subcutaneous tissue into the node-bearing fat. Any blue-stained or hot node (defined as the hottest node), and any other node with at least 5-fold the background radioactivity, were excised and sent for pathologic analysis. Definitive wide excision of the primary cutaneous melanoma was performed, if required, after the SNB procedure.
SN Pathologic Evaluation
SNs were evaluated according to the protocol suggested by a panel of pathologists skilled in melanoma and SN evaluation. SNs were cut along their longitudinal axis in 2- to 3-mm-thick slices and embedded in paraffin blocks. At least 10 serial sections were obtained from each block and examined by conventional hematoxylin–eosin staining (sections 1, 3, 5, 7) and by immunohistochemistry using both S100 (sections 2, 4, 8) and HMB45 antibodies. Sections 9 and 10 were available for additional staining. A positive SN was defined as a lymph node containing melanoma cells detected by either hematoxylin–eosin or immunohistochemistry.
Micrometastases were defined as tumor deposit of ≤2 mm.
False-Negative Cases
Those patients with negative SNB who experienced lymph node metastasis in the same lymphatic basin(s) during the follow-up period were considered false-negative cases. The false-negative rate was calculated as the number of false-negative cases over the sum of the true-positive plus the false-negative cases.
Patients with signs of distant or in-transit metastases without lymph node relapse were not considered as false-negative.
Quality Control Program
A QCP on the SNB surgical procedure was performed by means of site visits performed during the study period. The QCP was organized in 2 steps: during the first phase, the 3 centers with the highest accrual audited the 3 centers with the second highest accrual and vice versa. During the second phase, the remaining centers with the lowest accrual were assigned to 1 of the 6 centers for an audit visit. All site visits occurred during a SNB procedure performed on a patient enrolled in the study. At the end of the visit, the surgeon in charge of the audit compiled a structured questionnaire regarding the procedure and assigned an overall judgment.
With regard to the pathologic evaluation of SN, the data center (Clinical Trials and Biostatisitical Unit, Università di Padova [IOV-Padova]) randomly selected 5 patients for each participating center, 1 SN positive and 4 negative, at the end of the study. The histologic samples were submitted to a panel of pathologists who reviewed them with no knowledge of findings. The panel included 5 pathologists involved in the study and 1 external reviewer.
For each case, the procedural quality was assessed, scoring the hematoxylin–eosin sections, the immunohistochemistry sections, and the number of sections, according to a prespecified scale. Finally, a diagnosis about the SN status was issued for each case.
Statistical Analysis
All data were collected and analyzed by the same data center (Clinical Trials and Biostatisitics Unit, IOV-Padova). To verify the association between the number of lymphoscintigraphy-detected and excised SNs the Kendall test was used.
To evaluate any univariate association between the number of SNs removed, or the SN status, and each of the characteristics of the lymphatic mapping, the ANOVA and the χ2 test were used whenever appropriate.
A logistic regression model, with a stepwise selection procedure, was used to examine the joint effect of the technical variables on SN metastasis.
A multiple linear regression model was used to evaluate the independent association between the technical covariates and the number of excised nodes. The variables considered for the analysis were the maximal length of primary tumor excisional biopsy, number of radiotracer injections, volume of radiotracer injected, dose of radiotracer, and center's case load.
Statistical significance was determined using an α-level of 0.05 and 2-sided tests. Microsoft Access database software (Microsoft Corp.) and SAS statistical software (SAS Institute Inc.) were used for the compilation of data and statistical analysis, respectively.
RESULTS
SN Identification
No lymphatic basin was identified in 8 patients and in 1 the biopsy was not performed because the radiotracer indicated activity in the parotid region: therefore, the overall SN identification was 99.3% (1,304/1,313). As shown in Table 2, in the majority of the 1,304 patients only 1 lymphatic basin was identified (1,121 patients, 85.9%).
Description of Lymphatic Basin Identified and Status of SN
The mean number of identified SNs on lymphoscintigraphy per patient was 1.77 (range, 1–7) and the mean number of biopsied SNs per patient was 2.0 (range, 1–17). There was a significant correlation between the number of lymphoscintigraphy-detected and the excised SNs (Kendall τ-b = 0.57059; P < 0.0001).
Only 1 SN was removed in 591 patients (45.4%). The axilla was the site of the SN in 52% of the cases, followed by the groin (37.6%).
SN Status
SN positivity rate was 16.9% (220 of 1,304 patients), most patients having only 1 positive SN (80.4%). The positivity rate per basin (axilla, 13.9%; groin, 18.1%; laterocervical, 12.5%; other sites, 6.8%) and for primary site (head and neck, 15.47%; trunk, 16.36%; superior limbs, 14.46%; inferior limbs, 18%) was not significantly different.
Micrometastases were present in 84 of the 220 patients with positive nodes (38.2%).
Lymphoscintigraphy Variables
The variability of the lymposcintigraghic aspects of the SNB procedure is illustrated in Table 3. One or 2 radiotracer injections were performed in 697 patients and 3 or 4 in the remaining 587. An injected total volume of 0.5 mL was used the most frequently. There was some variability in the radiotracer dose used, mainly because of the different time intervals between the lymphoscintigraphy and the surgical procedure.
Distribution of Technical Variables of LS
At univariate analysis (Table 4), a lower number of radiotracer injections, as well as its lower volume, were inversely associated with the number of excised SNs (P < 0.0001 and P = 0.002, respectively). At multivariate analysis, only the number of radiotracer injections was retained in the model (P < 0.0001). Similar results were obtained for the number of SNs detected through lymphoscintigraphy. In details, the mean number of LS-detected SNs was 1.9 when <3 injections were used and was 1.6 when ≥3 were performed (P = 0.002); as for the total volume of radiotracer, the mean number of LS-detected SNs was 1.8 when <0.5 mL of the total injected volume was used and was1.7 when ≥0.5 mL was injected (P = 0.047).
Association Between Technical Variables and SN Mean Number
As for the SN status, fewer radiotracer injections were significantly associated, on univariate analysis (Table 5), with a lower percentage of positive patients (P = 0.021). However, on multivariate analysis, none of the technical variables showed an independent impact on SN status when Breslow thickness was included as a control variable.
Association Between Technical Variables and SN Status
Follow-up
With a median follow-up of 31 mo there were 38 false-negative cases (false-negative rate, 14.7%; 95% confidence interval [CI], 10.4%–19.1%).
The false-negative rate did not differ among centers with large and small case loads. In the 172 patients enrolled across the centers with a case load of ≤50, there were 7 false-negative cases (12.7%; 95% CI, 3.9%–21.5%), whereas in the 837 patients enrolled in the centers with the major case load, there were 31 false-negative cases (15.3%; 95% CI, 10.3%–20.2%).
No technical variable was correlated with the occurrence of disease relapse in the same lymphatic basin(s) during observation.
Quality Control Program
With reference to surgery, the site visit was performed in 20 clinical centers. In the remaining 3 centers the visit was not performed because of logistic problems. The overall judgment was generally positive, as shown in Table 6, with only 1 center ranking “sufficient” because of insufficient staging procedures performed on the patient before the SNB took place.
Surgical Control Program
With regard to pathology, 17 clinical centers participated in the QCP. The overall score of the procedural quality is reported in Table 7. Quality was ranked “good” in 12 and “medium” in 5 of 17 centers.
Pathologic Control Program
Overall diagnostic accuracy was 98.8% (81/82 cases), with only one major disagreement documented: one patient, initially diagnosed as negative, was later found to be positive on reevaluation. Furthermore, other minor disagreements were found in the classification of the type of metastases.
DISCUSSION
Prophylactic radical lymph node dissection does not improve the survival of patients with cutaneous melanoma and is aggravated by relatively high morbidity rates (3). Over the past decade, SNB has gained an overwhelming consensus, rapidly becoming a model of minimally invasive oncologic surgery. At the present time, SNB is considered the standard procedure for staging patients with cutaneous melanoma as it provides clinicians with a powerful prognostic tool characterized by a low morbidity rate (7). However, there is no definitive evidence of survival advantage for patients undergoing SNB (8), either because elective lymph node dissection indicated by SN positivity does not improve the clinical outcome or because of the lack of effective adjuvant therapies. Therefore, SNB should still be performed as an investigational diagnostic/prognostic procedure (9).
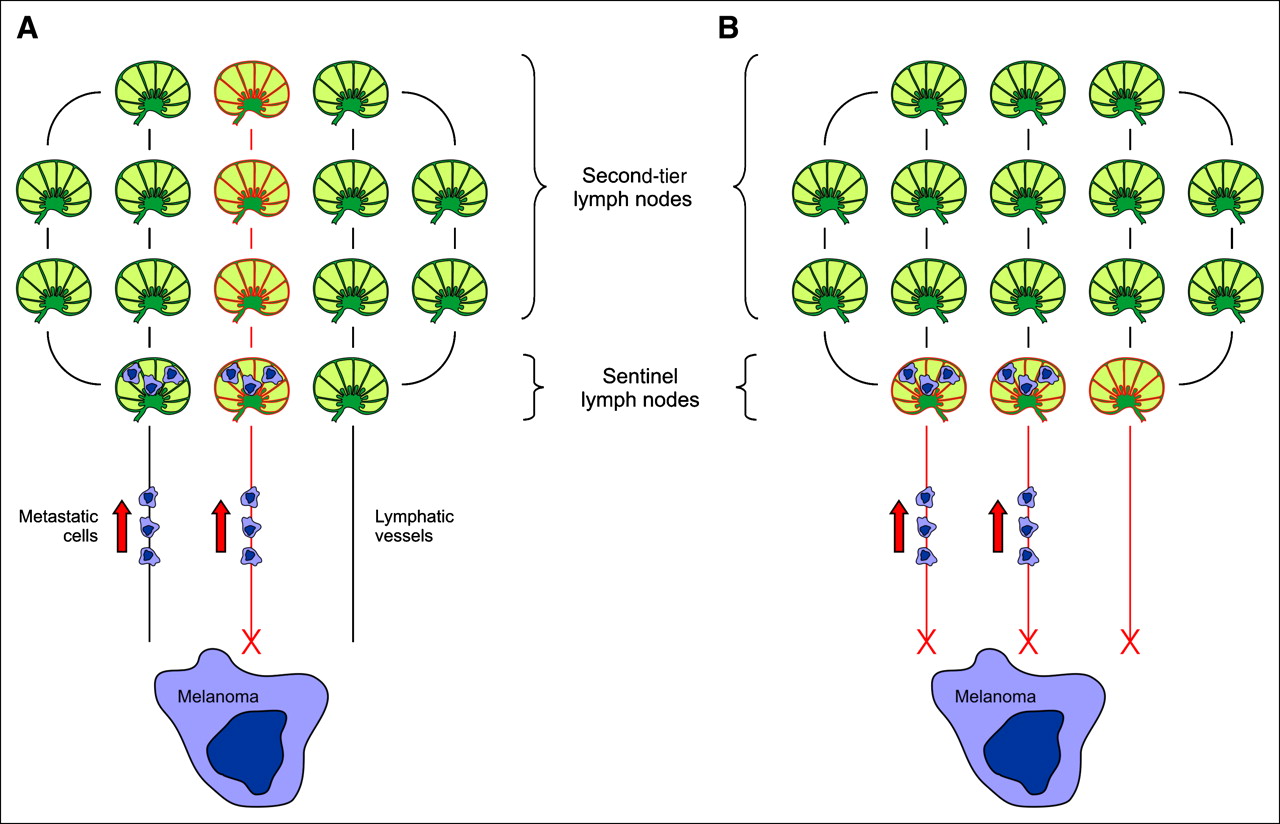
According to the original definition by Morton et al., the SN is the lymph node that receives direct drainage from the primary lesion (1). Therefore, after diagnostic biopsy, lymphoscintigraphy is performed in most patients with cutaneous melanoma to identify the SN and differentiate it from nonsentinel nodes of the same lymphatic basin (i.e., second- or third-tier lymph nodes; Figure 1) (10). In the 1990s, the IMI formulated a protocol on SNB and gathered together 23 Italian clinical centers to perform an observational prospective study with the main aim of spreading a common protocol nationwide. The surgical guidelines (including lymphatic mapping with blue dye) for SNB and the histologic examination were quite stringent, as they were taken primarily from Morton's experience (1). By contrast, a certain degree of variability in the lymphoscintigraphy technique (e.g., the number and site of radiotracer injections and the radiotracer dose/concentration) was considered acceptable, as reported in a survey performed among European centers performing the SNB procedure (11). At that time, the level of reproducibility of lymphoscintigraphy was approximately 85% and the procedure was already considered the gold-standard to detect the SN in melanoma patients, whereas the additional use of blue dye was suggested whenever difficulties in identifying the SN were anticipated by lymphoscintigraphy (11–13). We have therefore considered blue mapping as a complementary procedure and did not further investigate its impact on the outcome of SNB.
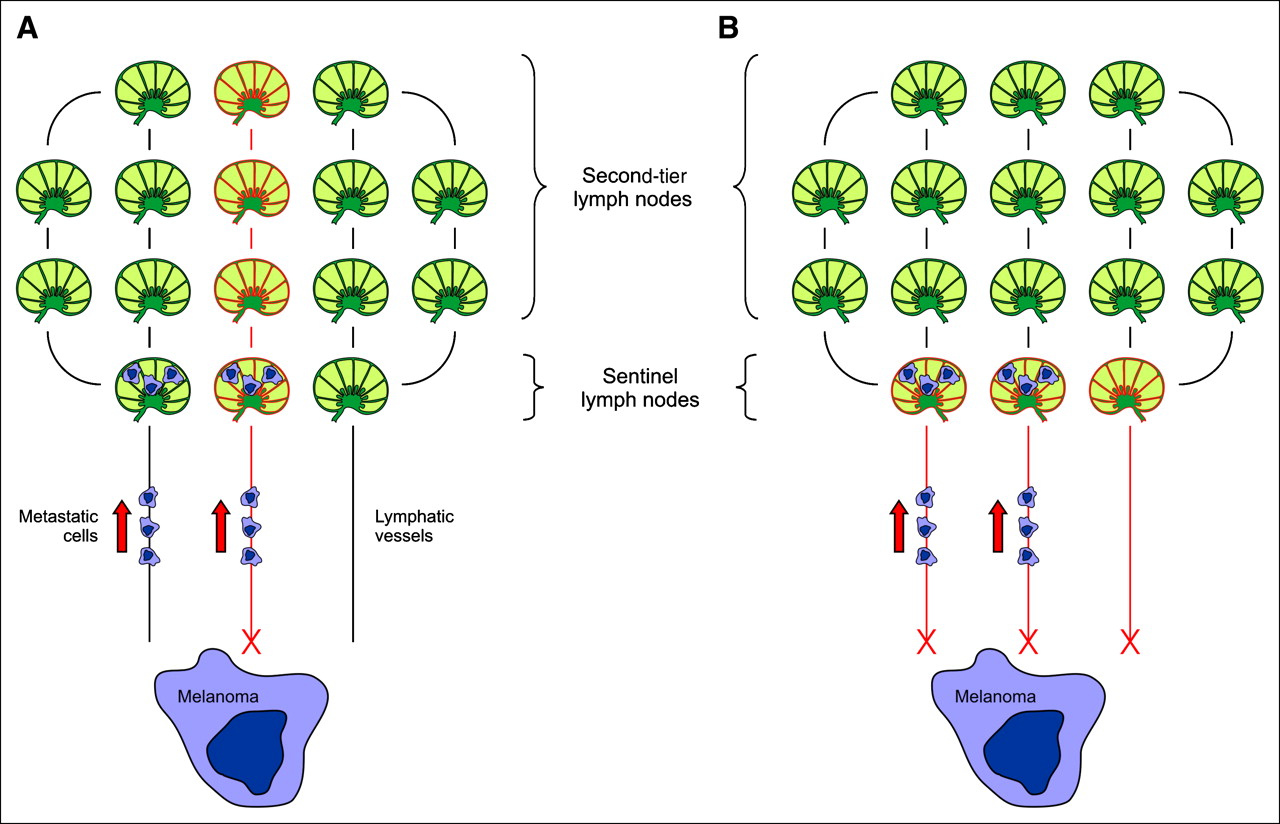
Lymphoscintigraphy for detection of SNs in patients with cutaneous melanoma. Schematic view of how the different number of radiotracer injections might affect the outcome of the procedure. (A) Single injection, X (large volume), might only enter central lymphatic vessels (with respect to the scar following primary melanoma resection), thus missing those potentially involved by malignant cells; moreover, the large volume of the radiotracer might be responsible for identification of non-SNs. (B) Multiple injections, X, might instead enter peripheral lymphatic vessels and thus identify sentinel nodes involved by metastatic melanoma cells; in addition, the low volume characterizing multiple injections might avoid identification of second tier(s). Arrows represent lymphatic flow.
The data collected were validated by a QCP, performed by means of site visits at the participating centers for the control of the SNB procedure and by a pathologic review of a random selection of SN samples. To our knowledge, this is the first example of a systematic quality control process for SNB, which we considered to be an essential part of the study, as there were no selection criteria to include a center, apart from the declaration according to which a learning phase had been completed (at least 30 SNBs in melanoma patients) (14) before entering patients in the study, and a commitment statement certifying that the protocol would be prospectively followed for all consecutive patients. The outcome of this QCP was satisfactory as 19 of 20 visited centers achieved a high score with regard to application of the procedure, both for preoperative lymphoscintigraphy and for intraoperative lymphatic mapping, and surgical technique. Moreover, a very high degree of accuracy was registered for the pathologic diagnosis (presence or absence of metastases in the SN). As a matter of fact, the panel's diagnosis was concordant in 82 of 83 reviewed specimens, and some negative notes were registered only in a few cases because of the low number of sections examined or the low quality of immunohistochemistry.
The results achieved in our study with regard to the SNB procedure (identification, positivity, and false-negative rate of 99.3%, 16.9%, and 14.7%, respectively) are comparable with those reported in literature (15–21), thus confirming the validity of this technique. Interestingly, we observed that the case load did not affect the outcome of the surgical procedure, as there was no significant difference in SN detection, positivity, and false-negative rates among the participating centers enrolling <50 or >50 consecutive patients.
Overall, these findings support the idea that SNB can be reliably performed once an adequate learning phase has been completed. Nevertheless, there is still room for improving this technique. Although increasing the SN identification rate (presently ranging between 98% and 99%) is rather unlikely, it seems more reasonable to focus on the possibility of lowering the false-negative rate (calculated as the number of false-negative cases over the sum of true-positive and false-negative cases), which ranges from 13% to 18% in the largest series reported so far (9,15,18), by modifying some technical details. For instance, some investigators have recently demonstrated that the use of carbon dye for lymphatic mapping and a more accurate protocol of SN pathologic or polymerase chain reaction–based examinations can identify SN metastasis with higher accuracy (22–24). Improving the reproducibility of lymphoscintigraphy might also be useful for this purpose (11–13,17). The high number of patients enrolled in our study and the variability in performing lymphoscintigraphy prompted us to investigate whether any technical detail might have an influence on this issue. By considering the most common parameters that might affect the results of lymphoscintigraphy, we found that only the number of radiotracer injections significantly affects the selectivity (i.e., the number of SNs removed) and the sensitivity of this procedure. In fact, when >3 radiotracer injections were used, a lower number of SNs was found (1.7 vs. 2.2; P < 0.0001), whereas the proportion of positive nodes was higher (19.2% vs. 14.1%; P = 0.021), although it was not retained in the multivariate analysis, when the tumor thickness variable was included in the model.
Furthermore, in our experience, the different positivity rate observed in the 2 study groups (higher vs. lower radiotracer injection number) did not translate into a significant difference in the false negativity rate. However, given the low number of false-negative cases in our series, a longer follow-up is warranted to verify this finding.
A hypothetic explanation for the correlation between radiotracer injection number and SNB outcome could be the microanatomy and physiology of cutaneous lymphatic vessels. Initial lymphatic capillaries are formed by overlapping endothelial cells with an incomplete basement membrane and do not have a complete muscle layer. The flow through these vessels can be markedly enhanced by increasing the interstitial pressure (e.g., through massage) (25,26). According to this hypothesis, an increased interstitial pressure can favor the entry of the radiotracer into the lymphatics and eventually the corresponding lymph nodes (10). For the same reason, the intradermal injection of relatively large volumes of radiotracer (using a low number of injections—that is, <3) might increase the interstitial pressure and, consequently, the amount of radiocolloid into each lymphatic vessel (Fig. 1A): this would increase the number of lymph nodes reached by the radiotracer (second-tier lymph nodes) and, ultimately, the number of excised SNs. Moreover, a few injections might not be enough to enter all the lymphatic capillaries draining a given skin area and, therefore, to visualize an adequate number of SNs (12,13,27). By contrast, smaller radiotracer volumes, such as those achieved with a higher number of injections, might lead to visualization and excision of fewer second-tier lymph nodes (Fig. 1B). In addition, the greater distribution of the injections along the scar might account for the visualization of peripheral lymphatic vessels used by metastatic cells to reach the draining lymphatic basin, thus accounting for the higher number of positive SNs detected and excised.
CONCLUSION
Taken together, our findings suggest that the number of radiotracer injections may influence the outcome of SNB independently from the dose of radiocolloid, which is hypothetically linked to the effect of the radiotracer volume on the flow kinetics of the lymphatic vessels. If these results are confirmed in a controlled trial, 3 radiotracer injections might become the lower limit recommended for lymphoscintigraphy protocols to increase the reliability of the SNB procedure.
APPENDIX
A full list of group participants and institutions is given here.
Data Center
-
P. Del Bianco (statistician), D. Kilmartin (data manager), P. Lunardi (data manager), Clinical Trials & Biostatistic Unit—Istituto Oncologico Veneto, Padova, Italy
Pathology Panel
-
D. Brancorsini, Torrette General Hospital, Ancona, Italy
-
L. Macrì, Dipartimento di Scienze Biomediche Università di Torino, Torino, Italy
-
M.C. Montesco, University General Hospital of Padova, Padova, Italy
-
L. Riccioni, Bufalini General Hospital, Cesena, Italy
-
G. Mazzarol, Istituto Europeo Di Oncologia, Milano, Italy
-
C. Clemente, Casa Di Cura S. Pio X, Milano, Italy
Participating Centers
-
L. Morresi (dermatologist), Sestilli Hospital, Ancona, Italy
-
D. Dioguardi (plastic surgeon), University General Hospital, Bari, Italy
-
L. Barutta (surgeon), Ospedale S. Martino, Belluno, Italy
-
A. Zaccagna (dermatologist), IRCC–Istituto Ricerca e Cura Cancro, Candiolo, Italy
-
A. Savani (plastic surgeon), A. Batacchi (surgeon), M. Germanò (surgeon), Sant' Anna Hospital, Como, Italy
-
M. Landra (surgeon), Santa Croce General Hospital, Cuneo, Italy
-
G. Soliani (surgeon), Surgery Clinical Institute, Ferrara, Italy
-
G. Verdecchia (surgeon), A. Ascari (dermatologist), GB Morgagni Pierantoni Hospital, Forlì, Italy
-
G. Fabrizio (surgeon), G. Vetri General Hospital, Larino, Italy
-
M. Simonacci (dermatologist), M. Sigona (dermatologist), General Hospital, Macerata, Italy
-
G.L. Lazzaro (surgeon), Istituto Europeo Di Oncologia, Milano, Italy
-
P. Pecoraro (surgeon), F. Costanzo (surgeon), General Hospital, Montebelluna, Italy
-
L. Nespoli (dermatologist), San Gerardo General Hospital, Monza, Italy
-
A. Vecchiato (surgeon), University General Hospital, Padova, Italy
-
M. Anzà (surgeon), Regina Elena General Hospital, Roma, Italy
-
L. Cozzaglio (surgeon), Humanitas Clinical Institute, Rozzano, Italy
-
S. Pau (surgeon), S. Lazzaro Molinette Hospital, Torino, Italy
-
P. Cristofolini (surgeon), Santa Chiara Hospital, Trento, Italy
-
G. Siciliano (plastic surgeon), Santa Maria della Misericordia General Hospital, Udine, Italy
-
M. Governa (surgeon), General Hospital, Verona, Italy
-
G. Sandri (plastic surgeon), General Hospital, Vicenza, Italy
-
A. Bianco (medical oncologist), P. Mainente (surgeon), General Hospital. Vittorio Veneto, Italy
Acknowledgments
The authors thank Dr. Paola Lunardi for extensive study data management, Dr. Claudio Clemente for his helpful contribution to the pathologic QCP, and Pierantonio Gallo for the artwork.
References
- Received for publication July 6, 2005.
- Accepted for publication September 27, 2005.





{kind=link}
Jump to section
Related Articles
Cited By...
- Accuracy and Reproducibility of Lymphoscintigraphy for Sentinel Node Detection in Patients with Cutaneous Melanoma
- Optimal Detection of Sentinel Lymph Node Metastases by Intraoperative Radioactive Threshold and Molecular Analysis in Patients with Melanoma
- Optimal 57Co Flood Source Activity and Acquisition Time for Lymphoscintigraphy Localization Images
- The Role of Interval Nodes in Sentinel Lymph Node Mapping and Dissection for Melanoma Patients
- Sentinel Lymph Node Biopsy in Melanoma