


Abstract
Radioiodine remnant ablation (RRA) is frequently used after a thyroidectomy for differentiated thyroid carcinoma because it has been reported to reduce the number of local recurrences and to increase overall survival. Although the traditional method of preparation for RRA is thyroid hormone withdrawal, several physicians at our medical center have offered the option of having RRA after preparation by recombinant human thyroid-stimulating hormone (thyrotropin; TSH) over the past 2 y. During this same time period, other patients at our center were prepared for RRA by hormone withdrawal. Methods: We took this opportunity to retrospectively review the rate of complete remnant ablation in patients having RRA after hormone withdrawal compared with those having RRA after recombinant human TSH. Only patients who had RRA after January 1, 1999, and follow-up diagnostic studies at our medical center, were included in the analysis. A successful ablation was defined as no visible radioiodine uptake on the follow-up diagnostic scans, performed with 185 MBq (5 mCi) 131I. The 2 groups had comparable patient and tumor characteristics and received similar ablative activities of 131I. Results: We found that 84% of those prepared by recombinant human TSH, and 81% of those prepared by hormone withdrawal, had complete resolution of visible thyroid bed uptake after RRA (P = not significant). Conclusion: Given the biases that exist in retrospective studies, we cannot yet recommend RRA preparation by recombinant human TSH for routine use. However, these preliminary findings are favorable enough to support the design of a prospective randomized trial comparing RRA success rates after preparation by either thyroid hormone withdrawal or recombinant human TSH.
Radioiodine remnant ablation (RRA) is a procedure primarily intended to destroy normal thyroid remnants after a near-total or total thyroidectomy for differentiated thyroid carcinoma (1,2). When doses of 300 Gy can be delivered to the thyroid remnant, successful ablation rates as high as 84% have been reported (3–9). Although there are debates over the most appropriate use of this procedure, it has been reported to reduce the frequency of locoregional recurrences and to reduce overall mortality in patients with large primary tumors (10–12). This antitumor effect has been postulated to be due to destruction of microscopic deposits of thyroid carcinoma. The destruction of all normal thyroid cells increases the sensitivity of the serum thyroglobulin (Tg) level at detecting thyroid cancer recurrences (13) and allows the achievement of a totally negative diagnostic whole-body radioiodine scan (DxWBS). However, not all investigators agree on the value of RRA because its use has not been based on prospective randomized trials (14).
All published studies on RRA, to date, have been based on treatments after thyroid hormone withdrawal (THW). Furthermore, they are generally based on the assumptions that (a) radiation doses of 300 Gy are necessary to ablate normal thyroid tissue and that (b) an elevated thyroid-stimulating hormone (thyrotropin; TSH) level will stimulate 131I uptake and retention in the thyroid (15).
Diagnostic studies using recombinant human thyrotropin (rhTSH) for surveillance of thyroid cancer patients have found this method of preparation to be as sensitive and specific as those studies done after THW (16–18). It has been proposed that rhTSH stimulates iodine uptake via activation of the sodium-iodide symporter. If this is correct, rhTSH has the potential to assist in treatment paradigms in which increased sodium-iodide symporter activity is also necessary. We reported previously that exogenous rhTSH could stimulate sufficient 131I uptake in thyroid remnants to result in complete remnant ablation, while the patients remained on l-thyroxine suppression (19). In the first 10 patients treated in this manner at our medical center, complete ablation of thyroid bed uptake was achieved in all.
Beginning in January 1999, some clinicians at our medical center offered thyroid remnant ablation after preparation by rhTSH while patients were on thyroid hormone suppression. Other clinicians continued to prepare patients for remnant ablation by withdrawal of thyroid hormone. All thyroid remnant ablations, regardless of method of preparation, were done by the same nuclear medicine group following a standard protocol, which includes formal radioiodine dosimetry. We have taken this unique opportunity to retrospectively review these 2 practice patterns and examine the rates of successful remnant ablation between them. Because rhTSH preparation was shown to be comparable with THW for diagnostic studies, we hypothesized that RRA success rates would be indistinguishable between patients who were prepared by THW or by rhTSH. Because this was not a prospective research study, no written informed consent was obtained, no fixed amounts of radioiodine were used, no specific follow-up intervals were prescribed, and there was no prospective data collection.
MATERIALS AND METHODS
Subjects
This is a retrospective review of 87 patients who underwent RRA at our medical center between January 1999 and December 2000. These patients were cared for by 12 attending physicians who made decisions concerning diagnostic studies and therapeutic interventions based on what they and the patients agreed would be the optimal care. Patients had total or near-total thyroidectomy performed by a variety of surgeons, although most had surgery at our hospital. These patients and their physicians agreed to proceed with RRA. There was no prospective research design or data collection. Patients were informed by their attending physicians that the traditional RRA method involved THW preparation to raise endogenous TSH levels and that the euthyroid rhTSH preparation was an “ off-label” approach, as the U.S. Food and Drug Administration has approved rhTSH (Thyrogen; Genzyme Corp., Cambridge, MA) only for use in diagnostic studies. Some patients who had a failed RRA had a second RRA during this time interval. We considered only the initial RRA for any patients who had >1 evaluation during the 2-y period. Evaluable patients were those who had both RRA and follow-up whole-body radioiodine scans at our medical center by the time of the preparation of the manuscript (December 2001). On the basis of these inclusion and exclusion criteria, we identified 42 evaluable patients who had RRA after THW (group 1) and 45 evaluable patients who had RRA after rhTSH preparation (group 2).
Nuclear Medicine Studies
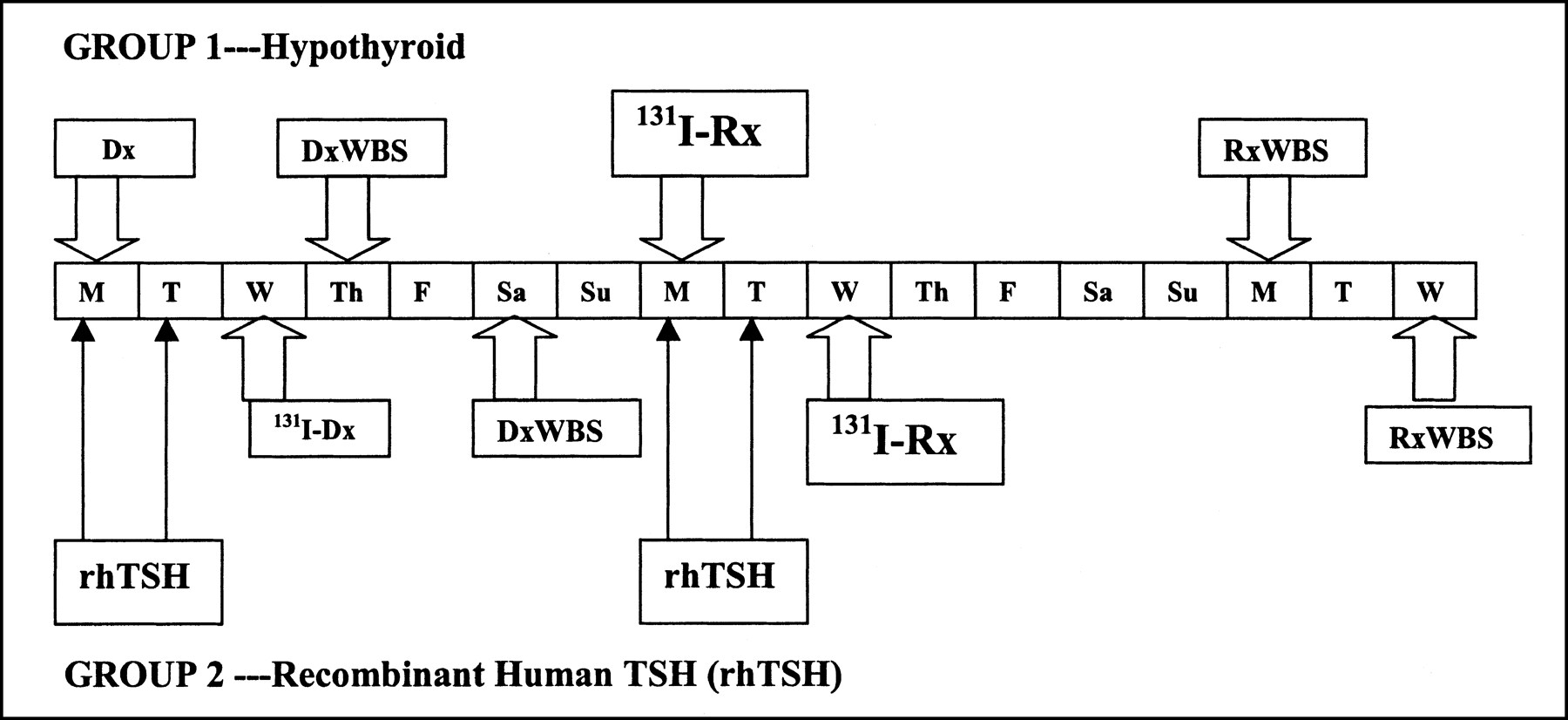
At our medical center, RRA has 2 distinct parts: first, a 1-wk diagnostic study (dosimetry) using a 37- to 185-MBq (1–5 mCi) test dose of 131I and, then, the actual therapeutic dose of 131I (Fig. 1). The diagnostic study includes neck and whole-body scanning and neck uptake measurements to determine the extent of functioning thyroid tissue and blood and whole-body clearance measurements to determine the patient’s MTA for the subsequent RRA. The MTA is the maximum activity that can be given without potential adverse effects to the marrow, or to the lungs if there is diffuse lung disease, and can vary widely between individuals (20, 21).
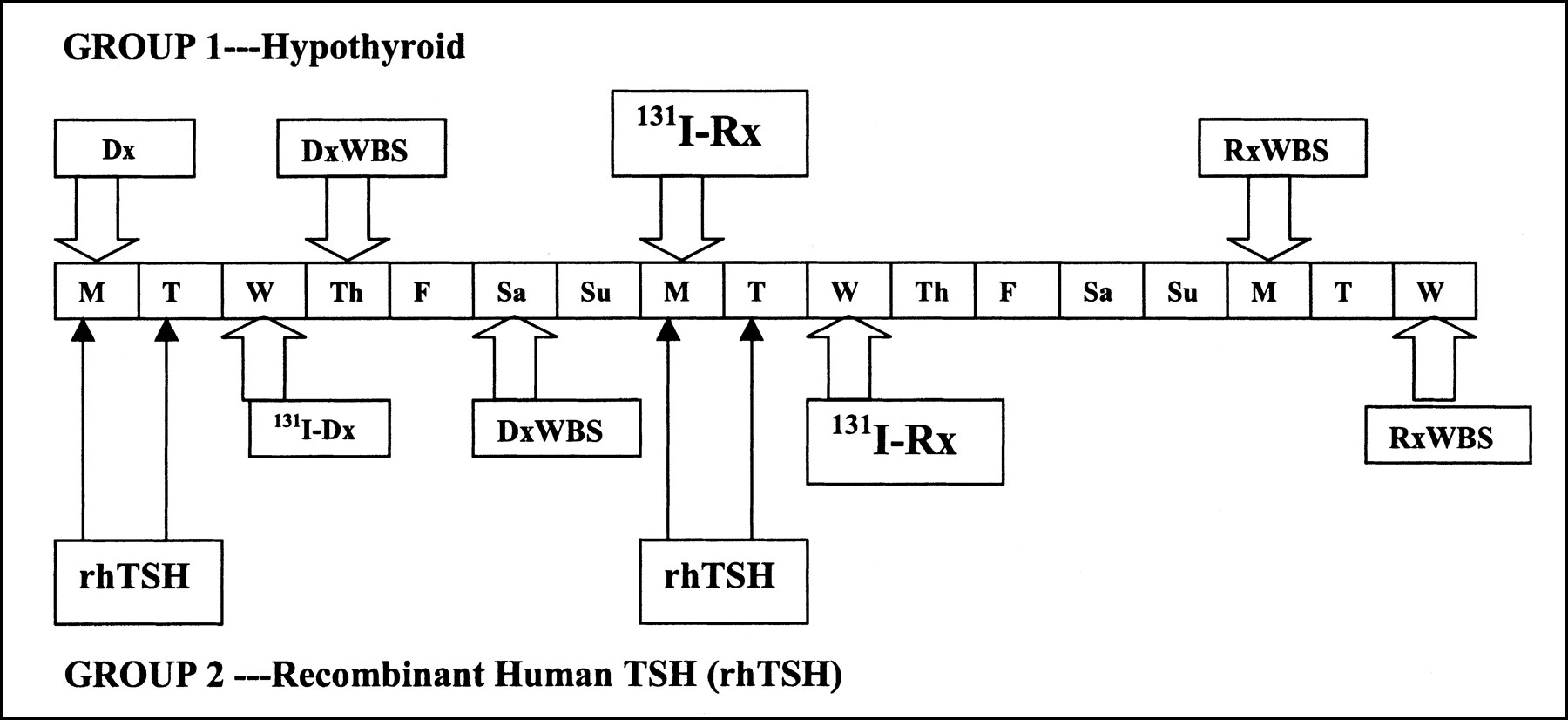
Overview of diagnostic (Dx) and therapy time schedules. 131I-Dx, diagnostic radioiodine administration; 131I-Rx, therapeutic administration of 131I; RxWBS, whole-body scan after therapy. Letters in horizontal row of boxes indicate days of week.
Patient Preparation
Patients in group 1 (THW) were not placed on thyroxine after thyroidectomy. Some individuals were placed on triiodothyronine for 2–4 wk and then withdrawn for 2 wk before the diagnostic study. Their stimulated TSH and Tg levels were drawn on the day that the test dose of radioiodine was administered (day 1). Patients in group 2 (rhTSH) were placed on l-thyroxine within 1 wk of surgery. Thyroxine daily doses varied between 100 and 225 μg l-thyroxine. Group 2 patients received 0.9 mg rhTSH intramuscularly on day 1 and day 2. On day 3, they received the diagnostic dose of 131I. All patients were provided with information on low-iodine diets and encouraged to adhere to them carefully. Women of childbearing age were documented to have a negative pregnancy test before the testing. The dose of 131I was given orally after overnight fasting.
Imaging, Neck Uptake, and Whole-Body Counting
Imaging was performed using a Genesys dual-head gamma camera (ADAC Laboratories, Milpitas, CA) and a high-energy, general-purpose collimator. Anterior, posterior, and lateral images of the neck were obtained at 24 and 72 h. Typically, 10-min neck views were obtained with a 256 × 256 × 16 matrix and a 38-cm2 field of view, with a 20% width energy window centered at 364 keV. Anterior and posterior whole-body scans were obtained at 72 h with the patient supine using a 256 × 256 × 16 matrix and an 8-cm/min scanning motion, with the gamma-camera heads slowly scanning the 2 heads over the patient’s body from the top of the head to just below the soles of the feet.
Neck uptake was measured at 24, 48, and 72 h using a thyroid probe containing a 5.1-cm-diameter (2 in) sodium iodide crystal and fitted with an extended-length, flat-field collimator. Just before counting, the patient was asked to empty the urinary bladder. Counts were obtained with the patient seated, neck extended, and the collimator positioned over the thyroid bed, so as to just brush the skin. Counts of the midthigh were also obtained as a surrogate for neck background. A thyroid standard and room background were also counted. The percentage of uptake in the neck was calculated from the formula: percentage uptake = 100([net neck counts/37 kBq (μCi) administered])/([net standard counts]/37 kBq (μCi) in the standard]).
As part of the MTA determination (20), heparinized whole-blood samples were obtained at 4, 24, 72, and 96 h for group 1 and at 4, 24, 48, and 72 h for group 2. Aliquots were counted in an automated scintillation well counter to determine activity concentration. These data were used to determine the locally deposited β -particle dose to blood.
The γ-ray component of dose to blood was determined from whole-body retention measurements taken at similar time points, with the addition of 2 early points at 5 min and 2 h. Whole-body counts were obtained using a 12.7-cm-diameter (5 in) sodium iodide detector (energy window, 314–414 keV) with the patient sitting at a fixed distance from the detector, about 3 m, on a small rotating stool. To reduce the effects of changes in geometry of distribution of radioactivity within the patient, at each time point, anterior and posterior counts were taken and averaged arithmetically. The initial measurements with 100% of the administered dose present allowed the patient to act as his or her own calibration in terms of counting efficiency, attenuation, and scatter. A 131I standard was counted at each time point just to monitor consistency of the detector performance.
MTA Calculation
The MTA, the administered activity that would deliver 2 Gy to blood (or result in 2.96 GBq [80 mCi] retained at 48 h if there was diffuse lung disease), was calculated as described (20,21). No patients received the full MTA. The principal reason for determining the individual MTA for RRA is to prevent overtreatment of patients who have unusually low MTA (i.e., 3.7 GBq [<100 mCi]). The MTA does not define the final activity to be administered but only serves as 1 factor that is considered when the final activity is chosen.
Treatment
The activity of 131I chosen for ablation was based on recommendations of a thyroid cancer tumor board, consisting of adult and pediatric endocrinologists, nuclear medicine physicians, thyroid surgeons, and oncologists. The results of the dosimetric analysis (MTA) were available before the choice of the therapeutic dose for each patient. The final activity administered was based on all available clinical data. Patients in group 1 who had any thyroid bed activity and wanted to proceed with RRA then received the therapeutic dose of 131I on day 8, still hypothyroid, after THW. Patients in group 2 who had any thyroid bed activity and wanted to proceed with RRA received 0.9 mg rhTSH on days 8 and 9 and the therapeutic 131I on day 10. A whole-body scan after therapy was then obtained 1 wk after the therapeutic activity was given. Evaluable patients were those that remained on thyroxine suppression after RRA and had their first follow-up DxWBS at our medical center according to the methods described above under Imaging, except that 185 MBq (5 mCi) 131I was used for the follow-up DxWBS.
Treatment Outcomes
We categorized the treatment outcomes as (a) a complete response (CR), in which no visible radioiodine uptake was present in the thyroid bed; (b) a partial response (PR), in which some radioiodine uptake was still present in the thyroid bed, but the 24-h radioiodine uptake was <50% of the baseline; and (c) no response (NR), in which residual radioiodine uptake was present in the thyroid bed, and the 24-h uptake was ≥50% of the baseline. Two nuclear medicine attending radiologists evaluated the DxWBSs. The nuclear medicine readings were not performed in a blinded fashion, although the physicians who read the films were unaware that a retrospective analysis of these data would occur.
Laboratory and Pathology Studies
Serum Tg was measured with an immunoradiometric assay using 2 antigen-specific antibodies, each reacting with different epitopes on the Tg molecule (Dynotest-TgS; Brahms Inc., Berlin, Germany). One antibody (rabbit polyclonal) is immobilized on the inside of a plastic test tube and the second antibody (mouse monoclonal) is labeled with 125I and acts as a tracer. A recovery assay using 50 ng Tg per tube is performed simultaneously with each Tg assay to monitor for potential interference by Tg autoantibodies. The interassay precisions for the Tg assay at 3.0 and 60.0 ng/mL were 3.2 ng/mL (8.7% coefficient of variation [CV]) and 62.8 ng/mL (2.3% CV), respectively. The functional sensitivity was 0.3 ng/mL. Tg concentrations of <0.3 ng/mL were reported as <0.3 ng/mL. Recovery assay precision was considered acceptable between 42 and 58 ng/mL higher than that of the unspiked patient specimen. Tg recovery levels beyond these limits indicate recovery disturbance or a high-dose (>2,000 ng/mL) hook effect, and results were considered unreliable. TSH was determined by a heterogeneous sandwich immunoassay on an Immuno 1 System (Bayer Corp., Tarrytown, NY). The assay exhibits a functional sensitivity of 0.014 mU/L. The normal range for this assay is 0.37–4.42 mU/L. Free thyroxine (l-3,5,3′,5′-tetraiodothyronine; T4) was measured on an Immuno 1 System with a heterogeneous competitive magnetic separation assay that has a sensitivity of 0.1 ng/dL and an interassay CV of 6.0% at 1.25 ng/dL. The normal range for free T4 is 0.8–2.0 ng/dL.
Surgical pathology slides from all patients were reviewed by attending pathologists and confirmed to be differentiated thyroid cancer before any nuclear medicine studies. Pathology specimens for all patients included in this study were reread by another attending pathologist for reconfirmation of the histologic diagnosis.
Statistical Methods
Data are presented as mean ± SD, with median values and ranges given when the distribution of data was markedly skewed. Individual factors in both groups were analyzed by the Levene test for equality of variances, by the Pearson χ2 test for discontinuous variables, and by a t test for continuous variables. Significance was chosen at the P < 0.05 level.
RESULTS
Patient and Tumor Characteristics
The mean age of the patients in group 2 was statistically higher than that in group 1 patients (Table 1). There was a higher female-to-male ratio in group 2, but it was not statistically different. There were no significant intergroup differences in tumor size or in the frequency of distant metastases. Group 2 patients were more likely to have an N0 status at the time of initial diagnosis (P < 0.01). There was no difference in the overall American Joint Committee on Cancer (AJCC) stage of the disease between groups. The RRA was performed a median of 6 wk after thyroidectomy in group 1 (range, 2–18 wk) and a median of 9 wk after thyroidectomy in group 2 (range, 4–168 wk).
Patient and Tumor Characteristics
Nuclear Medicine and Laboratory Testing
The patients in group 1 had a significantly lower free T4 and an elevated serum TSH before the ablation, consistent with having been withdrawn from thyroid hormone (Table 2). The patients in group 2 had been placed on thyroxine supplements after surgery and they had normal free T4 levels; however, their mean baseline TSH level was slightly above normal at 6 mU/L. The median baseline TSH was 1.4 mU/L. After 2 doses of rhTSH, the mean serum TSH level in group 2 rose to 105 mU/ L, which was not statistically different from the baseline TSH in group 1. However, TSH levels in group 1 were likely elevated for a much longer time compared with that of group 2. The median stimulated Tg level was slightly higher in patients who were withdrawn from thyroid hormone (P = 0.04). This correlated with a higher median pre-RRA 24-h uptake in the neck, suggesting either that the remnants were larger or that the prolonged elevation of TSH in the THW group more fully stimulated the remnants.
Nuclear Medicine and Laboratory Data
Patients in group 2 received a slightly, but significantly, higher amount of 131I for the initial diagnostic scan (P = 0.01). The choice of ablative activity was determined by standard clinical practice and the recommendation of a tumor board of thyroid cancer experts. There was no statistical difference between the mean activity administered to group 1 patients (4.77 ± 2.74 GBq [128.9 ± 74 mCi]) and that administered to group 2 patients (4.07 ± 2.41 GBq [110.4 ± 65 mCi]). Four of the patients in group 1 and 2 of the patients in group 2 had evidence of distant metastases on the DxWBSs. Seven patients in group 1 and 4 in group 2 had evidence of distant metastases on the scans obtained after therapy (P = 0.35, not significant).
Treatment Outcomes
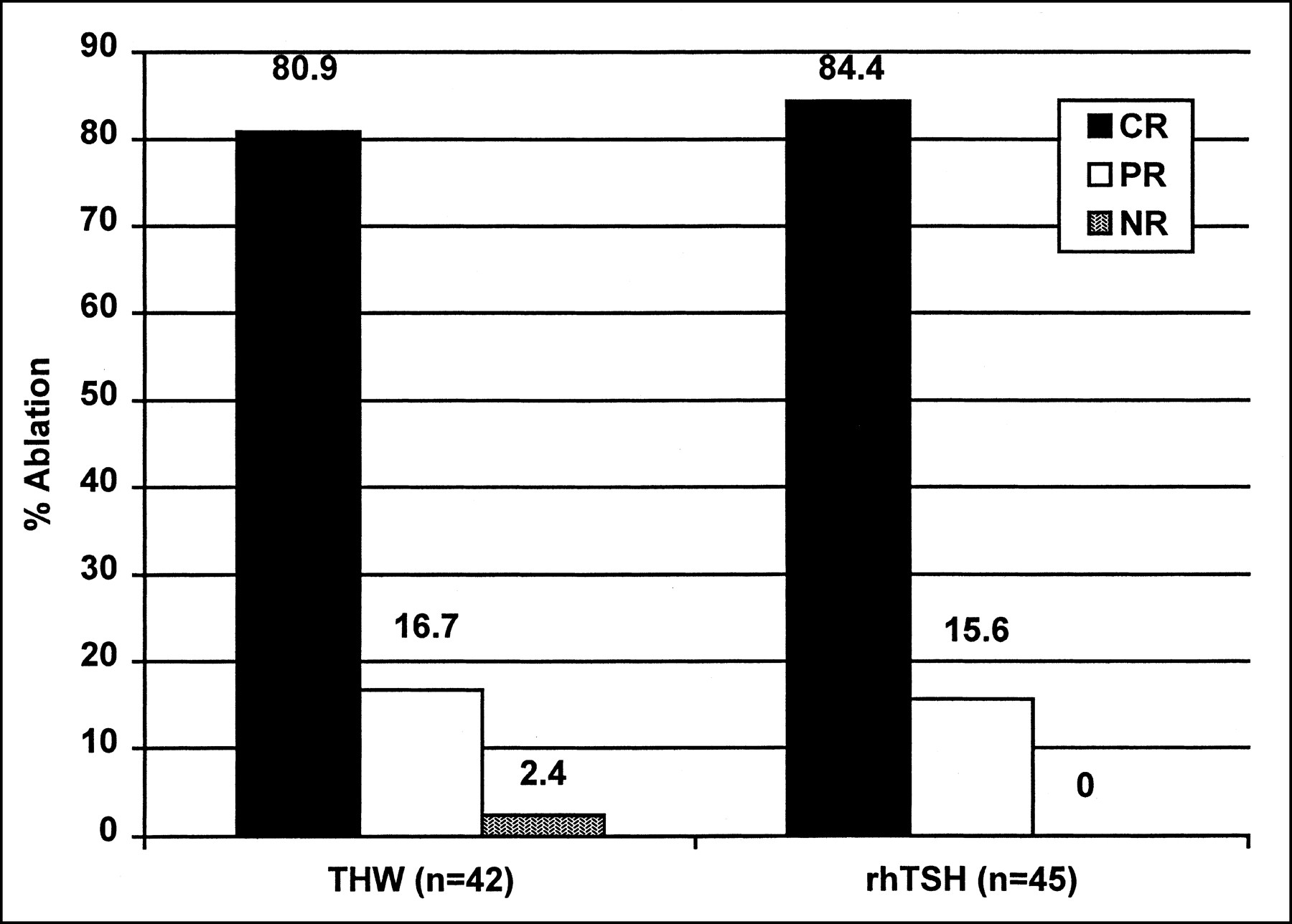
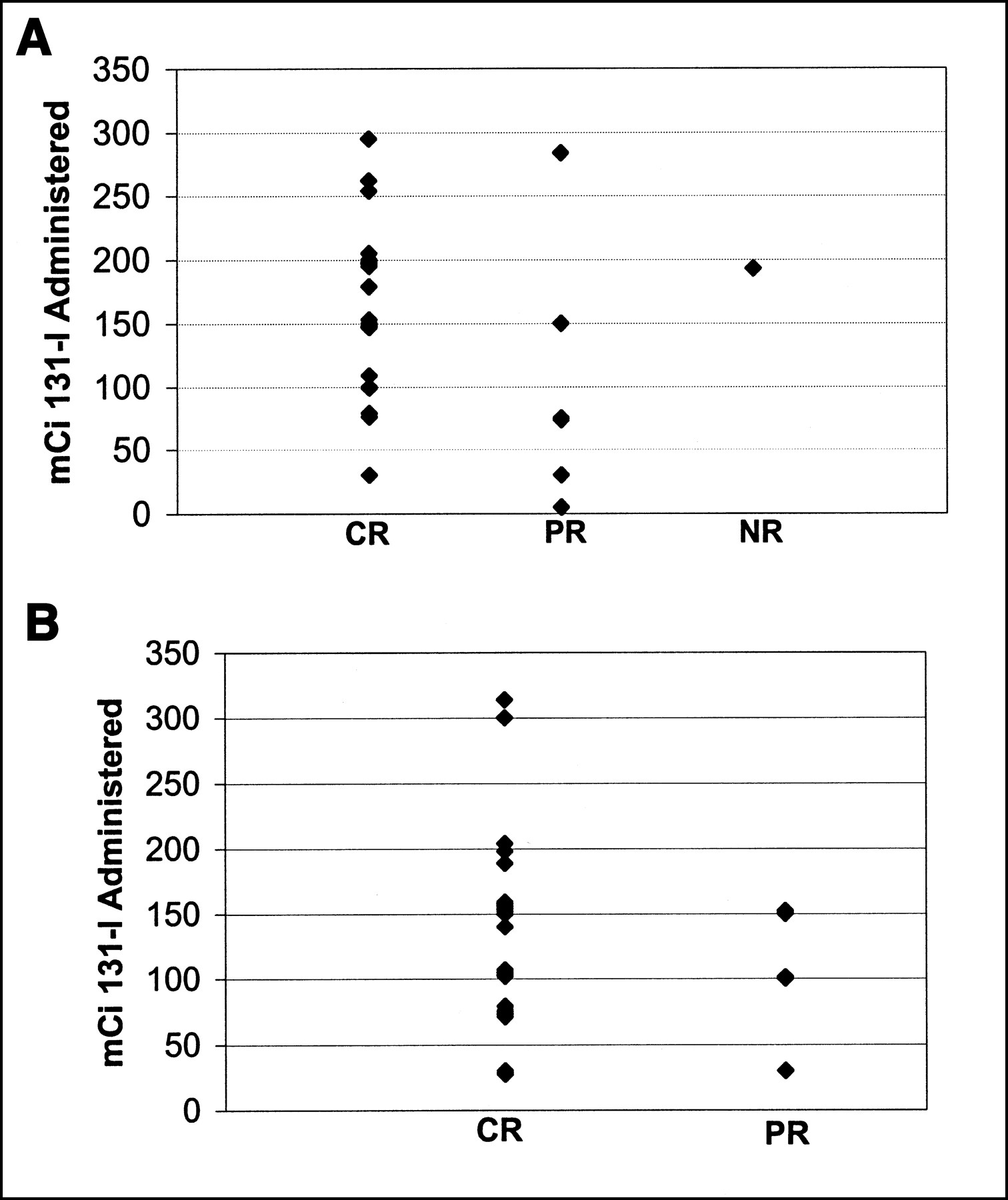
Follow-up scans were done 11.2 ± 2.5 mo after RRA in group 1 and 10.8 ± 3.2 mo after RRA in group 2. Thirty-seven of the 42 (88%) subsequent evaluations in group 1 were done after preparation by rhTSH, whereas all subsequent evaluations in group 2 were done after rhTSH. Only 1 of the 5 group 1 patients who had withdrawal follow-up scans had any uptake in the thyroid bed (categorized as a PR). Complete ablation of all radioiodine uptake in the thyroid bed (CR; Fig. 2) was achieved in 34 of the group 1 patients (80.9%) and in 38 of the group 2 patients (84.4%). PRs, defined as visible uptake in the thyroid bed but <50% of the baseline radioiodine uptake, were achieved in 7 patients (16.7%) in group 1 and in 7 patients (15.6%) in group 2. Only 1 patient in group 1 had an incomplete ablation with >50% of the baseline uptake still present on the follow-up scan (NR). There were no statistical differences between groups in the CR, PR, or NR rates. The activities of 131I administered to individual patients in relation to outcome are shown in Figure 3. The median stimulated Tg levels at follow-up (Table 2) were 0.65 ng/mL (range, 0.3–5,000 ng/mL) for group 1 and 0.5 ng/mL (range, 0.3–4,980 ng/mL) for group 2 (P = 0.48). Using the stimulated Tg cutoff of 2 ng/mL as indicating residual disease, 15 of 42 patients in group 1 were above this cutoff compared with 10 of 44 patients in group 2.

RRA rates in 2 groups: THW and rhTSH. Numbers above bars indicate exact percentage obtained for each category.
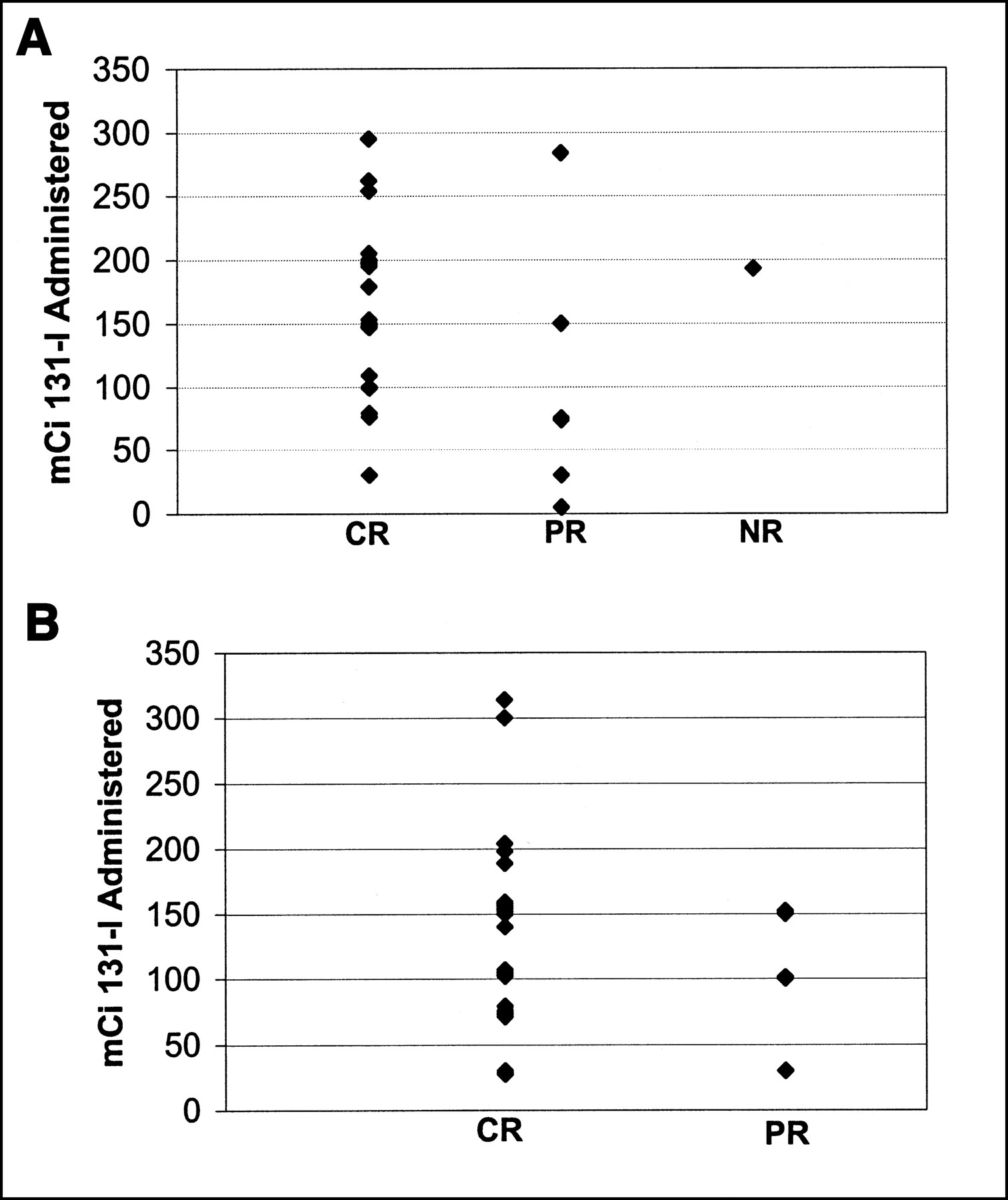
Comparison of amount of 131I administered and final clinical outcome. (A) Group 1. (B) Group 2.
DISCUSSION
Radioiodine ablation of remnants after near-total or total thyroidectomy has become a standard therapeutic procedure in many medical centers, based on reports that this maneuver can reduce locoregional recurrences and, in some patients, can increase overall survival (12,22), with a minimum of side effects.
On the basis of our earlier compassionate need studies using rhTSH to assist delivery of 131I therapy (23,24), we found that iodine clearance rates were generally faster in patients who remained on thyroid hormone suppression and received rhTSH compared with those of patients who were hypothyroid after THW. We were unable to create formulas to reliably calculate a hypothyroid MTA if the dosimetry data were collected in the euthyroid state after rhTSH. Therefore, the administration of the therapeutic activity had to be done in the same physiologic state as that in which the calculation of the MTA was made. Several clinicians at our medical center then began offering rhTSH-assisted therapy to patients who had had rhTSH dosimetry, given that the safety limits could be accurately defined, in that physiologic state. The product used in this study, Thyrogen, has been approved by the Food and Drug Administration only for diagnostic studies. Its use in this study is an off-label one. We do not encourage routine use of Thyrogen to prepare patients for radioiodine therapy until more studies are available on its safety and efficacy.
Analysis of the subsequent DxWBSs in the first 10 patients who had rhTSH-assisted ablations at our center revealed complete absence of any radioiodine uptake in all 10 (19). It is important to point out that the follow-up scans on all of those patients were obtained after rhTSH preparation. Two recent reports have found that DxWBSs tend to be slightly less sensitive, though not statistically different, in patients who are prepared by rhTSH compared with those prepared by THW (16–18).
In this retrospective review of RRA, we found few clinically significant differences in the patient or tumor characteristics between the patients who were prepared by THW and those prepared by rhTSH. Patients in the rhTSH group were older, but there were no practice trends that we could identify to explain this difference. All patients had diagnostic and therapeutic administration of 131I at 1 medical center, using a similar standard-of-care protocol. We found that the likelihood of a complete resolution of radioiodine uptake in the thyroid bed on a 1-y follow-up scan was not statistically different whether the patients were prepared by rhTSH or by THW.
It is important to emphasize that complete thyroid remnant ablation does not mean that the patient is cured of thyroid cancer. It is not uncommon for microscopic metastatic deposits to escape detection on a DxWBS only to be detected years later on the basis of physical examinations, elevation in serum Tg, or abnormal neck sonography. Conversely, an elevated serum Tg is not proof of failed ablation because this protein can be produced by locoregional or distant metastases.
Retrospective studies have limitations, especially with unquantifiable biases that are part of everyday medical practice. It is possible, for instance, that clinicians who chose to offer the option of rhTSH preparation, did so in lower risk patients. As can be seen in Table 1, patients who underwent THW tended to have more evidence of lymph node involvement, although there was no tendency for the THW patients to have a higher AJCC stage. There may have been a tendency to administer higher amounts of 131I to rhTSH patients because they are thought to have more rapid whole-body iodine clearance, although the administered activities were comparable in our 2 groups. It is also possible that the THW group was more likely to have had positive follow-up scans because 5 of the patients (12%) had their follow-up scans performed while they were hypothyroid. However, only 1 of the 5 patients had less than a complete ablation, making this hypothetic difference insignificant in our cohort.
Previous reports on the success of remnant ablation have focused on the dose of 131I used and have all been done in patients after THW (7). Because there has been a wide variation in the preparation, the scan techniques, and the definition of success, there is no gold-standard protocol for ablating thyroid remnants (15,25). Reported RRA success rates range from 50% to 84% (3–9). Some investigators use the 24-h radioiodine uptake in the neck to define ablation, with residual uptakes as high as 1% being considered a successful ablation (26). It is not yet known if rhTSH alters the dwell time of radioiodine in the thyroid remnant. It is generally accepted, however, that whole-body iodine clearance is reduced in the hypothyroid state. Therefore, if comparable ablation rates can be achieved by similar amounts of 131I in the euthyroid state, patients would theoretically be exposed to less total-body radiation.
We chose to use the total lack of visible uptake of radioiodine as the criterion for complete ablation. Other investigators consider visible uptake in the thyroid bed that is <1% of the administered activity at 24 h as a success. We believe that the 24-h neck uptake is less reliable because it can be influenced by several variables, including residual radioiodine in metastatic lymph nodes, in the oropharynx, in salivary glands, or in the esophagus. Neck uptake is also influenced by the geometry of probes, and in the operator’s variability in placing probes, unless carefully controlled in a prospective study. The decision of whether to retreat or reablate patients who have less than complete ablation has never been carefully investigated and remains in the realm of clinical judgment.
One technical issue that is often discussed in analyzing ablation rates is the possibility that the dose of 131I used to perform the diagnostic studies before RRA may stun the remnant and reduce its ability to concentrate radioiodine (6,8,27). A significantly higher pre-RRA scanning dose was used in the rhTSH group; however, the difference was so small that it is unlikely that there was significantly more stunning in that group.
Several issues regarding RRA are still not well defined. One factor is the optimal interval between the thyroidectomy and the RRA. The standard of care in most medical centers is to perform the RRA 6 wk after surgery to allow the TSH to rise above 25–30 U/L. Our rhTSH group received RRA a median of 9 wk after surgery compared with 6 wk for the THW group. Studies to examine the optimal timing of RRA could be more easily performed using the rhTSH preparation because patients are not symptomatic from hypothyroidism. A second issue is the optimal 131I activity administered for RRA (28). An analysis of all studies published on this point recently concluded that the appropriate dose still remains to be defined (25). Because there is variability in remnant production of thyroid hormones after THW, the levels of TSH seen before RRA vary widely. On the other hand, the use of rhTSH, which produces a similar, short-lived, and reliable elevation of serum TSH level, despite age and body mass differences, might provide a better basis for examining this issue in prospective studies.
CONCLUSION
In this uncontrolled retrospective analysis of practice patterns at our medical center, we did not find a significant difference in the rates of complete ablation between a group of patients who were prepared by THW and another similar group of patients who were prepared by rhTSH. On the basis of our findings, we believe that a prospective randomized trial comparing the 2 methods of RRA preparation would be reasonable and valuable. If our findings were confirmed, the choice of preparation for RRA (THW vs. rhTSH) would be made on the basis of the patient’s quality of life and the “cost” of hypothyroidism versus the cost of rhTSH, and not on the likelihood of a complete ablation, which appears to be similar for these 2 methods of preparation.
Acknowledgments
The authors thank the staff of the Nuclear Medicine Service for their careful and compassionate interactions with our patients and thank the physicians who have provided excellent care for these patients, including: Drs. Lanceford Chong, Alexandra Dimich, William Drucker, Dennis Kraus, Eseng Lai, Jatin Shah, Martin Sonenberg, Sam Yeh, and Henry Yeung. The authors also thank Cherryl Murray-Marone for editorial assistance. These studies were funded in part by the Research and Development Fund of the Endocrinology Service and the Byrne Research Fund. Drs. Robbins and Tuttle have received consultant and lecture honoraria from the Genzyme Corporation. The Genzyme Corporation had no role in the design, analysis, interpretation, writing, or funding of this research report.
Footnotes
Received Feb. 12, 2002; revision accepted Jul. 9, 2002.
For correspondence or reprints contact: Richard J. Robbins, MD, Endocrinology Service, Box 296, Memorial Sloan-Kettering Cancer Center, 1275 York Ave., New York, NY 10021.
E-mail: robbinsr{at}mskcc.org
REFERENCES
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Retrospective study of the influence of hypothyroidism on liver function before radioiodine therapy in China: a comparison analysis based on patients with differentiated thyroid cancer
- The SNMMI Practice Guideline for Therapy of Thyroid Disease with 131I 3.0
- Salivary Gland Side Effects Commonly Develop Several Weeks After Initial Radioactive Iodine Ablation
- Reply: A New Age for Recombinant Human Thyroid-Stimulating Hormone?
- Recombinant Human TSH-Assisted Radioactive Iodine Remnant Ablation Achieves Short-Term Clinical Recurrence Rates Similar to Those of Traditional Thyroid Hormone Withdrawal
- Role of Radioactive Iodine for Adjuvant Therapy and Treatment of Metastases
- Prediction of Absorbed Dose to Normal Organs in Thyroid Cancer Patients Treated with 131I by Use of 124I PET and 3-Dimensional Internal Dosimetry Software
- Empiric Radioactive Iodine Dosing Regimens Frequently Exceed Maximum Tolerated Activity Levels in Elderly Patients with Thyroid Cancer
- Cost-effectiveness of using recombinant human TSH prior to radioiodine ablation for thyroid cancer, compared with treating patients in a hypothyroid state: the German perspective
- European consensus for the management of patients with differentiated thyroid carcinoma of the follicular epithelium.
- Iodine Biokinetics and Dosimetry in Radioiodine Therapy of Thyroid Cancer: Procedures and Results of a Prospective International Controlled Study of Ablation After rhTSH or Hormone Withdrawal
- Post-surgical use of radioiodine (131I) in patients with papillary and follicular thyroid cancer and the issue of remnant ablation: a consensus report
- rhTSH-aided radioiodine ablation and treatment of differentiated thyroid carcinoma: a comprehensive review
- The Evolving Role of 131I for the Treatment of Differentiated Thyroid Carcinoma
- Coming of Age: Recombinant Human Thyroid-Stimulating Hormone as a Preparation for 131I Therapy in Thyroid Cancer