


Abstract
Prostate-specific membrane antigen (PSMA) is a well-established target for developing radiopharmaceuticals for imaging and therapy of prostate cancer (PCa). We have recently reported that novel 99mTc-labeled small-molecule PSMA inhibitors bind with high affinity to PSMA-positive tumor cells in vitro and localize in PCa xenografts. This study reports the first, to our knowledge, human data in men with metastatic PCa and in healthy male subjects. Methods: Under an exploratory investigational new drug, using a cross-over design, we compared the pharmacokinetics, biodistribution, and tumor uptake of 99mTc-MIP-1404 and 99mTc-MIP-1405 in 6 healthy men and 6 men with radiographic evidence of metastatic PCa. Whole-body images were obtained at 10 min and 1, 2, 4, and 24 h. SPECT was performed between 3 and 4 h after injection. Results: Both agents cleared the blood rapidly, with MIP-1404 demonstrating significantly lower urinary activity (7%) than MIP-1405 (26%). Both agents showed persistent uptake in the salivary, lacrimal, and parotid glands. Uptake in the liver and kidney was acceptable for imaging at 1–2 h. In men with PCa, both agents rapidly localized in bone and lymph node lesions as early as 1 h. SPECT demonstrated excellent lesion contrast. Good correlation was seen with bone scanning; however, more lesions were demonstrated with 99mTc-MIP-1404 and 99mTc-MIP-1405. The high-contrast images exhibited tumor-to-background ratios from 3:1 to 9:1 at 4 and 20 h. Conclusion: Compared with the standard-of-care bone scanning, 99mTc-MIP-1404 and 99mTc-MIP-1405 identified most bone metastatic lesions and rapidly detected soft-tissue PCa lesions including subcentimeter lymph nodes. Because 99mTc-MIP-1404 has minimal activity in the bladder, further work is planned to correlate imaging findings with histopathology in patients with high-risk metastatic PCa.
It is estimated that in 2014 there will be 233,000 new cases of prostate cancer (PCa) diagnosed and that 29,480 men will die of the disease (1,2). When detected early, and when disease is localized to the prostate gland, the 5-y survival rate is nearly 100%. However, once PCa has spread beyond the prostate, survival rates fall dramatically (2). The primary goal of staging is to define the anatomic extent of the tumor and to distinguish patients with organ-confined, locally invasive, or distant metastatic disease. Because accurate staging is critical to determine appropriate patient management, it follows that sensitive and specific localization of disease is a vital component of staging.
Prostate-specific antigen (PSA) testing cannot easily distinguish between low-risk and high-risk disease so as to appropriately direct treatment (3). Current diagnostic imaging modalities are suboptimal for detecting local disease, lymphatic spread, and distant metastatic disease. Confirmatory and disease staging/monitoring imaging methods, such as CT, MR imaging, bone scanning, and 111In-capromab pendetide imaging, suffer from poor sensitivity and specificity, significantly limiting their value in therapy-selection decisions (4,5). Early detection of skeletal metastases is critical in the management of patients with high-risk PCa. Newly diagnosed patients with localized disease and no metastases may benefit from radical treatment with curative intent. In contrast, most guidelines recognize that patients with bone metastases should forgo local therapy to avoid unnecessary side effects and be treated with systemic therapy instead (6). Early metastases to bone may be missed with bone scanning because this technique relies on osteoblastic activity (mineralization) rather than detection of actual tumor cells (7). New molecular imaging approaches to more accurately assess the status of the disease and the progress of therapy may facilitate the selection of optimal treatment and improve patient outcomes.
PSMA (prostate-specific membrane antigen), also known as folate hydrolase I or glutamate carboxypeptidase II, a transmembrane, 750 amino acid, type II glycoprotein, is expressed virtually by all PCa (8), including metastatic PCa (9,10). The expression of PSMA is further increased in poorly differentiated, metastatic, and hormone-refractory carcinomas (11,12) as well as after androgen-deprivation therapy (13) and in lymph node metastases (14). In addition, increased expression of PSMA in primary PCa correlates with other adverse traditional prognostic factors and independently predicts disease outcome (11,15). Therefore, PSMA is an ideal target for developing imaging biomarkers for PCa (16–19).
PSMA is highly homologous to N-acetylated R-linked acidic dipeptidase, a neuropeptidase that produces the neurotransmitter glutamate and N-acetylaspartate through the hydrolysis of N-acetylaspartylglutamate (20–22). The investigators at Molecular Insight Pharmaceuticals (MIP) developed a series of novel glutamate-urea (Glu-urea) amino acid heterodimeric inhibitors of PSMA for developing SPECT radiopharmaceuticals using 123I or 99mTc (23–26). It has been reported recently that 2 radioiodinated small molecules, 123I-MIP-1072 and 123I-MIP-1095, localized to lesions in bone and soft tissue that correlated with radiologic evidence of metastatic PCa (27). Because 99mTc is the optimal radionuclide for developing SPECT radiopharmaceuticals, the investigators at MIP developed 2 high-affinity small-molecule PSMA inhibitors, MIP-1404 and MIP-1405, which can be labeled with 99mTc based on novel tricarbonyl chemistry (25,26).
A particular advantage of an exploratory investigational new drug application (IND) is to rapidly bring similar compounds into the clinic to confirm preclinical data. To compare the biodistribution of 99mTc-MIP-1404 and 99mTc-MIP-1405 in the human subject, a phase I study in healthy human subjects and patients with metastatic PCa was performed on the basis of crossover design (28). We report here the results of this preliminary clinical study comparing the pharmacokinetics, biodistribution, tumor uptake, and radiation dosimetry of these 2 novel radiopharmaceuticals for PSMA and PCa imaging studies.
MATERIALS AND METHODS
Study Design
The study was an open-label, crossover design of 2 novel study drugs, 99mTc-MIP-1404 and 99mTc-MIP-1405, involving 6 healthy controls and 6 patients with metastatic PCa. The sequence of study drugs was randomized. This phase I clinical study was performed under an exploratory IND at a single site (New York Weill Cornell Medical Center) and was approved by the institutional review board.
For healthy subjects, the inclusion criteria required normal rectal examination and a PSA of 4.0 ng/mL or less. For patients, the inclusion criteria required a documented history of prostate PCa by histopathology and radiologic evidence of metastatic disease with rising PSA. Patients were required to undergo bone scanning within 1 mo and CT/MR imaging within the last 3 mo before the first dose administration of the study drug and have received no prior therapies within the last 3 mo. All subjects were required to use condoms or agree to use an acceptable form of birth control throughout the study period. Patients who received an IND drug within the past 30 d before enrollment and androgen-deprivation therapy or other forms of hormonal therapy for a period of 14 d before screening were excluded from this protocol. The subjects were invited to participate, after signing an informed consent form, and then were screened for eligibility. After undergoing baseline examinations, each subject received the first study drug and then was followed for 24 h to obtain whole-body planar γ-camera images and blood and urine samples for assay of radioactivity. SPECT/CT imaging of the pelvis, chest, or abdomen was performed at 3 h. On completion of a 2-wk washout period, the same patient was administered the second study drug and underwent the evaluation described above.
Study Drugs
The synthesis of study drug precursors MIP-1404 and MIP-1405 (Fig. 1) and radiolabeling with 99mTc were described previously (25,26). These PSMA inhibitors were synthesized by the attachment of glutamate-urea-lysine and glutamate-urea-glutamate pharmacophore to novel, hydrophilic single-amino-acid chelate (29). The radiolabeling of the study drug precursors MIP-1404 and MIP-1405 with the novel intermediate {99mTc(CO)3}+ to form the desired metal complexes was accomplished in 2 steps using standard methodology (25,29). IsoLink kits (Covidien) were used to generate the intermediate {99mTc(CO)3}+ in the final preparation of study drugs 99mTc-MIP-1404 and 99mTc-MIP-1405 (Fig. 1). Briefly, 7.4 GBq (200 mCi) in 1–2 mL of sodium 99mTc pertechnetate was added to an IsoLink kit, followed by the addition of study drug precursor (100 μg in 0.1 mL). The mixture was incubated for 1 h at 100°C. After neutralization and C18 Sep-Pack (Waters) purification, the study drug was collected in 1 mL of absolute ethanol and diluted with 9 mL of sterile saline. Subsequently, the final drug formulation was sterilized by passing through a 0.22 μm membrane filter. The radiochemical and chemical purity of the final drug formulation was determined using high-performance liquid chromatography. In addition, tests for endotoxins and sterility were also performed on every batch of the study drug preparation.
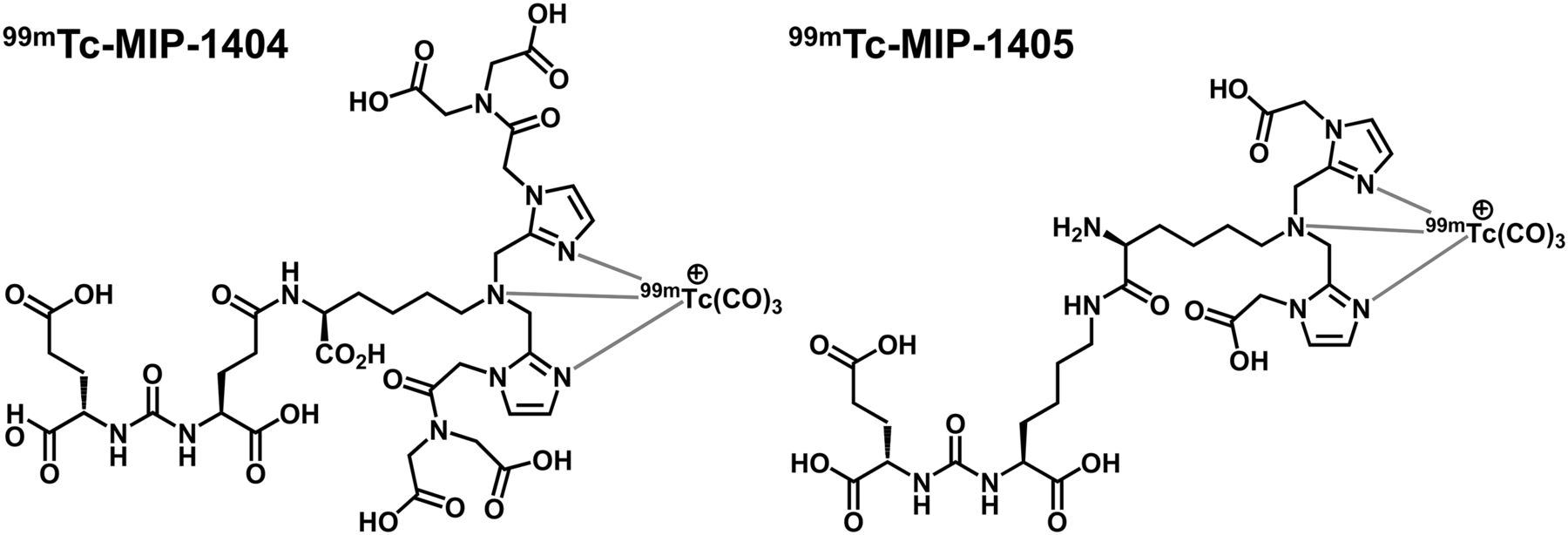
Structures of small-molecule inhibitors of PSMA, 99mTc-MIP-1404 and 99mTc-MIP-1405.
Administration of Study Drugs
Each subject was randomly assigned to receive intravenously 740 ± 111 MBq of either 99mTc-MIP-1404 or 99mTc-MIP-1405, followed 2 wk later by the second compound.
Pharmacokinetics and Excretion
Blood samples were collected at 0.1, 0.5, 1, 2, 4, 6, and 24 h after injection of 99mTc-MIP-1404 and 99mTc-MIP-1405; urine was collected and pooled at time intervals of 0–1, 1–2, 2–4, and 4–24 h after dosing. Blood and urine samples were analyzed for 99mTc activity using γ well counting. The pharmacokinetic data were obtained with WinNonlin 4.1 software (Pharsight) as previously described (27). Blood and tissue concentration time data were computed and pharmacokinetic parameters, for example, maximum concentration in plasma (Cmax) and mean residence time (MRT) were generated. Total clearance was calculated as dose divided by area under the curve and steady-state volume of distribution as the product of total clearance and MRT. Distribution half-life (T1/2α) and elimination half-life (T1/2β) were obtained by fitting the 2-compartment model with bolus input and first-order output. The rate of urinary clearance and 99mTc activity recovered in the urine was also computed by noncompartmental analysis (WinNonlin Model 211; Pharsight).
Image Acquisition
Whole-body scintigraphy was performed at 10 min and 1, 2, 4–6, and 24 h after injection. Anterior and posterior planar projections were acquired using a dual-head γ camera (Infinia Hawkeye 4 GP-3; GE Healthcare) equipped with low-energy high-resolution collimators. Scan velocity was incrementally slowed from 15 cm/min at 10 min 1 and 2 h after injection to 10 cm/min at 4 h and 5 cm/min at 24 h. A matrix size of 256 × 1,024 pixels and a symmetric window of 20% centered on a 140-keV photopeak were used for all acquisitions. A single imaging standard of approximately 18.5 MBq (500 μCi) was placed in the field of view for each whole-body acquisition to allow for decay and scan speed correction across all time points.
Tomographic SPECT of the abdomen, pelvis, or chest was obtained at approximately 3–5 h after injection. When available, SPECT/CT was performed to obtain measured attenuation-correction maps and to aid in anatomic localization using standard low-dose CT parameters. SPECT parameters consisted of a 360° rotation, 30 s per stop, and a 3° azimuth using a step-and-shoot technique. A matrix size of 128 × 128 and a symmetric window of 15% centered on a 140-keV photopeak were used for all SPECT acquisitions. Raw SPECT data were reconstructed into 3-dimensional volumes and corrected for attenuation on a Hermes workstation (Hermes Medical Solutions) using ordered-subset expectation maximization iterative reconstruction methods (3 iterations/30 subsets) and filtered with a Butterworth filter (1.2 cutoff, 5 order).
Image Analysis
Regions of interest (ROIs) were created over the imaging standard, tissues, and healthy organs on each anterior and posterior planar whole-body projection to extract count data corresponding to 99mTc-MIP-1404 and 99mTc-MIP-1405 uptake. Count data, including the whole body, various organs, and urinary bladder contents, were collected. The mean count for each ROI at the first postdose image was divided by the mean count for the whole-body ROI at the first postdose image. The resulting ratio is expressed as a percentage and referred to as the percentage injected dose (%ID) for that organ at the initial time point. Data describing the %ID in each source organ were mathematically simulated using monoexponential functions with a nonlinear least-squares regression algorithm and SAAM II software (version 1.2; The Epsilon Group, a Division of MAS) (30). Additional analyses of target-to-background (T/B) count ratios were performed on planar and reconstructed SPECT images as previously described (27). T/B ratios for lesions within the SPECT field of view were calculated by obtaining counts from a circular 10-pixel ROI in the axial projection and an equal-sized ROI placed immediately adjacent as the background. The abnormal foci of activity on the scans (identified by the physicians) were used for measuring the radiotracer uptake. Only the lesions with 2 times the background were defined as positive uptake and included in the estimation of T/B values. The T/B ratios were measured at 1, 2, 4, and 20 h.
Organ Radiation-Absorbed Dose Estimates
The OLINDA/EXM software was used to estimate radiation-absorbed dose to target organs (31,32). The adult male model was used for all patients. The urinary bladder was assumed to be voided regularly at 4.8-h intervals (i.e., 5 times per day). The urinary bladder residence times were computed using OLINDA/EXM implementation of the dynamic bladder model of Cloutier et al. (33). The small bowel and upper and lower large intestinal residence times were computed using the provided implementation of the ICRP publication 30 (34) gut transit model for the adult male. The radiation doses to salivary glands and tumors were determined using spheric S values as implemented in OLINDA/EXM.
Safety
Safety data were collected from treatment-emergent adverse event reports, pre- versus postinjection electrocardiograms, physical examinations, vital signs, and laboratory measurements (including clinical chemistry, hematology, and urinalysis). The safety analysis was performed with data from all subjects. Adverse events were coded by the MedDRA dictionary (http://www.meddra.org/) and were summarized by occurrences and percentages of patients according to CTC (National Cancer Institute Common Terminology Criteria) grade, body system, preferred term, intensity, and causal relationship to study agent. SAS software (version 9.1; SAS Institute) was used for the safety analysis.
RESULTS
Preparation of 99mTcMIP-1404 and 99mTc-MIP-1405
Each milliliter of the sterile, apyrogenic drug product (99mTc-MIP-1404 or 99mTc-MIP-1405) in physiologic saline contained approximately 92.5–185 MBq of 99mTc activity and 0.1 mL (0.79 mg) of ethanol. The radiochemical purity of the final drug formulation was 94.2% ± 1.4% for 99mTc-MIP-1404 and 97.2% ± 1.7% for 99mTc-MIP-1405. The amount of free 99mTc as pertechnetate was less than 1.0%. The specific activity at the end of synthesis was about 37–44.4 MBq/μg of either drug product. The average dose injected in each subject was 784.4 ± 59.2 MBq and approximately 20 μg of the drug product.
Subject Population
Eight healthy subjects and 7 patients were recruited in the protocol. Two of 8 healthy subjects dropped out of the study after the screening tests. Of the 7 patients recruited, 1 dropped out after the study and did not complete the protocol. The remaining 6 patients had a documented history of PCa by histopathology and had radiologic evidence of metastatic disease with rising PSA (Table 1). The PSA levels in 5 of 6 healthy controls were 0.8–3.3 ng/mL, and only 1 healthy subject had a PSA of 9.3 ng/mL. In patients with PCa, the PSA varied from 2.0 to 48.4 (13.8 ± 12.3) ng/mL. Four of the 6 patients had intact prostate glands, and 3 of 6 patients had prior radiation therapy.
Demographics and Clinical Data for Patients with Metastatic PCa
Pharmacokinetics and Excretion
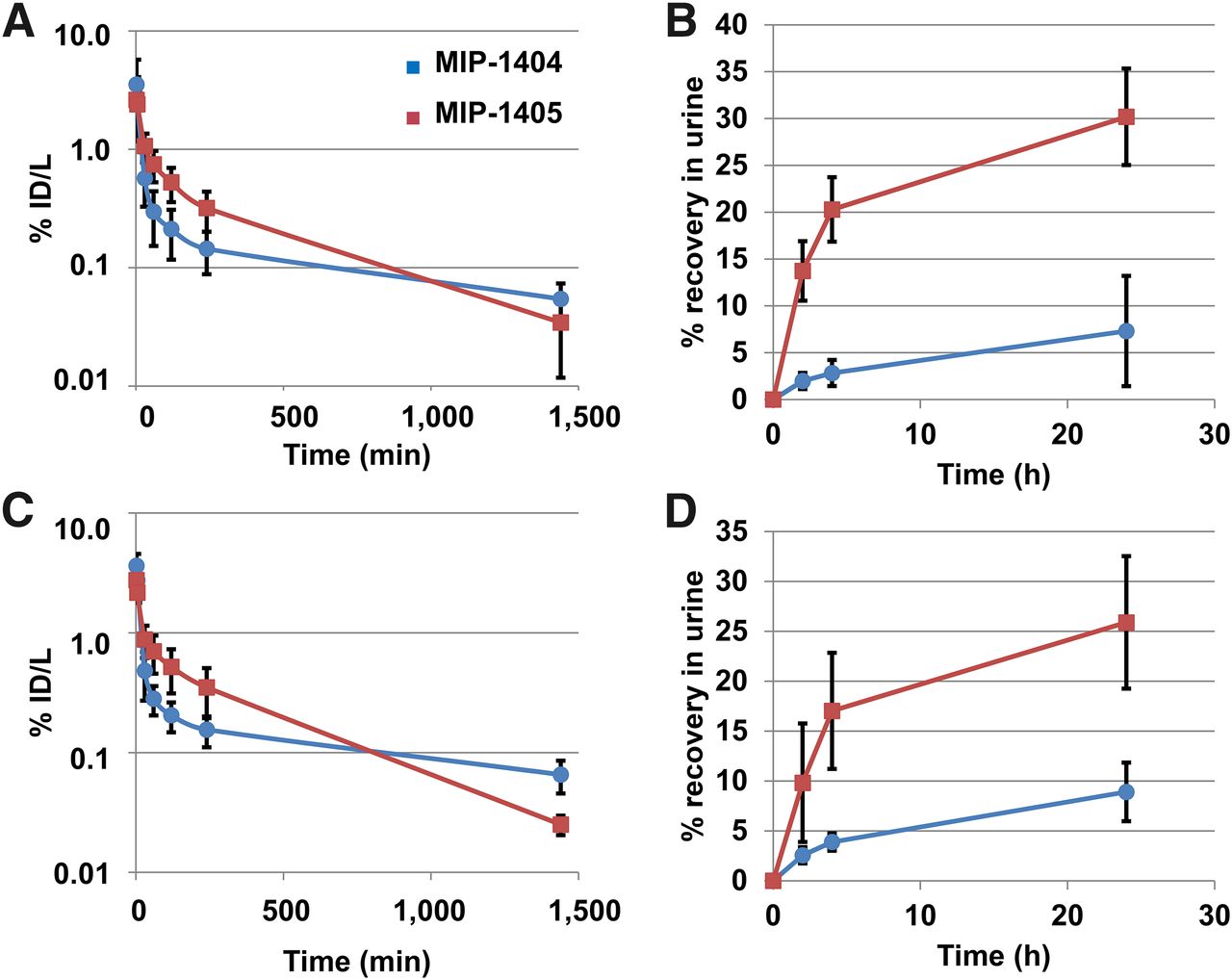
After intravenous administration, the blood levels of 99mTc-MIP-1404 and 99mTc-MIP-1405 reached maximum concentration in plasma at the first time point (5 min) collected and declined rapidly in a biphasic fashion (Figs. 2A and 2B; Table 2). Both 99mTc-MIP-1404 and 99mTc-MIP-1405 were rapidly cleared from the vascular compartment and moved into the extravascular space, resulting in similar total blood exposure of 99mTc-MIP-1404 and 99mTc-MIP-1405 in both healthy subjects and PCa patients. No apparent differences in any pharmacokinetic parameters were noted when comparing healthy subjects with PCa patients. Preliminary analysis, however, indicates a significant difference (P < 0.05) in steady-state volume of distribution, half-life, MRT, and T1/2β when comparing these 2 agents between healthy subjects and PCa patients. By 24 h, approximately 5%–10% of the injected dose of 99mTc-MIP-1404 and 25%–30% of the injected dose of 99mTc-MIP-1405 was present in the urine (Figs. 2B and 2D).
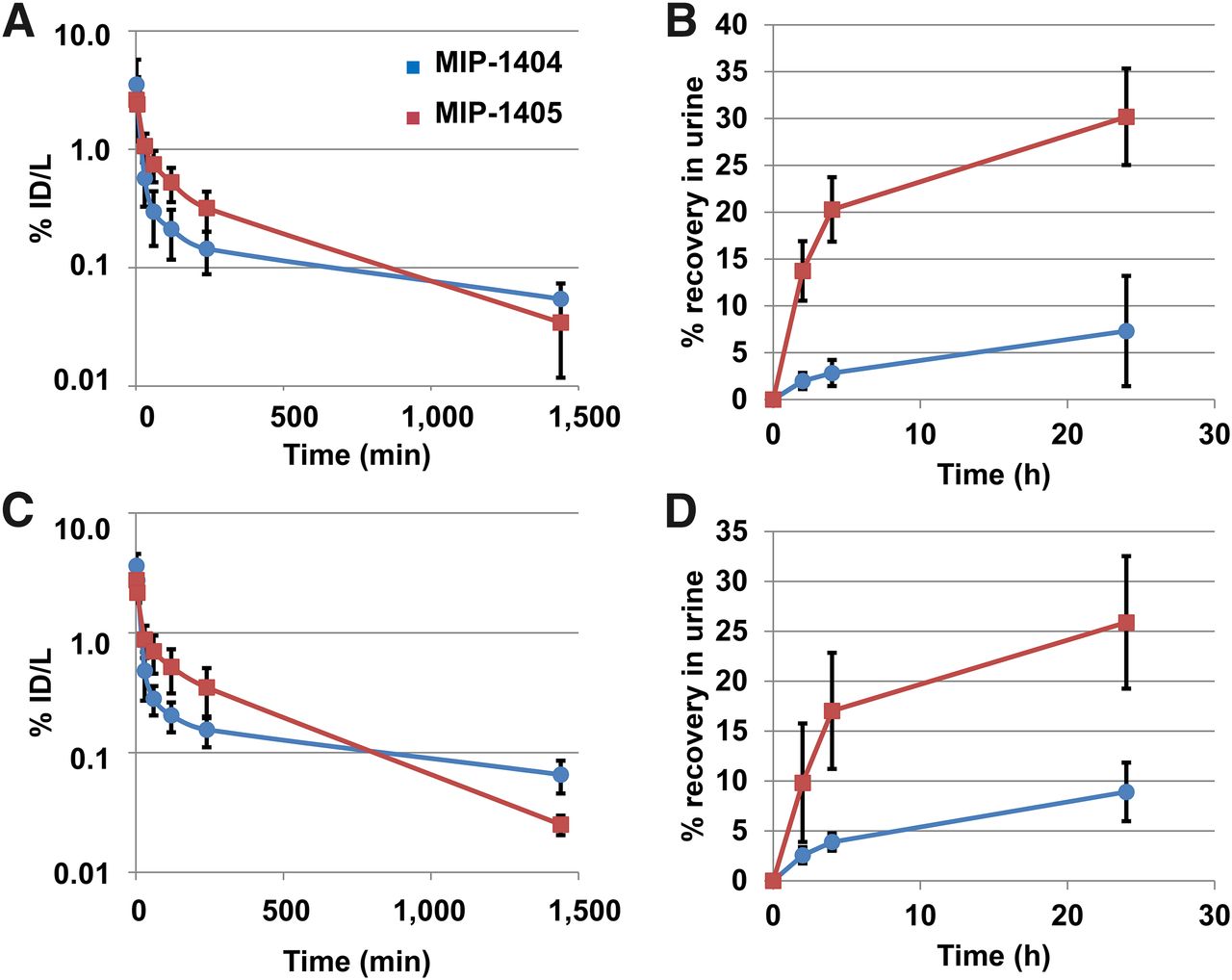
Blood clearance and urinary excretion of 99mTc-MIP-1404 and 99mTc-MIP-1405 in healthy subjects (A and B) and in patients with PCa (C and D).
Blood Pharmacokinetic Analysis of 99mTc-MIP-1404 and 99mTc-MIP-1405 in Healthy Subjects and Patients with PCa
Imaging Studies and Tissue Distribution
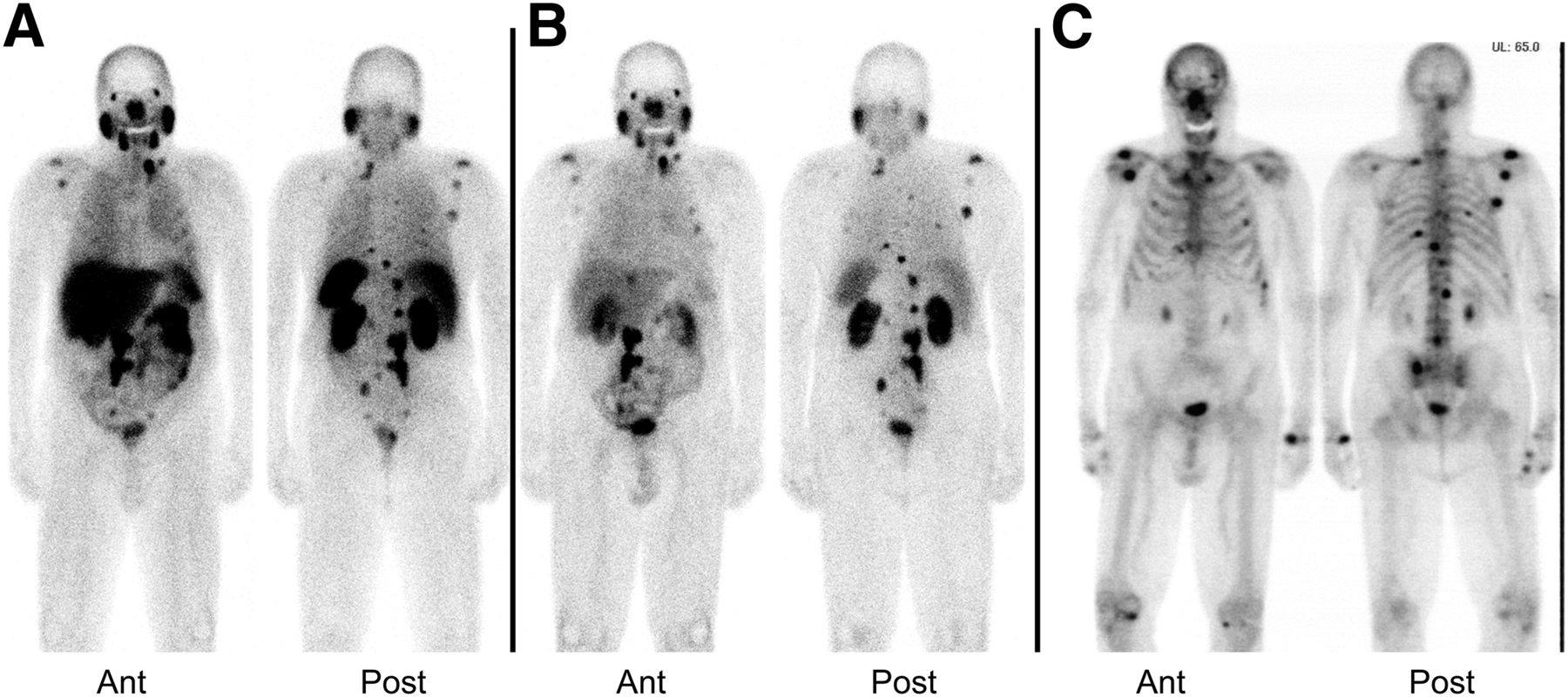
Typical whole-body planar images for a patient administered 99mTc-MIP-1404 and 99mTc-MIP-1405 through 24 h after injection are depicted in Figure 3. In healthy subjects and in patients with metastatic PCa, uptake of both agents was evident in the parotid and salivary glands, liver, kidneys, and gastrointestinal tract. As shown in Figure 3, the whole-body clearance of 99mTc-MIP-1405 was significantly greater and the liver and kidney uptake was much lower than those of 99mTc-MIP-1404. Significantly lower uptake was seen in the bladder with 99mTc-MIP-1404 than with 99mTc-MIP-1405, as illustrated in planar images in Figure 3 and SPECT/CT images in Figure 4.
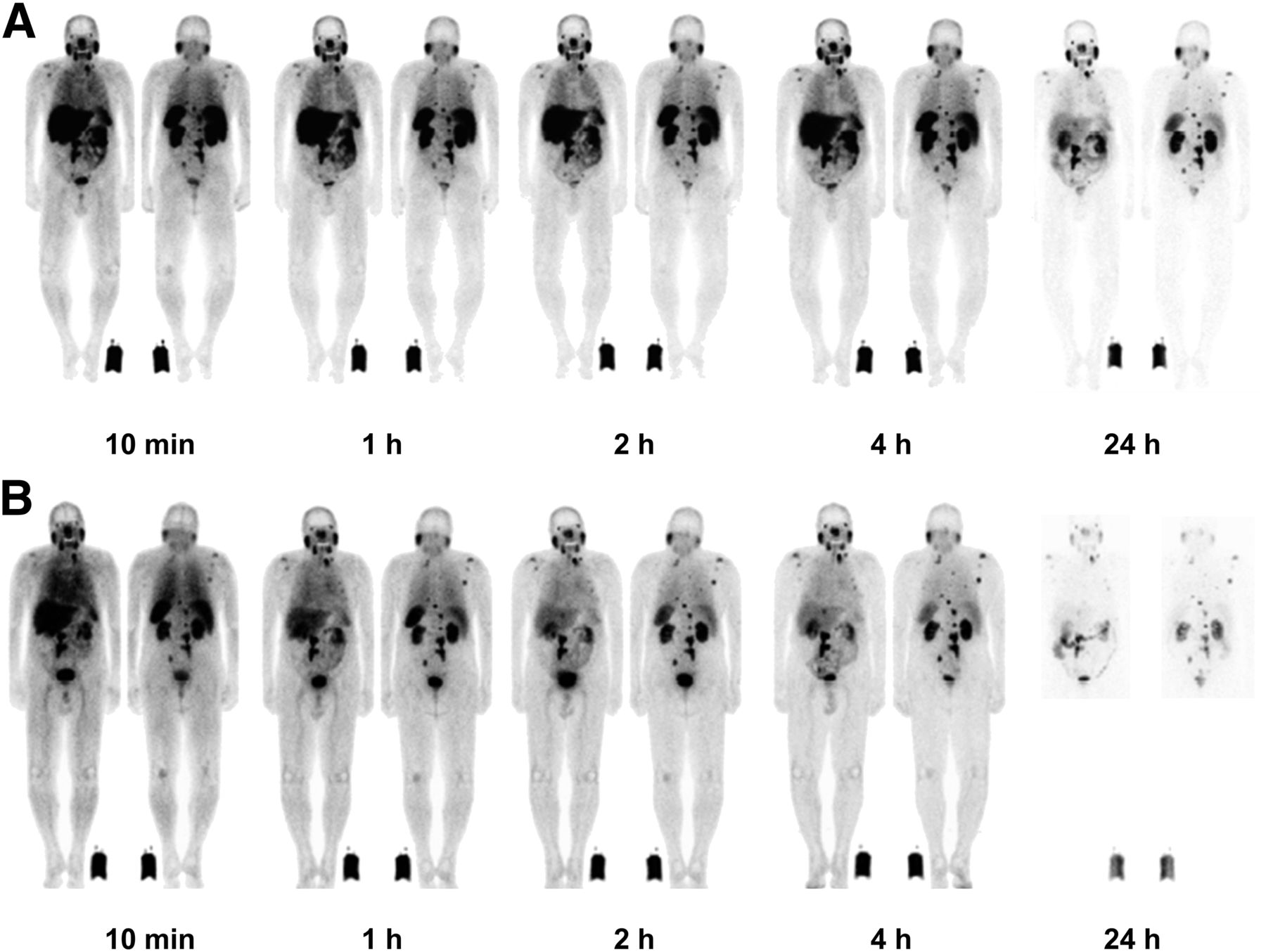
Whole-body planar images of 99mTc-MIP-1404 (A) and 99mTc-MIP-1405 (B) at different times after intravenous injection showing biodistribution in patient with metastatic PCa.
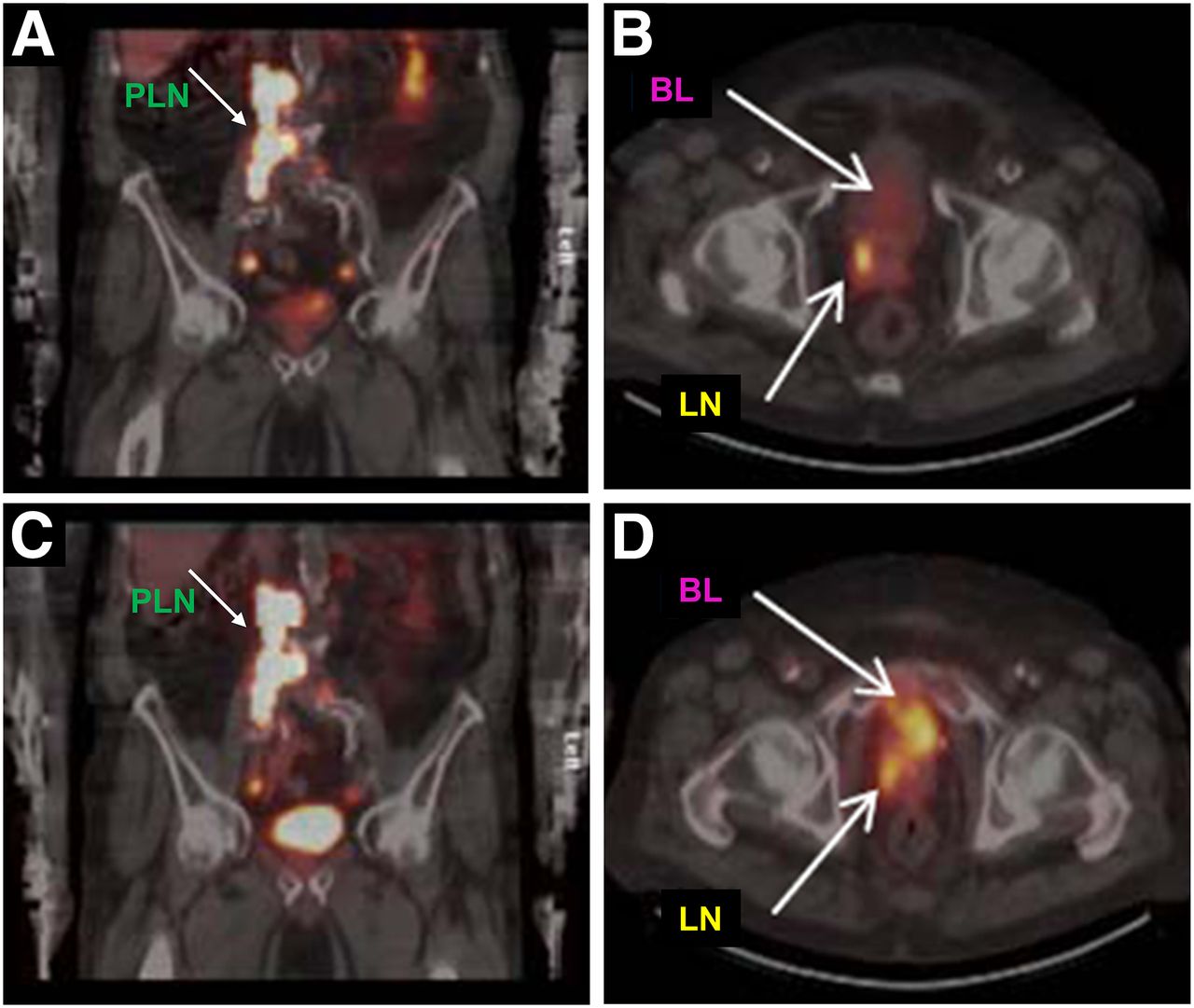
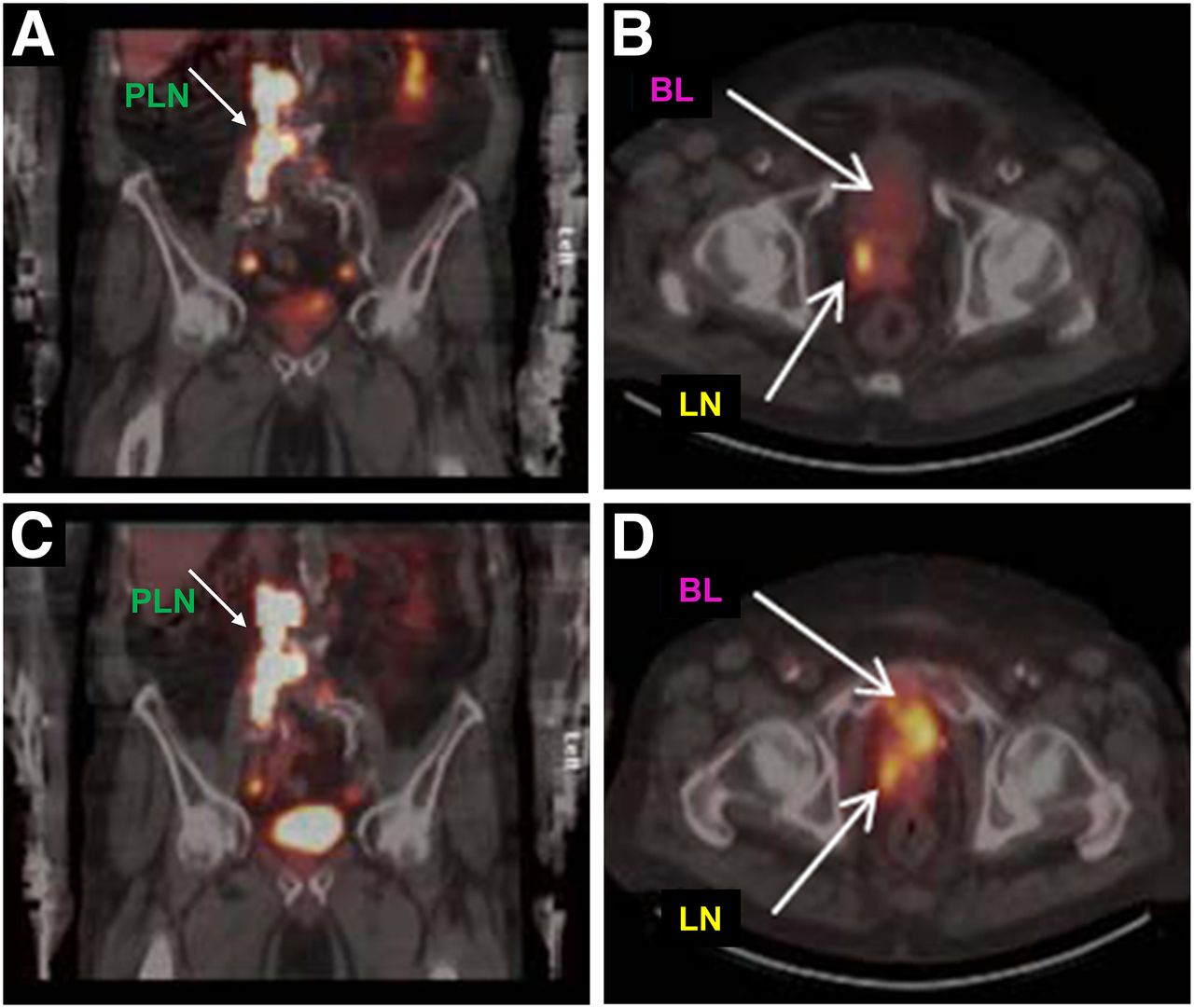
Differences in urinary excretion between 99mTc-MIP-1404 and 99mTc-MIP-1405. The planar and SPECT images of 99mTc-MIP-1404 (A and B) show minimal urinary excretion and bladder (BL) activity, compared with that of 99mTc-MIP-1405 (C and D). Images also identify metastasis in lymph node (LN) in pelvis and paraaortic lymph nodes (PLN).
ROIs were created over the imaging standard, tissues, and normal organs on the anterior and posterior planar whole-body images of each subject to extract count data corresponding to the in vivo distribution of these 2 agents. 99mTc-MIP-1405 was cleared from the whole body more rapidly than 99mTc-MIP-1404 (Supplemental Fig. 1; supplemental materials are available at http://jnm.snmjournals.org). With 99mTc-MIP-1405, 63 %ID remained in the body at 4 h and 27 %ID at 20 h. In contrast, 99mTc-MIP-1404 was cleared from the body more slowly, resulting in increased soft-tissue uptake. At 4 h, 93 %ID remained in the body, and at 20 h 84 %ID remained. In all organs examined (kidneys, liver, brain, salivary glands, heart, lungs, and spleen), greater retention was observed with 99mTc-MIP-1404 than with 99mTc-MIP-1405. Minimal uptake was detected in the brain and heart. Because the whole-body clearance and biodistribution of these 2 agents are similar in both healthy subjects and patients with PCa, the values (Supplemental Fig. 1) represent the mean ± SD of all 12 subjects in the study.
Detection of PCa Metastatic Lesions
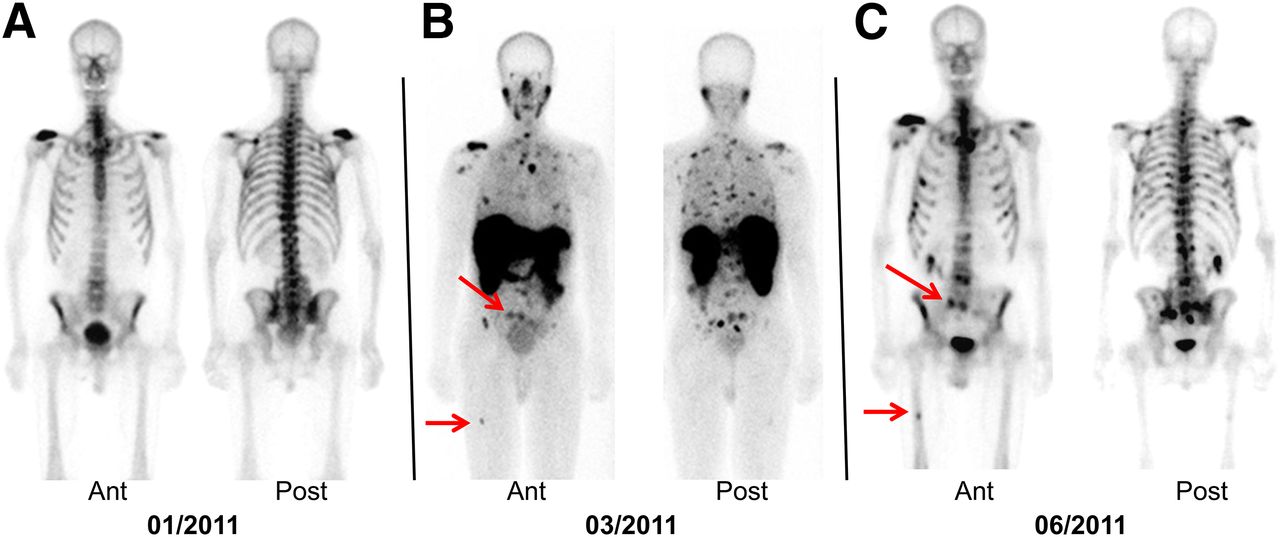
In patients with PCa, suspected metastatic lesions present in the bone, lymph nodes, and prostate bed were observed with both 99mTc-MIP-1404 and 99mTc-MIP-1405 within 10 min after injection. The planar images, however, showed better contrast at 2 and 4 h after injection. The uptake in metastatic lesions and the salivary glands was seen even at 24 h after injection. The planar images in a patient with metastatic PCa (patient 6, Table 1) demonstrate that both 99mTc agents identified the abnormal metastatic foci detected by the standard-of-care bone scan (Fig. 5). In 5 of 6 patients, 99mTc PSMA planar scans clearly identified all the metastatic lesions previously detected by bone scanning. In one of the patients (patient 2, Table 1), both 99mTc agents identified more abnormal foci than the bone scanning performed 2 mo earlier. A repeated bone scan obtained 3 mo after the 99mTc-MIP-1404 PSMA scan identified additional metastatic sites not seen in the first bone scan (Fig. 6).
Tumor uptake of 99mTc-MIP-1404 (A) or 99mTc-MIP-1405 (B) at 4 h in patient with metastatic PCa, compared with that of standard bone scan (C). Images also show uptake of radiotracer in normal parotid and salivary glands. Ant = anterior; Post = posterior.

Comparison of 99mTc-MIP-1404 scan with bone scans in patient with metastatic PCa. PSMA imaging with 99mTc-MIP-1404 (in March) detected more metastatic lesions than 2 bone scans obtained either before (in January) or after (in June) PSMA scan. Ant = anterior; Post = posterior. Metastatic sites (red arrows) shown in PSMA scan (B) were detected by bone scan (C) performed 3 mo after PSMA scan.
As the blood and soft-tissue background cleared, T/B ratios derived from whole-body planar images increased from an average value of 3:1 at 1 h to 9:1 at approximately 20 h after injection for both these agents (Fig. 7). Although higher total uptake of 99mTc-MIP-1404 was detected in suspected lesions, there were no statistically significant differences in T/B ratios for either of these agents at 2 and 4 h, ideal time points for imaging studies.

T/B ratios of 99mTc-MIP-1404 and 99mTc-MIP-1405 in patients with metastatic PCa.
Radiation Dosimetry
The radiation-absorbed dose for organs was estimated in units of mGy/MBq. The complete radiation dose estimates for various organs for both 99mTc-MIP-1404 and 99mTc-MIP-1405 are shown in Table 3. The mean effective dose is 0.0088 mSv/MBq with 99mTc-MIP-1404 and 0.0079 mSv/MBq with 99mTc-MIP-1405. For a 740-MBq (20 mCi) administered dose, the mean effective dose is about 6.5 mSv for 99mTc-MIP-1404 and 5.82 mSv for 99mTc-MIP-1405. The critical organ for 99mTc-MIP-1404 is the kidney (54.24 mGy/740 MBq [5.42 rads/20 mCi]) and for 99mTc-MIP-1405 the urinary bladder wall (32.1 mGy/740 MBq [3.21 rads/20 mCi]). With both agents, the salivary gland is 1 of the organs receiving the largest radiation-absorbed dose along with the kidneys and the urinary bladder wall.
Radiation Dosimetry
Safety
Both 99mTc-MIP-1404 and 99mTc-MIP-1405 were well tolerated in this study. There were no treatment-emergent adverse events and serious adverse events reported in this study. Clinical laboratory, vital signs, and electrocardiogram results were unremarkable, with no clinically significant differences between the 2 study drugs.
DISCUSSION
PSMA was one of the first PCa biomarkers successfully cloned and has been the subject of intense clinical inquiry as an imaging and therapeutic agent since 1993 (9). We recently reported the potential clinical utility of 123I-labeled small-molecule PSMA inhibitors for imaging PCa (27). Because the 99mTc atom has the ideal nuclear properties of γ energy (140-keV photon) and half-life (6 h), as well as its convenient availability from commercial generators, it has become the most ideal radionuclide to develop radiopharmaceuticals for SPECT. The polyvalent nature of technetium, however, demands that due consideration is given to the chemical approach used for its incorporation into a targeting ligand. How the metal is bound can greatly influence the overall pharmacologic character and biologic fate of the complex, by altering the overall charge, polarity, hydrophobicity, and steric bulk. The chelate, the metal–chelate complex, and the nature of the outer solvation sphere of the metal chelate complex all directly or indirectly influence the performance of such a radiolabeled ligand in regards to its intended clinical use (25). Maresca et al. have previously reported the development of a single-amino-acid–based radiolabeling platform, constructed from derivatized amino acids modified to provide 3 donor groups (L3) for chelation to the {M(CO)3}+1 core (Fig. 1). On the basis of this chemistry, 99mTc labeling of MIP-1404 and MIP-1405 (>90%) was achieved with only 100 μg of ligand (∼10−5 M), and the 99mTc complexes were stable (>90%) for 24 h (25).
Although both 99mTc agents are based on the glutamate-urea amino acid core and display similar PSMA binding affinities (26), significantly different pharmacokinetic parameters were observed in the human studies reported here, most likely because of modest structural differences affecting hydrophobicity and protein binding. After intravenous administration, blood levels of 99mTc-MIP-1404 and 99mTc-MIP-1405 declined rapidly in a biphasic fashion (Figs. 2A and 2C; Table 2) from the vascular compartment and moved into the extravascular space, resulting in similar total blood exposure in both healthy controls and patients with PCa. However, on the basis of serial imaging studies (Fig. 3), 99mTc-MIP-1405 was cleared from the whole body, via the kidneys, more rapidly than 99mTc-MIP-1404. At 4 h after injection, 37% of 99mTc-MIP-1405 activity cleared from the whole body, compared with only 7% of 99mTc-MIP-1404 activity. Also the cumulative urinary activity was significantly higher at 4 and 24 h for 99mTc-MIP-1405 than for 99mTc-MIP-1404 (Figs. 2B and 2D). These results of the in vivo distribution and urinary excretion suggest that 99mTc-MIP-1404 may be more suitable for imaging lesions in the pelvis, whereas 99mTc-MIP-1405 may provide better contrast for imaging metastatic sites outside the pelvis.
In all 6 patients with metastatic PCa, both 99mTc-MIP-1404 and 99mTc-MIP-1405 localized to lesions in bone and soft tissue that correlated with radiologic evidence of metastatic disease identified by the bone scan (Figs. 5 and 6). Between 1 and 4 h after injection, the T/B ratios (Fig. 7) were similar for both agents even though the image contrast outside the pelvis appears to be slightly better with 99mTc-MIP-1405 (Figs. 3 and 5). In a 71-y-old patient who had prior prostatectomy and with a rising PSA (1.37–8.9 ng/mL over a period of 4 mo), PSMA imaging with 99mTc-MIP-1404 (in March) detected more metastatic lesions earlier than with the 2 bone scans obtained either before (in January) or after (in June) the PSMA scanning (Fig. 6). This observation suggests that PSMA-targeted molecular imaging may have the potential to identify disease progression earlier than the standard bone scanning. In addition, in several patients, significant uptake was also observed in lymph nodes smaller than 10 mm, considered normal by size threshold criteria used in cross-sectional imaging such as CT and MR. Although histologic confirmation of the disease in the lymph nodes is needed, these observations suggest an improvement in the sensitivity of lesion detection with molecular imaging using small-molecule 99mTc-labeled PSMA inhibitors. The phase I data with 99mTc agents described here are consistent with preclinical studies in PSMA-expressing LNCaP xenografts. In addition, the biodistribution, blood clearance, and tumor uptake profiles of 99mTc-MIP-1404 and 99mTc-MIP-1404 are also similar to those of 2 other high-affinity PSMA inhibitors, MIP-1092 and MIP-1095 labeled with 123I, previously studied in healthy subjects and subjects with advanced metastatic cancer (27).
Recently, several PET radiopharmaceuticals based on small-molecule PSMA inhibitors labeled with 18F or 68Ga have been reported (18,19,35). Initial phase I studies with 18F-N-[N-[(S)-1,3-dicarboxypropyl]carbamoyl]-4-18F-fluorobenzyl-l-cysteine (18F-DCFBC) demonstrated the potential of targeting PSMA for the detection of metastatic PCa. However, there was decreasing but moderately persistent blood-pool and liver activity. The slow rise in decay-corrected hepatic uptake suggests the possibility of some hepatic excretion of 18F-DCFBC with a long biologic elimination period (18). In addition, unlike 99mTc agents reported here, PET scans with 18F-DCFBC did not show any uptake by the parotid and salivary glands. Initial clinical studies with the 68Ga-N,N′-bis[2-hydroxy-5-(carboxyethyl)benzyl]ehtylenediamine-N,N′-diacetic acid radiotracer, however, showed in vivo distribution similar to the 99mTc agents reported here. The PET scans showed significant 68Ga uptake in the salivary glands and kidneys only and to a lesser extent in lacrimal glands, liver, spleen, and bowel as well as normal prostate tissue (19). In a study comparing 68Ga-PSMA PET with 18F-fluorocholine PET, it was reported that 68Ga-PSMA can detect PCa relapses and metastases with significantly improved contrast when compared with fluorocholine (19).
The results of the present study demonstrate that targeting PSMA with both 99mTc-MIP-1404 and 99mTc-MIP-1405 facilitates the detection of radiologically proven PCa in bone, lymph nodes, and the prostate gland. Also the radiation dosimetry from a single administration of a diagnostic dose for either of these agents is only around 6 mSv, which is similar to the radiation dose from the conventional bone scan in nuclear medicine. Although both of these agents showed minimal or no uptake in the prostate of healthy male subjects, only 99mTc-MIP-1404 showed minimal urinary excretion. This finding suggested that 99mTc-MIP-1404 may have distinct advantage for detecting PCa in the gland and in the pelvis at early stages of the disease. On the basis of these results, a preliminary phase I study and a multicenter phase II study were conducted in high-risk PCa patients scheduled for prostatectomy and extended pelvic node lymph node dissection (36,37).
CONCLUSION
Microdosing studies under an exploratory IND allowed for the assessment of preliminary pharmacokinetics and pharmacodynamics for two 99mTc-labeled small molecules, MIP-1404 and MIP-1405, that bind to PSMA with high affinity. After intravenous administration, blood levels of 99mTc-MIP-1404 and 99mTc-MIP-1405 declined rapidly, and high-contrast planar and SPECT scans were obtained within 1–2 h after injection. In patients with metastatic PCa, both 99mTc-MIP-1404 and 99mTc-MIP-1405 localized to lesions in bone and soft tissue that correlated with radiologic evidence of metastatic disease identified by the bone scan. Because 99mTc-MIP-1404 showed minimal urinary excretion, it had a distinct advantage for detecting PCa in the gland and pelvis at early stages of the disease and was selected for phase II studies to determine sensitivity and specificity to detect PCa in high-risk patients.
DISCLOSURE
The costs of publication of this article were defrayed in part by the payment of page charges. Therefore, and solely to indicate this fact, this article is hereby marked “advertisement” in accordance with 18 USC section 1734. The single center phase I study described in this article was funded by the Molecular Insight Pharmaceuticals (MIP). No other potential conflict of interest relevant to this article was reported.
Footnotes
Published online Oct. 23, 2014.
- © 2014 by the Society of Nuclear Medicine and Molecular Imaging, Inc.
REFERENCES
- Received for publication March 19, 2014.
- Accepted for publication September 30, 2014.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- A New Labelling Method of 99mTc-PSMA-HBED-CC
- Eligibility for 177Lu-PSMA Therapy Depends on the Choice of Companion Diagnostic Tracer: A Comparison of 68Ga-PSMA-11 and 99mTc-MIP-1404 in Metastatic Castration-Resistant Prostate Cancer
- Robot-Assisted Prostate-Specific Membrane Antigen-Radioguided Surgery in Primary Diagnosed Prostate Cancer
- Radiation Dosimetry of 99mTc-PSMA I&S: A Single-Center Prospective Study
- Intraindividual Comparison of 99mTc-Methylene Diphosphonate and Prostate-Specific Membrane Antigen Ligand 99mTc-MIP-1427 in Patients with Osseous Metastasized Prostate Cancer
- Intraindividual Comparison of 18F-PSMA-1007 and 18F-DCFPyL PET/CT in the Prospective Evaluation of Patients with Newly Diagnosed Prostate Carcinoma: A Pilot Study
- Phase 2 Study of 99mTc-Trofolastat SPECT/CT to Identify and Localize Prostate Cancer in Intermediate- and High-Risk Patients Undergoing Radical Prostatectomy and Extended Pelvic LN Dissection
- Prostate-Specific Membrane Antigen Ligands for Imaging and Therapy
- Glu-Ureido-Based Inhibitors of Prostate-Specific Membrane Antigen: Lessons Learned During the Development of a Novel Class of Low-Molecular-Weight Theranostic Radiotracers
- Preclinical Evaluation of 18F-PSMA-1007, a New Prostate-Specific Membrane Antigen Ligand for Prostate Cancer Imaging
- Preclinical Evaluation and First Patient Application of 99mTc-PSMA-I&S for SPECT Imaging and Radioguided Surgery in Prostate Cancer
- Synthesis and Biologic Evaluation of Novel 18F-Labeled Probes Targeting Prostate-Specific Membrane Antigen for PET of Prostate Cancer
- The Rise of PSMA Ligands for Diagnosis and Therapy of Prostate Cancer
- Comparison of Prostate-Specific Membrane Antigen-Based 18F-DCFBC PET/CT to Conventional Imaging Modalities for Detection of Hormone-Naive and Castration-Resistant Metastatic Prostate Cancer
- 68Ga- and 177Lu-Labeled PSMA I&T: Optimization of a PSMA-Targeted Theranostic Concept and First Proof-of-Concept Human Studies