


Abstract
PET using 18F-FDG has prognostic value when performed at the completion of initial chemotherapy in patients with diffuse large B-cell lymphoma (DLBCL). 18F-FDG PET may also be predictive of outcome when performed during the treatment course of DLBCL, but robust prospective studies and standardization of 18F-FDG PET interpretation in this setting are lacking. Methods: In this prospective study, patients with advanced-stage DLBCL were treated with standard rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisone chemotherapy, and 18F-FDG PET/CT was performed after cycle 2 or 3 and at the end of therapy. The 18F-FDG PET/CT scans were interpreted according to the International Harmonization Project for Response Criteria in Lymphoma, and the maximum standardized uptake value (SUV) of the most 18F-FDG–avid lesions was recorded. Results: Fifty patients were enrolled, and all underwent interim 18F-FDG PET/CT. At a median follow-up of 33.9 mo, the positive predictive value (PPV) of interim 18F-FDG PET/CT for relapse or progression was 42%, and the negative predictive value (NPV) was 77%. Interim 18F-FDG PET/CT was significantly associated with event-free survival (P = 0.017) and with progression-free survival (P = 0.04) but not with overall survival (P = 0.08). End-of-therapy 18F-FDG PET/CT had high PPV and NPV (71% and 80%, respectively) and was significantly associated with event-free survival, progression-free survival, and overall survival (P < 0.001). SUV measurements did not discriminate patients who relapsed or progressed from those who remained in remission. Conclusion: When performed after 2 cycles of immunochemotherapy and interpreted according to International Harmonization Project criteria, early response assessment with PET/CT has a high NPV but low PPV in patients with advanced-stage DLBCL. Prospective trials are required to validate different criteria for the interpretation of interim 18F-FDG PET/CT and establish the role of interim 18F-FDG PET/CT in the management of patients with DLBCL.
PET with 18F-FDG is a reliable and widely used imaging modality for the staging and response assessment of aggressive non-Hodgkin lymphomas (NHLs), including diffuse large B-cell lymphoma (DLBCL). For response assessment, 18F-FDG PET adds valuable information to that obtained with CT, because, unlike CT, 18F-FDG PET often can differentiate viable tumor from posttreatment fibrosis or necrosis. Two meta-analyses have supported the important prognostic value of 18F-FDG PET performed at the completion of therapy for aggressive NHL (1,2). The most recent lymphoma response criteria incorporate 18F-FDG PET into the definition of response (3), using standards established by the International Harmonization Project for Response Criteria in Lymphoma (IHP) to interpret end-of-therapy 18F-FDG PET scans as positive or negative (4).
The value of 18F-FDG PET performed during the course of induction chemotherapy for DLBCL is less well established. Interim 18F-FDG PET may reflect the lymphoma's chemosensitivity and predict whether the malignant cells will be completely eradicated by the end-of-chemotherapy course. This principle is supported by multiple studies that have reported high positive and negative predictive values (PPVs and NPVs, respectively) of 18F-FDG PET performed after 2–4 cycles of therapy for lymphoma (5–9). Unfortunately, these studies are hampered by heterogeneity with respect to lymphoma subtypes, chemotherapy regimens, timing of interim PET, and the criteria used to interpret the scans.
Here we report the results of a prospective study of patients with newly diagnosed, advanced-stage DLBCL treated with standard rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisone (R-CHOP) chemotherapy, all of whom underwent 18F-FDG PET/CT after 2–3 cycles of chemotherapy. In an effort to standardize the interpretation of interim 18F-FDG PET scans, we evaluated the predictive value of interim 18F-FDG PET/CT based on the IHP criteria established for end-of-treatment PET.
MATERIALS AND METHODS
This prospective single-arm study enrolled adult patients with histologically proven, advanced-stage, untreated DLBCL. Initially, the primary objective of the study was to correlate gene polymorphisms that responded to R-CHOP with response defined by 18F-FDG PET/CT after 2 cycles of therapy. When the IHP criteria were established in 2007, we reviewed the 18F-FDG PET/CT scans in our data set, with the aim of correlating the interim 18F-FDG PET/CT results, interpreted according to IHP criteria, with clinical outcomes.
Inclusion criteria were diagnosis of de novo, untreated DLCBL; Ann Arbor stage III–IV; and age 18 y or older. Patients were excluded if they had central nervous system involvement, had HIV infection, or were to receive radiation therapy as part of the initial treatment plan. The study was approved by the institutional review board, and all patients gave written informed consent.
Patients were treated with standard-dose R-CHOP at 3-wk intervals for 6 cycles (10). The protocol called for 18F-FDG PET/CT to be performed at 3 wk after cycle 2 and at the end of treatment. Therapy was not changed on the basis of interim 18F-FDG PET/CT results.
18F-FDG PET/CT and Analysis
The interim and end-of-therapy18F-FDG PET/CT scans were obtained at our institution with a Biograph Duo or a Biograph-40 (Siemens) scanner, following our standard clinical protocol, which is consistent with the recommendations of the IHP Imaging Subcommittee (4). The fasting glucose was required to be less than 200 mg/dL (mean, 111 mg/dL; range, 84–188 mg/dL) immediately before injection of 370–555 MBq (10–15 mCi) of 18F-FDG. After approximately 1 h, a spiral CT scan (typically 95–111 effective mAs, 130 kvP, and 5-mm slice thickness), with oral—but not intravenous—contrast agent administration, was acquired, followed by pelvis–to–skull base emission images. The PET emission images were corrected for measured attenuation and reconstructed using an ordered-subset expectation maximization iterative algorithm per the manufacturer's instructions.
All PET/CT images were interpreted in standard clinical fashion. After all patients had been treated, the 18F-FDG PET/CT scans were retrospectively reviewed by 2 nuclear radiologists and designated positive or negative according to the following consensus response criteria of the IHP (4):
Focal or diffuse 18F-FDG uptake above background
In a mass 2 cm or larger, mild and diffusely increased 18F-FDG uptake that is greater than that in mediastinal blood-pool structures
Any increased uptake in a mass smaller than 2 cm
New lung nodules 1.5 cm or larger, with uptake less than that in the mediastinal blood pool
Hepatic or splenic lesions 1.5 cm or larger, if uptake is more than uptake in liver or spleen; or diffusely increased splenic uptake
Clearly increased focal or multifocal bone involvement
The radiologists were unaware of the clinical outcomes. To explore whether quantification of 18F-FDG uptake in residual masses would allow discrimination of patients who do and do not relapse, the maximum standardized uptake value (SUVmax) was measured at residual sites of disease on interim scans that were positive by IHP criteria. Whenever available, baseline 18F-FDG PET/CT scans were used to identify initial sites of disease. In patients with multiple lesions, the standardized uptake values (SUVs) of the most 18F-FDG–avid lesions (≤7) were determined, and the average value correlated with response. The SUVmax of the lesions was compared with the average SUVs of the aortic blood pool, as determined by drawing a 1-cm oval region of interest in the aortic arch, and the average SUV of the liver, as determined by drawing a spheric 3 × 3 cm region of interest in the mid liver.
Statistical Analysis
The objective of this analysis was to estimate the predictive value of interim 18F-FDG PET/CT in patients with advanced-stage DLBCL treated with R-CHOP, using the IHP consensus response criteria for interpretation of 18F-FDG PET/CT scans. Our sample size of 50 patients provides 95% power to detect a 2-y progression-free survival (PFS) of 30% for positive interim PET versus 85% for negative interim PET (11). Sensitivity, specificity, PPV, NPV, and positive and negative likelihood ratios, with 95% confidence interval, for predicting disease progression were calculated for interim and end-of-therapy 18F-FDG PET/CT scans. Overall survival (OS), PFS, and event-free survival (EFS) were separately defined to be the time interval from enrollment in the study to date of death, to date of relapse, and to the earlier date of an event (death, relapse, or next therapy), respectively. Kaplan–Meier curves were generated for the time-to-event outcomes according to interim or final 18F-FDG PET/CT result (positive vs. negative). P values from log-rank tests were calculated, and survival probabilities at year 2 were estimated. SUVs were compared between 2 groups using the Wilcoxon rank sum test. All tests were 2-sided, and the significance level was set at 0.05. All analyses were performed in R 2.7.1 (http://cran.r-project.org).
RESULTS
Patient Characteristics
Fifty-two patients were enrolled between March 2005 and May 2008 (mean age, 58 y; range, 29–80 y). Two patients were excluded for histology other than DLBCL (Burkitt's and mantle cell lymphoma), and they are not included in the analysis. All patients had stage III or IV disease, and 68% had International Prognostic Index scores indicating high–intermediate risk or high risk (Table 1) (12).
Characteristics of Patients (n = 50)
Patient Outcomes
Forty-four patients (88%) completed 6 cycles of R-CHOP. Three patients stopped therapy after 4 (n = 2) or 5 (n = 1) cycles because of toxicity, and 3 patients had progressive disease after 2, 4, and 5 cycles of R-CHOP.
Interim 18F-FDG PET/CT was performed at 3 wk after cycle 2 in 47 patients (94%) but was delayed until the end of cycle 3 in the remaining 3 patients because of scheduling errors. Forty-two patients (84%) also underwent end-of-therapy 18F-FDG PET/CT after 6 (n = 41) or 5 (n = 1) cycles of R-CHOP. Eight patients did not undergo end-of-therapy 18F-FDG PET/CT because they stopped treatment early for toxicity (n = 2) or progressive disease (n = 3) or because only a CT scan was obtained after cycle 6 (n = 3). No patients were treated with radiation or underwent biopsy of a residual 18F-FDG–avid site. Baseline 18F-FDG PET was not a study requirement and was performed in only 29 patients (58%). The 2-y EFS and OS of the entire study population were 74% (95% confidence interval [CI], 63%–87%) and 75% (95% CI, 69%–90%), respectively (Fig. 1). Thirteen patients died from progressive disease (n = 8), infection (n = 3), heart failure (n = 1), or complications of allogeneic stem cell transplantation (n = 1). Median follow-up for all surviving patients was 33.9 mo (range, 16–44 mo).

OS (A) and PFS (B) for study population, with 95% CIs.
Predictive Value of 18F-FDG PET/CT Using IHP Criteria
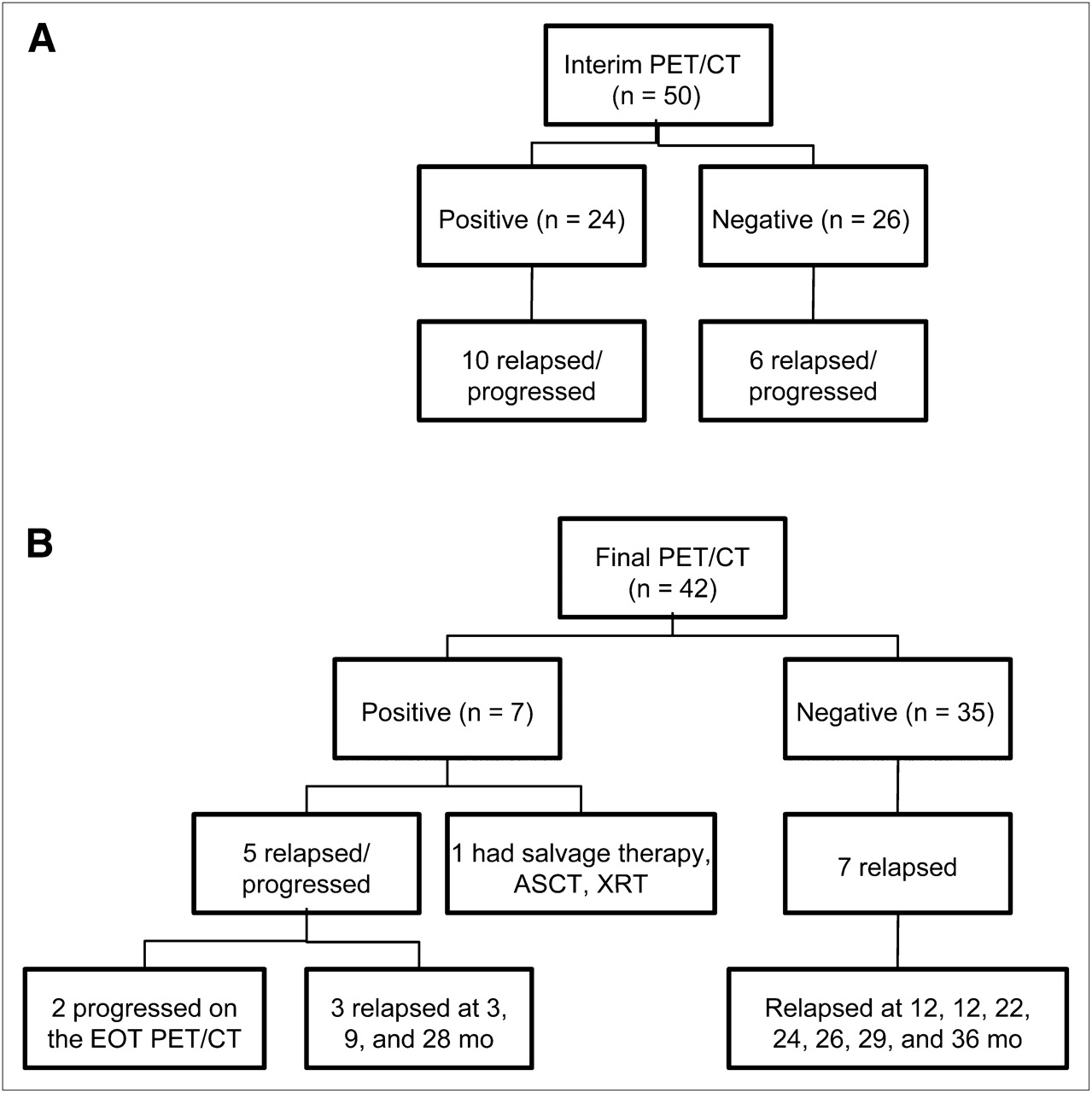
On the basis of the IHP criteria, 24 patients, 10 of whom relapsed or progressed, had a positive interim 18F-FDG PET/CT scan result (PPV, 42%; 95% CI, 22%–61%; Fig. 2A). Among these 10 patients, 1 patient had progressive disease in the central nervous system after cycle 4 of R-CHOP, and 2 patients had obvious disease progression on the end-of-therapy 18F-FDG PET/CT scan. Another 7 patients with positive interim 18F-FDG PET/CT scan results relapsed at 3, 9, 12, 24, 26, 28, and 29 mo after completion of R-CHOP. In 6 of these 7 patients, relapse occurred in the sites of residual 18F-FDG uptake. An additional patient had residual intense uptake in a mediastinal mass after both cycle 2 and cycle 6 of R-CHOP and went on to salvage chemotherapy, autologous stem cell transplantation (ASCT), and mediastinal radiation therapy, with no subsequent disease progression. Two of the 10 patients who relapsed after a positive interim 18F-FDG PET/CT scan result are in a second complete remission 10 and 24 mo after ASCT.

Patient outcomes according to interim (A) and end-of-therapy (B) 18F-FDG PET/CT results. EOT = end of therapy; XRT = radiation therapy.
Twenty-six patients, 6 of whom relapsed or progressed, had a negative interim 18F-FDG PET/CT scan result (NPV, 77%; 95% CI, 60%–94%). Two had progressive disease in the central nervous system after cycles 2 and 5 of R-CHOP, and 4 relapsed 12, 22, 36, and 39 mo after completion of R-CHOP. The sensitivity and specificity of interim 18F-FDG PET/CT for relapse were 0.63 and 0.59, respectively (positive likelihood ratio, 1.52, and 95% CI, 0.87–2.64; negative likelihood ratio, 0.64, and 95% CI, 0.32–1.27).
Among the 42 patients who underwent 18F-FDG PET/CT at the end of therapy, 7 (17%) had a positive scan result and 35 (83%) had a negative scan result by IHP criteria. The PPV and NPV of end-of-therapy 18F-FDG PET/CT were 71% (95% CI, 30%–95%) and 80% (95% CI, 63%–91%), respectively (positive likelihood ratio, 6.25, and 95% CI, 1.40–27.9; negative likelihood ratio, 0.63, and 95% CI, 0.39–1.01; details of patient outcomes are provided in Fig. 2B). Among the 21 patients who had a positive interim PET scan result and an end-of-therapy PET scan, 7 continued to have a positive PET scan result at the end of therapy and 14 had converted to a negative PET scan result. All patients with a negative interim PET scan result also had a negative end-of therapy PET scan result, if that scan was performed.
Survival According to 18F-FDG PET/CT Results
Although a trend was observed, there was not a statistically significant difference in OS between patients with a positive or negative interim 18F-FDG PET/CT scan result (P = 0.08, Fig. 3A). PFS and EFS probability were lower in patients with a positive interim 18F-FDG PET/CT scan result (P = 0.04 and 0.031, respectively, Fig. 3B), with a 2-y EFS probability of 63% (95% CI, 46%–85%) in patients with a positive interim scan result versus 85% (95% CI, 72%–100%) in patients with a negative interim 18F-FDG PET/CT scan result. OS, PFS, and EFS were significantly associated with the end-of-therapy 18F-FDG PET/CT results (P < 0.00001 for all 3 measures; Figs. 3C and 3D).

(A) OS according to interim 18F-FDG PET/CT results. (B) PFS according to interim 18F-FDG PET/CT results. (C) OS according to end-of-therapy 18F-FDG PET/CT results. (D) PFS according to end-of-therapy 18F-FDG PET/CT results
SUVs of Positive Interim 18F-FDG PET/CT Studies
Because of technical limitations, SUVs could not be measured on 1 of 24 positive interim 18F-FDG PET/CT studies, from a patient who relapsed. In the other patients who relapsed or progressed, the average SUVmax of the most 18F-FDG–avid disease site on the interim scan was 5.2 (range, 1.2–13.8), compared with 4.8 (range, 1.7–14.0) in the patients who remained in remission (P = 0.56). The average SUVs of the most 18F-FDG–avid sites (≤7) on the interim scans also were not statistically different in patients who relapsed or progressed and those who remained in remission (3.2 vs. 3.0, respectively, P = 0.45). SUVs of 18F-FDG–avid disease sites were also analyzed as a ratio of lesion SUV to blood pool or liver SUV. For reference, the mean SUVs of the blood pool and liver in the interim 18F-FDG PET/CT studies were 1.6 (range, 0.88–2.5) and 2.4 (range, 1.7–3.6), respectively. The mean ratio of SUVmax and SUV of the blood pool was 3.3 (range, 1.2–10.5) in patients who relapsed or progressed, compared with 3.0 (range, 1.1–9.0) in those who remained in remission (P ≥ 0.5). Similarly, there was no statistically significant difference between the 2 outcome groups when SUVmax was referenced to liver SUV or when the average SUVs of the most 18F-FDG–avid sites were referenced to the blood pool or liver SUV (all P ≥ 0.5).
DISCUSSION
In this prospective study of patients with advanced-stage DLBCL treated with standard R-CHOP immunochemotherapy, interim 18F-FDG PET/CT had a low positive-predictive value for relapse (42%) and did not have a statistically significant association with OS, although there was an association with PFS and EFS. These results are in contrast to previous studies, which have a reported PPV of 71%–100% for interim 18F-FDG PET in aggressive NHL (5–8,11,13), and a recent meta-analysis, which found a sensitivity of 0.78 and specificity of 0.87 for interim 18F-FDG PET in DLBCL (14). However, these studies have important limitations. For instance, the meta-analysis included 311 DLBCL patients from 6 studies who had stage I–IV disease and were treated with a variety of regimens, with and without rituximab, radiation, and even consolidative stem cell transplantation. Median follow-up ranged from 15 to 36 mo, and 18F-FDG PET was performed after 2, 3, or 4 cycles of therapy. In fact, the authors of the meta-analysis could not draw a conclusion about the value of interim 18F-FDG PET in DLBCL because of the heterogeneity of the available studies.
Although limited by small sample size, our study enrolled a homogeneous population of advanced-stage DLBCL patients who received standard immunochemotherapy and had consistent timing and interpretation of the interim 18F-FDG PET/CT scans. One weakness of our study is that the treating physician was aware of the interim 18F-FDG PET/CT results. However, in no patient was treatment changed on the basis of the interim 18F-FDG PET/CT results, and only 1 patient underwent additional therapy after R-CHOP based on persistent abnormal 18F-FDG uptake, but not frank progression, on the end-of-therapy scan. Another weakness is that baseline 18F-FDG PET was not performed on all patients. This deficiency does not affect our application of the IHP criteria to the interim 18F-FDG PET/CT scans, but it does limit our ability to explore the predictive value of the change in SUV and it may have impaired the radiologists’ ability to interpret the interim scans. Also, the 18F-FDG PET/CT scans were not obtained using a strict research protocol, but rather reflect the variations in technique, particularly scan timing, that occur in the course of routine clinical practice.
The important potential of interim 18F-FDG PET in aggressive lymphomas is to distinguish prognostic groups whose outcomes are sufficiently divergent to warrant a change in therapy. Our results demonstrate that the IHP criteria applied to interim scans in DLBCL do not accomplish this goal. Although patients with a positive interim 18F-FDG PET/CT scan did have inferior EFS, their EFS probability at 2 y was still 63%. On the other hand, we found that the NPV of interim 18F-FDG PET/CT interpreted by IHP criteria was high (77%), consistent with previous reports.
Application of other criteria may improve the prognostic value of interim 18F-FDG PET. For instance, Mikhaeel et al. have separated patients with minimal residual uptake from those with a more obviously positive interim 18F-FDG PET scan (8,15). Although we did not formally apply these criteria in our study, it is unlikely a minimal residual uptake category would improve the predictive value of our data set, given that the mean, median, and range of SUVs were essentially identical in patients who did and did not relapse after a positive interim scan. In response to criticism that minimal residual uptake is too subjective, a 5-point scoring system for 18F-FDG PET interpretation was developed at Guy's and St. Thomas’ Hospital, London, and is being applied in several European studies (16,17). This scoring system has the potential to provide reproducible grades of positive and negative 18F-FDG PET results, but it requires validation in NHL. A final method for interpretation of interim 18F-FDG PET scans is a semiquantitative approach based on relative reduction in SUV. Lin et al. found that an SUV-based assessment improved the PPV of interim 18F-FDG PET in DLBCL over that achieved with visual assessment (18). However, it may prove difficult to reproduce any SUV-based criteria reliably when scan conditions are not controlled in a research setting.
Several recent reports support our findings and underline the importance of the criteria used to interpret interim 18F-FDG PET scans in DLBCL. Han et al. used criteria similar to the IHP criteria in a retrospective study of DLBCL and mantle cell lymphoma patients treated with rituximab and chemotherapy (19). They reported a PPV and NPV for interim 18F-FDG PET of 33% and 68%, respectively, similar to our results. In a preliminary report, Pregno et al. used the consensus response criteria to interpret 18F-FDG PET scans obtained for DLBCL patients after 2–4 cycles of R-CHOP (20). With relatively early follow-up, interim 18F-FDG PET did not correlate with PFS (P = 0.198). On the other hand, Safar et al. used a more stringent definition of positive interim 18F-FDG PET in their prospective study of DLBCL patients treated with rituximab and chemotherapy (21). They scored scans with minimal residual uptake as negative. In their initial analysis, they report a 5-y PFS of 81% for patients with a negative 18F-FDG PET scan result after cycle 2 versus 47% for those with a positive scan result (P < 0.0001). In another preliminary report, Micallef et al. found no correlation between 2-y EFS and PET performed after 2 cycles of epratuzumab combined with R-CHOP in patients with DLBCL (22). Similar to our findings, 2-y EFS was 60% in the patients with a positive interim PET scan, although the criteria they used for PET interpretation are not defined.
Our data support the recommendation that interim 18F-FDG PET should be performed only in the context of clinical trials and should not yet be used to make treatment decisions in routine clinical practice. Ongoing clinical trials that alter therapy on the basis of the interim 18F-FDG PET may be difficult to interpret, as it is not clear that a positive 18F-FDG PET scan result defines a poor-risk group of patients in whom a change in therapy is warranted. For instance, Kasamon et al. used a risk-adapted approach to treat 59 patients with aggressive lymphoma, 56 of whom had DLBCL treated with R-CHOP (23). Patients who had a positive 18F-FDG PET scan result after cycle 2 (using criteria similar to IHP criteria) had their treatment changed to salvage chemotherapy, followed by ASCT. More than half of the DLBCL patients had a positive interim 18F-FDG PET scan result. The 2-y EFS for those who underwent ASCT was 74%, compared with 88% for those who had a negative interim 18F-FDG PET scan result and had completed R-CHOP. In a study by Moscowitz et al., 18F-FDG PET was performed in 97 patients with DLBCL after 4 cycles of dose-dense R-CHOP, and treatment was changed to ifosfamide–carboplatin–etoposide in patients who had a positive scan result (24). PFS was 79%, with no difference in outcome based on the interim 18F-FDG PET scan result. Of note, in 33 of 38 patients, biopsy of a positive site on the interim scan was negative for residual lymphoma. These outcomes with intensification of therapy for positive interim 18F-FDG PET are difficult to interpret in light of our results, as well as those of Han et al. (19) and Pregno et al. (20), who found that fewer than half of patients with a positive interim 18F-FDG PET scan result will relapse after a standard course of immunochemotherapy. If our results are supported by larger patient cohorts, intensification of therapy based on interim 18F-FDG PET would lead to overtreatment of a substantial portion of patients.
A recent report from Horning et al. (25) sounds an additional note of caution for the use of interim 18F-FDG PET in clinical decision making. A panel of 3 expert nuclear medicine physicians reviewed the 18F-FDG PET scans collected after 3 cycles of R-CHOP in the Eastern Cooperative Oncology Group E3404 study. Agreement among the 3 reviewers was only 68% and 71% when they interpreted the interim scans according to modified IHP criteria and the London criteria, respectively. Given that reporting of interim 18F-FDG PET can vary significantly even in a controlled research setting, further standardization of 18F-FDG PET interpretation is clearly needed. To that end, an international consensus group is validating interim PET assessment in DLBCL based either on a 5-point visual scale or on SUV analysis (26).
CONCLUSION
Mid-treatment 18F-FDG PET may prove useful as a predictive factor for patients with DLBCL undergoing induction chemotherapy, but the appropriate criteria for interpretation and subsequent modifications in therapy are yet to be established. Our results do not support use of the IHP criteria for interpretation of 18F-FDG PET/CT scans obtained after cycle 2 of immunochemotherapy. Future studies should consider use of different interpretive criteria or delay of interim 18F-FDG PET to later in the treatment course. On the other hand, our results do confirm the strong predictive value of 18F-FDG PET performed at the end of therapy. Outside a clinical trial, 18F-FDG PET/CT should be used only to guide end-of-therapy decisions, a setting in which it has established prognostic value.
Acknowledgments
This study was supported by a grant from the Barnes-Jewish Hospital Foundation.
- © 2011 by Society of Nuclear Medicine
REFERENCES
- Received for publication August 26, 2010.
- Accepted for publication December 8, 2010.





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Interim PET-driven strategy in de novo diffuse large B-cell lymphoma: do we trust the driver?
- Early treatment intensification with R-ICE and 90Y-ibritumomab tiuxetan (Zevalin)-BEAM stem cell transplantation in patients with high-risk diffuse large B-cell lymphoma patients and positive interim PET after 4 cycles of R-CHOP-14
- Response Assessment Criteria and Their Applications in Lymphoma: Part 2
- Prospective Study of 3'-Deoxy-3'-18F-Fluorothymidine PET for Early Interim Response Assessment in Advanced-Stage B-Cell Lymphoma
- Prospective International Cohort Study Demonstrates Inability of Interim PET to Predict Treatment Failure in Diffuse Large B-Cell Lymphoma
- Recommendations for Initial Evaluation, Staging, and Response Assessment of Hodgkin and Non-Hodgkin Lymphoma: The Lugano Classification
- Role of Imaging in the Staging and Response Assessment of Lymphoma: Consensus of the International Conference on Malignant Lymphomas Imaging Working Group
- Early Determination of Prognosis by Interim 3'-Deoxy-3'-18F-Fluorothymidine PET in Patients with Non-Hodgkin Lymphoma
- Early PET/CT Scan Is More Effective Than RECIST in Predicting Outcome of Patients with Liver Metastases from Colorectal Cancer Treated with Preoperative Chemotherapy Plus Bevacizumab
- Interim PET-CT in the management of diffuse large B-cell lymphoma
- Oncologic PET/MRI, Part 2: Bone Tumors, Soft-Tissue Tumors, Melanoma, and Lymphoma