


For few tumors are there such accurate and specific tools for diagnosis and treatment as those routinely used in the management of differentiated thyroid carcinoma (DTC). Highly specific serum thyroglobulin (Tg) measurements signal the presence of residual tumor well before it is manifested by routine imaging studies, and the application of 131I provides the unique opportunity both to visualize and to irradiate metastases even when their exact location is unknown; this strategy often is referred to as empiric 131I therapy. However, this strategy also creates the darker prospect of overtreating patients, a situation that has produced controversy (1,2). This is the latest in a long series of debates concerning virtually every aspect of the management of DTC, a group of tumors comprising papillary, follicular, and Hürthle cell thyroid cancers.
MEASURING OUTCOME
Death and Tumor Relapse Rates
Few patients die from DTC, but up to 30% experience tumor relapse (3), sometimes decades after initial therapy. One third of the recurrences in that study were in distant sites (usually the lungs), and many of the recurrences were detected 20–40 y after initial therapy (3). Most were found by diagnostic whole-body scanning (DxWBS) performed 48–72 h after the administration of 131I, the main test then available to identify metastases; this test is not a sensitive means of revealing occult tumor foci (4–6), many, if not all, of which probably were present at the time of the initial surgery. Indeed, given recent follow-up observations with more sensitive tools, it is highly likely that most of these so-called recurrences were cases of persistent tumor that had fallen below the detection limits of older surveillance tests, causing a delay in treatment that was associated with an increase in cancer-specific mortality rates (3). Observations such as these account for the current recommendation that patients with thyroid cancer undergo lifelong follow-up (5,7). Whether such follow-up will be necessary in the future, when surveillance paradigms become even more accurate, is uncertain. However, it is important to settle this question because there are about 330,000 patients in the United States (8) and 200,000 patients in Europe (7) living with thyroid cancer, and any change in follow-up recommendations likely will affect large numbers of patients.
On pages 1164–1170 of this issue of The Journal of Nuclear Medicine, Kuang (9) reports the results of a literature review designed to evaluate the efficacy of empiric 131I treatment of patients with high serum Tg levels and negative whole-body 131I scan results. To place the findings in perspective, it is useful to review briefly the basis of the current management of DTC and to remember the differences between posttreatment whole-body scanning (RxWBS) done 5–7 d after the administration of 100 mCi or more of 131I and DxWBS—an insensitive test that has vanished from the follow-up paradigms now proposed in the United States and Europe (5,7).
DxWBS
Although 123I has better imaging characteristics than and may be equivalent or superior to 131I for DxWBS imaging (10), DxWBS results nonetheless often are negative in low-risk patients who have residual tumor but no clinical evidence of tumor and who have low or undetectable baseline serum Tg levels during thyroid-stimulating hormone (TSH) suppression that rise with TSH stimulation. The sensitivity of DxWBS for detecting thyroid cancer recurrence is improved when the amount of 131I is increased, but this increase may interfere with the subsequent uptake of 131I on RxWBS (11); this effect, referred to as thyroid stunning, is not always seen (11) but occurs with as little as 3 mCi of 131I and becomes increasingly greater with larger amounts of 131I. Studies show that performing DxWBS during follow-up of low-risk patients usually fails (∼80%) to identify persistent tumor (4,5,7,12–15); many researchers, including myself, believe that it is not necessary to perform DxWBS even before the first postoperative 131I treatment in low-risk patients who have no clinical evidence of tumor after surgery (3,5,7,11,16).
RxWBS
RxWBS may detect new foci of tumor not seen on DxWBS in up to 50% of patients (17), with a substantial number of the newly found lesions being distant metastases (3,18). RxWBS is most likely to yield important new diagnostic information in young patients with high serum Tg concentrations and negative DxWBS results, especially if they were treated previously with 131I (19). Older patients with bulky tumor visualized on radiographs or CT or with previous negative RxWBS results rarely show 131I uptake on subsequent RxWBS (19) and should not be retreated with 131I unless they were not properly prepared for therapy.
INITIAL THERAPY FOR DTC
Total Thyroidectomy
Long-term retrospective cohort studies have provided most of the information about the key clinical and pathologic features that determine outcome in patients with DTC (3). Initial debates that centered on the efficacy of total thyroidectomy and 131I remnant ablation focused mainly on concerns about the complications of therapy. At present, American (20,21) and European (22) surgeons perform total or nearly total thyroidectomy with few complications on almost all patients with DTC. There are several reasons to do this, but the main ones are to lower recurrence rates and to set the stage for thyroid 131I remnant ablation.
Remnant Ablation
There are many analogies between performing routine 131I remnant ablation and empirically treating high serum Tg levels with 131I. Thyroid 131I remnant ablation, which is done to enhance follow-up with Tg and to destroy microscopic residual tumor (23), can be performed with relatively small amounts of 131I—in the range of 30–50 mCi (24). It is an integral part of the initial management of DTC (3,25), even for young patients with low-risk tumors, including children (26,27). A major benefit of remnant ablation is that RxWBS often reveals metastases not seen on DxWBS (3).
A recent meta-analysis by Sawka et al. (28) revealed a trend for a statistically significant treatment effect of remnant ablation on local–regional recurrences and distant metastases but indicated that the results were inconsistent among centers for some outcomes and that the incremental benefit of remnant ablation in low-risk patients treated with bilateral thyroidectomy and thyroid hormone suppression of TSH was unclear (28). The authors called for a randomized trial, but there are almost insurmountable barriers to performing such a study (29). Moreover, low-risk patients are those most likely to benefit from remnant ablation. Hundahl et al. (20) found that in almost 54,000 thyroid carcinoma patients treated in the United States between 1985 and 1995, papillary carcinoma—the tumor with the lowest 10-y cancer-specific mortality rate (7%)—accounted for the majority (∼53%) of the deaths, because it comprised about 80% of all thyroid carcinomas. About two thirds of the thyroid cancer deaths occurred in patients considered to be at low risk by a classification based on age, metastases, extension, and size (20,30).
One reason for inconsistent results of remnant ablation (28) is the short duration of follow-up in most studies. After a median follow-up of 16.6 y, 131I remnant ablation was found to reduce significantly the rates of local–regional recurrences, distant metastases, and cancer-specific mortality (3). Likewise, Chow et al. (31) found that 131I remnant ablation reduced the rates of both local–regional failure and distant metastases, but cause-specific survival was not affected, probably because the mean follow-up was only 9.2 y. In another study, Chow et al. (32) found that 131I remnant ablation for patients with papillary microcarcinoma (tumors of ≤1 cm) significantly reduced the lymph node recurrence rate and also found that the presence of lymph node metastases increased the rate of distant metastases over 11-fold. Even Hürthle cell carcinoma, a tumor that tends to be resistant to 131I therapy, may respond to 131I remnant ablation (33). These studies support the notion that empiric 131I treatment of high serum Tg levels is beneficial, especially when the tumor burden is minimal, but the benefit of therapy measured in terms of a decrease in cause-specific survival may not be apparent for decades after treatment.
CURRENT FOLLOW-UP PARADIGMS
Classification of Tumor Status After Initial Therapy
After total thyroidectomy and 131I remnant ablation, low-risk patients are classified as being free of disease when the following criteria are fulfilled (5,7): all identifiable tumor has been resected; there is no clinical evidence of tumor; postablation RxWBS shows no uptake outside the thyroid bed; neck ultrasonography (US) results are negative; serum anti-Tg antibodies (TgAb) are undetectable; and Tg is undetectable (<1 μg/L) during TSH suppression and stimulation, achieved either by administration of recombinant human TSH (rhTSH) (12) or by withdrawal of thyroid hormone to raise the level of TSH (5,7), producing symptomatic hypothyroidism (7,12).
Goal of Follow-up
The main goal of surveillance is to identify tumor at the earliest possible stage while concurrently distinguishing patients who are free of disease. It is important to differentiate the 2 groups because therapy has the greatest potential to extend survival in the first group while sparing the others from unnecessary 131I therapy and thyroid hormone suppression of TSH, with its potential for producing adverse cardiac events and loss of bone mineral density.
SERUM Tg
Measuring Tg Concentrations over Time
When the TSH level is stable during thyroid hormone therapy, any change in serum Tg usually reflects a change in tumor mass (38), provided that the measurements are made in the same laboratory (39). Recurrent DTC thus is marked by a gradual rise in Tg levels, a pattern that is more useful and has a higher positive predictive value (>80%) (14) than an isolated Tg measurement (∼50%) (4,13). Still, it is possible to interpret a very high isolated Tg level (12,39), which tends to suggest extensive disease that requires aggressive diagnostic testing and therapy.
TgAb
TgAb interfere with Tg measurements made by immunometric assay (IMA) or radioimmunoassay (RIA) methods (39–41). TgAb currently compromise the use of serum Tg as a tumor marker in about 25% of patients with DTC; this rate is much higher than the 11% rate of TgAb found in the general population (39,42). Because even low TgAb levels have the potential to interfere with Tg measurements, all sera should be tested for TgAb by a sensitive IMA method. The magnitude and direction of TgAb interference depend on the type of assay used to measure Tg (41). In the presence of TgAb, serum Tg levels are consistently undetectable when measured by IMA, which is the type of assay used by most commercial laboratories (41). RIA methods for measuring Tg levels generally are less prone to TgAb interference, but the direction and magnitude of interference are less predictable and TgAb may elevate Tg levels (41). TgAb levels can be used as a surrogate marker for Tg levels. All major antithyroid antibodies, including TgAb, may disappear over time; TgAb have been shown to disappear 2–4 y after complete ablation of thyroid tissue, supporting the notion that TgAb production depends on persistent tumor antigen (43).
Serum Heterophile Antibodies (HAB)
HAB, which are often found in human sera, can form a bridge between capture and detection antibodies in IMA systems, leading to a false elevation in serum Tg levels. Preissner et al. (44) found that HAB interference caused false Tg elevations in up to 3% of their patients; this finding was serious because the Tg levels often were in the range commonly recommended for empiric 131I therapy (44). HAB interference should be suspected when Tg levels do not match the clinical findings, especially when Tg levels fail to rise and fall with TSH stimulation and suppression or when Tg levels fail to follow a straight line with serial dilution of the serum specimen. The simplest thing to do is to remeasure Tg levels in another laboratory that takes explicit steps to block HAB interference; this procedure should be carried out before empiric treatment of a high serum Tg level if there is any question about HAB interference (41). HAB interference also can be transient (44); therefore, falling serum Tg levels after 131I therapy may not necessarily be evidence of successful 131I treatment but may simply reflect a spontaneous decrease in HAB levels rather than a true decline in Tg levels as a result of treatment. In a study (45) of 131I therapy of Tg-positive, scan-negative patients, serum Tg levels fell in a historical control group that had not received 131I therapy.
IMAGING STUDIES IN PATIENTS WITH HIGH SERUM Tg CONCENTRATIONS
Although many different types of imaging studies are available for patients thought to have a thyroid cancer recurrence, most are neither cost-effective nor necessary early in the patient’s evaluation.
Neck US
For patients with high serum Tg levels, US is the first imaging study performed in my clinic. The central and lateral cervical compartments often reveal small (<1-cm) malignant lymph nodes, even in patients with undetectable serum Tg after TSH stimulation (46–48). Size alone is not a good criterion for malignancy. The use of a 1-cm cutoff value for differentiating benign and malignant lymph nodes often fails to identify smaller malignant lymph nodes, which are more reliably recognized by their shape and other characteristics (49). Neck US combined with measurement of TSH-stimulated serum Tg levels has the highest diagnostic accuracy for detecting persistent neck tumors. Pacini et al. (37) found that US and measurement of rhTSH-stimulated serum Tg levels used together had the highest sensitivity (96%) and negative predictive value (99.5%) compared with measurement of rhTSH-stimulated serum Tg levels, DxWBS, and US used alone. Others reported similarly good results with US, even in children (47,48). Torlontano et al. (34) found that neck US identified lymph node metastases in 67% of patients with rhTSH-stimulated Tg levels of >5 ng/mL, in 13% with Tg levels of 1–<5 ng/mL, and in only 3% with Tg levels of <1 ng/mL.
18F-FDG PET
A variety of imaging studies have been useful for studying patients with high serum Tg levels and negative RxWBS results. TSH-stimulated 18F-FDG PET/CT fusion seems to have the highest sensitivity and is the preferred imaging method, although cost remains high (50). An elevated serum Tg level (>10 μg/L) with negative RxWBS results currently is the main indication for 18F-FDG PET (51–54), which often identifies tumor that is amenable to surgery (55,56). For example, in 1 study (54), 18F-FDG PET results were found to be positive in 70% of 27 patients. Of these patients, 14 had tumors in cervical lymph nodes, 2 had mediastinal lymph node metastases, 3 had lung metastases, and 2 had bone metastases that resulted in surgical intervention for 17 of the patients, 82% of whom achieved a disease-free status. The sensitivities of 18F-FDG PET for detecting metastases in 1 study (57) were 11%, 50%, and 93% in patients with Tg levels of <10, 10–20, and >100 ng/mL, respectively. Sensitivity is enhanced by raising serum TSH levels either by thyroid hormone withdrawal (52) or by rhTSH administration (58).
18F-FDG PET also provides prognostic information. 18F-FDG-avid metastatic DTC lesions are resistant to 131I treatment (59), a situation that portends a poor prognosis. Wang et al. (59) found that the 3-y survival rates were 96% and 18% for patients with 18F-FDG PET volumes of ≤125 and >125 mL, respectively. No cancer deaths occurred in 66 patients with 18F-FDG PET–negative results, including 10 patients who had distant metastases but who were alive and well at the end of the follow-up period; however, almost 70% of 59 patients with 18F-FDG PET–positive results died during the same period.
DIFFERENTIAL DIAGNOSIS OF HIGH Tg LEVELS AND NEGATIVE RxWBS RESULTS
In the past, the most common scenario for high serum Tg levels and negative imaging study results occurred when DxWBS had been done to identify a tumor. Now the most common problem is that the patient has received empiric 131I therapy for an elevated serum Tg level and the RxWBS results are negative.
Before empiric 131I treatment is entertained, certain clinical situations other than persistent tumor should be considered; these include false-positive serum Tg levels from HAB and thyroid injury caused by 131I therapy or surgery, which may elevate serum Tg levels for 4–6 wk (39). When the serum Tg level during TSH suppression is detectable or rises above a certain cutoff value with rhTSH stimulation or thyroid hormone withdrawal and RxWBS results are negative, the usual presumption is that the tumor does not concentrate 131I. However, one must be certain that there were no technical problems in the preparation for the administration of 131I and that thyroid stunning did not occur during recent preceding DxWBS (11). Technical problems are a common cause of a false-negative RxWBS, particularly when physicians are unfamiliar with the routines used in preparing patients for 131I treatment. I almost never perform DxWBS in this situation to avoid stunning. Otherwise, the main differential diagnoses for negative RxWBS results include the following: a TSH level that is too low after thyroid hormone withdrawal to stimulate 131I uptake; an excess iodine pool from radiographic contrast material or drugs or failure to adhere to a low-iodine diet; metastases that are too small to visualize on RxWBS (i.e., the Tg level is too low for treatment); a very short biologic half-life of 131I (retention time) in the tumor; and reduced or absent sodium–iodine symporter function in the tumor.
According to a study carried out by Maxon et al. (60), a short effective half-life of 131I (which includes both the biologic turnover of iodine and isotope decay) is the major cause of failure of 131I therapy. This property may be a more important cause of negative RxWBS results than reduced or absent sodium–iodide symporter function.
EMPIRICALLY TREATING HIGH SERUM Tg LEVELS
The current diagnostic paradigm used to identify residual tumor during follow-up is so sensitive that it sets the stage for one of the more difficult management problems that clinicians encounter during the follow-up of patients with DTC: unexplained high serum Tg levels. Unless one opts to completely forgo 131I therapy until a randomized prospective trial is done—the prospect of which is even more foreboding than a randomized trial of 131I remnant ablation (29)—there are several important therapeutic questions that must be answered. Perhaps the most important are as follows: What are the frequency and location of tumors treated only on the basis of high serum Tg levels? Why and how should patients be treated? What is the evidence that treatment is efficacious? The answers are elusive and have led to wide differences in opinion concerning the treatment of this group of patients (1,13,61).
Frequency and Location of Tumors
In some studies (6,62,63), RxWBS performed after the administration of 100 mCi of 131I revealed uptake in tumor foci in the neck or at distant sites in up to 80% of patients with high serum Tg levels and no other evidence of tumor, including negative results of DxWBS with 2–5 mCi of 131I. However, the frequency of metastases depends on patient selection and the Tg level used to trigger 131I therapy. An analysis of 8 studies found that rhTSH-stimulated Tg levels increased >2 μg/L in 21% of 784 patients who were found to be clinically free of tumor and had baseline serum Tg levels of <1 μg/L (5). About one third of those with Tg levels of >2 μg/L (∼7% of 784 patients) had metastases, one third of which (∼2%) were in the lungs; the other tumors were in the neck and mediastinum (5). DxWBS failed to identify 80% of the tumors.
Evidence of Therapeutic Efficacy of Empiric 131I Therapy
Kuang (9) summarizes the literature on this issue and reaches the conclusion that 131I therapy should be individualized according to the clinical characteristics of the patient. For 310 patients reported in the literature who were empirically treated with 131I, Kuang found that slightly more than 59% had positive RxWBS results after 131I therapy and that serum Tg levels decreased in about 72% of the treated patients. Kuang concluded that empiric 131I therapy may be justified for a Tg cutoff value of 10 μg/L. These observations relate more to negative DxWBS results. Most of the studies did not have a control arm, and although Tg levels fell, most patients did not achieve complete remission. When the RxWBS results were positive, foci of 131I uptake were found in a variety of locations, including the thyroid bed, regional lymph nodes, and distant metastases. These findings make it difficult to sort out when empiric 131I may be most efficacious.
There are no prospective controlled studies to show that cancer-specific survival is enhanced by empiric 131I therapy based on high serum Tg levels alone, without imaging evidence of tumor, compared with waiting until the tumor becomes evident. Still, several benchmark studies strongly support the idea of empirically treating patients with 131I for high serum Tg levels without imaging evidence of tumor. In 1988, Schlumberger et al. (62) were the first to report that empiric 131I therapy was effective in some patients with DTC. They reported finding lung metastases on whole-body 131I scans as late as 24 y after initial therapy in 23 patients with normal chest radiographs, almost one half of whom also had lung micronodules identified by CT. Lung metastases were documented by DxWBS with 2 mCi of 131I in 11 patients and by RxWBS with 100 mCi of 131I in 12 patients. After all of the patients were treated with 131I, no uptake was found on the last RxWBS with 100 mCi of 131I in 20 patients (87%). The serum Tg levels became undetectable during thyroid hormone treatment in 8 patients (35%), and CT scans showed that the lung micronodules had disappeared in 7 patients (30%). Lung biopsy specimens did not show evidence of disease in 2 patients, and no patient developed radiation lung fibrosis. In a more recent publication, Schlumberger (64) reported complete remission and 10-y survival rates, respectively, of 96% and 100% in 19 patients with tumors found only on RxWBS, 83% and 91% in 55 patients with metastases found only on DxWBS, 53% and 63% in 64 patients with micronodules seen on chest radiographs, and 14% and 11% in 77 patients with macronodules seen on chest radiographs.
Bal et al. (65) reported outcomes for 28 children and adolescents with lung metastases from DTC; these patients comprised 23% of the children and adolescents with DTC in their cohort. Chest radiographs were normal in 21 (75%) of the children with lung metastases, all of which were identified by whole-body 131I scanning. The metastases were seen in only about half (54%) of the children on the first postsurgery 2- to 3-mCi DxWBS, with the rest being discovered on the first postablation RxWBS (14%), or the second or third RxWBS study (35%). The mean ± SD first 131I and cumulative 131I doses were 75.4 ± 39.5 and 352 ± 263 mCi, respectively. Children with positive initial radiographs required significantly more 131I for their first and cumulative 131I therapies and required more 131I treatments than did children with negative radiographs. Micronodular pulmonary metastases were seen in 5 of 18 children who underwent CT. After an average of 3.3 131I treatments and a mean ± SD duration of 33.2 ± 28.5 mo, lung lesions disappeared and Tg became undetectable (≤10 ng/mL after thyroid hormone withdrawal) in 70% (14) of the patients. Four other children had no radiologic or scintigraphic evidence of pulmonary metastases after treatment, but Tg levels were high, and 2 had persistent disease.
Negative Aspects of Empiric 131I Therapy
Kuang (9) summarizes some of the important immediate and long-term complications of 131I therapy that must be balanced against the potential advantages of 131I treatment. Although long-term complications, such as leukemia and bladder cancer, tend to be related to large cumulative 131I radiation doses (66), acute complications, especially parotid gland injury (67), xerostomia, and injury to lacrimal ducts (68), can occur with relatively small amounts of 131I, such as those used for empiric treatment of high serum Tg levels. On the other hand, smaller tumors require less 131I to ablate. The question here is whether one must visualize tumors to tip the balance toward treating them with 131I. I believe that there is enough evidence that waiting to treat tumors may not be in a patient’s best interests.
MY APPROACH TO TREATING PATIENTS WITH HIGH SERUM Tg LEVELS AND NEGATIVE IMAGING STUDIES
The most common scenario for referral to my clinic is an rhTSH-stimulated Tg level of >2 μg/L with negative findings for tumor. For such patients, I first perform a US examination of the neck, where about two thirds of tumors causing the problem reside. If the neck US examination is positive, a lymph node sample is obtained by fine-needle aspiration biopsy for cytologic evaluation, and the needle washing is analyzed for Tg levels (69). If either is diagnostic, surgery and 131I therapy are considered. If the US examination is negative and the Tg levels are high enough, I consider 131I therapy if the evidence for the lack of 131I uptake is based on negative DxWBS results or if there is uncertainty that the negative RxWBS results were the result of the patient not having been prepared properly for 131I therapy or having been contaminated with iodine.
The exact Tg level that should prompt empiric 131I treatment remains a matter of debate, but the higher the Tg level is at the time of treatment, the more likely that RxWBS will show 131I uptake (3). Rising Tg levels—a reasonable guideline is a doubling of Tg levels over 12 mo—is a considerably more reliable indicator of tumor than is a single Tg measurement. I usually advise 131I therapy when the Tg levels are rising and reach 5 μg/L after rhTSH stimulation or 10 μg/L after thyroid hormone withdrawal, or one can simply repeat the rhTSH testing annually—most patients in my clinic refuse annual thyroid hormone withdrawal—until the serum Tg reaches a level that the physician and patient feel comfortable treating. Although a Tg level of 2 μg/L was established as the best cutoff value for detecting metastases in a large multicenter study with rhTSH (12) and was verified by a subsequent study (5) with rhTSH, there is enough variation in Tg testing that the cutoff value should be established for each clinic. Empiric 131I therapy with 100 mCi should be considered especially for young adults and children who have had previous therapy for metastases that concentrate 131I. For children, 131I activity should be adjusted to give the equivalent of about 100–150 mCi according to body size (square meters) (70). Children and young adults have the highest potential for having diffuse lung metastases seen only on RxWBS; such metastases show the best response to 131I.
If a patient opts for 131I therapy, I measure 24-h urine iodine levels, give instructions to the patient regarding a 2-wk low-iodine diet, prepare the patient with lithium for 1 wk to enhance 131I retention (71), and use rhTSH to stimulate the uptake of 100 mCi of 131I. Thyroid hormone is stopped for 4 d before and 1 d after 131I treatment (72) to shrink the total-body iodine pool. If there is any question about HAB before therapy, I measure Tg levels in a laboratory that explicitly checks for the presence of these antibodies. If RxWBS results are negative after the administration of 100 mCi of 131I in a patient prepared in this way, no further 131I is administered, and rhTSH-stimulated 18F-FDG PET/CT is performed to identify non-131I-avid tumor and to provide an estimate of prognosis.
If a patient’s status is uncertain after the initial evaluation, careful observation over time with neck US and measurement of TSH-stimulated serum Tg levels is a good strategy because high serum Tg levels may decline spontaneously over several years after initial 131I ablation therapy or may rise to prompt empiric 131I therapy. If they remain high but stable over time, HAB interference should be excluded.
There is no doubt that this paradigm (summarized in Figs. 1–3) will change as more is learned about how to treat these patients, but a therapeutic approach with 131I seems reasonable for some patients on the basis of present knowledge of therapy for DTC. The notion of treating patients with high serum Tg levels but negative whole-body 131I scan results probably is outmoded, because in most studies such treatment has been used for patients with negative DxWBS results, which are now known often to be negative in the presence of tumor. The current most common problem is a negative RxWBS with high serum Tg levels, about which the above discussion applies. It is better to consider these findings simply to be the natural early expression of persistent tumor observed during the early follow-up of patients with DTC measured in terms of serum Tg levels.

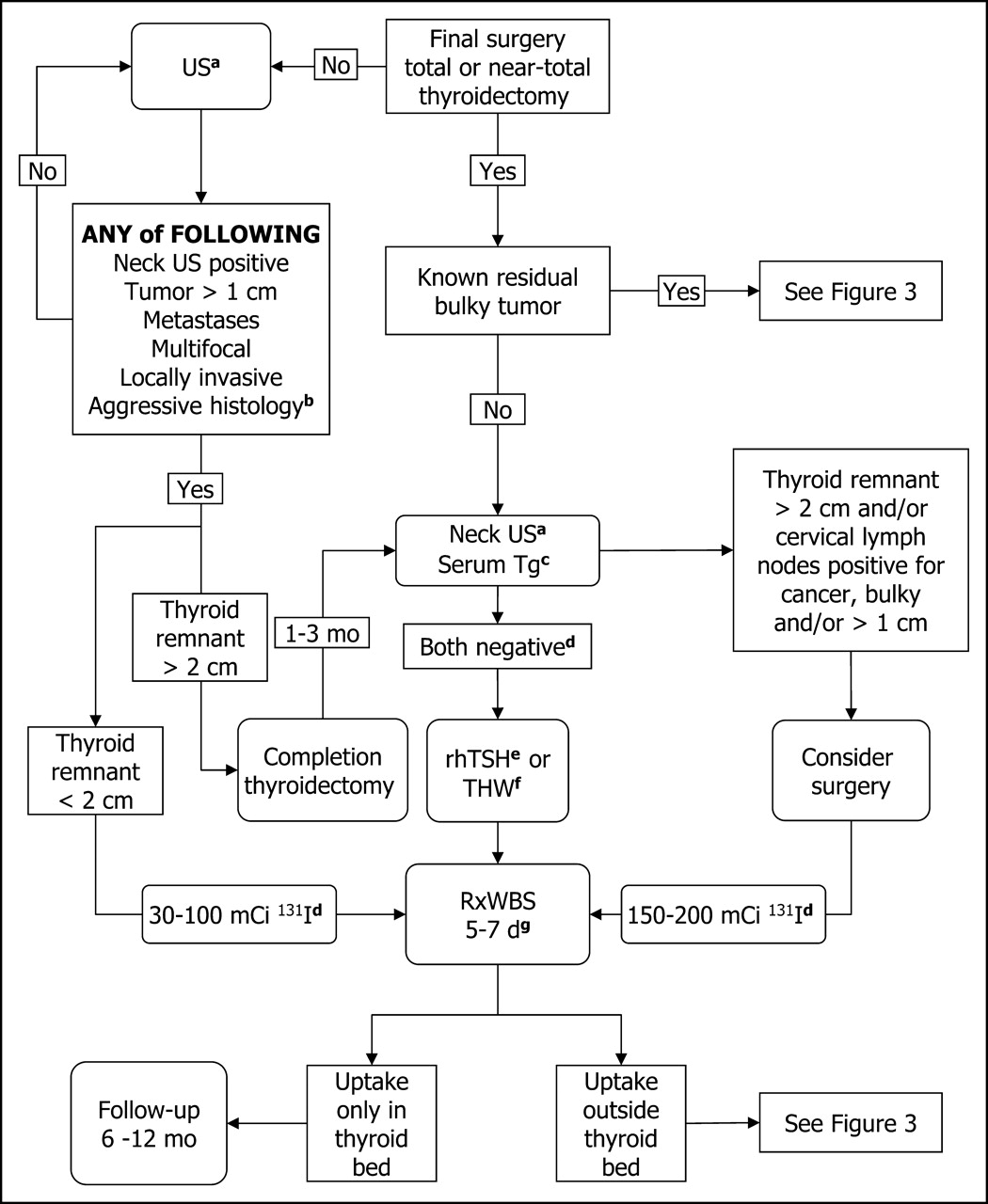
Algorithm for initial follow-up of patients with differentiated thyroid carcinoma, about 1–3 mo after surgical ablation of remnant. See Appendix for footnotes.

Algorithm for follow-up at 6–12 mo after surgical ablation of remnant. See Appendix for footnotes.

Algorithm for follow-up at 12 mo or more after surgical ablation of remnant, when empiric 131I therapy is being considered. See Appendix for footnotes.
APPENDIX
Footnotes to Figures
aNeck US is usually not performed until 6–8 wk after surgery.
bVascular invasion; thyroid capsular invasion; and tall cell, columnar cell, diffuse sclerosing, insular variant, invasive follicular, or Hürthle cell carcinoma.
cSerum Tg is falsely elevated for 4–6 wk by injury from surgery.
dDxWBS is not necessary (73,74).
erhTSH is not approved by the U.S. Food and Drug Administration for preparing patients for remnant ablation but was approved for this indication in 2005 in Europe and is administered as follows: 0.9 mg rhTSH intramuscularly on 2 consecutive days, followed by 131I therapy on the third day and RxWBS 4–7 d after 131I administration.
fThyroid hormone withdrawal.
gRxWBS is done 5–7 d after therapeutic 131I administration.
hTg is usually measured by IMA (see text).
iTg RIA undergoes less interference than does Tg measured by IMA.
jDo not stimulate with TSH, because after TSH stimulation with rhTSH or THW, the results for Tg are invalidated by TgAb in the serum even when Tg is measured by RIA (see text).
kSee text for levels of Tg at which therapy should be considered; for fine-needle–positive identification of large (>1-cm) or multiple tumors, modified neck dissection is usually advised for lateral neck compartments, or complete compartment dissection for central compartment.
lRemeasure Tg in another laboratory or a laboratory that explicitly checks for heterophile antibodies.
mFor fine-needle–positive identification of large (>1-cm) or multiple tumors, modified neck dissection is usually advised for lateral neck compartments, or complete compartment dissection for central compartment.
nThis is especially important if PET scan shows extensive uptake of 18F-FDG. Exceptions occur if patient had inadequate preparation before previous RxWBS with negative findings.
oA target of 100 μg/24 h is acceptable; the ideal target is 50 μg/24 h after a 2-wk low-iodine diet.
pKoong et al. (71).
qRxWBS should first be done at 2–5 d after 131I if rhTSH is used for preparation and can be repeated in 24 h if uptake is too intense.
rMeasurement of TSH levels after rhTSH administration is not necessary.
Footnotes
Received Apr. 13, 2005; revision accepted Apr. 15, 2005.
For correspondence or reprints contact: Ernest L. Mazzaferri, MD, 4020 S.W. 93rd Dr., Gainesville, FL 32608-4653.
E-mail: mazz01{at}bellsouth.net
REFERENCES
In this issue





{kind=link}
{kind=link}
{kind=link}
Jump to section
- Article
- MEASURING OUTCOME
- INITIAL THERAPY FOR DTC
- CURRENT FOLLOW-UP PARADIGMS
- SERUM Tg
- IMAGING STUDIES IN PATIENTS WITH HIGH SERUM Tg CONCENTRATIONS
- DIFFERENTIAL DIAGNOSIS OF HIGH Tg LEVELS AND NEGATIVE RxWBS RESULTS
- EMPIRICALLY TREATING HIGH SERUM Tg LEVELS
- MY APPROACH TO TREATING PATIENTS WITH HIGH SERUM Tg LEVELS AND NEGATIVE IMAGING STUDIES
- APPENDIX
- Footnotes
- REFERENCES
- Figures & Data
- Info & Metrics