


Abstract
Although various noninvasive methods have been used to detect vasospasm, none of them are sensitive enough for patients with sporadic attacks. Because abnormal fatty acid metabolism and cardiac adrenergic neuronal damage are observed in ischemic myocardium, 123I-15-(p-iodophenyl)-3-R,S-methyl pentadecanoic acid (BMIPP) and 123I-metaiodobenzylguanidine (MIBG) have recently been proposed as useful tracers for detection of myocardial damage. This study investigated the relationships among the coronary vasospastic regions, abnormal left ventricular regional wall motion, fatty acid metabolism, and sympathetic nerve functions and their changes during treatment in patients with vasospastic angina. Methods: We evaluated 50 patients with vasospastic angina (25 with clinically documented vasospasm [group A] and 25 with vasospasm induced by ergonovine provocation [group B]) and 25 control subjects who had chest pain but had normal coronary arteries without ergonovine provocation of spasm. Sixteen patients in group A were reevaluated 6 mo after medical treatment. The territorial regions of the vasospasm-induced coronary artery, wall motion determined by left ventriculography, and BMIPP and MIBG uptake were compared. Results: Regions exhibiting a positive reaction to the ergonovine provocation were observed in the right coronary artery in 41 patients, the left anterior descending artery in 33, and the left circumflex artery in 21. Provocation occurred in multiple vessels in 29 patients (58%). Reduction of wall motion was observed in 19 patients (38%). Sensitivity and specificity for the identification of vasospastic angina were 86% (43/50 patients) and 88% (22/25 control subjects), respectively, for BMIPP scintigraphy and 100% (50/50 patients) and 56% (14/25 control subjects), respectively, for MIBG scintigraphy. In the region exhibiting a reduction in left ventricular wall motion, BMIPP or MIBG uptake was decreased. The sensitivity and specificity of determination of vasospasm-induced coronary arteries were 71% (67/95 arteries) and 95% (71/75 arteries), respectively, for BMIPP scintigraphy and 96% (91/95 arteries) and 55% (41/75 arteries), respectively, for MIBG scintigraphy. After 6 mo, during treatment, vasospasm was reinduced by ergonovine provocation in 6 patients (group I) and was not reinduced in 10 patients (group II). Improvements of decreased BMIPP and MIBG uptake were lower in group I (25% ± 4% and 16% ± 4%, respectively) than in group II (69% ± 4% and 50% ± 3%, respectively; both P < 0.01). The regions in which vasospasm was reinduced exhibited decreased BMIPP and MIBG uptake. Conclusion: Abnormal fatty acid metabolism and cardiac sympathetic denervation were observed more frequently than were wall motion abnormalities in the vasospastic region in patients with vasospastic angina. BMIPP and MIBG scintigraphy are highly accurate and noninvasive techniques for determining the presence and location of vasospasm.
Vasospastic angina is characterized by resting anginal attacks occurring mainly at night and in the early morning, but asymptomatic ischemic attacks are more frequent in patients with vasospastic angina. Some patients may exhibit reduced left ventricular wall motion due to transient myocardial ischemia resulting from vasospastic attacks (1–3). Although various noninvasive methods have been used to detect vasospasm, none of them are sensitive enough for patients with sporadic attacks.
Long-chain fatty acids are major cardiac energy substrates, and decreased myocardial fatty acid metabolism has been demonstrated in some patients with ischemic heart disease. 123I-labeled 15-(p-iodophenyl)-3-R,S-methyl pentadecanoic acid (BMIPP) is a tracer that has been widely used for assessing myocardial fatty acid metabolism, and BMIPP is appropriate for use with SPECT because of its stable accumulation in the myocardium (4–8). 123I-metaiodobenzylguanidine (MIBG), an analog of norepinephrine, has been used to evaluate cardiac sympathetic nerve activity (9–11). Reduced myocardial accumulation of MIBG has been reported in patients with ischemic heart disease (9–11). This abnormal finding has been considered to reflect a decreased uptake and accelerated release of norepinephrine from adrenergic nerve endings.
The aim of this study was to clarify the clinical implications of fatty acid metabolic imaging with BMIPP and of myocardial sympathetic nerve functional imaging with MIBG in patients with vasospastic angina.
MATERIALS AND METHODS
Subjects
Between January 1994 and June 2000, 406 patients with vasospastic angina were admitted to our institution. Fifty patients (45 men, 5 women; mean age ± SE, 57 ± 3 y; age range, 44–69 y) were prospectively selected for this study using the following criteria. All 50 patients had angiographically normal coronary arteries (defined as <25% stenotic) and angiographically documented coronary artery vasospasm. Coronary arteriography was performed using the Judkins technique. Left ventriculography in the right and left anterior oblique projections was used to evaluate segmental contraction abnormalities. If coronary artery stenosis was more than 90%, with ST-segment elevation or depression (≥1 mm) developing after intracoronary injection of methyl ergometrine maleate (ergonovine), coronary vasospasm was diagnosed as reported previously (3,12–14). Ambulatory electrocardiogram monitoring (SM-60; Fukuda Denshi Co., Tokyo, Japan) for at least 48 h demonstrated that 25 patients (clinically documented definite vasospasm group, group A) had spontaneous vasospastic attacks (ST-segment elevation with or without chest pain) and that 25 (vasospasm-induced group, group B) did not have signs of spontaneous vasospastic attacks.
This study also included 25 control subjects (group C) who were suspected of having coronary artery vasospasm because of characteristic chest pain (14 men, 11 women; mean age, 55 ± 4 y; age range, 36–68 y). These control subjects underwent diagnostic cardiac catheterization for evaluation of chest pain. They had angiographically normal coronary arteries and did not have coronary artery vasospasm after injection of ergonovine. Ambulatory electrocardiogram monitoring did not detect any spontaneous vasospastic attacks in any of these control subjects.
In all 75 study subjects, medical treatment, except sublingual nitroglycerin, had not yet been administered, and chest pain attacks had occurred. BMIPP or MIBG scintigraphy was performed on all study subjects within 2 wk before diagnostic cardiac catheterization.
Although exercise 201TlCl myocardial scintigraphy was performed before treatment in all 75 subjects, no persistent abnormalities in 201TlCl uptake were seen. None of the subjects had myocardial infarction, cardiomyopathy, valvular heart disease, left ventricular hypertrophy, congenital heart disease, or hypertensive heart disease.
Written informed consent was obtained from each subject before the study. This study was performed in accordance with the guidelines of the ethical committee of our institution.
Myocardial BMIPP or MIBG SPECT Scintigraphy
BMIPP scintigraphy was performed the morning after an overnight fast. BMIPP (111 or 148 MBq) or MIBG (111 MBq) was intravenously injected into the subjects at rest. The BMIPP and MIBG scintigrams were obtained 15 and 180 min after injection, respectively. In 16 patients in group A, a second study was performed 6 mo after the beginning of medical treatment.
The SPECT system consisted of a single-head large-field-of-view digital gamma camera equipped with a general-purpose, low-energy parallel-hole collimator (ZLC-D-Orbiter; Siemens, Erlangen, German) connected to a microcomputer (Scintipak 24000; Shimadzu Co., Tokyo, Japan), as previously reported (3,12,14). All image sequences consisted of 32 projections with a 64 × 64 matrix acquired for 40 s (BMIPP and MIBG) or 30 s (201TlCl) over a 180° circular orbit, from 30° right anterior oblique to 60° left posterior oblique.
Imaging Analysis
Locations where reduced wall motion and vasospasm occurred, as revealed by left ventriculography and coronary angiography, were described according to the American Heart Association classification (15). The left ventriculogram and angiogram were analyzed using a cine angiocardiography system (CAA-10 ELK; Nishimoto Co., Tokyo, Japan), and the region of reduced wall motion was the area that deviated from the lower limit of the normal range as defined by our institution (3,12,14). BMIPP and MIBG scintigrams of the basal short-axis, the middle short-axis, and the vertical long-axis patterns were obtained by SPECT and were fractionated into 17 segments by coronary artery territory (10,14,16). The left ventricle was divided into the 3 major coronary artery territories. Coronary arteries perfusing 2 overlapping areas were determined by the method of Segar et al. (16). The defect scores of BMIPP and MIBG uptake (graded as normal uptake = 0, mildly decreased uptake = 1, moderately decreased uptake = 2, severely decreased uptake or defect pattern = 3) were visually assessed by 2 physicians who were unaware of the coronary angiography results, as reported previously (3,12,14). Differences of opinion were resolved by consensus. A summational point of a defect score of more than 3 in the respective coronary artery territories was defined as decreased BMIPP or MIBG uptake. The total defect score (TDS) was calculated as the summation of all counts. We assessed the improvement in TDS from the initial and second BMIPP or MIBG scintigrams (initial score − second score/initial score × 100%).
The intraobserver and interobserver variations for determining the defect score of BMIPP were tested in 50 coronary artery territories, and the correlation coefficients were 0.95 and 0.90, respectively (14).
Study 1.
The territorial regions of the vasospasm-induced coronary artery, wall motion determined by left ventriculography, and BMIPP and MIBG uptake were compared in 50 patients with vasospastic angina (25 of group A and 25 of group B) and 25 control subjects (group C).
Study 2.
Sixteen of the 25 patients in group A underwent a second BMIPP and MIBG myocardial scintigraphy, left ventriculography, and ergonovine-provoked coronary arteriography examination after 6 mo of single or combined administration of nifedipine at 40–120 mg/d, diltiazem at 90–300 mg/d, amlodipine at 5–20 mg/d, and isosorbide dinitrate at 40–120 mg/d (14,17). Ambulatory electrocardiogram monitoring for at least 48 h did not detect any cardiac symptoms with ST-segment depression or elevation, confirming that anginal attacks were completely suppressed by this treatment. The dosage and combination of medications were optimized and stabilized for suppression of cardiac symptoms, and all medications were continued during this study.
Statistical Analysis
The Fisher exact test and the Student t test were used to compare the defect score, abnormalities in BMIPP and MIBG uptake, and wall motion in the patients with vasospastic angina and the control subjects. P < 0.05 was considered statistically significant. Values are presented as mean ± SE.
RESULTS
Provocation of Coronary Vasospasm at Cardiac Catheterization
Vasospasm was induced in the right coronary artery (RCA) of 41 patients, in the left anterior descending artery (LAD) of 33 patients, and in the left circumflex artery (LCX) of 21 patients. Multiple-artery vasospasm occurred in 29 patients (58%), 18 (72%) in group A and 11 (44%) in group B. Overall, after intracoronary administration of ergonovine, coronary vasospasm developed in 95 (63%) of 150 coronary arteries in all 50 patients in groups A and B (i.e., vasospasm-induced coronary artery) and did not develop in 55 (i.e., non-vasospasm-induced coronary artery).
Left Ventriculography
Left ventriculography showed reduced wall motion in 19 patients (38%), 11 (44%) in group A and 8 (32%) in group B. The location of reduced wall motion coincided with the territorial regions of the vasospasm-induced coronary artery. Reduced wall motion was more frequently associated with multiple-artery vasospasm than with single-artery vasospasm (15 [52%] of the 29 patients with multiple-artery vasospasm and 4 [19%] of the 21 patients with single-artery vasospasm, P < 0.05). Reduced wall motion was observed in 1 (4%) subject in group C.
BMIPP and MIBG SPECT Scintigraphy
Decreased BMIPP uptake was observed in 43 patients (86%), 23 (92%) in group A and 20 (80%) in group B; decreased MIBG uptake was observed in all 50 patients (P = not statistically significant). The regions with decreased BMIPP or MIBG uptake were consistent with the territorial regions of the vasospasm-induced coronary artery. In most patients, decreased BMIPP or MIBG uptake was observed in the regions where reduced wall motion was indicated by left ventriculography. Of the 25 control subjects, 3 (12%) showed decreased BMIPP uptake and 11 (44%) showed decreased MIBG uptake. Based on these results, sensitivity for the identification of vasospastic angina was 86% (43/50 patients) for BMIPP and 100% (50/50 patients) for MIBG, and specificity was 88% (22/25 control subjects) for BMIPP and 56% (14/25 control subjects) for MIBG.
Among the patients, decreased BMIPP uptake by the vasospasm-induced coronary artery was seen in 24 (73%) of 33 LAD regions, 6 (29%) of 21 LCX regions, and 37 (90%) of 41 RCA regions, and decreased MIBG uptake was seen in 31 (94%) of 33 LAD regions, 19 (90%) of 21 LCX regions, and 41 (100%) of 41 RCA regions. Among the control subjects, decreased BMIPP uptake was seen in 2 (8%) of 25 LAD regions, 0 (0%) of 25 LCX regions, and 2 (8%) of 25 RCA regions, and decreased MIBG uptake was seen in 10 (40%) of 25 LAD regions, 3 (12%) of 25 LCX regions, and 21 (84%) of 25 RCA regions. Overall among the patients, decreased BMIPP uptake was detected in 67 (71%) of the 95 myocardial regions that were perfused by vasospasm-induced coronary arteries, and decreased MIBG uptake was detected in 91 (96%) of the 95 regions. In addition, decreased BMIPP uptake was detected in 12 (22%) of the 55 regions that were perfused by non-vasospasm-induced coronary arteries, and decreased MIBG uptake was detected in 15 (27%) of the 55 regions. Among the control subjects, decreased BMIPP uptake was detected in 4 (5%) of the 75 regions that were perfused by non-vasospasm-induced coronary arteries, and decreased MIBG uptake was detected in 34 (45%) of the 75 regions. For BMIPP, sensitivity for the identification of vasospastic coronary artery was 71% (67/95 arteries) and specificity was 95% (71/75); for MIBG, sensitivity was 96% (91/95) and specificity was 55% (41/75).
Reevaluation by Left Ventriculography, Coronary Arteriography, and BMIPP and MIBG Scintigraphy
Sixteen patients in group A were reevaluated 6 mo after medical treatment. Vasospasm was reinduced by ergonovine provocation in 6 patients (group I) and was not reinduced in 10 (group II) (Table 1; Figs. 1 and 2). Medications were continued during the study, and the dosage and combination of medications did not differ significantly between the 2 groups. In all 6 patients in group I, higher doses of ergonovine were required to induce vasospasm, compared with pretreatment provocation (31 ± 2 vs. 16 ± 3 μg for each coronary artery, P < 0.01). Although in group I there were many patients with multiple-artery vasospasm and reduced wall motion, the TDS of BMIPP and MIBG before medical treatment was not higher for group I than for group II (13.3 ± 2.6 and 28.5 ± 3.1, respectively, for group I vs. 14.9 ± 2.1 and 25.5 ± 2.4, respectively, for group II; not statistically significant).
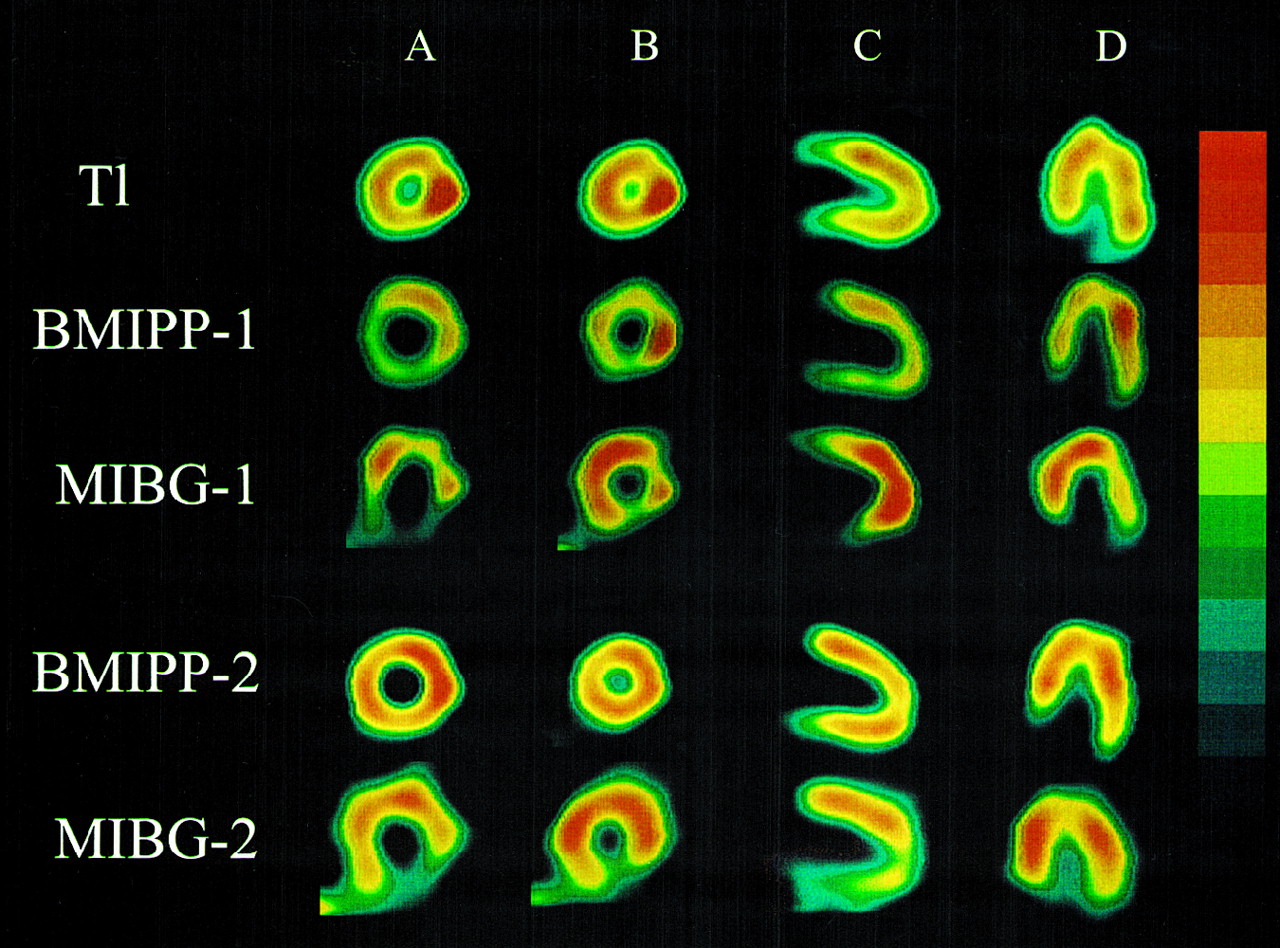
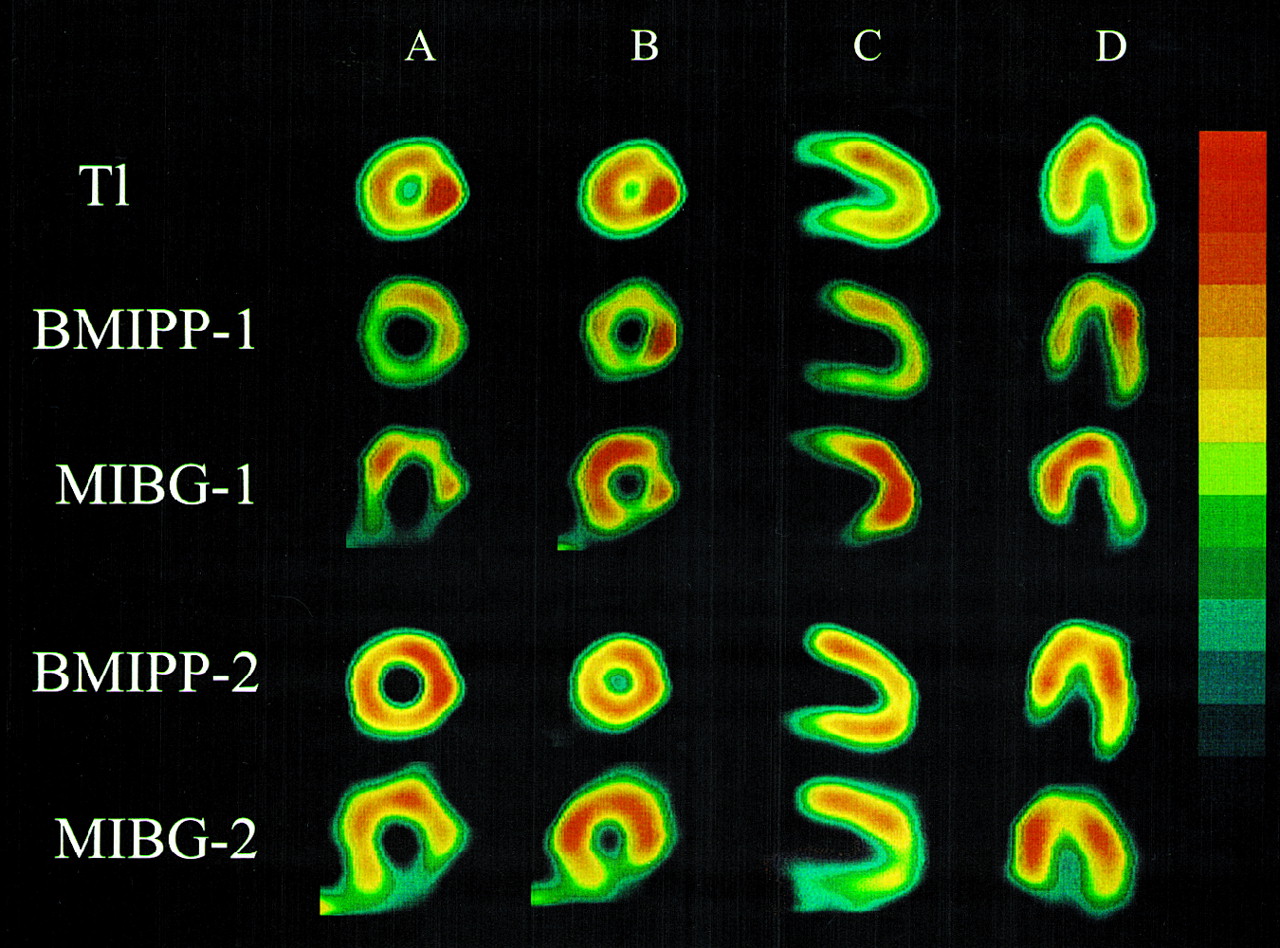
BMIPP scintigrams of vasospastic angina before and after medical treatment of 50-y-old man (patient 1 in group II). Patient had spontaneous vasospastic attacks, and coronary vasospasm was induced in LAD, LCX, and RCA by ergonovine provocation. Decreased BMIPP uptake was seen in anterior, interventricular septum, inferior, and apex regions (BMIPP-1). TDS of BMIPP was 19. Decreased MIBG uptake was observed in anterior, lateral, and inferior regions (MIBG-1). TDS of MIBG was 21. After 6 mo of medical treatment, anginal attacks were completely suppressed and vasospasm was not reinduced by ergonovine provocation. TDS and percentage improvement of BMIPP were 4 and 79% (BMIPP-2). Regions of decreased MIBG uptake were alleviated 6 mo after treatment, except in inferior region (MIBG-2). TDS and percentage improvement of MIBG were 10 and 52%. A, B, C, and D indicate basal short-axis, midventricular short-axis, vertical long-axis, and horizontal long-axis images, respectively.
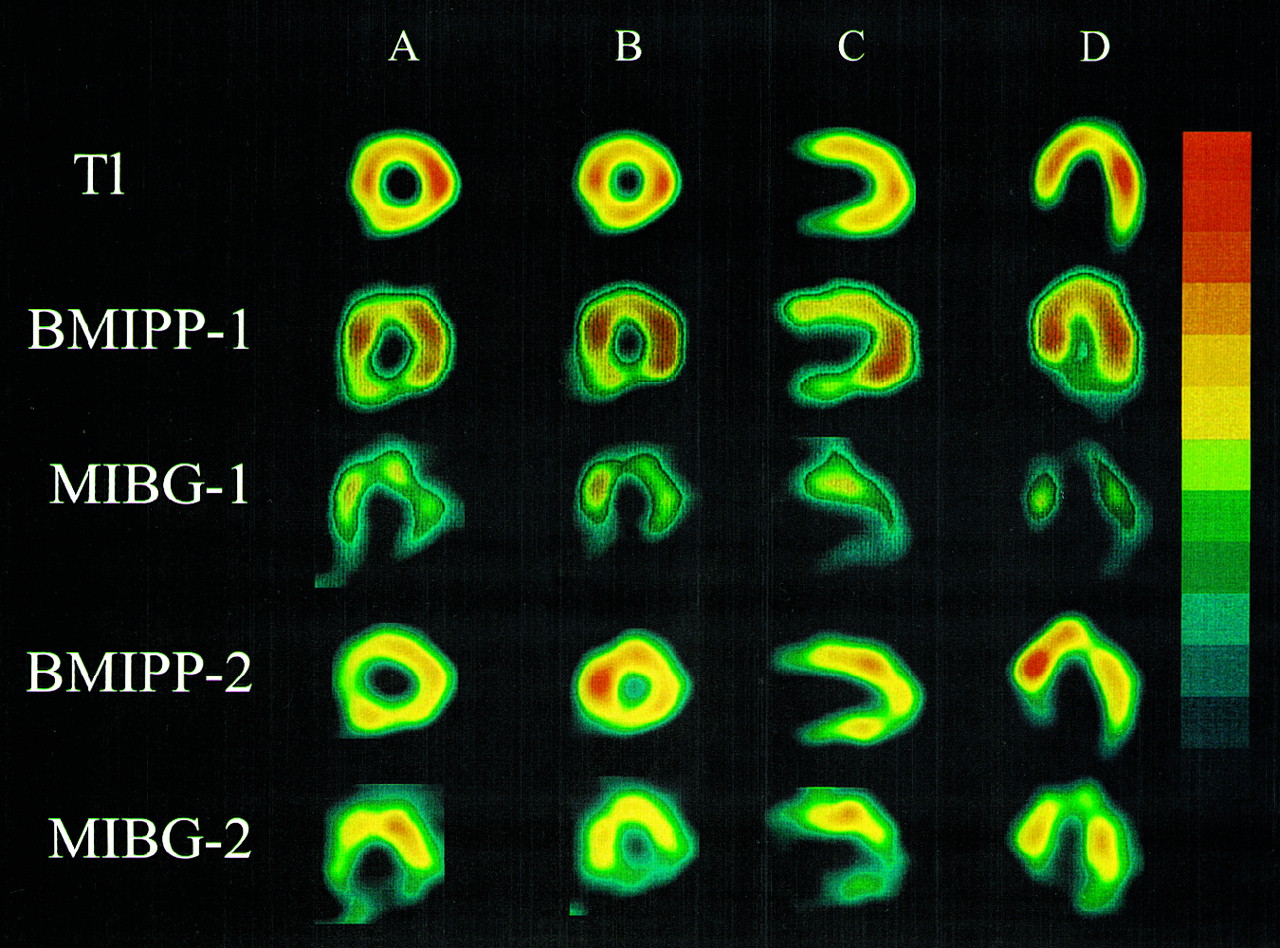
BMIPP scintigrams of vasospastic angina before and after medical treatment of 58-y-old man (patient 1 in group I). Patient had spontaneous vasospastic attacks, and coronary vasospasm was induced in LAD, LCX, and RCA by ergonovine provocation. Decreased BMIPP uptake was observed in anterior and inferior regions (BMIPP-1). TDS of BMIPP was 16. Decreased MIBG uptake was seen in anterior, lateral, inferior, and apex regions (MIBG-1). TDS of MIBG was 34. Although anginal attacks were completely suppressed after 6 mo of medical treatment, vasospasm was reinduced in 3 coronary arteries by ergonovine provocation. TDS and percentage improvement of BMIPP were 11 and 31%. TDS and percentage improvement of MIBG were 24 and 29% (BMIPP-2 and MIBG-2). Patient’s percentage improvements of both tracers were lower than those in group II (Fig. 1)
Defect Score of BMIPP or MIBG
After medical treatment, reduced wall motion was observed in 2 patients in group I and in no patient in group II by left ventriculography, and the region of occurrence corresponded to the region in which vasospasm was reinduced and in which decreased BMIPP or MIBG uptake was observed. Table 1 shows that decreased BMIPP and MIBG uptake still remained in all group I patients; in group II, decreased BMIPP uptake still remained in 4 patients (40%) and decreased MIBG uptake still remained in 10 patients (100%) (Figs. 1 and 2). The TDS of BMIPP and MIBG was higher in group I than in group II (10.2 ± 2.3 and 24.0 ± 2.8, respectively, for group I vs. 4.5 ± 0.9 and 12.6 ± 1.2, respectively, for group II; both P < 0.01), and improvements in the TDS of BMIPP and MIBG were poorer (25% ± 4% and 16% ± 4%, respectively, for group I vs. 69% ± 4% and 50% ± 3%, respectively, for group II; both P < 0.01; Table 1).
DISCUSSION
In some patients with vasospastic angina, abnormal left ventricular wall motion develops as a result of repeated vasospastic attacks, suggesting that metabolic disorders occur in these patients (18–20). Fatty acids are major substrates for normal myocardial energy metabolism. It is therefore important to determine the state of myocardial fatty acid metabolism to determine the viability and ischemic condition of the myocardium. Although positron CT has been useful for evaluating fatty acid metabolism in the myocardium, BMIPP, a 123I-labeled fatty acid with methyl-branching to reduce the rate of β-oxidation, has been used to clarify stunned myocardium and pathologic conditions related to the viability of the myocardium during acute myocardial infarction (4,5,14). MIBG is taken up by cardiac sympathetic nerve endings as a norepinephrine analog, and decreased MIBG uptake recovers after a few months of treatment (9–11). Because decreased BMIPP or MIBG uptake can be detected for about 1–3 mo, it is expected to be useful in the diagnosis of vasospastic angina (4–11). Therefore, we performed BMIPP or MIBG scintigraphy within 2 wk before cardiac catheterization in this study.
In the present study, regional wall motion was reduced in 19 (38%) of 50 patients with vasospastic angina. This finding suggested that the so-called stunned myocardium resulted from vasospasm, although no coronary stenosis was observed on coronary arteriography and the 201TlCl myocardial scintigraphy results were normal. In 5 of the 7 patients who could be reexamined during treatment, reduced left ventricular wall motion was alleviated 6 mo after treatment started. These results also supported the hypothesis that stunned myocardium results from vasospasm.
In contrast, BMIPP and MIBG uptake decreased in 43 patients (86%) and 50 patients (100%), respectively, of the 50 total. In addition, the territorial region of vasospasm-induced coronary artery was consistent with the region with decreased BMIPP or MIBG uptake, and BMIPP or MIBG uptake was decreased in the region where left ventricular wall motion was reduced in most patients. Reduced wall motion was more frequently associated with multiple-artery vasospasm than with single-artery vasospasm and was more frequent in group A than in group B. Abnormalities were more frequently revealed by BMIPP or MIBG scintigraphy than by left ventriculography. In some patients for whom a long interval had elapsed since the attack of chest pain, wall motion was normal despite decreased BMIPP or MIBG uptake. There are 2 possible reasons for these results. Although moderate or severe ischemic attacks cause abnormal left ventricular wall motion and decreased BMIPP or MIBG uptake, mild ischemic attacks may cause only the decreased BMIPP or MIBG uptake. Alternatively, abnormal BMIPP or MIBG uptake may last longer than abnormal ventricular wall motion.
Although noninvasive diagnosis of vasospastic angina has been performed by defect pattern identification or redistribution with 201TlCl during a vasospastic attack induced by exercise or hyperventilation, Koyanagi et al. (20) and Imamura et al. (21) reported that the sensitivity for the diagnosis of vasospasm with exercise 201TlCl scintigraphy was 44%. Some studies have found that the sensitivity for the diagnosis of vasospastic angina with BMIPP and MIBG scintigraphy was 72% and 92%, respectively (5,9,10). In this study, the sensitivity for detecting vasospasm-induced coronary artery was 71% with BMIPP and 96% with MIBG, and the specificity was 95% with BMIPP and 55% with MIBG. These values were determined by analyzing the location of the region of decreased BMIPP or MIBG uptake, using coronary vasospasm induced by ergonovine provocation as a reliable standard. Our results were therefore comparable with those obtained using invasive techniques (12,13). These observations strongly suggest that BMIPP or MIBG more accurately reflects myocardial damage resulting from vasospasm than does 201TlCl scintigraphy or left ventriculography.
The levels of fatty acid metabolism enzymes, such as 3-hydroxyacyl-coenzyme-A dehydrogenase, are lower and sympathetic activity is higher in the ischemic region than in the nonischemic region (7,8). In the 10 (group II) of 16 patients reexamined by BMIPP or MIBG scintigraphy 6 mo after starting medical treatment, the decreased regions of BMIPP or MIBG uptake improved. This finding suggested that myocardial damage involving fatty acid metabolism might recover within 6 mo, and myocardial sympathetic denervation might recover during the same period except in the inferior region. If decreased BMIPP or MIBG uptake is not alleviated after 6 mo of treatment, patients with vasospastic angina should be given additional treatment irrespective of cardiac symptoms.
The patients with vasospastic angina and negative ergonovine provocation have to be considered as healthy control subjects in this study. Decreased BMIPP or MIBG uptake was observed in some of our control subjects, especially in conjunction with reduced wall motion, as indicated by left ventriculography. We suspect that these patients had coronary vasospasm and were false-negative for ergonovine provocation. In all 3 subjects in group C who had decreased BMIPP uptake and could be reexamined during medical treatment, decreased BMIPP uptake was alleviated 6 mo after treatment, supporting our hypothesis. The decreased MIBG uptake was the same as the decreased BMIPP uptake, except in the inferior region. Although the sensitivity of MIBG was higher than that of BMIPP, the specificity of MIBG was lower than that of BMIPP because decreased MIBG uptake in the inferior region was detected not only in groups A and B but also in group C.
We previously encountered patients with vasospastic angina that appeared to be completely suppressed by treatment with calcium antagonists, but some of these patients subsequently experienced sudden death or myocardial infarction, prompting the present study. It is extremely difficult to frequently repeat invasive tests such as left ventriculography or coronary angiography. The effects of treatment can be better assessed, therefore, by observing the regions with decreased uptake in noninvasive BMIPP or MIBG imaging. Noninvasive BMIPP or MIBG scintigraphy should therefore be extremely useful. We now assess the effects of medical treatment for vasospasm using ambulatory electrocardiogram monitoring and BMIPP or MIBG scintigraphy before and after 6 mo of treatment. Although 2 parameters, the uptake and the washout rate of MIBG, are useful to evaluate the sympathetic nerve state in patients with vasospastic angina, we cannot discuss the washout rate of MIBG in this study.
CONCLUSION
Territorial regions in which vasospasm was induced by ergonovine provocation, regions with abnormal left ventricular wall motion, and BMIPP or MIBG scintigrams were compared in patients with vasospastic angina before and after medical treatment. Fatty acid metabolic imaging with BMIPP, which is a superior tracer for specificity, or sympathetic imaging with MIBG, which is superior for sensitivity, permitted the evaluation of vasospastic regions and the noninvasive assessment of the effects of medical treatment.
Acknowledgments
This study was supported by the Yujin Memorial Found; the Promotion and Mutual Aid Corporation for Private School of Japan; and Ministry of Education, Science, Sports and Culture.
Footnotes
Received Oct. 23, 2001; revision accepted Jul. 5, 2002.
For correspondence or reprints contact: Kenichi Watanabe, MD, Department of Clinical Pharmacology, Niigata University of Pharmacy and Applied Life Sciences, Kamishinei-cho, Niigata 950-2081, Japan.
E-mail: watanabe{at}niigata-pharm.ac.jp
REFERENCES
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Cardiac 123I-MIBG Imaging for Clinical Decision Making: 22-Year Experience in Japan
- Ischemic Episode and Hanging on to a Painful Memory...
- Cardiac Sympathetic Imaging With mIBG in Heart Failure
- Discrepant Recovery Course of Sympathetic Neuronal Function and {beta}-Adrenoceptors in Rat Hearts After Reperfusion Following Transient Ischemia