


Abstract
We compared the efficacies of 18F-FDG PET and 99mTc-bone scintigraphy for the detection of bone metastases in patients with differentiated thyroid carcinoma (DTC). Methods: We examined 47 patients (32 women, 15 men; mean age ± SD, 57.0 ± 10.7 y) with DTC who had undergone total thyroidectomy and were hospitalized to be given 131I therapy. All patients underwent both whole-body 18F-FDG PET and 99mTc-bone scintigraphy. The skeletal system was classified into 11 anatomic segments and assessed for the presence of bone metastases. Bone metastases were verified either when positive findings were obtained on >2 imaging modalities—201Tl scintigraphy, 131I scintigraphy, and CT—or when MRI findings were positive if vertebral MRI was performed. Results: Bone metastases were confirmed in 59 of 517 (11%) segments in 18 (38%) of the 47 study patients. The sensitivities (visualization rate) for bone metastases on a segment basis using 18F-FDG PET and 99mTc-bone scintigraphy were 50 of 59 (84.7%) and 46 of 59 (78.0%), respectively; the difference between these values was not statistically significant. There were only 2 (0.4%) false-positive cases in a total of 451 bone segments without bone metastases when examined by 18F-FDG PET, whereas 39 (8.6%) were false-positive when examined by 99mTc-bone scintigraphy. Therefore, the specificities of 18F-FDG PET and 99mTc-bone scintigraphy were 449 of 451 (99.6%) and 412 of 451 (91.4%), respectively; the difference between these values was statistically significant (P < 0.001). The overall accuracies of 18F-FDG PET and 99mTc-bone scintigraphy were 499 of 510 (97.8%) and 458 of 510 (89.8%), respectively; the difference between these was also statistically significant (P < 0.001). Conclusion: The specificity and the overall accuracy of 18F-FDG PET for the diagnosis of bone metastases in patients with DTC are higher than those of 99mTc-bone scintigraphy, whereas the difference in the sensitivities of both modalities is not statistically significant. In comparison with 99mTc-bone scintigraphy, 18F-FDG PET is superior because of its lower incidence of false-positive results in the detection of bone metastases of DTC.
Skeletal imaging by 18F-FDG PET has been shown to be useful in the detection of bone metastases of breast (1–6), lung (1,4,7,8), thyroid (4), esophageal (4,9), gastric (4), colorectal (4), endemic nasopharyngeal (10), renal cell (11), prostate (1), ovarian (4), and testicular (4) carcinomas. In most of these studies, 18F-FDG PET was proven to be superior to conventional scintigraphic imaging using 99mTc-labeled phosphate compounds (99mTc-methylene diphosphonate [99mTc-MDP] or 99mTc-hydroxymethylene diphosphonate [99mTc-HMDP]). For the detection and evaluation of bone metastases of various kinds of carcinomas, 99mTc-bone scintigraphy has been used widely because of its overall high sensitivity and the easy evaluation of the entire skeleton (12). However, 99mTc-bone scintigraphy leads often to false-positive lesions and, consequently, its specificity is reduced, because degenerative or inflammatory foci will be often confused with metastatic diseases.
Differentiated thyroid carcinoma ([DTC] papillary and follicular) is characterized by good prognosis in comparison with carcinomas of other organs. The 10-y survival rate of DTC is >80% because of treatments such as total thyroidectomy and ablation of remnants with radioiodine (13). However, metastases of thyroid carcinoma develop in 7%–23% of patients; the distant metastases occur commonly in the lungs, bones, and brain, and bones are the second common site of metastases from thyroid carcinoma (14).
Several earlier reports showed that 18F-FDG PET is highly sensitive in detecting DTC and is particularly useful for the evaluation of patients with negative radioactive iodine scintigraphy and elevated thyroglobulin levels (15–20). For the detection of bone metastases of thyroid carcinoma, 99mTc-bone scintigraphy has been also used widely. However, to our knowledge, there have been no systematic comparative studies on the efficacies of 18F-FDG PET and 99mTc-bone scintigraphy in the detection of bone metastases of thyroid carcinoma. The purpose of this study was to compare 18F-FDG PET and 99mTc-bone scintigraphy in the detection of bone metastases of DTC.
MATERIALS AND METHODS
Subjects
All procedures followed the clinical guidelines of Nagoya University Hospital and were approved by the International Review Board. Written consent was obtained after a complete description of the study was given to all patients and their relatives. Forty-seven patients (32 women, 15 men; mean age ± SD, 57.0 ± 10.7 y), who had DTC and had undergone total thyroidectomy, were selected for study. All patients were hospitalized to be given 131I therapy for ablation of remnants and underwent both whole-body 18F-FDG PET and 99mTc-bone scintigraphy to detect bone metastases. 18F-FDG PET and 99mTc-bone scintigraphy were performed from 3 to 30 d before the radioiodine therapy, and the interval between 18F-FDG PET and 99mTc-bone scintigraphy was, at most, 1 mo. At the start of the study, 25 (53%) of the 47 study patients had metastases to the cervical lymph nodes and 20 (43%) had distant metastases in the lungs and mediastinal or supraclavicular lymph nodes.
Histopathologic Type
Fifteen (32%) and 29 (62%) of the 47 study patients had follicular and papillary carcinomas, respectively. In the other 3 (6.4%) patients, the pathologic type was unknown, but they were diagnosed as having DTC by clinical and radiologic follow-up.
Bone Scintigraphy
99mTc-Bone scintigraphy was performed 3 h after intravenous injection of 555 MBq 99mTc-HMDP (Nihon Medi-Physics, Ltd.) or 740 MBq 99mTc-MDP (Daiichi Radioisotope Laboratories, Ltd.). Anterior and posterior whole-body planar images were obtained with high-resolution collimation on a dual-head γ-camera (E.CAM; Toshiba Corp.). At least 2 experienced radiologists interpreted the planar images visually.
PET Procedure
The patients fasted for at least 6 h before PET. Scanning was performed using 18F-FDG and a Headtome-V PET scanner (Shimadzu). 18F-FDG (296 MBq) was injected intravenously 40 min before imaging. Whole-body emission/transmission images were obtained simultaneously. At least 2 experienced radiologists interpreted the coronal and axial images visually.
Data Analysis
The presence of bone metastases was assessed in 11 bone segments: cervical, thoracic, and lumbar spines, sacrum with coccyx, right and left pelves, sternum, right and left scapulae with clavicles, and right and left ribs. At least 2 experienced radiologists diagnosed bone metastases using 201Tl scintigraphy, 131I scintigraphy, CT, plain film radiography, or MR images. The presence of bone metastases was verified by the following definitions. First, the positive findings for bone metastases must be obtained in >2 imaging modalities—201Tl scintigraphy, 131I scintigraphy, and CT. Second, if vertebral MRI was performed, the MRI findings must indicate the positive metastases. It has been demonstrated that MRI shows high sensitivity and specificity in detecting bone metastases (21–23). When the positive finding for bone metastases was detected in only 1 modality other than MRI, the bone segment showing such a finding was excluded, because it was unclear whether such a lesion was bone metastasis. Among the total 517 bone segments examined, 7 segments (1.4%) were excluded for this reason. When positive findings of bone metastases were detected in none of the 4 modalities (the above 3 modalities plus MRI), the cases were diagnosed as no bone metastases. Furthermore, all metastatic lesions in the bones were classified into the osteoblastic, osteolytic, and mixed-type lesions on the basis of the images on CT scan.
Statistical Analysis
Statistical analysis was performed using the McNemar test. A value of P < 0.05 was considered significant.
RESULTS
Eighteen (38%) of the 47 study patients were finally diagnosed to have bone metastases, and 59 bone segments were confirmed to have at least 1 metastatic lesion according to the definitions of this study. The distribution of metastases in the examined bone segments is given in Table 1. The difference in the patient populations (sex, age, and histopathologic type) between bone metastases-positive and -negative groups is shown in Table 2. The presence of bone metastases was 4 of 15 (27%) in the male group and 14 of 32 (44%) in the female group; the difference between these groups was not statistically significant (P = 0.34). There was no difference in the average age of patients between the bone metastases-positive and -negative groups. Thirteen (87%) of 15 patients with follicular carcinoma had bone metastases, whereas only 3 (19%) of 29 patients with papillary carcinoma had bone metastases; the difference between these values was statistically significant (P < 0.001).
Incidence of Bone Metastases in 11 Bone Segments of Patients with DTC
Difference in Patient Populations between Bone Metastases-Positive and -Negative Groups of Patients with DTC
As indicated in Table 3, 50 (84.7%) of the 59 bone segments with metastases were detected by 18F-FDG PET, and 46 (78.0%) of the 59 bone segments were detected by 99mTc-bone scintigraphy. However, the difference in the sensitivity between 18F-FDG PET and 99mTc-bone scintigraphy was not statistically significant (P = 0.45).
Sensitivity, Specificity, and Overall Accuracy of 18F-FDG PET and 99mTc-Bone Scintigraphy in Detection of Bone Metastases in Patients with DTC
As also shown in Table 3, there were only 2 (0.4%) false-positive cases in the 451 bone segments that were confirmed to have no bone metastases when examined by 18F-FDG PET, whereas 39 (8.6%) of the 451 bone segments were false-positive when examined by 99mTc-bone scintigraphy. Therefore, the specificity of 18F-FDG PET in diagnosing the bone metastases of DTC (449/451, 99.6%) was higher than that of 99mTc-bone scintigraphy (412/451, 91.4%); the difference between these values was statistically significant (P < 0.001). The overall accuracy of 18F-FDG PET (499/510, 97.8%) was also higher than that of 99mTc-bone scintigraphy (458/510, 89.8%); the difference between these values was statistically significant (P < 0.001) (Table 3).
Sixty-seven metastatic lesions were detected in the 59 affected bone segments. Among them, 52 (78%) were classified into the osteolytic, 7 (10%) into the osteoblastic, and 3 (4.5%) into the mixed-type lesions on the basis of the CT images. Five (7.5%) lesions could not be classified because of their unclear CT images. The detectability of 18F-FDG PET and 99mTc-bone scintigraphy for these metastatic bone lesions is shown in Table 4. Of the 52 osteolytic metastatic lesions, 48 (92%) and 42 (81%) lesions were detected by 18F-FDG PET and 99mTc-bone scintigraphy, respectively; the difference between these values was not statistically significant (P = 0.15). Of the 7 osteoblastic lesions, 4 and 5 lesions were detected by 18F-FDG PET and 99mTc-bone scintigraphy, respectively.
Detectability of 18F-FDG PET and 99mTc-Bone Scintigraphy for Osteoblastic and Osteolytic Metastases in Patients with DTC
The exemplary images of bone metastases of DTC by 18F-FDG PET, 99mTc-bone scintigraphy, and the other radiologic methods in 3 patients are shown in Figures 1, 2, and 3.

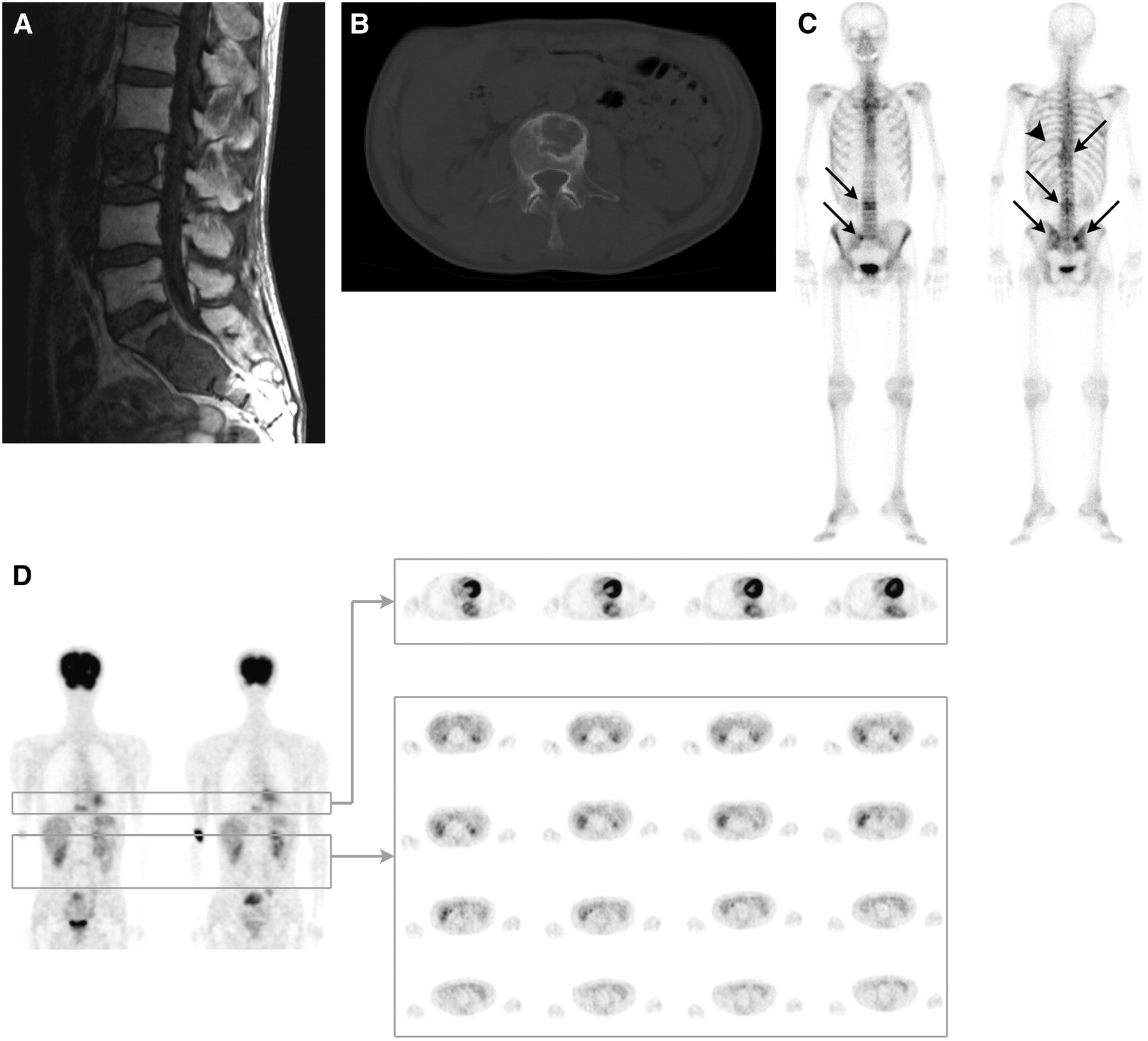
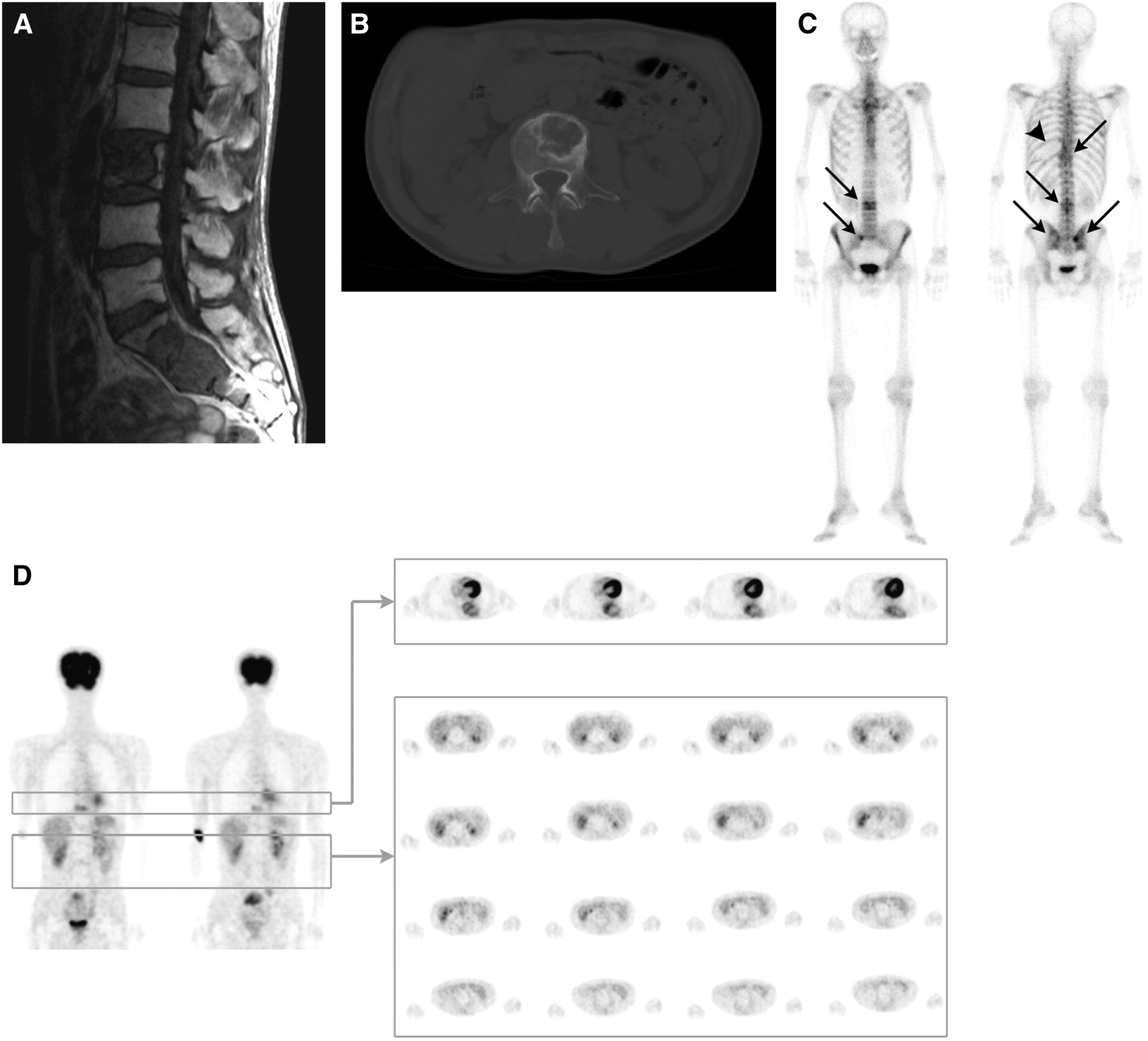
(A) T1-weighted MR image (left) shows massive lesion of low signal intensity, and T2-weighted MR image (right) shows lesion of high signal intensity. (B) CT scan shows osteolytic changes at thoracic spine (T4–T5). (C and D) 18F-FDG PET coronal image (C) and 99mTc-bone whole-body scintigram (D) show high uptakes at thoracic spine (T4–T5), sacrum, and iliac bones (arrows).

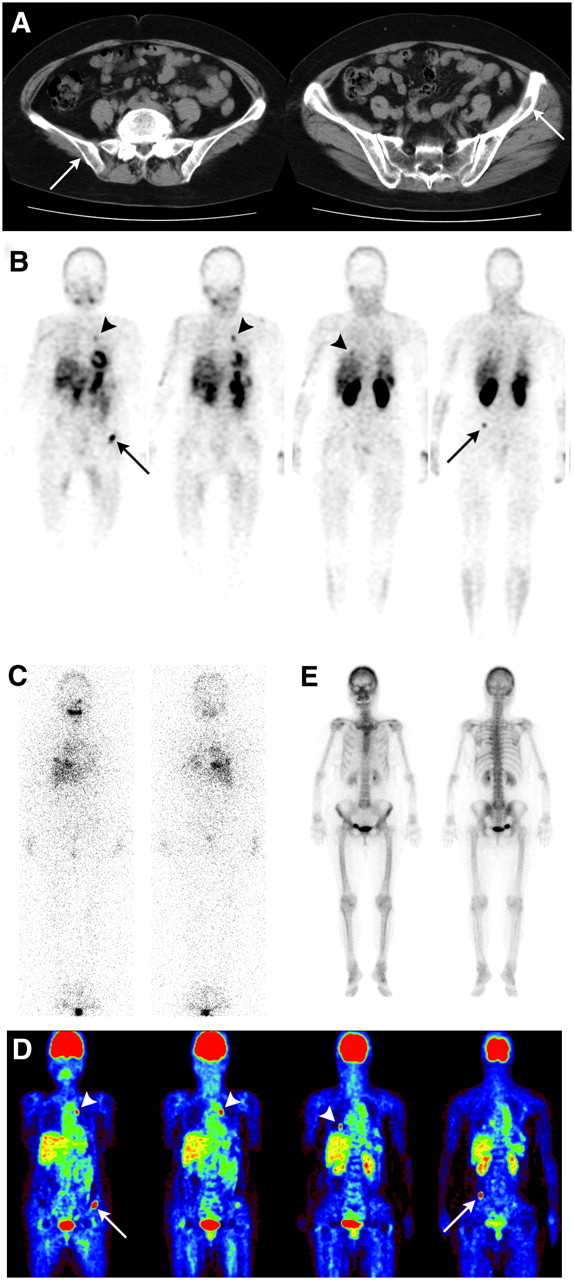
In this patient, there were multiple lung metastases besides bone metastases. (A) CT scan shows osteolytic lesions on both sides of iliac bones (arrows). (B) 201Tl SPECT image shows high uptake on both sides of iliac bones (arrows), right lower lung, and left lung hilus (arrowheads). (C) 131I scintigraphy shows no obvious abnormal uptake. (D) 18F-FDG PET shows high uptake on both sides of iliac bones (arrows), right lower lung, and left lung hilus (arrowheads). (E) 99mTc-HMDP bone scintigraphy shows no obvious abnormal uptake.
(A) T1-weighted MR image shows metastases at lumbar spine (L3) and sacrum. (B) CT scan shows osteolytic lesions at L3. (C) 99mTc-MDP scan shows high accumulation at thoracic spine (T10), lumbar spine (L3), and iliac bones (arrows), and unlabeled (cold) lesion at left ninth rib (arrowhead). (D) 18F-FDG PET image shows metastases at thoracic spine (T10) and left ribs but no accumulation at L3.
DISCUSSION
The incidence of bone metastases in the patients examined in this study (38% on a patient basis) seems to be unusually high. We believe that this finding is due to the fact that the patient group contained a large proportion of high-risk patients who showed extrathyroidal extension of the disease or distant metastases.
Earlier studies of bone metastases in patients with breast carcinoma showed that 18F-FDG PET had a similar sensitivity and a higher specificity in detecting bone metastases in comparison with conventional bone scintigraphy (1–3,24)—however, there were conflicting reports, which showed that 18F-FDG PET was less sensitive than conventional 99mTc-bone scintigraphy (25,26). The results indicating that 18F-FDG PET and 99mTc-bone scintigraphy had a similar sensitivity for the detection of bone metastases but that 18F-FDG PET was more specific than 99mTc-bone scintigraphy were also obtained in patients with lung carcinoma (1,27,28). Furthermore, many comparative studies showed different results with regard to the sensitivity and specificity of 18F-FDG PET and conventional 99mTc-bone scintigraphy for the detection of bone metastases of various kinds of carcinoma. 18F-FDG PET was more sensitive and specific than 99mTc-bone scintigraphy for the detection of bone metastases in patients with renal cell carcinoma (11) and esophageal carcinoma (9). 18F-FDG PET also revealed more bone metastatic lesions than did 99mTc-bone scintigraphy, independent of the type of carcinoma or the location of bone metastases (4). A recent report indicated that 18F-FDG PET was more sensitive than 99mTc-bone scintigraphy for the detection of bone metastases in patients with endemic nasophryngeal carcinoma (10). According to Fogelman et al. (29), the efficacy of 18F-FDG PET for the detection of bone metastases in patients with prostate carcinoma has not yet been conclusive. Thus, so far, there is no definite consensus as to the detection of 18F-FDG PET for bone metastases in comparison with 99mTc-bone scintigraphy in various kinds of carcinomas. However, the present study definitely showed that the specificity and the accuracy of 18F-FDG PET for the diagnosis of bone metastases in patients with DTC are higher than those of 99mTc-bone scintigraphy.
In this study, we assessed whole planar images in 99mTc-bone scintigraphy in place of SPECT bone imaging. The most conspicuous observation of our results is that there were only 0.4% false-positive cases in 451 bone segments—which were confirmed to be no bone metastases when examined by 18F-FDG PET—whereas 8.6% were false-positive when examined by 99mTc-bone scintigraphy. Even if we use SPECT bone imaging for 99mTc-bone scintigraphy, it is difficult to imagine that the false-positive cases will be largely decreased.
On the basis of the CT images, bone metastases are classified into the osteoblastic, osteolytic, mixed, and invisible types. Nakai et al. studied bone metastases from breast carcinoma and reported that the sensitivity of 99mTc-bone scintigraphy/18F-FDG PET was 100%/55.6% for the blastic type, 70.0%/100% for the lytic type, 84.2%/94.7% for the mixed type, and 25.0%/87.5% for the invisible type (5). The sensitivity of 99mTc-bone scintigraphy for the blastic type and 18F-FDG PET for the in visible type were significantly higher. On the basis of these results, they concluded that 18F-FDG PET has limitations in depicting metastases of the osteoblastic type, although it is useful for detection of bone metastases from breast carcinoma (5). In a study with bone metastases from breast carcinoma, Abe et al. reported that 18F-FDG PET was superior to 99mTc-bone scintigraphy in detection of osteolytic lesions (92% vs. 73%) but was inferior in the detection of osteoblastic lesions (74% vs. 95%); they concluded that 18F-FDG PET should play a complementary role in detecting bone metastases with 99mTc-bone scintigraphy (6). In the present study, the sensitivities of 18F-FDG PET and 99mTc-bone scintigraphy for the detection of both the osteolytic and the osteoblastic lesions were not largely different (Table 4). However, we cannot conclude that the detectability of 18F-FDG PET for the osteoblastic metastatic lesions of DTC is almost the same as 99mTc-bone scintigraphy because the number of the osteoblastic lesions examined in this study was too small. Elucidation of this problem must await further investigation.
CONCLUSION
On the basis of our results, we conclude that the specificity and the overall accuracy of 18F-FDG PET for the diagnosis of bone metastases in patients with DTC are higher than those of 99mTc-bone scintigraphy and that 18F-FDG PET is superior to 99mTc-bone scintigraphy because of its lower incidence of false-positive results in the detection of bone metastases of DTC.
Footnotes
-
COPYRIGHT © 2007 by the Society of Nuclear Medicine, Inc.
References
- Received for publication January 8, 2007.
- Accepted for publication March 16, 2007.





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Comparison of 18F-fluoride PET/CT, 18F-FDG PET/CT and bone scintigraphy (planar and SPECT) in detection of bone metastases of differentiated thyroid cancer: a pilot study
- The SNMMI Practice Guideline for Therapy of Thyroid Disease with 131I 3.0
- Bone metastases from differentiated thyroid carcinoma
- Bone metastases of differentiated thyroid cancer: impact of early 131I-based detection on outcome