


Abstract
64Cu (half-life, 12.7 h; β+, 0.653 MeV [17.4%]; β−, 0.579 MeV [39%]) has shown potential as a radioisotope for PET imaging and radiotherapy. 111In-diethylenetriaminepentaacetic acid (DTPA)-d-Phe1-octreotide (OC) was developed for imaging somatostatin-receptor–positive tumors using conventional scintigraphy. With the advantages of PET over conventional scintigraphy, an agent for PET imaging of these tumors is desirable. Here, we show that 64Cu-TETA-OC (where TETA is 1,4,8,11-tetraazacyclotetradecane-N,N′,N′′,N′′′-tetraacetic acid) and PET can be used to detect somatostatin-receptor–positive tumors in humans. Methods: Eight patients with a history of neuroendocrine tumors (five patients with carcinoid tumors and three patients with islet cell tumors) were imaged by conventional scintigraphy with 111In-DTPA-OC (204–233 MBq [5.5–6.3 mCi]) and by PET imaging with 64Cu-TETA-OC (111 MBq [3 mCi]). Blood and urine samples were collected for pharmacokinetic analysis. PET images were collected at times ranging from 0 to 36 h after injection, and the absorbed doses to normal organs were determined. Results: In six of the eight patients, cancerous lesions were visible by both 111In-DTPA-OC SPECT and 64Cu-TETA-OC PET. In one patient, 111In-DTPA-OC showed mild uptake in a lung lesion that was not detected by 64Cu-TETA-OC PET. In one patient, no tumors were detected by either agent; however, pathologic follow-up indicated that the patient had no tumors. In two patients whose tumors were visualized with 111In-DTPA-OC and 64Cu-TETA-OC, 64Cu-TETA-OC and PET showed more lesions than 111In-DTPA-OC. Pharmacokinetic studies showed that 64Cu-TETA-OC was rapidly cleared from the blood and that 59.2% ± 17.6% of the injected dose was excreted in the urine. Absorbed dose measurements indicated that the bladder wall was the dose-limiting organ. Conclusion: The high rate of lesion detection, sensitivity, and favorable dosimetry and pharmacokinetics of 64Cu-TETA-OC indicate that it is a promising radiopharmaceutical for PET imaging of patients with neuroendocrine tumors.
Targeting of somatostatin receptors (SSRs) in tumors has been a goal in cancer treatment and diagnosis since the 1980s. The somatostatin analog octreotide (OC) has been labeled with 123I (1) and 111In (2) and used to image SSR-positive tumors in humans (3) by conventional scintigraphy. 123I-Tyr3-OC has a high hepatobiliary excretion that hinders visualization of tumors in the abdomen, whereas 111In-diethylenetriaminepentaacetic acid (DTPA)-d-Phe1-OC clears primarily through the kidneys (3) and is currently used routinely as an imaging agent for neuroendocrine tumors. Because of the limited sensitivity and resolution of SPECT, we are interested in designing a positron-emitting agent for PET imaging of SSR-positive tumors. Using OC labeled with a positron-emitting radionuclide and PET, tracer accumulation within tissues can be quantitatively assessed, potentially offering improvements over SPECT when quantitative results are needed and when tumors are small or deep within the body.
An attractive radionuclide for PET imaging is 64Cu (half-life, 12.7 h; 39% β− [0.579 MeV]; 17.4% β+ [0.653 MeV]; 43.6% electron capture). 64Cu can be produced by either a reactor (4) or a medical cyclotron (5). Recently, a method was developed at Washington University School of Medicine to produce large quantities of 64Cu (up to 37 GBq) on demand using a biomedical cyclotron (5). 64Cu also has shown potential as a therapeutic radionuclide. In radioimmunotherapy studies, we showed that 64Cu-labeled monoclonal antibody 1A3 caused complete tumor regression with no regrowth of tumors in a well-established animal model (6,7).
We showed that 64Cu-TETA-OC (where TETA is 1,4,8,11-tetraazacyclotetradecane-N,N′,N′′,N′′′-tetraacetic acid) had a similar biodistribution to 111In-DTPA-OC in a tumor-bearing rat model (8). In targeted radiotherapy studies, 64Cu-TETA-OC inhibited the growth of tumors in the same tumor-bearing rat model (9). PET imaging of tumors using low doses of 64Cu-TETA-OC could also be used to determine individual absorbed doses before therapy with either 64Cu- or 67Cu-labeled OC. For these reasons, we are investigating 64Cu-TETA-OC as a PET imaging agent for patients with neuroendocrine tumors.
In this study, we compared 64Cu-TETA-OC and PET with 111In-DTPA-OC and conventional scintigraphy in eight patients with a history of neuroendocrine tumors. The blood and urine clearance of 64Cu-TETA-OC was determined, and absorbed doses to normal organs were measured from the PET images.
MATERIALS AND METHODS
Preparation of 64Cu-TETA-OC
64Cu-TETA-OC was prepared in compliance with guidelines established by the Washington University Radioactive Drug Research Committee. 64Cu was produced on a biomedical cyclotron (5). The specific activity of 64Cu ranged from 222,000 to 1,850,000 GBq/mmol. TETA-OC was prepared as previously described (9). 64Cu was labeled to TETA-OC as previously described (8). Briefly, 64Cu-acetate (370 MBq [10 mCi]) was labeled to 10 μg TETA-OC in 0.1 mol/L ammonium acetate buffer, pH 5.5. Gentisic acid (1 mg) was added to the radiolabeled conjugates to reduce the effects of radiolysis. The preparations were purified by a C18 SepPak (Waters, Milford, MA) to remove uncomplexed 64Cu-acetate. 64Cu-TETA-OC was sterile filtered with a 0.22-μ Millex GV (Millipore, Bedford, MA) before injection. Radiochemical purity was assessed by radio–thin-layer chromatography (Bioscan, Inc., Washington, DC), using reversed-phase C18 plates developed in 70:30 methanol:5% ammonium acetate, and by reversed-phase high-performance liquid chromatography (Waters). Patients received an injection of 107–130 MBq (2.9–3.5 mCi) (3–5 μg) 64Cu-TETA-OC.
111In-DTPA-OC was prepared using the OctreoScan kit provided by the manufacturer (Mallinckrodt, Inc., St. Louis, MO). Patients received an injection of 204–233 MBq (5.5–6.3 mCi) 111In-DTPA-OC labeled to 10 μg DTPA-OC.
Patients
Patients who were scheduled for routine imaging with 111In-DTPA-OC were eligible for 64Cu-TETA-OC and PET. Eight patients (six men, two women; age range, 45–70 y) with a history of neuroendocrine tumors who were being evaluated with 111In-DTPA-OC as part of their routine clinical evaluation also underwent PET with 64Cu-TETA-OC at our institution. This investigation was approved by the Human Studies Committee and the Radioactive Drug Research Committee at Washington University School of Medicine. Each patient gave informed consent before participating in the study. In all patients but one, the 111In-DTPA-OC was administered before 64Cu-TETA-OC. The time between administration of 111In-DTPA-OC and 64Cu-TETA-OC ranged from −1 to 40 d (mean time, 14 d).
Imaging
PET imaging was performed with an ECAT EXACT scanner (Siemens/CTI, Knoxville, TN). Single-photon imaging was also performed on each patient using a dual-head Genesys scanner (ADAC Laboratories, Milpitas, CA) fitted with medium-energy collimators. Conventional scintigraphy was performed after injection of 204–233 MBq (5.5–6.3 mCi) 111In-DTPA-OC. All patients underwent whole-body planar scintigraphy at 4 and 24 h. The whole-body planar study consisted of anterior and posterior views proceeding from head to toe at 6 cm/min. All but one patient underwent SPECT (imaging of the chest and abdomen at 24 h in one patient and at 4 and 24 h in one patient; imaging of only the abdomen at 24 h in two patients, at 4 h in one patient, and at 4 and 24 h in two patients). Full-field SPECT was performed without attenuation correction on the chest and abdomen for 20 min each. On a separate day, PET was performed after intravenous injection of approximately 111 MBq (3.0 mCi) 64Cu-TETA-OC in an antecubital vein. Delay intervals ranging from 0 to 24 h between injection and imaging were evaluated, from which an optimal delay of 4–5 h was selected as providing the best combination of image quality and lesion-to-background contrast. Five of the eight PET studies were performed to estimate the radiation dosimetry of 64Cu-TETA-OC. In these patients, the entire torso was scanned to allow complete determination of the activity biodistribution throughout the body. In the other three patients, only a single bed position was used, covering 16 cm axially around the suspected tumor region. At each bed position, the study consisted of static (if delayed) or dynamic (if at injection) data acquisition, 20 min in duration, followed by a 2- to 3-min transmission scan. From the transmission scan, segmented attenuation maps were derived (10) and used to apply full attenuation correction to the emission image volume. PET and SPECT images were reconstructed using filtered backprojection (Hanning filter, cutoff of 0.8 Nyquist) and were volume rendered for cinegraphic viewing.
The 111In-DTPA-OC and 64Cu-TETA-OC images were examined qualitatively. The criteria for interpretation were those routinely used in scintigraphic imaging. The PET images were examined by a nuclear medicine physician, and the interpretation of the images was based on knowledge of normal biodistribution of 64Cu-TETA-OC derived from animal models. Foci of abnormal radiotracer uptake were recorded on a four-point scale (0 = no uptake; + = mild uptake; ++ = moderate uptake; and +++ = intense uptake).
Measurement of 64Cu Activity in Blood and Urine of Patients
64Cu activity in the blood and urine was measured in a gamma counter (Beckman, Arlington Heights, IL) containing a NaI crystal. Two blood samples were drawn per patient at times ranging from 1.5 to 22 h after injection of 64Cu-TETA-OC. Urine was collected from patients (from two to six samples per patient) at times ranging from 1.5 to 27 h after injection.
Human Absorbed Dose Measurements from Patient PET Images
For evaluation of biodistribution and calculation of dosimetry, five of the eight PET studies involved imaging the chest and abdomen at different times (0 and 4 h in two patients, 5 and 24 h in two patients, and 5 h in one patient) after administration of 64Cu-TETA-OC. All but one of the patients were imaged twice.
Activity was observed mainly in the liver, spleen, kidneys, bladder, and tumors. Regions of interest (ROIs) were drawn on the PET images of the five dosimetry study patients to measure the total activity in these organs. For the liver, the average activity concentration was calculated from ROIs traced inside and encompassing most of the organ for five to six adjacent slices. The average activity concentration in the liver was then multiplied by the estimated liver volume. For the other visible organs, ROIs were drawn around the entire organ. The total activity in these organs was thus directly measured. In addition, ROIs were traced around the heart to evaluate the activity concentration in the blood. The blood activity concentration was measured by the average maximum value in the slices containing the lower left ventricle. Finally, elliptic ROIs were drawn in several adjacent slices of the lower abdomen beside the bladder to measure the average soft-tissue activity concentration. The red marrow activity concentration, Arm, was calculated from the blood activity concentration, Abl, in proportion to the mass of the red marrow, mrm, and assuming a hematocrit value of 39%, as follows (11): Arm = Ablmrm0.19/(1 − 0.39).
Measurements were repeated for each time point. The percentage of injected activity in each organ immediately after the injection (at to+) was calculated from its estimated blood volume. This decision was based on the assumption that the bolus of activity distributes uniformly throughout the body immediately after the injection. The fractions of injected activity at to+ were 4.9% for the liver, 5.9% for the lungs, 1.5% for the spleen, 1.4% for the kidneys, 3.7% for the bones, and 10% for the heart.
A time–activity curve was drawn for each organ combining the data from all patients. The measured organ activities were corrected for decay to the time of the start of the scan to simplify the subsequent fitting procedure. The time–activity curves were fitted with a sum of one or two exponentials in which the parameters were determined by a least squares minimization procedure. The fitted functions were then integrated analytically (including physical decay) to give the residence times. Dose calculation was performed by the MIRD methodology in which the S values were calculated with the MIRDOSE3.0 program using the adult male model. Along with any unaccounted activity, the soft-tissue activity and 72% of the blood activity were assigned to the remainder of the body as a MIRD source organ. Although some activity was seen to accumulate in the tumors, this contribution could not be included under the MIRD scheme. Instead, the tumor activity was assumed to be distributed uniformly throughout the body. An uptake function was fitted to the time-cumulated urine data from all patients. The absorbed fraction and the filling half-time were used in the MIRDOSE3 bladder model (12) along with a voiding period of 4 h to obtain the residence time of the bladder contents.
Human Absorbed Dose Estimates from Baboon PET Images
The biodistribution of 64Cu-TETA-OC was also determined in a 25-kg male baboon by PET imaging. This study was performed in compliance with the Guidelines for the Care and Use of Research Animals established by the Animal Studies Committee of Washington University School of Medicine. Images of the animal’s torso were acquired at approximately 30-min intervals from 0 to 3 h and then again at 24 h after injection. The baboon was anesthetized with isoflurane during the first 3-h imaging session and then was allowed to recover. The baboon was placed in approximately the same position the following day, anesthetized with isoflurane, and imaged for 30 min. Activity concentration values were derived from the PET images as previously described (13). The absorbed fraction and filling half-time were used in the MIRDOSE3 bladder model (12) along with a voiding period of 4 h to obtain the residence time of the bladder contents.
Blood samples were collected from the baboon at 6, 20, 40, 60, and 120 min after injection of 64Cu-TETA-OC. The percentage injection dose (%ID) in the blood at those times was determined, and the data were used to determine blood clearance.
RESULTS
Radiochemistry
64Cu-TETA-OC was prepared in greater than 95% radiochemical purity as shown by radio–thin-layer chromatography and radio–high-performance liquid chromatography.
Absorbed Dose Estimates from Baboon Imaging
PET imaging of a nonhuman primate was performed to estimate the human absorbed doses before beginning human PET imaging studies. The estimated human absorbed doses from the baboon PET images, in comparison with estimated human absorbed doses from rat biodistribution data (9), are listed in Table 1. The baboon PET data suggest that the dose-limiting organ is the bladder wall (0.17 mGy/MBq [0.62 rad/mCi]), followed by the kidneys (0.13 mGy/MBq [0.49 rad/mCi]). The largest discrepancy between dosimetry calculated from rats to baboons is in the intestinal absorbed doses. Rodents show excretion patterns significantly different from those of primates, and this fact is indicated by the data.
Estimated Human Absorbed Doses of 64Cu-TETA-OC to Normal Organs Using Biodistribution Data from Rats and PET Data from Baboons and Humans
Patient Imaging Studies
The clinical and pathologic features of the eight patients are outlined in Table 2. All patients had histologically proven neuroendocrine tumors. Five patients had proven carcinoid tumors of the gastrointestinal tract, and three had pancreatic islet cell tumors.
Clinical, Imaging, and Histopathologic Patient Data
Abnormal foci of increased 64Cu-TETA-OC and 111In-DTPA-OC accumulation were seen in seven of the eight patients. These foci of increased activity were detected in several locations: small or large bowel (three patients), stomach (one patient), liver (four patients), pancreas (two patients), skin (one patient), abdominal and pelvic nodes (four patients), lung (one patient), and bone (two patients). The results of 64Cu-TETA-OC PET were, in general, similar to those of 111In-DTPA-OC and conventional scintigraphy (Figs. 1 and 2). One patient (patient 6, Fig. 2) showed osseous involvement in addition to the small-bowel lesions on 64Cu-TETA-OC PET. In two patients, more than one lesion was observed in the small bowel and bone with both agents (patients 2 and 6), and 64Cu-TETA-OC PET detected more lesions than did 111In-DTPA-OC imaging (Figs. 1 and 2). Although image contrast was better on 64Cu-TETA-OC PET, in some cases the image quality was better with 111In-DTPA-OC because of absence of intense activity in the kidneys and bladder. 64Cu-TETA-OC PET was falsely negative in a patient with a lung lesion, which showed uptake on the 111In-DTPA-OC scan. Disease seen with 64Cu-TETA-OC PET and 111In-DTPA-OC conventional scintigraphy was confirmed by a combination of histologic, radiologic, and clinical follow-up of the patients.
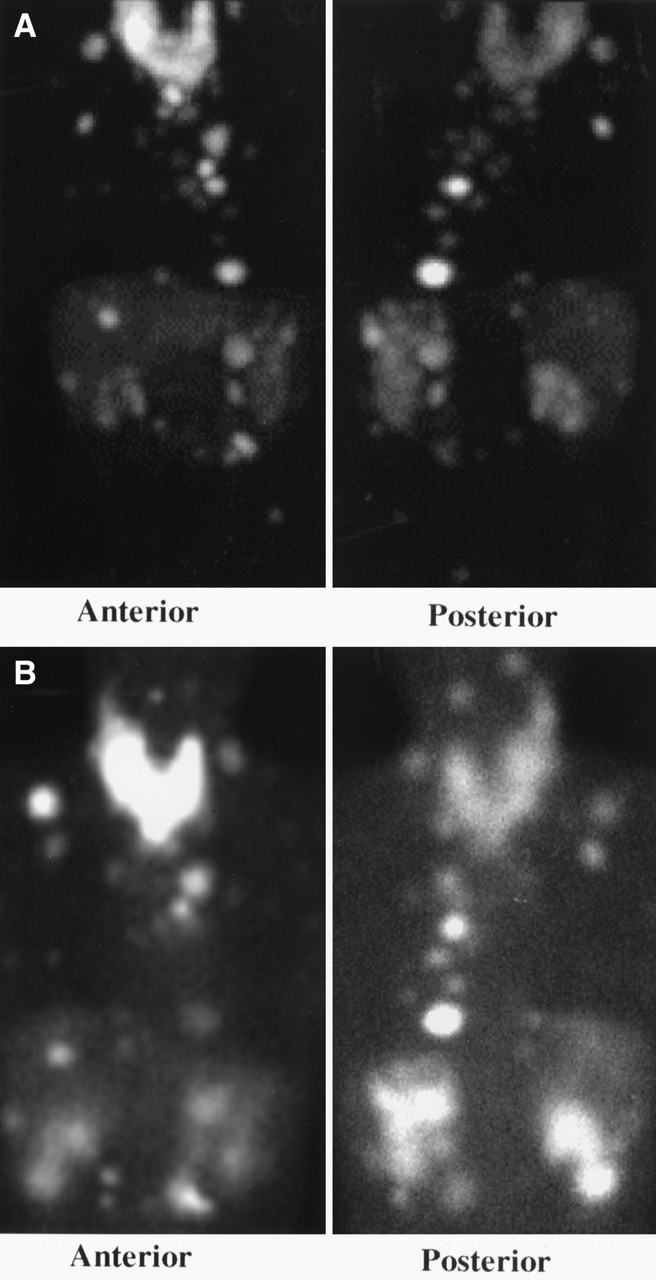
Anterior and posterior volume-rendered maximum pixel activity reprojected images of 64Cu-TETA-OC PET (A) vs. anterior and posterior planar images of 111In-DTPA-OC (B) throughout neck, chest, and abdomen of patient 2, 45-y-old man with numerous metastatic foci of carcinoid tumor. Images were obtained 4 h after injection.
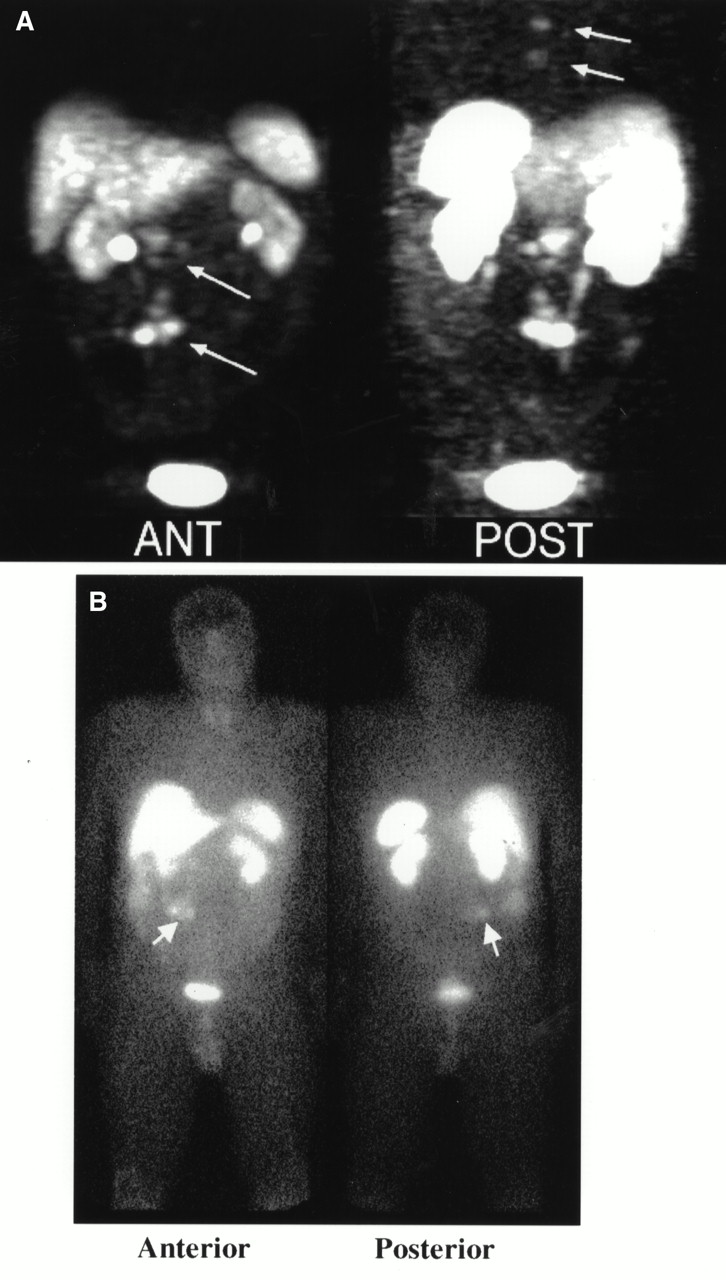
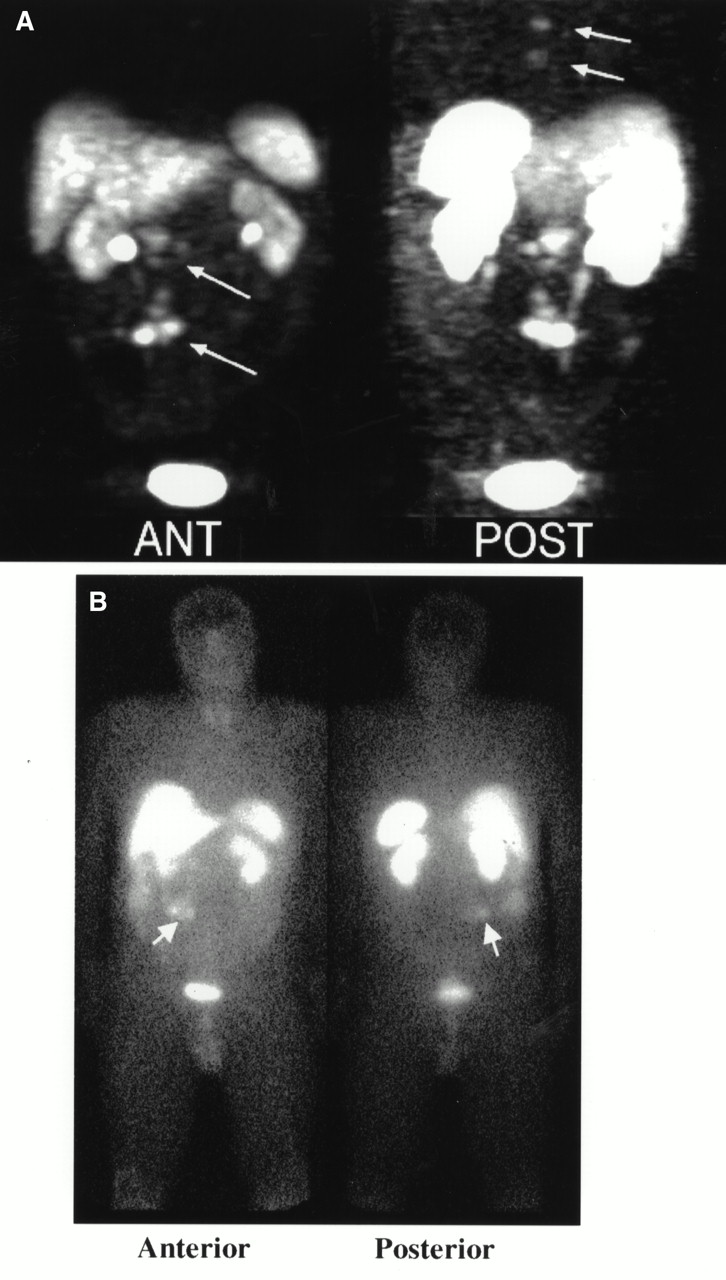
Anterior and posterior volume-rendered maximum pixel activity reprojected neck, chest, and abdomen images of 64Cu-TETA-OC PET (A) vs. anterior and posterior whole-body planar images of 111In-DTPA-OC (B) of patient 6, both obtained at 4 h after injection. Arrows in anterior image of (A) show abdominal carcinoid lesions, whereas posterior view of (A) shows osseous lesions. Arrows in anterior and posterior views of (B) indicate abdominal carcinoid tumors.
Mild to moderate blood-pool activity was present on images obtained immediately after tracer administration, with only faint blood-pool activity seen thereafter. Adrenal glands were visualized in three of eight patients (patients 1, 2, and 7) with 64Cu-TETA-OC PET. SSRs have been reported to be present in normal human adrenal glands as well as in malignant pheochromocytomas (14). No activity was seen in the gallbladder. Bowel activity was not present on early images but appeared faintly after 2 h and became more intense (mild to moderate) at 21–24 h after injection. Hepatic uptake was less than splenic uptake on the early images and became more intense with time, with the liver exhibiting activity similar to that in the spleen on delayed images. The renal collecting systems and bladder had high uptake at early times but became less intense on delayed images. Lesions were more clearly visualized on the early images than on the delayed images. The best imaging time appeared to be approximately 4–6 h after tracer injection.
Pharmacokinetic Analysis
Blood samples were obtained from patients during their imaging sessions. 64Cu-TETA-OC cleared rapidly from the blood. The amount in the blood varied from patient to patient; however, by 4 h after injection, 7.9 ± 3.7 %ID remained (range, 3.2–13.5 %ID). From 6 to 22 h after injection, the activity in the blood decreased further, with the amount in the blood ranging from 0.8 to 6.6 %ID (mean, 3.3 ± 2.3 %ID). The large differences in blood-pool data are most likely related to patient-to-patient variation, possibly because of differing tumor burden. Urine excretion also varied between patients. During the first 4 h after injection, the amount excreted in the urine was 44.6 ± 10.6 %ID, and the amount during 27 h was 63.7 ± 18.6 %ID.
Human Dosimetry from Patient PET
Using PET data from five patients, the absorbed doses of 64Cu-TETA-OC to the normal organs were measured. Time–activity curves are shown in Figure 3. Residence times were determined for seven tissues in which most of the 64Cu activity was localized, and they are listed in Table 3. From these data, the absorbed doses listed in Table 1 were determined. Residence times measured in the organs listed in Table 3 account for 35% of the maximum residence time, whereas 47% of activity was excreted in the urine. As predicted from the estimated absorbed doses from the rodent and baboon PET data, the human PET data indicate that the bladder wall is the dose-limiting organ, with an absorbed dose of 0.25 mGy/MBq (0.94 rad/mCi). This dose was calculated assuming emptying of the bladder at 4 h after injection. Other organs with higher absorbed doses include the liver (0.092 mGy/MBq [0.34 rad/mCi]), kidneys (0.078 mGy/MBq [0.29 rad/mCi]), and spleen (0.070 mGy/MBq [0.26 rad/mCi]). The intestinal dose was relatively low, as was the dose to the bone marrow.

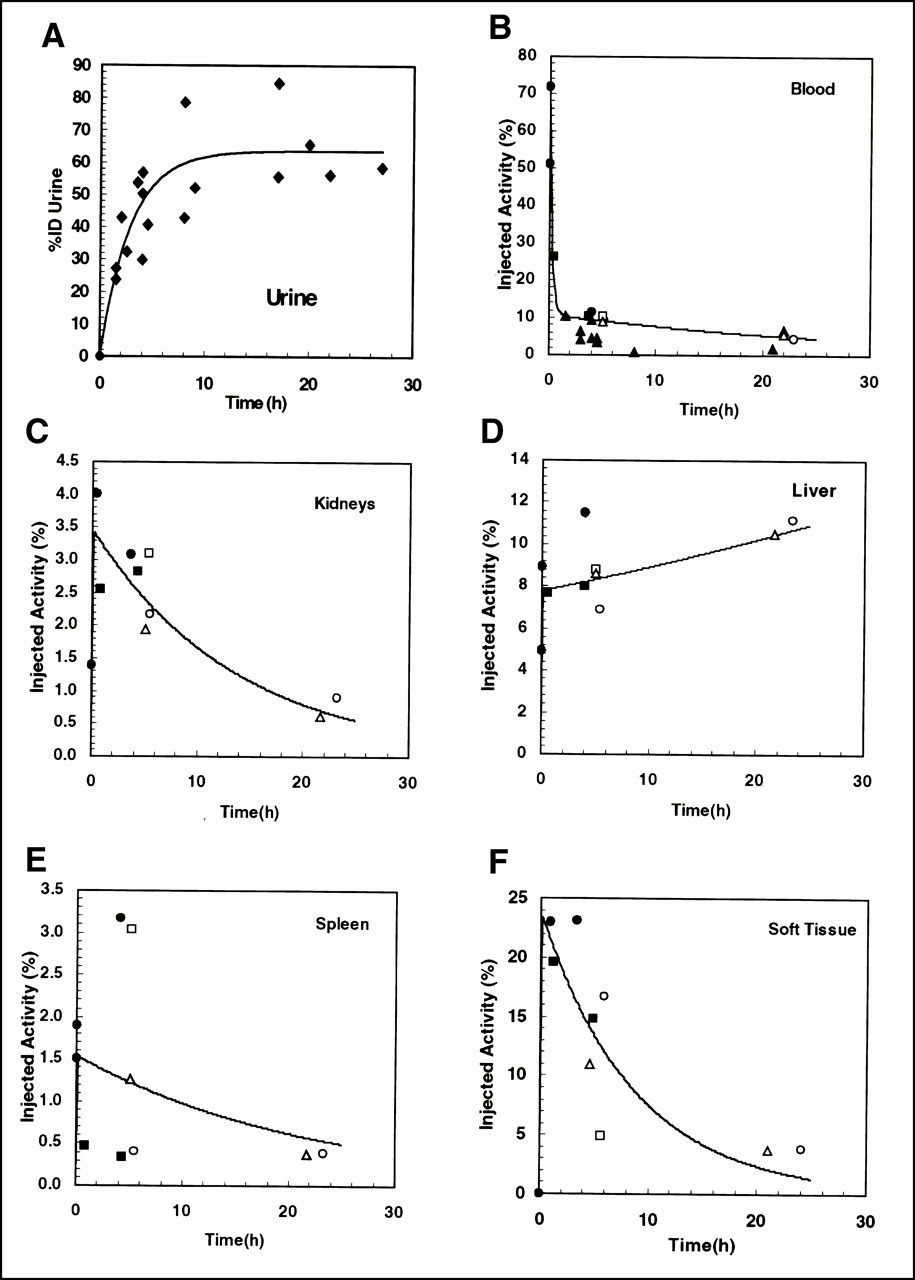
Cumulated patient time–activity curves. Unless noted, all values were determined from PET imaging data. (A) Urine data fitted with uptake function (percentage injected activity [%IA] = Af (1 − exp(−Fht × t)), Af = 63.6, Fht = 0.35). These parameters were used in MIRDOSE3.0 bladder model with voiding period of 4 h to obtain average residence time of bladder contents. Urine data presented here were collected from all eight patients, and individual patient data are not indicated. (B–F) Data for blood clearance (B), kidney uptake (C), liver uptake (D), spleen uptake (E), and soft-tissue uptake (F). ▴ = values determined from PET data; • = patient 1; ○ = patient 2; ▪ = patient 6; □ = patient 7; and ▵ = patient 8.
Organ Residence Times in Humans for 64Cu-TETA-OC from PET Images
DISCUSSION
The primary objective of this study was to determine the feasibility of PET imaging of neuroendocrine tumors in humans with 64Cu-TETA-OC. 64Cu-TETA-OC PET revealed tumors comparably with 111In-DTPA-OC SPECT in six patients. Neither method detected tumors in patient 4; however, follow-up by CT did not reveal any tumors. The PET agent detected a larger number of lesions in two patients but did not detect a lung metastasis that showed mild uptake with 111In-DTPA-OC SPECT in patient 8. Although the 64Cu-TETA-OC PET images in patient 8 did not show the lung lesion, we were unable to obtain a delayed image for this patient, which may have shown the lesion. Figures 1 and 2 show images of patients 2 and 6, in whom more lesions were seen with 64Cu-TETA-OC PET than with conventional imaging and SPECT with 111In-DTPA-OC. Patient 2, whose images are shown in Figure 1, had numerous metastatic foci of a carcinoid tumor throughout his body. Especially extensive lymphadenopathy was present in the neck, and numerous lesions were in the liver, mediastinum, and bone. The 64Cu-TETA-OC PET images revealed some of the smaller lesions, especially hepatic metastases, better than did the 111In-DTPA-OC images. The reason may be either the better tumor-to-nontumor ratios for 64Cu-TETA-OC or the better spatial resolution of PET compared with planar scintigraphy. In patient 6, carcinoid tumors in the abdomen were shown by both imaging methods. However, with 64Cu-TETA-OC PET, osseous lesions were apparent that were not seen in the 111In-DTPA-OC planar or SPECT images.
Urinary excretion of 111In-DTPA-OC has been reported by several investigators (3,15,16). Although the reports vary, generally the total excretion during 24 h ranged from 65 to 85 %ID. In a study of 10 patients, Krenning et al. (3) reported a mean cumulative urinary excretion of 25 %ID at 3 h, 50 %ID at 6 h, and 85 %ID at 24 h. The cumulative urinary excretion of 64Cu-TETA-OC was similar to that of 111In-DTPA-OC, for which excretion was 26.0 ± 12.3 %ID at 2 h, 44.6 ± 10.6 %ID at 4 h, and 63.7 ± 18.6 %ID at 27 h after injection. A few patients had an extensive tumor burden, and they excreted less 64Cu-TETA-OC.
Blood clearance of 64Cu-TETA-OC was similar to that of 111In-DTPA-OC at the earlier times; however, 111In-DTPA-OC cleared to a greater extent from the blood at later times. In a comparison study between 111In-DTPA-OC and 111In-DOTA-Tyr3-OC, both agents showed approximately 10 %ID in the blood at 2 h after injection, with approximately 1 %ID remaining at 24 h (16). We observed approximately 8 %ID at 4 h, with clearance to approximately 3 %ID at 22 h after injection. The retention of 64Cu in the blood was not entirely surprising, because we found that in rats, 64Cu-TETA-OC also did not completely clear from the circulation (8). Recently, using a superoxide dismutase–specific assay, we showed that in rat liver, 64Cu dissociates from 64Cu-TETA-OC and binds to superoxide dismutase (17). Mirick et al. (18) reported that 67Cu-BAT-2IT-Lym-1 (where BAT = 6-[p-(bromoacetamido)benzyl]-1,4,8,11-tetraazacyclotetradecane-N,N′,N′′,N′′′-tetraacetic acid and 2IT = 2-iminothiolane) dissociated and that 67Cu bound to ceruloplasmin, causing retention of 67Cu in the blood. In the patients administered 64Cu-TETA-OC, some dissociation of 64Cu likely occurred, with subsequent binding to plasma proteins. Future patient PET imaging studies will include metabolite analyses of blood and urine.
A preliminary evaluation of absorbed doses in normal organs, performed by averaging PET data from five patients, showed that the urinary bladder was the dose-limiting organ (0.25 mGy/MBq [0.94 rad/mCi]). This finding was predicted from human absorbed dose measurements estimated from rat biodistribution and baboon PET imaging data. The dose to the urinary bladder using baboon PET imaging data and human PET data was determined using the MIRDOSE3 bladder model (12) along with a voiding period of 4 h to obtain the residence time of the bladder contents. If patients were to be given intravenous fluids or asked to drink large quantities of fluids, the voiding time could be decreased to 1 h, which would reduce the absorbed dose to 0.062 mGy/MBq (0.23 rad/mCi). The liver would than be the dose-limiting organ (0.091 mGy/MBq [0.34 rad/mCi]).
Although the human absorbed dose estimates from rats, nonhuman primates, and humans indicate the bladder wall to be the dose-limiting organ, significant differences are seen when different species are used to estimate dosimetry. The use of rodent biodistribution data is generally thought to give a worst-case estimate of absorbed doses to normal organs; however, the data in Table 1 suggest that the use of rat biodistribution data underestimates the dose to the liver and spleen. As shown in Figure 3D, the percentage injected activity of 64Cu-TETA-OC in the liver increases over time. 64Cu may dissociate from the TETA chelator in human liver to a greater extent than it does in rat or baboon liver, and this dissociation may be responsible for the higher absorbed dose. The human dosimetry data also show the spleen to have a considerably higher absorbed dose than was extrapolated from rodent and baboon data. One proposal is that somatostatin regulates immune function in humans and that, therefore, SSRs are present in the spleen (19). The cumulative time–activity curve for the spleen (Fig. 3E) shows that the data are highly variable among the different patients, and a large error is therefore associated with the absorbed dose value. The absorbed dose to the spleen from 111In-DTPA-OC measured in humans is consistent with our data obtained with 64Cu-TETA-OC and PET (15).
Overall, the normal-organ dosimetry suggests that PET imaging with 111 MBq (3 mCi) 64Cu-TETA-OC gave reasonable absorbed doses to normal organs, with the urinary bladder (the critical organ) receiving less than 20 mGy (3 rad). In future PET imaging studies, the administered dose will be raised to approximately 518 MBq (14 mCi) and the patients will be asked to drink large quantities of fluids and to void frequently. We anticipate that these changes will provide higher image quality with less than 50 mGy (5 rad) to the urinary bladder or liver.
CONCLUSION
We evaluated 64Cu-TETA-OC as a potential PET tracer for imaging neuroendocrine tumors. 64Cu-TETA-OC PET compared well with 111In-DTPA-OC and conventional imaging, with more tumors being visualized in two patients. The blood clearance and urinary excretion of 64Cu-TETA-OC were similar to those of 111In-DTPA-OC at earlier times, but at later times 111In-DTPA-OC clearance from the blood and excretion into the bladder were greater. The human absorbed doses to normal organs from 64Cu-TETA-OC were estimated using rodent biodistribution data, baboon PET imaging data, and human PET imaging data. The baboon PET data more accurately estimated the human dosimetry than did the rodent data; however, both methods underestimated the absorbed doses to the liver and spleen. Although 64Cu-TETA-OC has promise as a PET imaging agent for neuroendocrine tumors, our ultimate goal would be to use this agent for PET imaging before using this agent for targeted radiotherapy. Future studies include determining tumor dosimetry, which will provide information on the potential of 64Cu-TETA-OC for therapy.
Acknowledgments
The authors thank Dr. Michael J. Welch for providing 64Cu; Diana Trask, Helen Kaemmerer, and John Englebach for excellent technical assistance; and Dr. Barry A. Siegel for helpful discussions. This study was supported by grant CA64475 from the National Institutes of Health, Bethesda, MD; a grant from Mallinckrodt, Inc.; and grant DE-FG02-96ER92216 from the Department of Energy.
Footnotes
Received Apr. 6, 2000; revision accepted Aug. 14, 2000.
For correspondence or reprints contact: Carolyn J. Anderson, PhD, Mallinckrodt Institute of Radiology, Washington University School of Medicine, 510 S. Kingshighway Blvd., Campus Box 8225, St. Louis, MO 63110.
REFERENCES
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- 64Cu-SARTATE PET Imaging of Patients with Neuroendocrine Tumors Demonstrates High Tumor Uptake and Retention, Potentially Allowing Prospective Dosimetry for Peptide Receptor Radionuclide Therapy
- Promising Prospects for 44Sc-/47Sc-Based Theragnostics: Application of 47Sc for Radionuclide Tumor Therapy in Mice
- Promises of Cyclotron-Produced 44Sc as a Diagnostic Match for Trivalent {beta}--Emitters: In Vitro and In Vivo Study of a 44Sc-DOTA-Folate Conjugate
- VPAC1 Receptors for Imaging Breast Cancer: A Feasibility Study
- Clinical PET of Neuroendocrine Tumors Using 64Cu-DOTATATE: First-in-Humans Study
- A Novel Technology for the Imaging of Acidic Prostate Tumors by Positron Emission Tomography
- Preparation and Biological Evaluation of 64Cu-CB-TE2A-sst2-ANT, a Somatostatin Antagonist for PET Imaging of Somatostatin Receptor-Positive Tumors
- Tumor Receptor Imaging
- Nanoparticle PET-CT Imaging of Macrophages in Inflammatory Atherosclerosis
- In Vivo Imaging of 64Cu-Labeled Polymer Nanoparticles Targeted to the Lung Endothelium
- PET Imaging of CCND1 mRNA in Human MCF7 Estrogen Receptor Positive Breast Cancer Xenografts with Oncogene-Specific [64Cu]Chelator-Peptide Nucleic Acid-IGF1 Analog Radiohybridization Probes
- Dosimetry in Peptide Radionuclide Receptor Therapy: A Review
- microPET Imaging of Glioma Integrin {alpha}v{beta}3 Expression Using 64Cu-Labeled Tetrameric RGD Peptide
- Synergistic effects of light-emitting probes and peptides for targeting and monitoring integrin expression
- Preparation and Biological Evaluation of Copper-64-Labeled Tyr3-Octreotate Using a Cross-Bridged Macrocyclic Chelator
- PET Imaging of Oncogene Overexpression Using 64Cu-Vasoactive Intestinal Peptide (VIP) Analog: Comparison with 99mTc-VIP Analog
- First 18F-Labeled Tracer Suitable for Routine Clinical Imaging of sst Receptor-Expressing Tumors Using Positron Emission Tomography
- Two-Step Methodology for High-Yield Routine Radiohalogenation of Peptides: 18F-Labeled RGD and Octreotide Analogs
- Subcellular Localization of Radiolabeled Somatostatin Analogues: Implications for Targeted Radiotherapy of Cancer
- Enhancing Targeted Radiotherapy by Copper(II)diacetyl- bis(N4-methylthiosemicarbazone) Using 2-Deoxy-D-Glucose
- In Vivo Evaluation of Pretargeted 64Cu for Tumor Imaging and Therapy