


Abstract
The purpose of the present study was to evaluate the role of 67Ga scintigraphy and CT in treatment monitoring of bone lymphoma. Methods: Forty-four lymphoma patients with 91 sites of bone involvement were evaluated. Eight patients had Hodgkin’s disease, and 36 patients had non-Hodgkin’s lymphoma. Thirteen patients had primary lymphoma of the bone, and 31 patients had secondary lymphoma of the skeleton. 67Ga and CT studies were performed at baseline, during and at the end of treatment, and during follow-up. Positive 67Ga studies showed abnormal uptake in sites of lymphomatous involvement. Positive CT studies showed lesions with patterns of osteolysis, patterns of osteosclerosis, or a mixed pattern. A negative 67Ga or CT study showed disappearance of all lymphoma-related abnormalities. The sensitivity and specificity of 67Ga scintigraphy at presentation were calculated. Patterns of bone lymphoma on CT and their treatment-related changes were analyzed and recorded. Freedom-from-progression (FFP) curves were used to determine the prognostic value of positive and negative 67Ga and CT findings for predicting outcome after treatment. Results: The sensitivity of 67Ga for diagnosis of bone lymphoma was 93%, and the specificity was 91%. A CT pattern of osteolysis was seen in 70% of skeletal disease sites at diagnosis and in 21% during follow-up. Osteosclerosis was present in 23% of sites at diagnosis and in 38% during follow-up. 67Ga findings became negative in 25% of patients during treatment, whereas only 1 patient showed negative CT findings. Forty-two percent of patients had negative 67Ga findings at the end of treatment, compared with 18% who had negative CT findings. Sixty-one percent of patients had negative 67Ga findings during follow-up, compared with 21% who had negative CT findings. A statistically significant difference in FFP was found between patients with positive and negative 67Ga findings at all evaluated time points. No statistically significant difference in FFP was found at any time point between patients with positive and negative CT findings. Conclusion: 67Ga scintigraphy has a high sensitivity and specificity for diagnosis of bone lymphoma. Bone lymphoma may show osteosclerotic and osteolytic CT patterns at diagnosis, during treatment, and after treatment. In most patients, CT studies do not become negative even 1 y after treatment. 67Ga scintigraphy, however, may be used as a predictor of long-term outcome in patients with lymphoma of the skeleton.
Diagnosis and treatment of lymphoma have improved significantly over the last several decades. Novel therapeutic options have been introduced. Developments in functional and anatomic imaging techniques now provide accurate diagnosis as well as good monitoring of response to treatment—the basis for successful management of lymphoma. 67Ga scintigraphy plays an important role in serial assessment of the effect of therapy in both Hodgkin’s disease (HD) and non-Hodgkin’s lymphoma (NHL). The advantages of 67Ga scintigraphy over CT studies as an indicator of tumor viability are well documented (1–3). 67Ga scintigraphy has the ability to discriminate between patients who achieve a complete response and those who show no or only partial response to induction therapy (2,3). Prognosis can be predicted during treatment, as soon as after 1 cycle of chemotherapy, and recurrent disease can be diagnosed early during follow-up (4–6). The value of 67Ga scintigraphy has been assessed in patients with both nodal and extranodal lymphoma (7,8).
Involvement of the skeleton occurs in up to 20% of patients with HD. Approximately 3%–5% of all cases of NHL are primary disease of the skeleton; secondary involvement occurs in up to 25% of patients (9–11). With successful treatment, bone lymphoma has a good prognosis and a high survival rate, and accurate assessment of the response to treatment of lymphoma of the bone is therefore of high clinical significance (12–14). Anatomic imaging modalities, such as CT or MRI, are of value in the initial assessment of the extent of both soft-tissue and skeletal involvement and characterization of bone texture (15–18). Monitoring the response of bone lymphoma to treatment, however, is a diagnostic dilemma (15,19). Studies on the role of CT and MRI in assessing treated bone lymphoma consist usually of small patient series and have found variable imaging patterns (15,20). The value of 67Ga scintigraphy for assessing the response of bone tumors to treatment has also been questioned because of the bone-seeking properties of the radiopharmaceutical (11). Some studies have demonstrated that 67Ga scintigraphy is of value in assessing bone lymphoma (7,18,21), whereas others have suggested that 67Ga uptake in skeletal lesions after treatment may preferentially reflect bone healing, which may not be accurately differentiated from active disease (15,22–24).
The purpose of the present study was to evaluate the role of 67Ga scintigraphy and CT for predicting outcome in treated bone lymphoma. CT patterns of bone lymphoma at baseline and their treatment-related changes are also described. In addition, the value of 67Ga scintigraphy for the initial diagnosis of lymphomatous skeletal lesions was reassessed.
MATERIALS AND METHODS
Patient Population
Fifty-four lymphoma patients evaluated routinely using 67Ga scintigraphy and CT had evidence of lymphoma involving the skeleton. Inclusion criteria into the study were confirmation of 67Ga avidity of the lymphoma before treatment and availability of CT and 67Ga follow-up examinations during and for the first year after completion of therapy. Ten of the 54 patients did not meet these criteria and were therefore excluded from the study. One patient had a non-67Ga-avid lymphoma, 1 patient had no follow-up examinations, 2 patients had surgical removal of a single bone lesion, and 6 patients died early during treatment. Four patients had bone biopsy of a single skeletal lymphoma site before baseline 67Ga scintigraphy. 67Ga avidity of the lymphoma could not be established in these 4 patients, and they were included only in the analysis of CT data. Thus, the final study population included 44 patients with data available for CT and 40 patients with data available for 67Ga scintigraphy. Diagnosis of lymphomatous involvement of the bone was made by radiography and CT in all patients and was confirmed by biopsy in 27 patients.
The study included 19 female patients and 25 male patients with a median age of 38 y (range, 1–79 y). Eight patients had HD, all with secondary involvement of the skeleton. Thirty-six patients had NHL. Of those, 31 had aggressive NHL, 3 had low-grade NHL, and the histologic subclassification of 2 with NHL could not be precisely defined. Thirteen had primary lymphoma of the bone, and 23 had secondary involvement of the skeleton. There was a median of 2 skeletal lymphoma sites in each patient (range, 1–7 sites). The distribution of lymphomatous bone lesions in the peripheral and axial skeleton is shown in Table 1. Twenty-three patients had evidence of soft-tissue involvement in lymph nodes or extranodal sites, in addition to skeletal lymphoma lesions.
Sites of Bone Involvement in Patients with NHL and HD
Six patients with HD received doxorubicin-containing chemotherapy regimens, and 2 patients received other treatment combinations. Chemotherapy of patients with NHL consisted of doxorubicin-containing regimens in 26 patients and other combinations in 10 patients. Radiation therapy was added to involved sites in 19 patients. The median duration of clinical follow-up of patients was 24 mo (range, 5–119 mo).
Imaging Studies
67Ga scintigraphy and CT studies were performed at the time of the initial diagnosis, during treatment at a median of 3 chemotherapeutic cycles (range, 1–7 cycles), at the completion of therapy, and twice during the first year of follow-up. The early follow-up study (FU1) was performed at a median of 4 mo after the end of treatment (range, 2–7 mo). The late follow-up study (FU2) was performed at a median of 11 mo (range, 8–19 mo) from the end of treatment.
67Ga scintigraphy was performed using previously described techniques (3,7). Adult patients received 296–370 MBq (8–10 mCi) 67Ga-citrate intravenously, and children received 2.77 MBq (75 μCi) per kilogram of body weight. Scintigraphy was performed at 48 h and 7 d after the injection of the radiopharmaceutical. The images were obtained using a dual-head camera (Helix; Elscint, Haifa, Israel, or VG; General Electric Medical Systems, Milwaukee, WI). Triple-energy 67Ga peaks of 93, 184, and 300 keV and a parallel-hole, medium-energy collimator (APC-5 or HPC-5; Elscint) were used. SPECT was performed routinely for the whole torso after the planar study at 48 h.
CT studies earlier than 1994 were performed using a standard single-slice CT scanner (Elscint). Thereafter, CT was performed using a helical Twin Flash scanner (Elscint) or a multislice spiral scanner (Marconi Medical Systems, Haifa, Israel). Nonionic contrast medium (80–100 mL iopamidol, 300 mg iodine/mL) was delivered by an automatic injector into the median cubital vein at a flow rate of 2 mL/s, except when contraindicated in patients with allergy to iodine or with creatinine levels higher than 1.5 mg/100 mL. Scanning was performed using a 8.8-mm slice thickness after a 30-s delay for chest and a 60-s delay for abdomen and pelvis examinations. Dedicated examinations using 3- to 5-mm-thick contiguous sections were performed for highly suggestive or proven bone lesions of the axial and peripheral skeleton.
67Ga scintigraphy findings at all evaluated time points were interpreted as positive if they showed 1 or more areas of abnormal uptake in the bone or soft tissues, outside the normal pattern of 67Ga biodistribution. Negative 67Ga findings showed uptake only in regions of normal, physiologic activity.
Findings considered positive for lymphomatous bone involvement on CT before and after treatment were either lytic lesions, seen as separate or coalescent areas of a mottled, permeative, moth-eaten pattern; discrete or diffuse sclerotic lesions; or sites showing a mixed pattern of lysis and sclerosis. Irregularities of the bone cortex, usually in association with osteolysis or osteosclerosis, were also recorded. Any abnormality (bone, soft-tissue, or both) was considered a positive CT finding at the time of the initial evaluation and at each time point related to treatment. CT findings were considered negative when all pathologic findings disappeared. After initiation of treatment, a test was considered positive in the presence of residual findings such as a persistent area of abnormal 67Ga activity, even if decreasing in intensity, or a persistent lesion on CT, even if decreasing in size or showing a change in pattern.
Statistical Analysis
The sensitivity and specificity of 67Ga scintigraphy for detecting bone lymphoma at the time of diagnosis were calculated according to the equations TP/(TP + FN) for sensitivity and TN/(TN + FP) for specificity, where TP = true-positive, FN = false-negative, TN = true-negative, and FP = false-positive. TP studies showed 67Ga uptake in skeletal lymphoma lesions. Patients showing no uptake of 67Ga in sites of bone lymphoma were recorded as FN. TN studies showed no 67Ga uptake when there was no evidence of lymphoma on CT, radiography, or biopsy. FP studies showed 67Ga uptake in bone when CT, radiography, biopsy, or long-term clinical follow-up were negative for lymphoma. Data for sensitivity calculation (TP, FN) were taken from our group of lymphoma patients with proven bone involvement. Data for specificity calculation (TN, FP) were based on findings from the baseline 67Ga studies of a randomly chosen group of 135 lymphoma patients from our institution without bone involvement. For the purpose of this study, the follow-up data from 67Ga and CT performed on the patient group without bone involvement were not further analyzed.
Freedom-from-progression (FFP) curves were used to determine the prognostic value of positive and negative 67Ga scintigraphy and CT findings during and after treatment. FFP was defined as the time from initiation of therapy until disease progression or until the last follow-up examination. Disease progression was defined either as worsening of the primary disease or as the appearance of new sites of lymphoma after the patient had achieved a complete response. Subsets of positive and negative 67Ga scintigraphy and CT findings were compared at each evaluated time point to assess their impact as predictors of FFP. FFP curves for positive and negative 67Ga and CT findings were calculated using the Kaplan-Meier method. Differences in FFP curves were compared using the log-rank test, with statistical significance defined as P < 0.05.
RESULTS
The sensitivity and specificity of 67Ga scintigraphy for the initial diagnosis of bone lymphoma were calculated using a combination of CT, radiography, and biopsy results as the gold standard. A group of 40 patients with known involvement of the skeleton and 135 lymphoma patients of a randomly chosen group with no skeletal involvement were assessed. There were 37 TP studies, 3 FN studies, 123 TN studies, and 12 FP studies. The sensitivity of 67Ga scintigraphy for diagnosis of lymphoma of the bone was 93%, and the specificity was 91%.
67Ga scintigraphy findings were negative for 25% of studies performed during treatment and for 42% of studies performed at the end of treatment. At FU1, 68% of 67Ga studies had negative findings. At FU2, 67Ga scintigraphy findings were negative in 61% of the patients. In 12 of the 23 patients showing soft-tissue involvement in addition to bone lymphoma, changes in 67Ga uptake occurred at the same time points both for involved lymph nodes and for skeletal lesions. In the other 11 patients, disappearance of 67Ga uptake in sites of nodal involvement preceded changes in bone lymphoma lesions. CT findings were negative in 3% of studies (1 patient) during treatment, in 18% of studies at the end of treatment, in 17% of studies at FU1, and in 21% of studies at FU2. The number of 67Ga and CT studies with negative and positive results in relation to treatment is shown in Table 2. The 3-y FFP rate for the entire group of patients was 73.6%. There was a statistically significant difference in the 3-y FFP between patients with positive and negative 67Ga scintigraphy at all evaluated time points: P < 0.05 during treatment, P < 0.03 at the end of treatment, P < 0.0001 at FU1, and P < 0.002 at FU2. CT results were not predictive for FFP. There was no statistically significant difference in the 3-y FFP between patients with positive and negative CT at all evaluated time points (Figs. 1–4; Table 3).
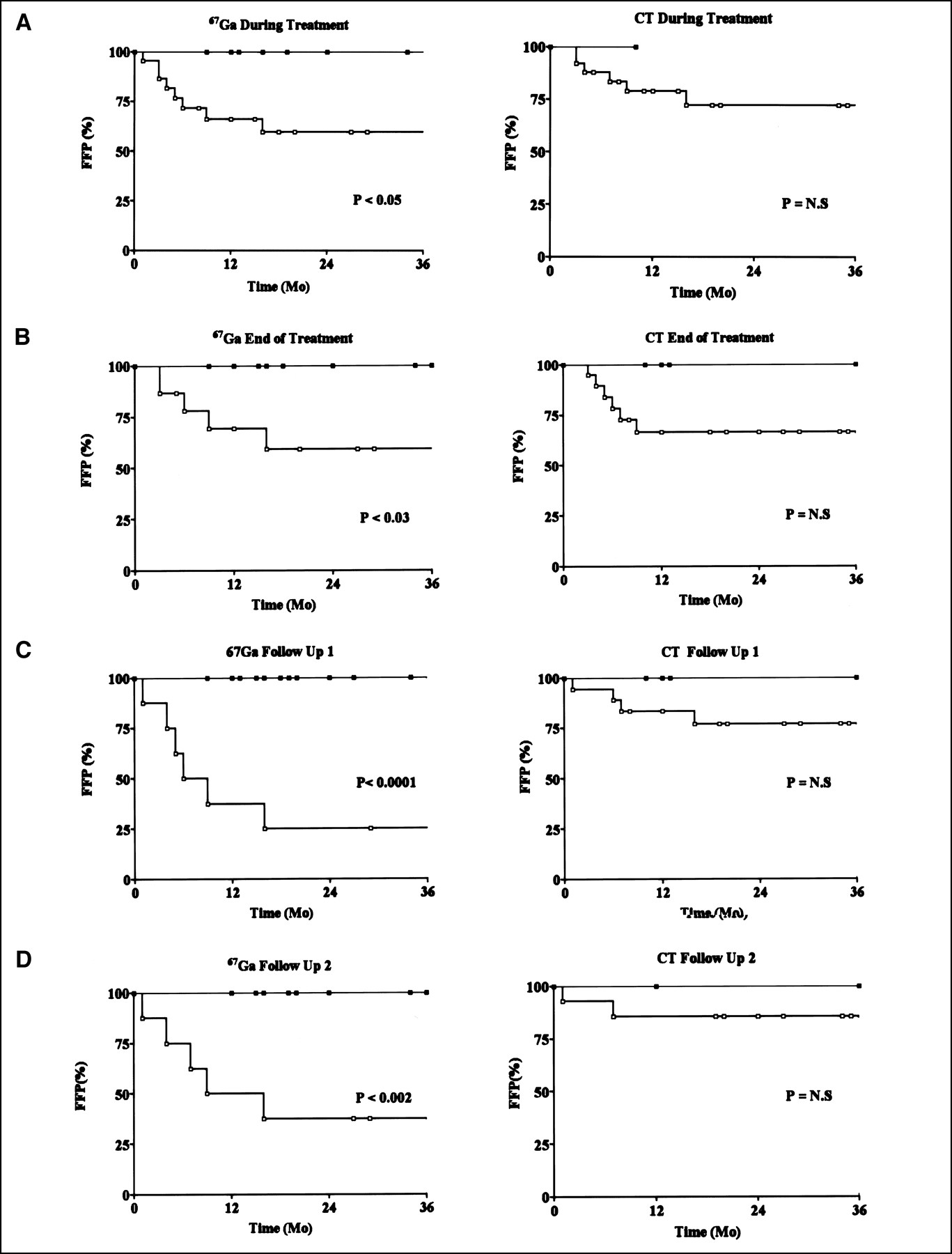
Three-year FFP in patients with positive (□) and negative (▪) 67Ga scintigraphy and CT findings. Graphs show findings during treatment (A), at end of treatment (B), at FU1 (C), and at FU2 (D).

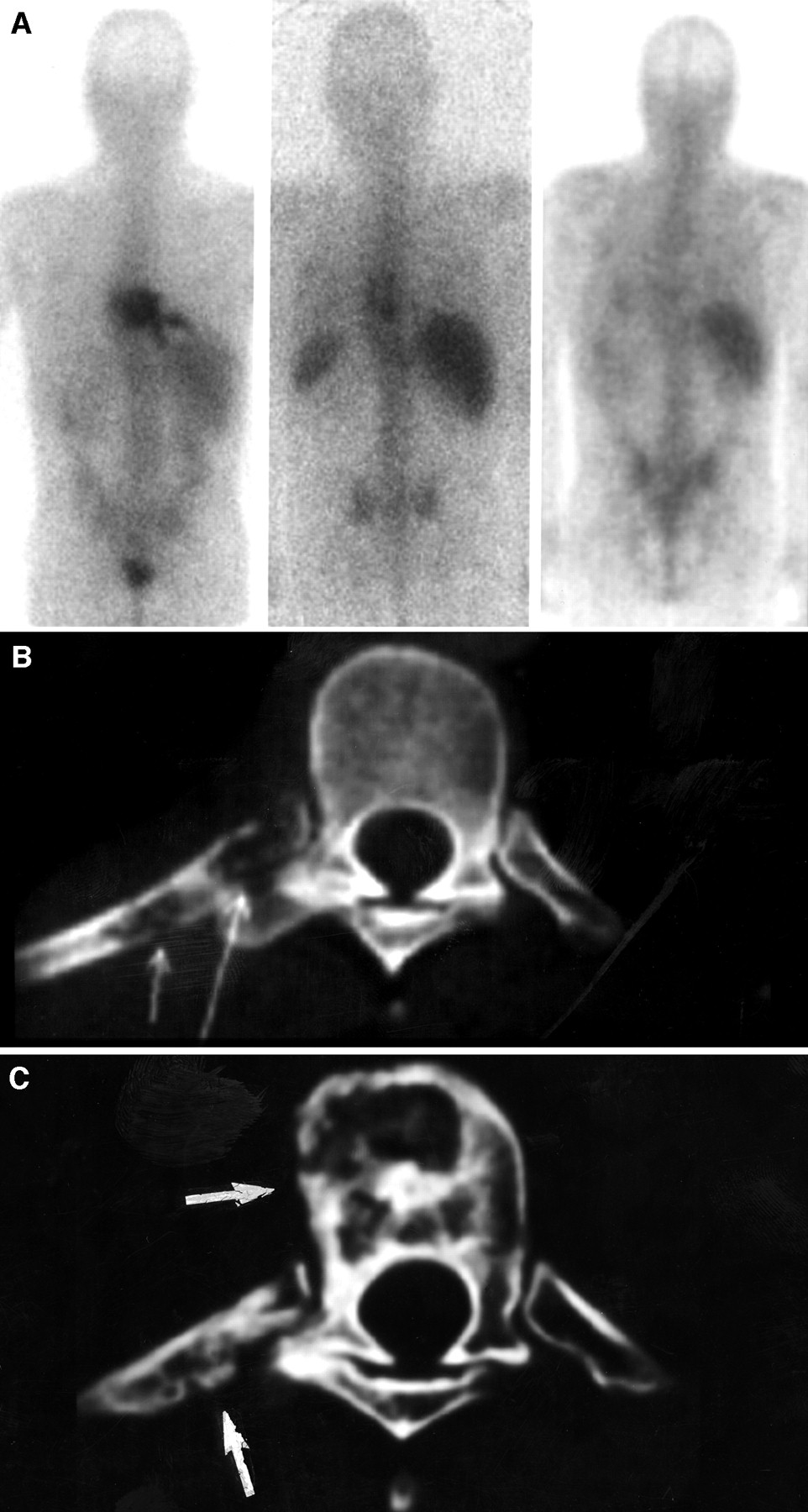
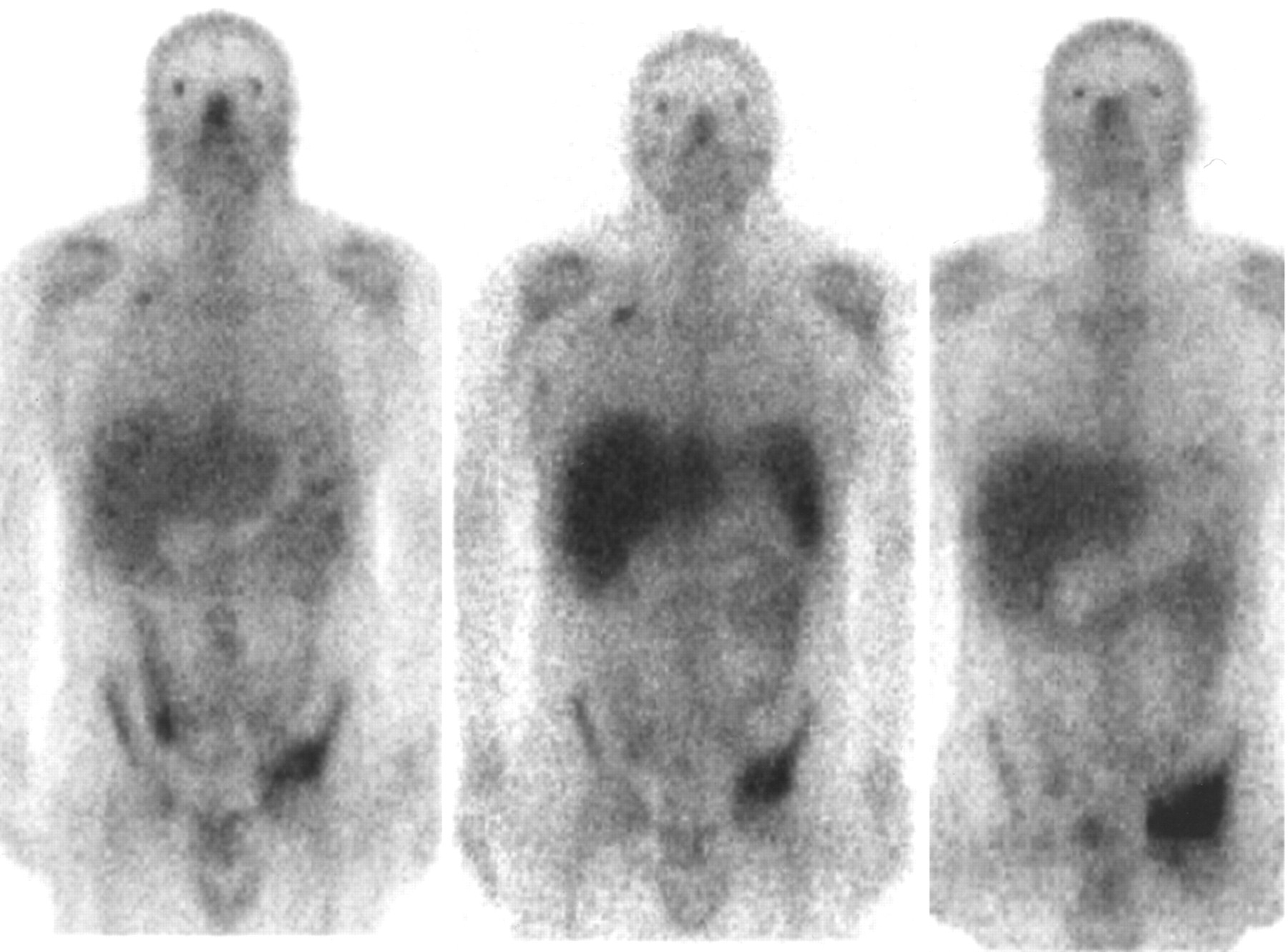
Negative 67Ga scintigraphy and abnormal CT findings at end of treatment in 37-y-old man with diffuse large cell B-type NHL, stage I EA, involving posterior arch of 9th and 10th right ribs and T9 and T10 vertebrae. (A) 67Ga scintigraphy at diagnosis (left) shows pathologic uptake at involved sites of disease. Marked improvement is seen at mid treatment (center), with residual abnormal 67Ga activity in lower thoracic spine. 67Ga scintigraphy findings at end of treatment (right) are negative. (B) CT at diagnosis shows infiltrative osteolytic lesion with cortical disruption of posterior arch of 9th right rib (arrows) and surrounding soft-tissue involvement. Moth-eaten pattern is seen in vertebral body of T9. (C) CT at end of treatment shows mixed sclerotic and lytic pattern in 9th rib and T9 vertebral body (arrows). Patient had no evidence of disease for 30 mo.
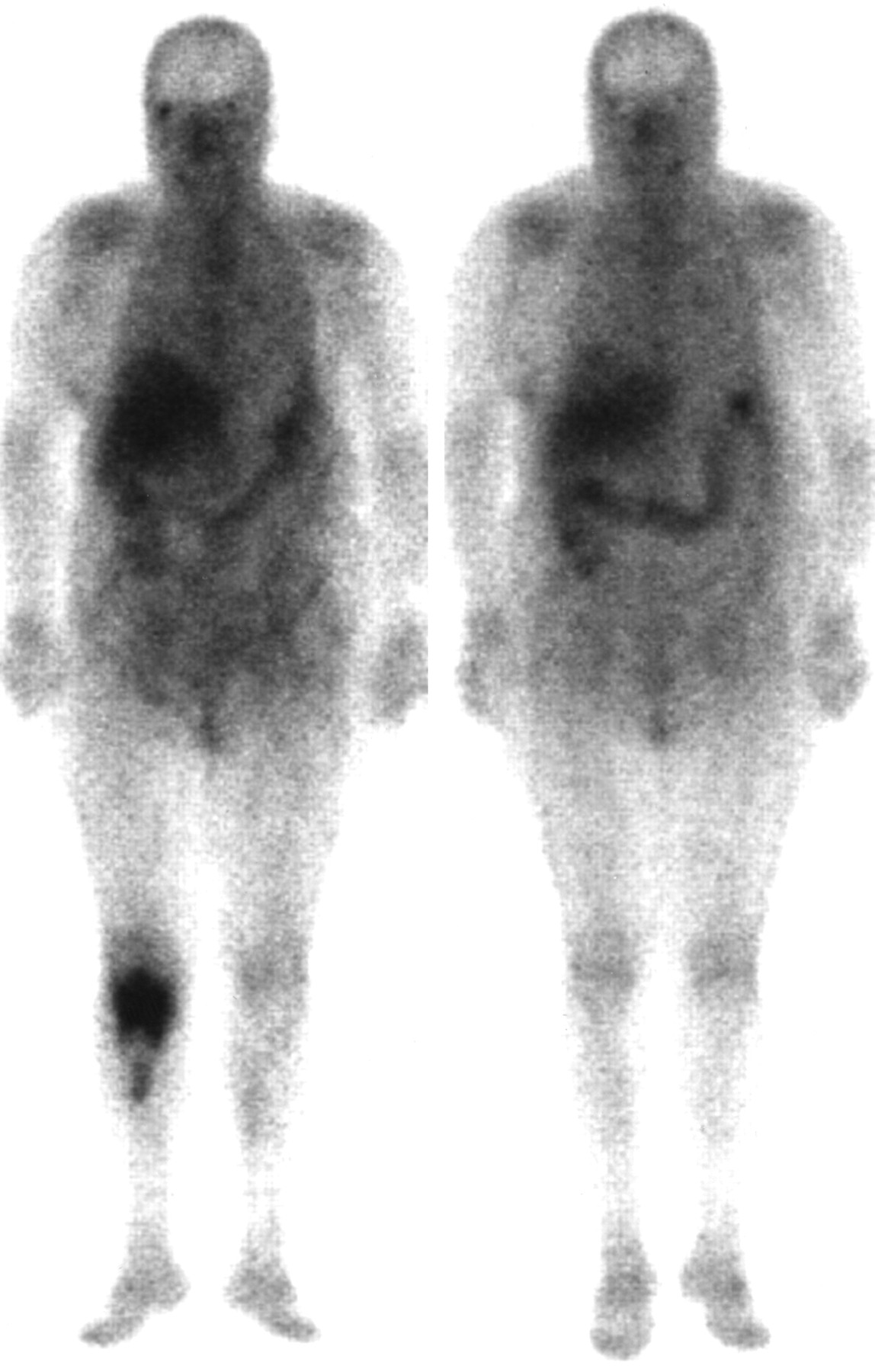
Negative 67Ga scintigraphy findings during chemotherapy in 68-y-old woman with follicular mixed low-grade lymphoma involving right inguinal lymph nodes and right tibia. 67Ga scintigraphy at baseline (left) shows abnormal uptake in proximal right tibia. Repeated 67Ga scintigraphy after 4 cycles of chemotherapy (right) shows negative findings, which remained unchanged at end of treatment and during follow-up. Disease has been in complete remission for 12 mo.
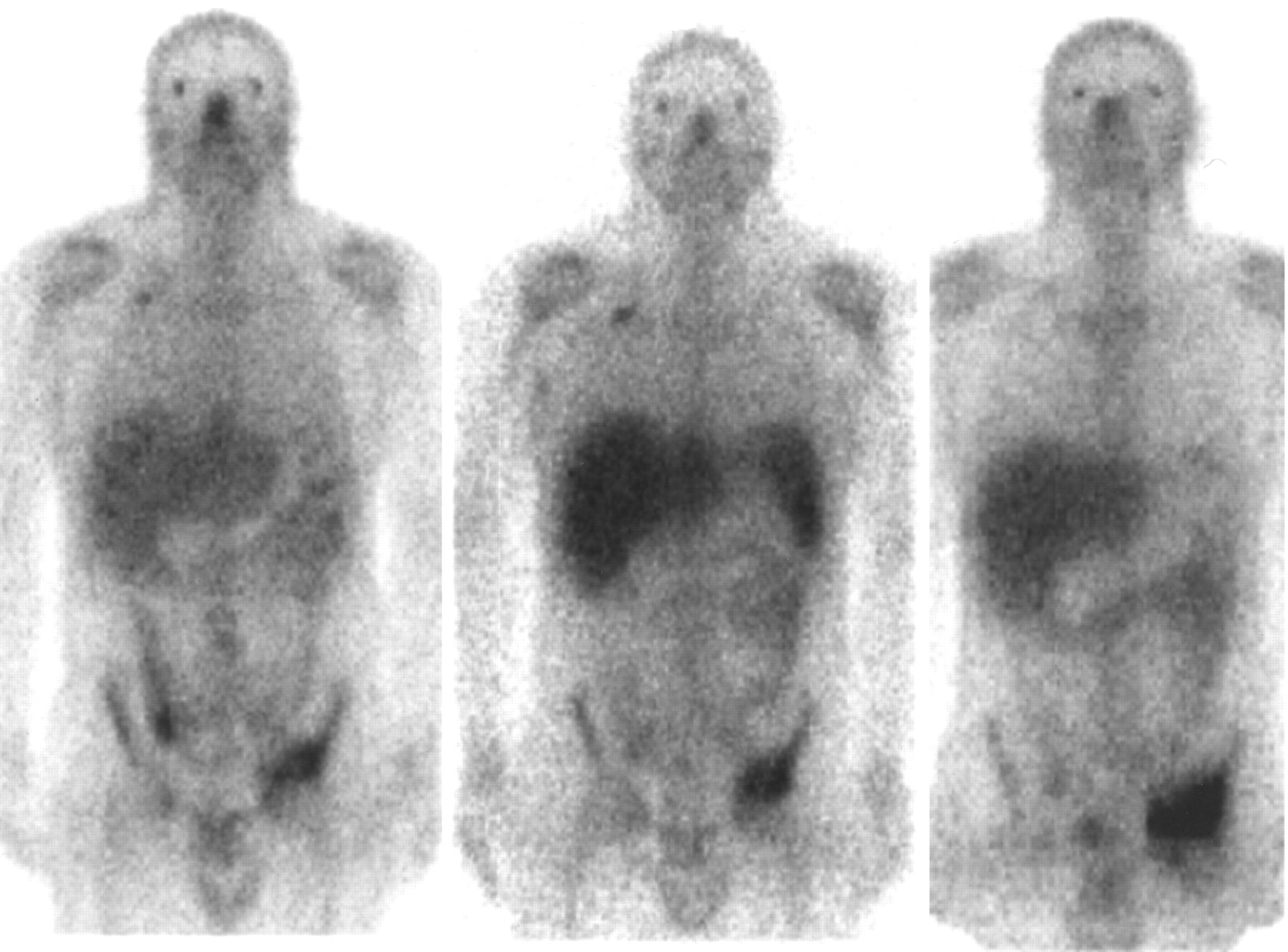
Abnormal 67Ga scintigraphy findings during and after chemotherapy in 33-y-old man with biopsy-proven recurrent HD involving left acetabulum. 67Ga scintigraphy before treatment (left) shows area of pathologic uptake in left acetabulum. Chemotherapy including dexamethasone, ifosfamide, cisplatin, and etoposide was initiated. 67Ga scintigraphy during treatment (center) and at completion of chemotherapy (right) shows increase in size and intensity of pathologic uptake. Repeated bone biopsy indicated presence of active HD. (Note also abnormal 67Ga uptake in involved right supraclavicular lymph node.) Tumor progression was diagnosed, and patient died 6 mo later.
Number of Patients with Negative and Positive 67Ga Scintigraphy and CT Findings During, at End of, and After Treatment
Three-Year FFP Rate in Lymphoma Patients with Negative and Positive 67Ga Scintigraphy and CT Findings
At diagnosis, CT of skeletal lymphoma lesions showed a predominant osteolytic pattern at 70% of sites. Predominant osteosclerotic lesions were seen in 23% of cases, whereas 7% of disease sites showed a mixed lytic and blastic pattern. CT studies performed during treatment, at the end of chemotherapy, and during follow-up showed a decrease in the percentage of osteolytic lymphoma lesions, from 70% at baseline to 21% at FU2; an increase in the number of lymphoma sites with osteosclerotic features, from 23% at presentation to 38% at 1 y after completion of treatment; and an increase in the number of lymphoma sites with a mixed lytic and sclerotic pattern, from 7% before treatment to 20% at FU2. The distribution of various CT patterns of lymphoma bone lesions in relationship to treatment and the correlation between the presence of these patterns and 67Ga avidity are shown in Table 4.
Treatment-Related Distribution of CT Patterns and Their Correlation with 67Ga Avidity
DISCUSSION
Primary lymphoma of the bone is rare and represents about 3%–5% of bone tumors and of extranodal lymphomas (9–11,19). It has been described in patients with NHL and involves mostly the appendicular skeleton. Secondary lymphomatous involvement of the skeleton is the result of hematogenous spread or direct extension from regional soft-tissue masses and may occur in both HD and NHL (9–11). Initial diagnosis of skeletal lymphoma lesions may be delayed because of a paucity of symptoms (12). At presentation, lymphoma of the bone may show several radiologic findings such as a moth-eaten osteolytic pattern, predominantly osteoblastic characteristics, or a mixed pattern of bone destruction and formation (15,25,26). MRI is highly sensitive for detection of bone lesions but lacks specificity, showing variable patterns of disease (11). Both CT and MRI provide, however, a good assessment of bone texture and of the relationship between bony lesions and their adjacent structures such as soft tissues and bone marrow, therefore allowing for accurate definition of the extent of the tumor (15–18,20).
67Ga has been used for imaging of bone lymphoma (7,11,15,21–24). Some authors have reported a high sensitivity and specificity of 67Ga scintigraphy for diagnosis of lymphoma of the skeleton (7,15,21), whereas other studies showed somewhat poorer results (22). These discordant data may have been the result of differences in radiopharmaceutical dosage and equipment used for scanning. Increased 67Ga uptake in bone may be due to skeletal lymphoma but may also occur in other areas of increased bone turnover such as epiphyseal growing plates in children, sites of previous bone biopsy, or nonlymphomatous skeletal lesions. The present study reports, however, a high sensitivity and specificity of 67Ga scintigraphy for diagnosis of bone lymphoma. Because lymphoma may involve both the axial and the peripheral skeleton, whole-body 67Ga scintigraphy including the limbs provides an additional clinical advantage. Documenting 67Ga avidity in skeletal lymphoma lesions at diagnosis is the basis for further assessment of treatment response during and after therapy.
Bone lymphoma is a tumor with a significant rate of remission and cure after treatment (12–14). Treatment options of bone lymphoma include chemotherapy, radiotherapy, or a combined multimodality approach. Knowledge of the value of the different imaging modalities in monitoring response to treatment and in predicting outcome is therefore important in clinical decision making. Early assessment of treatment response may result in an early change in the therapeutic strategy if necessary. Short- and long-term treatment-related toxicity is relatively common, especially in the pediatric patient population, and accurate and timely determination of the effect of a particular treatment is therefore of clinical significance (27,28).
Monitoring response to treatment of skeletal lesions is problematic (19,24). Although radiography and CT may show bone remodeling with reossification of lytic lesions (25), radiologic techniques have been found unreliable in assessing the effect of therapy (23). MRI may show prolonged T1 values in treated skeletal lesions (15) but has a low specificity for assessing the response of bone lymphoma to therapy (18). CT and MRI abnormalities may persist long after completion of treatment, and the differential diagnosis between residual disease and healing bone tissue is difficult (19). The definitive diagnosis of lymphomatous involvement of the skeleton at baseline is made by bone biopsy. Multiple biopsies could theoretically also represent the gold standard for evaluating response to treatment. Biopsy is, however, an invasive procedure and cannot be used repeatedly in the routine clinical work-up of patients (18,19,29).
The value of 67Ga scintigraphy for monitoring the response to treatment in lymphoma involving the lymph nodes and other soft tissues is well documented (2,30). Negative 67Ga findings at the end of treatment indicate a good response and outcome, regardless of the presence or absence of a residual mass on CT. Persistent 67Ga uptake at the end of treatment indicates the presence of active disease. 67Ga scintigraphy provides a means for early diagnosis of recurrence (6), and recent studies have shown that 67Ga scintigraphy performed early during treatment is a good predictor of prognosis and outcome (4,5).
The present data further demonstrate the role of 67Ga scintigraphy in the assessment of lymphoma involving the skeleton. During treatment, 25% of patients with bone lesions had normal 67Ga findings, whereas only 1 patient had normal CT findings. Most patients with lymphoma of the skeleton showed abnormal findings on CT even as late as 1 y after completion of treatment. At that time, 61% of patients had negative 67Ga findings, compared with only 21% of patients showing normal CT findings. Assessment of the rapidity of response using 67Ga scintigraphy for bone lymphoma is not as good as that previously reported for nodal disease (4,5). 67Ga scintigraphy is, however, a better predictor of the long-term outcome of patients with lymphoma of the skeleton than are anatomic imaging modalities such as CT. A statistically significant difference in FFP between patients with positive and negative 67Ga scintigraphy findings was found as soon as at mid treatment and thereafter. In contrast, no statistically significant difference in FFP at any time point was found between patients with positive and negative CT results. Patient outcome expressed as 3-y FFP was used as the indicator of efficacy for both 67Ga scintigraphy and CT for treatment monitoring. The significant difference in FFP between patients with positive and negative 67Ga findings early during treatment as well as during follow-up may be used in the future to tailor treatment according to the results of functional imaging modalities. Repeated bone biopsy sampling cannot be routinely performed.
Because of the variability found in CT patterns of skeletal lymphoma after treatment, the strict criterion of complete normalization of CT images was used for comparison of FFP. The lack of specific CT features in treated bone lymphoma is a diagnostic challenge further demonstrated by the present results. Although there was a decrease in the percentage of osteolytic lesions over time and an increase in the incidence of osteoblastic patterns, 1 in every 5 lymphoma lesions in the skeleton at 1 y after treatment still presents predominant features of bone destruction. At all evaluated time points, similar numbers of lytic and blastic skeletal lymphoma lesions showed 67Ga avidity despite an expected preferential 67Ga positivity in areas of bone repair. The fact that both osteosclerotic and osteolytic lymphoma lesions take up 67Ga in a similar fashion supports the hypothesis that the lymphoma-seeking properties, rather than the bone-seeking properties, of 67Ga play the primary role in uptake of this tracer in sites of active bone involvement.
PET using 18F-FDG is evolving as a sensitive and accurate method of assessing lymphoma (31). It has proven accurate for the initial diagnosis and staging of bone lymphoma (32,33). Having fewer bone-seeking properties, 18F-FDG has the potential of improving the assessment of patients with skeletal lymphoma lesions, especially for the prediction of outcome early during treatment. Possible drawbacks may be related to bone marrow uptake and its differential diagnosis from bone involvement, particularly in the axial skeleton (32,33). The development of new hybrid imaging devices combining nuclear medicine techniques with sequential CT acquisition may represent a further step in optimizing simultaneous evaluation of functional and morphologic characteristics of bone lymphoma before and after treatment (34). The role of 18F-FDG PET and hybrid imaging for monitoring the response of bone lymphoma to treatment still needs to be assessed.
CONCLUSION
67Ga scintigraphy has a high sensitivity and specificity for the diagnosis of bone lymphoma. CT may show variable patterns in patients with lymphomatous skeletal lesions at presentation, during treatment, and after treatment. In most patients with lymphoma involving the skeleton, CT findings do not become negative even at 1 y after treatment. 67Ga scintigraphy, however, may be used as a predictor of long-term outcome in patients with bone lymphoma. Tailoring and optimization of treatment in patients with bone lymphoma based on functional data provided by nuclear medicine procedures should increase the rate of successful therapy and decrease treatment-related toxicity.
Acknowledgments
The authors acknowledge Dr. Gerald M. Kolodny for his many useful suggestions during the revision of the manuscript. This study was supported by a grant from the Israel Cancer Association and the L. Rosenblatt Technion Fund for Research in Cancer.
Footnotes
Received Dec. 12, 2001; revision accepted Jun. 11, 2002.
For correspondence or reprints contact: Ora Israel, MD, Department of Nuclear Medicine, Rambam Medical Center, Haifa 35254, Israel.
E-mail: o_israel{at}rambam.health.gov.il





{kind=link}
{kind=link}
{kind=link}
{kind=link}