


Abstract
This study was undertaken to evaluate our hypothesis that most asymptomatic lower extremity uptake abnormalities are of no clinical consequence and to assess whether these findings should affect patient care. Methods: One hundred consecutive young athletes referred for bone scintigraphy by a sports medicine clinic because of low back pain were evaluated for the presence of asymptomatic bone scan abnormalities in the lower extremities. The patients were then reexamined by the referring sports medicine physician, who had full knowledge of the bone scan results. Scintigraphic findings were correlated with the clinical evaluation at the time of scintigraphy and on follow-up evaluations ranging from 8 to 14 mo later. Results: Asymptomatic lower extremity abnormalities were present in 34% of patients. There were abnormalities of the feet in 30 patients (focal uptake in 26 patients, diffuse uptake in 10 patients), the tibia in 13 patients (2 focal uptake, 11 diffuse uptake), and the femur in 2 patients (both with diffuse uptake). None of the regions of abnormal lower extremity uptake was symptomatic at the time of initial evaluation. There was no change in the clinical management of any patient because of the scan findings. None of the patients was advised to restrict the activity level because of the asymptomatic scan findings. None of the regions of scan abnormality became symptomatic on follow-up evaluation. Conclusion: This study shows that asymptomatic bone scintigraphic abnormalities of the feet, as well as diffuse abnormalities of the tibia, are common in young athletes. These findings are most likely of no clinical consequence and do not require a change in the activity level. Focal abnormalities of the femur or tibia are not commonly seen in asymptomatic young athletes.
Skeletal scintigraphy is generally recognized as the gold standard in the evaluation of suspected stress injuries because of its high sensitivity for stress fracture detection and its ability to show abnormalities in bone metabolism well before they are manifested radiographically (1). Demonstration of abnormal uptake at a symptomatic site in an athlete is useful to identify patients with significant stress-related injuries that require intervention to prevent more serious injury. Treatment usually consists of a restriction in the activity level, but occasionally immobilization with a cast is necessary. Normal skeletal scintigraphy is used to exclude stress fracture (2). Its sensitivity for this diagnosis approaches 100%, and skeletal scintigraphic findings have been falsely negative in only rare published reports (1).
During the evaluation of a symptomatic region, asymptomatic sites of increased uptake may be identified in 40% or more of athletes referred for skeletal scintigraphy (2,3). There is no universal agreement about the significance of these asymptomatic abnormalities. Some authors have attributed incidental uptake to functional adaptive bone remodeling that can be disregarded for clinical purposes (4,5). Others believe that even asymptomatic uptake should be considered early evidence of a possible impending fracture (1,6). Some have suggested that all otherwise unexplained lower extremity uptake abnormalities in physically active individuals represent stress fractures (2,3). Other authors believe that asymptomatic uptake abnormalities are indicative of bone strain (7) and do not necessarily warrant treatment (8).
The purpose of this study is to assess the clinical significance of asymptomatic lower extremity uptake abnormalities in young athletes.
MATERIALS AND METHODS
The patient population consisted of 100 patients (65 females, 35 males; age range, 10–33 y; mean age, 17.5 y), who were referred consecutively for skeletal scintigraphy after being evaluated for low back pain at a sports medicine clinic. Patients were involved in a variety of recreational or competitive athletic activities at differing levels. None of the patients had a known underlying disease.
Skeletal scintigraphy was performed 3–4 h after the administration of 99mTc-methylene diphosphonate (7.4 MBq/kg, to a maximum of 740 MBq) using a large field-of-view gamma camera equipped with a high-resolution collimator. Standard imaging included anterior planar spot images of the spine, pelvis, and lower extremities, lateral images of the feet and ankles, and SPECT images of the lumbosacral spine. Additional images were obtained at the discretion of the interpreting physician.
Sites of abnormally increased uptake in the lower extremities were noted. The pattern of abnormal uptake was characterized as focal or diffuse and was graded as mild or moderate by consensus of two nuclear medicine specialists (Fig. 1). The referring physician, a sports medicine specialist, reevaluated the patient with knowledge of these results after skeletal scintigraphy had been completed. Follow-up of all patients was in the sports medicine clinic because of their presenting back pain. The duration of follow-up ranged from 8 to 14 mo. On follow-up evaluation, the presence or absence of symptoms in the lower extremities was noted.

(A) Anterior image of feet shows focal area of increased uptake in left foot graded as moderate uptake. (B) Anterior image of feet shows diffuse increased uptake bilaterally in midfeet graded as mild uptake.
RESULTS
Asymptomatic sites of increased tracer uptake were identified in the lower extremities of 34 patients (34%). More than one abnormality was present in 21 of these patients. Thirteen patients had bilateral lower extremity findings. Uptake abnormalities in the feet were most common and were present in 30 patients, 26 of whom had focal abnormalities (5 bilateral) and 10 of whom had diffuse abnormalities (7 bilateral). Six patients had focal and diffuse abnormalities. Table 1 and Table 2 summarize the anatomic localization and grade of uptake abnormalities in the feet.
Localization and Grade of Focal Tracer Uptake in Feet
Localization and Grade of Diffuse Tracer Uptake in Feet
Asymptomatic tibial uptake abnormalities were found in 13 patients. These consisted of diffuse diaphyseal increased uptake (Fig. 2) in 11 patients (8 bilateral) and unilateral focal sites of increased uptake in 2 patients. The diffuse tibial uptake abnormalities were graded as mild in 9 patients and moderate in 2 patients. One focal tibial abnormality involved the posterior diaphysis and was graded as mild (Fig. 3). The other involved the anterior cortex and was graded as moderate (Fig. 4). The only other abnormalities encountered were diffusely increased femoral diaphyseal uptake of a mild degree in 2 patients.
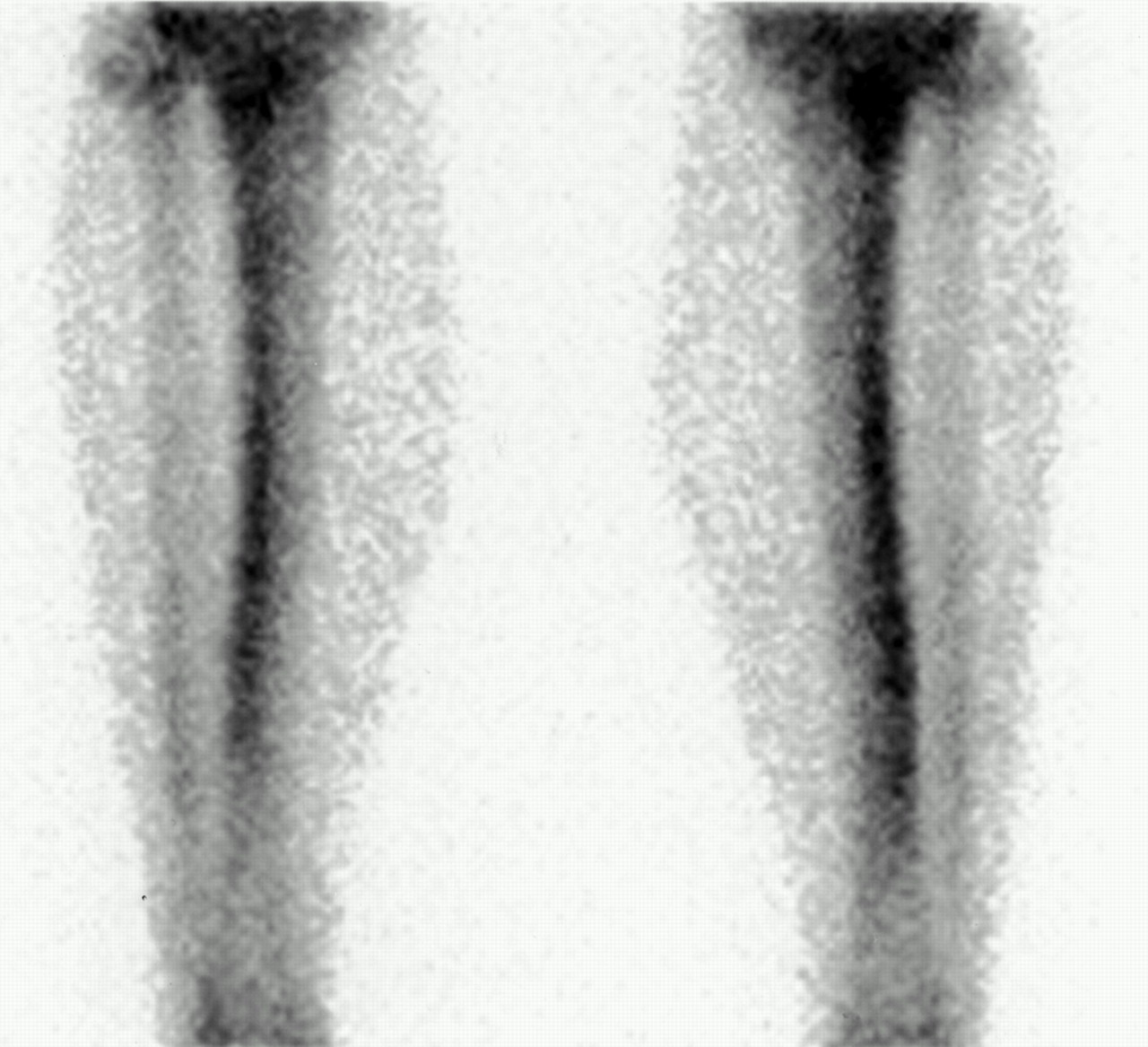
Anterior view of tibias shows bilateral mild diffuse increased uptake.

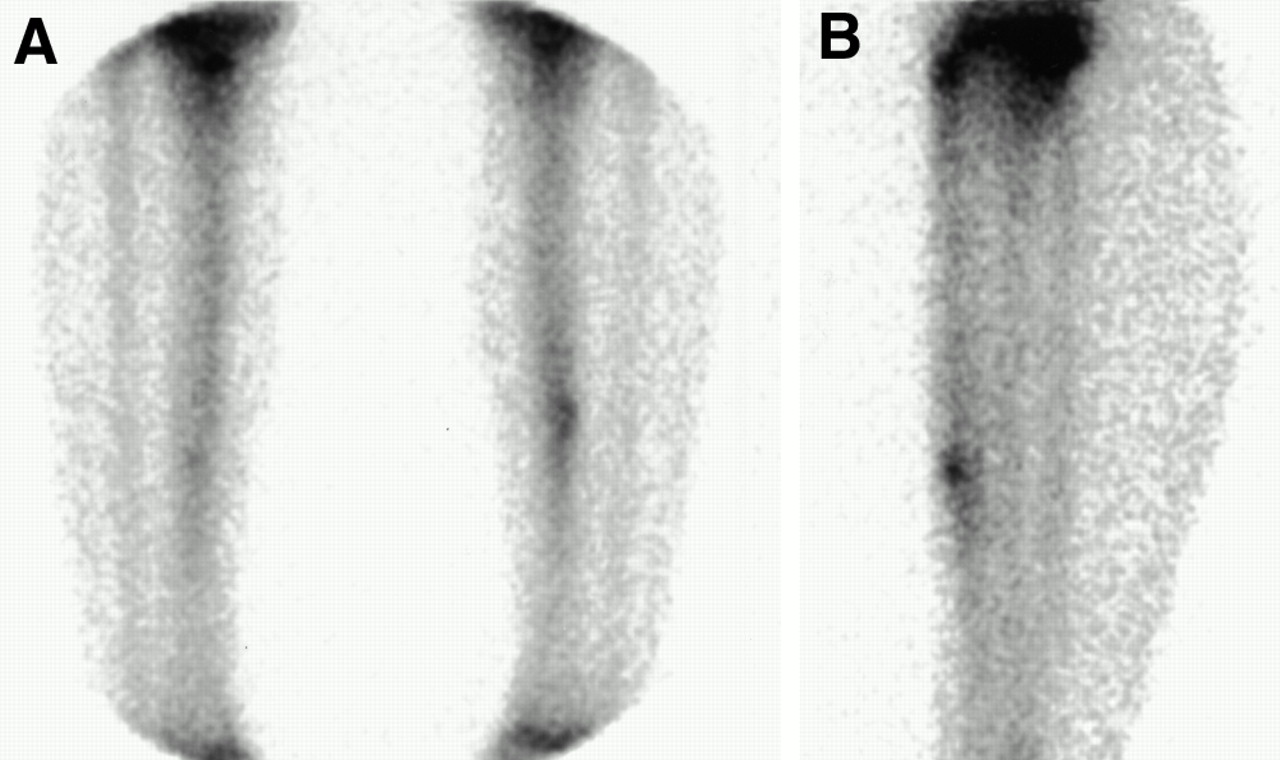
(A) Anterior views of tibias show focal increased uptake in mid tibia graded as mild uptake. (B) Lateral views show focal uptake in posterior cortex of tibia.
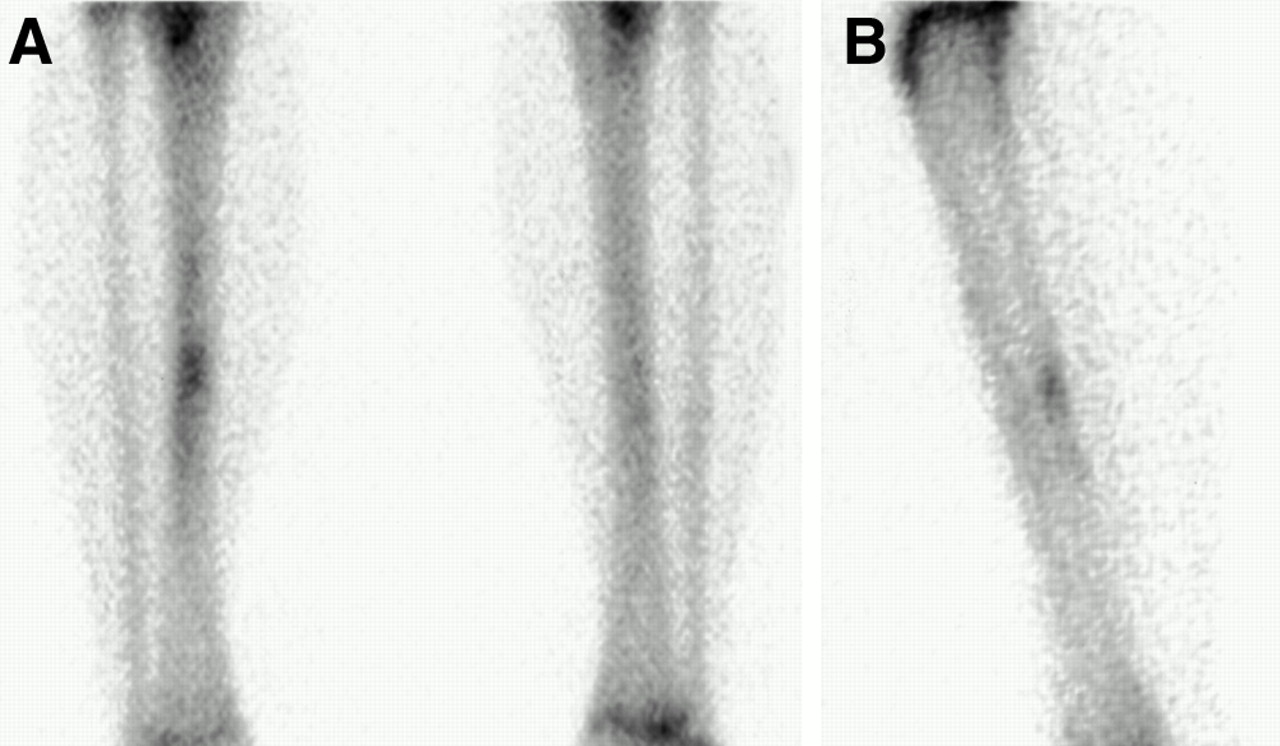
(A) Anterior views of tibias show focal increased uptake in mid tibia graded as moderate uptake. (B) Lateral views show focal uptake in anterior cortex of tibia.
Clinical examination directed at assessing the asymptomatic uptake abnormalities did not yield any previously unreported clinical complaints or reveal any physical findings to correlate with the scintigraphic abnormalities. There was only one case in which the scan findings prompted further radiologic evaluation. This patient had a focal anterior tibial abnormality that was graded moderate in intensity. His radiographs showed cortical thickening in the region of the scintigraphic abnormality. In the absence of clinical complaints or physical findings on direct examination, this finding was attributed to an unsuspected but healed stress fracture.
Clinical management was not affected by scintigraphic findings in any patient. Symptoms did not develop at any site of asymptomatic uptake abnormalities during follow-up ranging from 8 to 14 mo.
Among the 34 patients with asymptomatic uptake abnormalities, 11 patients, including the patient with the anterior tibial uptake abnormality, had scintigraphic evidence of pars interarticularis stress. In the other 23 patients with lower extremity abnormalities, planar imaging and SPECT of the spine revealed normal findings.
DISCUSSION
The frequency of asymptomatic lower extremity uptake abnormalities (34%) in the 34 patients is similar to that described in other reports (2,3). No patient became symptomatic in the region of scintigraphic abnormality. Clinical management was not altered by the presence of these abnormalities.
The absence of morbidity associated with the clinical decision to disregard asymptomatic lower extremity uptake abnormalities supports the premise that they represent functional adaptive bone remodeling. This remodeling results from the repetitive submaximal musculoskeletal loading that is required to build and sustain strength and endurance. During athletic training, altered biomechanical stress on the skeleton triggers a coordinated response that involves bone resorption, mediated by osteoclasts, and bone repair and hypertrophy, mediated by osteoblasts (4,5,7,9). Therefore, asymptomatic scintigraphic abnormalities can be regarded as reflecting a spectrum of adaptive changes that occur in bone subjected to stress (4,5,7,9,10).
Bone most often adapts to stress with proper internal remodeling, and a complete fracture does not develop. Stress-induced remodeling strengthens bone architecture to optimally withstand a particular stress. However, when an imbalance in favor of osteoclastic resorption exists, weakening of the bone predisposes to complete fracture (11). Scintigraphic uptake mirrors the new bone formation that is part of this remodeling process but provides little information about the degree of bone resorption.
The most important clinical information that might be provided by the bone scan would be to predict whether a stress injury has overwhelmed the reparative mechanism, thus suggesting that progression to a complete fracture is likely. The literature provides little guidance on this point. Our results suggest that such progression is not likely, even in the absence of clinical intervention directed at reducing the repetitive stress.
The results of this study may not be applicable to all clinical settings. In this series, most asymptomatic scintigraphic findings in the tibia consisted of diffuse uptake. Most focal abnormalities were located in the feet. Only two focal tibial abnormalities and no asymptomatic focal femoral abnormalities were found. It may not be possible to extrapolate our results to focal abnormalities in the tibia or femur. No focal abnormalities suggestive of femoral stress fractures were found in this series. It should be emphasized that femoral neck stress fractures, which can be quite insidious in their presentation, are an injury with significant potential morbidity (12,13). Even asymptomatic focal femoral neck uptake abnormalities may require aggressive management. Another abnormality that may need more attention is moderate asymptomatic focal anterior tibial uptake because anterior tibial stress fractures are prone to nonunion and avascular necrosis and are at higher risk of becoming displaced than are posterior tibial stress fractures (14,15).
In addition, there is evidence that the intensity of a focal scan abnormality may be an important determinant of its significance. Zwas et al. (2) showed that, in the tibia, intense focal uptake with a well-defined elongated or fusiform appearance was more likely to become radiographically evident than was less intense uptake. Thus, the lack of clinical significance of minor uptake abnormalities may not be predictive of the significance of more intense uptake. Intense uptake of the magnitude seen in an actual fracture was not found in any patient in our study. Most tibial abnormalities in our series were diffuse rather than focal. This diffuse pattern of uptake was similar to that seen frequently in symptomatic individuals and that has been attributed to periostitis incited by the soleus or posterior tibialis muscles (or both) and labeled as the medial tibial stress or soleus syndrome (16–18).
It was not possible to determine from our data why few cases of high-grade uptake or focal tibial or femoral abnormalities were found. It is possible that intense focal abnormalities are more likely to be symptomatic than are less intense findings.
A second potential limitation of this study is that modifications of activity necessitated by the patient’s presenting back pain could have lessened the likelihood that the lower extremity scintigraphic abnormalities might progress and become symptomatic. Of the 34 patients with lower extremity abnormalities, 23 (67%) did not have abnormalities of the spine, suggesting that valid conclusions can be drawn from the data.
Despite these potential limitations, our results suggest that asymptomatic focal or diffuse uptake in the feet and diffuse uptake in the tibia do not require a modification in activity or a change in clinical management. This is not to suggest, however, that these findings should be ignored. Because symptoms and clinical signs are considered in establishing the significance of uptake abnormalities in athletes (8,19) and because dedicated athletes are often motivated and encouraged to disregard pain, unsuspected scintigraphic findings should be correlated with direct clinical questioning and examination to confirm that the athletes are truly asymptomatic.
CONCLUSION
Bone scintigraphy in young athletes commonly shows asymptomatic regions of increased uptake in the lower extremities. The common patterns of abnormality consist of diffuse tibial uptake and focal and diffuse uptake in the feet. These asymptomatic regions of uptake did not progress to symptomatic findings in any patient and, therefore, are unlikely to be clinically significant.
Footnotes
Received Jun. 15, 2000; revision accepted Sep. 14, 2000.
For correspondence or reprints contact: Laura A. Drubach, MD, Division of Nuclear Medicine, Children’s Hospital, 300 Longwood Ave., Boston, MA 02115.
REFERENCES
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Diagnostic accuracy of MRI for identifying posterior element bone stress injury in athletes with low back pain: a systematic review and narrative synthesis
- Skeletal Scintigraphy of Young Patients with Low-Back Pain and a Lumbosacral Transitional Vertebra
- Clinical Spectrum of Asymptomatic Femoral Neck Abnormal Uptake on Bone Scintigraphy