


Abstract
FDG PET is increasingly performed in patients with differentiated thyroid cancer who present with elevated human thyroglobulin (hTG) levels and negative 131I scan. The aim of this study was to evaluate the impact of FDG PET on treatment in these patients. Methods: A total of 118 FDG PET studies were performed on 64 patients, and follow-up data were available for all patients. Whole-body images were acquired 1 h after intravenous injection of 370 MBq (10 mCi) FDG using a PET scanner with an axial field of view of 16.2 cm. Tumor-suspicious FDG PET studies were evaluated by histology, cytology, 131I uptake, CT or MRI, and follow-up of hTg levels. The therapeutic consequence was noted for each patient. Moreover, results of FDG PET were correlated with hTg levels. Results: Forty-four patients had positive scans, which were proven to be true-positive in 34 patients, whereas 7 patients had false-positive findings. Two patients exhibited a secondary malignancy. One patient did not fit in any category, having true-positive, false-positive, and false-negative findings. On the other hand, 20 patients had negative scans. These were true-negative findings in 5 patients, whereas the remaining 15 patients had false-negative results. Accordingly, the positive predictive value of FDG PET was 83% (34/41), whereas the negative predictive value was 25% (5/20). Treatment was directly changed in 19 of 34 patients with true-positive PET studies: 18 patients had further surgery, and 4 patients were referred for external irradiation, 3 of them after incomplete removal of local recurrences. FDG PET showed widespread disease in 7 patients; thus, palliative treatment, rather than curative therapy, was initiated. True-positive FDG PET findings were correlated positively with increasing hTg levels (i.e., FDG PET was true-positive in 11%, 50%, and 93% of patients with hTg levels of <10, 10–20, and >100 μg/L, respectively). Conclusion: FDG PET is a valuable diagnostic tool in patients with differentiated thyroid cancer who present with increased hTg levels and negative 131I scans because it permits selection of patients for surgery, which may be curative. FDG PET is most promising at hTg levels of >10 μg/L.
Elevated human thyroglobulin (hTg) levels and negative 131I scans represent both diagnostic and therapeutic problems of patients with differentiated thyroid cancer. Although 131I scanning has a very high specificity of 99%–100%, the amount of 131I-positive recurrences is about 50%–60% in papillary and 64%–67% in follicular thyroid cancer only (1–3). Because progression in differentiated thyroid cancer occurs very slowly, patients have a relatively good prognosis to live for many years—even after metastatic disease has been detected—provided adequate treatment has been offered. However, patients with metastatic disease and negative 131I scans are usually not treated with high-dose radioiodine. Thus, 131I-negative metastases need to be removed surgically, provided they can be localized. Although metastases of differentiated thyroid cancer grow rather slowly, they consume a considerable amount of glucose compared with that of normal tissues. Consequently, FDG PET has been suggested for patients with negative 131I scans and elevated hTg levels for the detection of both local recurrences and metastases of differentiated thyroid cancer (4–18). Moreover, the German interdisciplinary consensus conference recently classified FDG PET as a “1a-indication” in these patients (19,20).
However, the value of FDG PET for patient management is still unclear for patients with negative 131I scans and elevated hTg levels. Therefore, the aim of this retrospective study was to evaluate the impact of FDG PET on both follow-up and treatment of these patients. Initial results have been published briefly elsewhere (21–25).
MATERIALS AND METHODS
Patients
A total of 118 FDG PET studies were performed on 64 patients (39 women, 25 men; age range, 21–81 y) with histologically proven differentiated thyroid cancer. FDG PET was performed repeatedly in 21 patients. All patients had a complete clinical history and physical examination. Most of them (n = 48) had negative 131I scans and elevated hTg levels (hTg ≥ 2.0 μIU/mL) under thyroid-stimulating hormone (TSH) stimulation (TSH ≥ 30 μIU/mL), including 4 patients who had FDG PET later, when hTg levels were negative under TSH suppression (TSH ≤ 0.1 μIU/mL). In spite of a positive 131I scan, additional tumor lesions were suspected in 7 patients with elevated hTg levels. In the remaining 9 patients, thyroid cancer tissue was suspected because of findings on other imaging modalities (e.g., sonography, radiography of the chest, CT), although hTg levels were not elevated. Patients were followed-up at least until a decision was made concerning treatment strategy. Therefore, the follow-up interval amounted to 1–64 mo.
PET Scanning
Patients fasted for at least 12 h before PET scanning to minimize blood insulin levels and glucose use by normal tissue (26). Whole-body emission images were acquired without attenuation correction 60 min after intravenous injection of 370 MBq FDG using an ECAT EXACT 47 (921) PET scanner (Siemens/CTI, Knoxville, TN) with an axial field of view of 16.2 cm.
Patients were placed in the PET gantry in a supine position with both arms at the side of the body. Images were acquired for 8 min per bed position covering the neck down to the upper waist. The second set of images was acquired from the waist down to the upper legs. Before the second acquisition, patients were asked to empty the bladder (to decrease urine activity) and to raise their arms (to minimize photon attenuation in the abdomen). Emission data were reconstructed by filtered backprojection using a Hanning filter with a cutoff frequency of 0.4 unit of the Nyquist frequency. Transaxial spatial resolution was ∼12-mm full width at half maximum. PET images were printed on x-ray films and since 1998 have been printed on transparency film (Helios 810; Sterling Diagnostic Imaging, Bad Homburg, Germany) using a linear gray scale with highest activity displayed in black (27). Note that FDG PET was performed under varying TSH levels.
Evaluation
To evaluate the results of FDG PET, suspicious findings were correlated with histology, cytology, 131I uptake, CT, MRI, and hTg level. Because FDG PET was performed twice or multiple times on 20 patients, FDG PET was evaluated on a patient basis rather than on a study basis or a lesion basis. Thus, for each patient, the FDG PET study selected for evaluation was the one that influenced further treatment of the patient most. FDG PET was then classified as:
true-positive, if pathologic FDG uptake was proven by histology, cytology, or correlative imaging techniques and, therefore, led to a change of therapy
false-positive, if pathologic FDG uptake could not be verified and, therefore, had no clinical consequence
true-negative if no FDG uptake was found and patients had neither elevated hTg levels nor any evidence of recurrence in subsequent follow-up
false-negative if no FDG uptake was found in spite of elevated hTg levels or positive findings in correlative imaging methods
Moreover, results of FDG PET were correlated with the respective hTg level of the patient at the time of the study. Intervals of <10, 10–20, 20–50, 50–100, and >100 μg/L were chosen for serum hTg levels. Then, true-positive FDG PET studies at a certain hTg level were divided by the total number of patients investigated at that hTg level. The data for stimulated and suppressed TSH were analyzed separately.
RESULTS
Positive FDG PET
Forty-four of 64 patients had pathologic FDG uptake, and, thus, were classified as positive. In 2 patients (81-y-old man and 78-y-old woman), FDG PET revealed a second malignancy, which definitely changed the treatment strategy of these patients. A further patient (51-y-old woman) could not be classified according to the above criteria because FDG PET revealed true-positive as well as false-positive and false-negative findings, which changed the treatment strategy several times during follow-up. Therefore, these patients were excluded from the analysis, and the 41 remaining patients with positive findings on FDG PET were eligible for complete evaluation.
Validation of FDG PET findings and treatment strategy chosen is summarized in Table 1 and Table 2, respectively. FDG PET findings were true-positive in 34 of 41 patients. Treatment was directly changed in 19 of 34 patients with true-positive PET studies: 18 patients had further surgery (Fig. 1), and 4 patients were referred for external irradiation, 3 of them (57-y-old, 74-y-old, and 72-y-old women) after incomplete removal of local recurrences (Fig. 2). One of these patients (38-y-old woman) who presented with local recurrence underwent surgery in the same location 2 y later (data not included in Tables 1 and 2). Ten patients received 131I therapy when a follow-up 131I scan revealed a positive finding in the location of the FDG-positive lesions. 131I therapy was performed on 2 of these patients after incomplete resection of distant metastases (65-y-old and 64-y-old men). Note that the number of treatments summarized in line 1 in Table 2 (n = 39) exceeds the number of patients (n = 34) because of the 5 patients who had surgery and either external irradiation or 131I therapy. FDG PET showed widespread disease in 7 patients (e.g., in case of multiple pulmonary metastases); thus, palliative treatment, rather than curative therapy, was initiated.
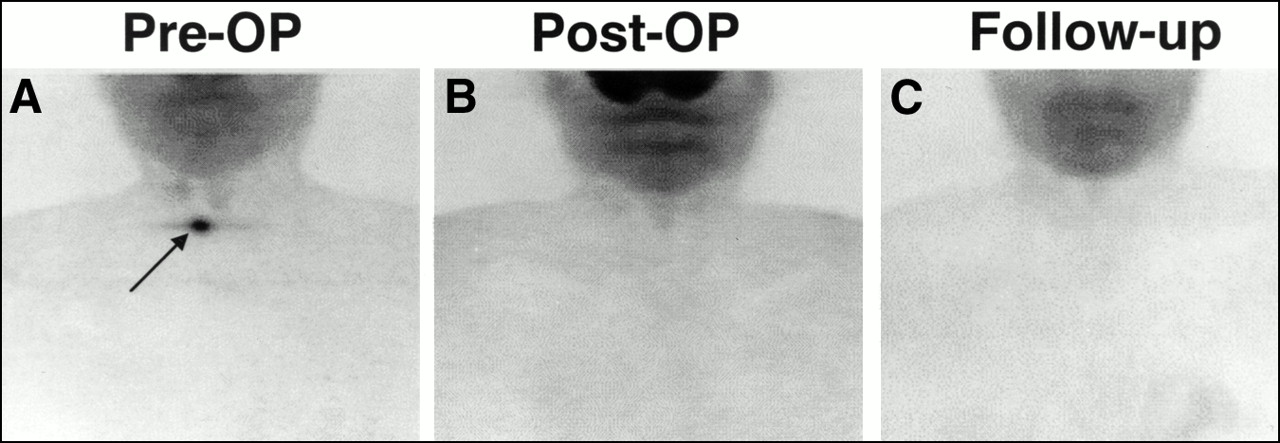
FDG-positive local recurrence (arrow) in 49-y-old man who presented with negative 131I scan after thyroidectomy and two courses of radioiodine treatment of papillary thyroid cancer initially staged as pT2bN0M0 (A). No tumor remnants were seen after further surgery (B) and during follow-up (C). Consequently, hTg levels dropped from 30 μg/L (preoperative) to 5 μg/L (postoperative) and 11 μg/L (follow-up). Images show maximum-intensity projections in anterior views.

FDG-positive residual tumor and lymph node metastasis (arrows) in 57-y-old woman who presented after incomplete thyroidectomy and tumor resection of papillary thyroid cancer initially staged as pT4bN1Mx (A). FDG PET was performed to assess tumor extension and possible metastases before further surgery. Residual tumor masses were seen after additional surgery (B), and external irradiation yielded good response (C). After irradiation, hTg levels dropped from 24 to 1.5 μg/L. Images show maximum-intensity projections in anterior views.
Validation of FDG PET Findings by Various Methods Applied
Treatment Strategy Drawn from Results of FDG PET
In contrast, positive FDG PET imaging of the remaining 7 of 41 patients turned out to be false-positive (Table 1). This was confirmed by histology (n = 2), cytology (n = 1), CT or MRI (n = 2), and subsequent measurements of hTg levels during follow-up (n = 2). Consequently, further treatment was not justified in these patients. However, 2 of these 7 patients underwent surgery, and no pathologic findings were found (Table 2).
Negative FDG PET
A physiologic pattern of FDG uptake was found in 20 of 64 patients; thus, FDG PET was classified as negative. Findings in 5 of these patients were proven to be true-negative by negative hTg levels during further follow-up (Table 1); consequently, these patients did not receive any specific therapy (Table 2). FDG PET of the remaining 15 patients turned out to be false-negative (Table 1), as proven by CT or MRI (n = 3), 131I uptake (n = 1), or persistently elevated or rising hTg levels (n = 11). The 3 patients who presented with positive CT or MRI findings were referred for surgery, and recurrent or metastatic disease of differentiated thyroid cancer was proven by histology in 2 of them thus far. One patient who had a positive 131I scan within the follow-up received 131I therapy. No specific treatment could be offered to the remaining 11 patients (Table 2) because CT, MRI, or 131I scanning did not reveal the origin of persistently elevated or rising hTg levels.
FDG PET and hTg Levels
The fraction of true-positive FDG PET was correlated positively with increasing hTg levels (Table 3). FDG PET findings were true-positive in 11%, 50%, and 93% of patients with hTg levels of <10, 10–20, and >100μg/L, respectively. The fraction of true-positive FDG PET was independent of TSH level (i.e., whether hTg measurement was performed under TSH stimulation or suppression).
True-Positive FDG PET Findings with Respect to hTg Level
DISCUSSION
Most patients with differentiated thyroid cancer who present with 131I-accumulating metastases receive 131I treatment, which may be curative. Patients without 131I-avid (negative 131I scan) metastases lack this option. Nevertheless, curative treatment can be achieved in these patients, provided tumor tissues are resected completely, before widespread metastatic disease occurs. Therefore, imaging methods that allow an accurate detection of recurrence or metastases (or both) of differentiated thyroid cancer in an early stage are crucial with respect to both prognosis and survival of the patients.
Imaging modalities that can be offered to a patient in this clinical setting (i.e., differentiated thyroid cancer, elevated hTg levels, and negative 131I scan) include sonography of neck and abdomen, chest radiography, bone scanning, CT, and MRI. Apart from these procedures, PET with FDG has been used for several years in these patients. One of the first reports on FDG PET in three patients suffering from differentiated thyroid cancer was published by Joensuu and Ahonen (4) almost 13 y ago. Since that time, several studies have shown the ability of FDG PET for the detection of 131I-negative lesions in differentiated thyroid cancer (6,16–18). This was confirmed by some studies with larger numbers of patients (5,9–11,14,15). In the meantime, FDG PET has been accepted as a valuable imaging method for patients with differentiated thyroid cancer who present with elevated hTg levels and negative 131I scans. Consequently, an interdisciplinary consensus conference held in Germany in 1996 and 1997 on the use of FDG PET in oncology classified this as a “1a-indication,” meaning that FDG PET has been shown to have “proven clinical value” in this clinical setting (19,20).
Although the value of FDG PET in the detection of thyroid cancer tissue is undeniable, the consequences of FDG-positive lesions in terms of clinical outcome are still under discussion. In general, FDG uptake and the concomitant loss of 131I uptake are known as a functional sign of dedifferentiation (4,9,17). Lietzenmayer et al. (28) observed that the intensity of FDG uptake is correlated with progressive dedifferentiation. They quantified FDG uptake by standard uptake values and found that an intense FDG uptake with the concomitant loss of 131I uptake indicates progress. Patients with an initially high standard uptake value had an unfavorable clinical course, whereas decreasing FDG uptake together with a persistent 131I uptake was associated with a good prognosis. As the pathophysiologic basis for these observations, a correlation of the expression of the glucose transporter GLUT 1 and the grade of dedifferentiation of thyroid cancer was described by Schönberger et al. (29). However, one specific patient may exhibit either 131I-avid lesions or FDG-avid lesions and even lesions that take up both radiotracers (16–18). Accordingly, in this study FDG uptake was also associated with a more aggressive behavior of metastatic lesions. Three patients with FDG-positive cervical tumor tissue underwent external irradiation after incomplete surgical resection (Fig. 2). In addition, FDG PET revealed extensive disease in seven patients, which changed the treatment regimen from a curative to a more palliative approach. On the other hand, it is important to note that four patients who underwent further surgery on the basis of locoregional findings had no signs for recurrence except for a slightly elevated hTg level later on (Table 3). Therefore, although FDG uptake can be considered as a sign of dedifferentiation, it does not automatically predict an unfavorable prognosis. Moreover, 131I-avid tumor tissue developed in some patients in the same location as earlier FDG-positive findings and the patients received 131I therapy later on. This observation is important because it indicates that further 131I scans may be promising even if a finding is only FDG positive. Hence, FDG-positive recurrences and metastases may indicate dedifferentiated and more aggressive tumor tissue but do not automatically predict a worse outcome.
These conclusions are supported by observations relating to hTg production. Although thyroid cancer tissue has lost the ability of taking up and storing iodine, it is primarily able to produce hTg, which indicates only partial differentiation. In our patients, FDG PET was more promising when the hTg level rose as described by others (13,15,30). Accordingly, Sophocleous et al. (31) reported in 1997 that false-negative hTg levels under TSH stimulation are rare (i.e., in the range of 3%–4% of patients with recurrences). The most probable explanation for this finding is the tumor mass itself: hTg production rises with an increasing number of tumor cells, and at a certain size the lesion will be detected as FDG positive. Similar observations have been made relating to 131I-avid tumor tissue. Arning et al. (32) found only a few patients with 131I-avid metastases and low hTg levels. The well-known observation that maximum hTg levels decrease after 131I therapy although 131I scans are negative indicates 131I-avid micrometastases, which are too small to be visualized by scintigraphy. Therefore, the ability to produce hTg is obviously maintained longer in the process of dedifferentiation than is the ability to take up 131I. This can be explained by the fact that the mechanisms necessary for iodine storage (i.e., iodination, iodization, and synthesis of hTg) are much more complex than is the synthesis of hTg alone.
We found that the fraction of true-positive FDG PET was correlated positively with increasing hTg levels (Table 3). FDG PET findings were true-positive in 11%, 50%, and 93% of patients with hTg levels of <10, 10–20, and >100μg/L, respectively. This observation is in accordance with Lubin et al. (2), who reported that a negative 131I scan was seen predominantly when the hTg level was <10 μg/L under TSH suppression. In addition, the cutoff level for determination of hTg as elevated is estimated to be between 1 and 10 μg/L (33,34). Thus, our data indicate that FDG PET is worthwhile, especially at hTg levels of >10 μg/L.
CONCLUSION
FDG PET is a valuable diagnostic tool for patients with differentiated thyroid cancer who present with increased hTg levels and negative 131I scans because it permits selection of patients for surgery, which may be curative. FDG PET is most promising at hTg levels of >10 μg/L.
Footnotes
Received Nov. 29, 1999; revision accepted Apr. 4, 2000.
For correspondence or reprints contact: Karl H. Bohuslavizki, MD, PhD, Department of Nuclear Medicine, University Hospital Eppendorf, Martinistrasse 52, D-20246 Hamburg, Germany.
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- ENDOCRINE TUMOURS: Imaging in the follow-up of differentiated thyroid cancer: current evidence and future perspectives for a risk-adapted approach
- NCCN Task Force: Clinical Utility of PET in a Variety of Tumor Types
- PET/CT fusion technology: its role in managing recurrent, well-differentiated thyroid cancer
- Comparison of 18F-FDG PET and Bone Scintigraphy in Detection of Bone Metastases of Thyroid Cancer
- 18F-FDG PET/CT in Patients with Suspected Recurrent or Metastatic Well-Differentiated Thyroid Cancer
- The contribution of PET/CT to improved patient management
- Possible Explanations for Patients with Discordant Findings of Serum Thyroglobulin and 131I Whole-Body Scanning
- Empirically Treating High Serum Thyroglobulin Levels
- Progress and Promise of FDG-PET Imaging for Cancer Patient Management and Oncologic Drug Development
- PET in the follow-up of differentiated thyroid cancer
- Clinical Usefulness of FDG PET in Differentiated Thyroid Cancer