


Abstract
Radioembolization with 90Y microspheres is a novel treatment for hepatic tumors. Generally, hepatic arteriography and 99mTc-macroaggregated albumin (MAA) scanning are performed before selective internal radiation therapy to detect extrahepatic shunting to the lung or the gastrointestinal tract. Whereas previous studies have used only planar or SPECT scans, the present study used 99mTc-MAA SPECT/CT scintigraphy (SPECT with integrated low-dose CT) to evaluate whether SPECT/CT and additional diagnostic contrast-enhanced CT before radioembolization with 90Y microspheres are superior to SPECT or planar imaging alone for detection of gastrointestinal shunting. Methods: In a prospective study, we enrolled 58 patients (mean age, 66 y; SD, 12 y; 10 women and 48 men) with hepatocellular carcinoma who underwent hepatic arteriography and scintigraphy with 99mTc-MAA using planar imaging, SPECT, and SPECT with integrated low-dose CT of the upper abdomen (acquired with a hybrid SPECT/CT camera). The ability of the different imaging modalities to detect extrahepatic MAA shunting was compared. Patient follow-up of a mean of 180 d served as the standard of reference. Results: Gastrointestinal shunting was revealed by planar imaging in 4, by SPECT in 9, and by SPECT/CT in 16 of the 68 examinations. For planar imaging, the sensitivity for detection of gastrointestinal shunting was 25%, the specificity 87%, and the accuracy 72%. For SPECT without CT, the sensitivity was 56%, the specificity 87%, and the accuracy 79%. SPECT with CT fusion had a sensitivity of 100%, a specificity of 94%, and an accuracy of 96%. In 3 patients, MAA deposits in the portal vein could accurately be attributed to tumor thrombus only with additional information from contrast-enhanced CT. The follow-up did not show any gastrointestinal complications. Conclusion: SPECT with integrated low-dose CT using 99mTc-MAA is beneficial in radioembolization with 90Y microspheres because it increases the sensitivity and specificity of 99mTc-MAA SPECT when detecting extrahepatic arterial shunting. The overall low risk of gastrointestinal complications in radioembolization may therefore be further reduced by SPECT/CT.
Radioembolization with 90Y microspheres via hepatic arterial administration is emerging as a promising treatment for patients with primary and metastatic liver cancer (1–4). 90Y microspheres are currently approved in the United States for the treatment of hepatocellular carcinoma (TheraSphere; MDS Nordion) and colorectal cancer (SIR-Spheres; Sirtex Medical). 90Y microspheres are injected into the arterial supply of the liver, where they preferentially flow into hypervascularized tumor areas, resulting in a significantly higher irradiation of tumor tissue than of normal liver parenchyma (5). With improvements in technology permitting smaller vessels to be catheterized and refinements in imaging techniques, the safety and efficacy of 90Y microsphere delivery has improved significantly (6–10).
Liver-directed therapy with 90Y provides several advantages over traditional treatment methods because of its low toxicity profile (6,8). Although postembolization syndrome may occur in as many as 50% of patients after radioembolization with 90Y microspheres, the severity is less than after transarterial chemoembolization (7–9,11). Rare but severe complications that may occur after administration of 90Y include nontarget irradiation leading to gastrointestinal ulceration, pancreatitis, cholecystitis, or radiation pneumonitis (8,12–15). Because of these potential risks, careful patient selection is of the utmost importance (7,16,17). Aggressive prophylactic embolization during hepatic arteriography is recommended because 90Y-induced ulcers may be refractory to medical therapy.
Generally, hepatic arteriography and 99mTc-macroaggregated albumin (MAA) scanning are performed before radioembolization with 90Y microspheres to detect extrahepatic shunting to the lung or the gastrointestinal tract (16). Whereas previous studies have used only planar imaging or SPECT of the upper abdomen to assess MAA distribution, the present study used 99mTc-MAA SPECT/CT scintigraphy (SPECT with integrated low-dose CT). SPECT/CT, a dual-modality imaging system that provides functional (SPECT) and anatomic (CT) images in the same scanning session, is now widely used in many fields of cancer imaging, in dosimetry for radionuclide therapy (18–20), and in the monitoring of anticancer drug distribution (21).
This study evaluated whether SPECT/CT and additional diagnostic contrast-enhanced CT before selective internal radiation therapy may be superior to SPECT or planar imaging alone when assessing treatment with 90Y microspheres in patients for gastrointestinal shunts before therapy.
MATERIALS AND METHODS
Patients
We enrolled 58 consecutive patients with unresectable HCC who underwent radioembolization with TheraSphere. The mean age was 66 y (range, 38–89 y). There were 10 women (17%) and 48 men (83%). Two of the 58 patients underwent separate MAA scans of the right and left liver lobes on different days. In 8 patients, MAA scans were repeated because of gastrointestinal shunting. Thus, 68 MAA scans were performed. Informed written consent was obtained from all patients before radioembolization with 90Y microspheres. All patients underwent 99mTc-MAA planar imaging, SPECT, and SPECT/CT of the liver.
MAA Scanning
Depending on the anatomy of the patient, 150 MBq of 99mTc-MAA were injected with a microcatheter either into the proper hepatic artery or the common hepatic artery after coil embolization of all visible nonhepatic arterial flow. If injection into the common or proper hepatic artery was not possible, the left and right hepatic arteries were injected separately. In variant anatomies, accessory or replaced vessels were injected separately. After MAA injection, the patient was transferred to the nuclear medicine department for imaging.
Image Acquisition
Anterior and posterior planar images of the whole body were obtained within 30 min after the MAA injection, using a dual-detector γ-camera with a mounted 2-row CT scanner (Symbia T; Siemens Healthcare). SPECT/CT images of the upper abdomen were acquired immediately after the delayed planar images. Acquisition parameters for SPECT were a 128 × 128 matrix with 128 frames (25 s/frame). The scan parameters for CT were 130 kV, 17 mAs, 5-mm slices, and image reconstruction with a medium smooth kernel. SPECT images were corrected for attenuation and scatter. The reconstructed data were visualized in sagittal, coronal, and axial slices. Fusion images were generated from the coregistered SPECT and low-dose CT images using the Esoft 2007 application package (Siemens Healthcare).
Image Interpretation
All images were masked as to patient identity. The images were reviewed for extrahepatic MAA deposition on a Syngo workstation (VD20K; Siemens Healthcare) by an experienced nuclear medicine physician and a radiologist, who achieved consensus. Images were read in the following order with an interval of 4 wk between reading sessions: planar images, SPECT (non–attenuation-corrected), SPECT/CT, and then SPECT/CT in combination with diagnostic contrast-enhanced CT.
Reference Standard
A combination of clinical and radiologic follow-up served as the standard of reference for extrahepatic gastrointestinal shunting. This follow-up included physical examination and laboratory tests on days 2, 7, 14, 21, 28, 90, and 180 after the intervention. Abdominal contrast-enhanced ultrasound, CT, and MRI were performed on days 30, 90, and 180 postinterventionally.
Data Analysis
On the basis of the standard of reference, potential gastrointestinal shunts detected on planar imaging, SPECT, and SPECT/CT were rated as true-positive, true-negative, false-positive, or false-negative. Sensitivities, specificities, and accuracies were calculated for all imaging modalities.
RESULTS
Extrahepatic shunting was revealed by planar imaging in 4, SPECT in 9, and SPECT/CT in 16 of the 68 examinations (true-positives) (Table 1). The number of false-positive results was 7 for planar imaging (13%), 7 for SPECT (13%), and 3 for SPECT/CT (6%). The number of false-negative results was 12 for planar imaging (75%), 7 for SPECT (44%), and 0 for SPECT/CT (100%). On the basis of these findings, the sensitivity in detecting extrahepatic shunting with planar imaging was 25%, the specificity was 87%, and the accuracy was 72%. For SPECT, the sensitivity was 56%, the specificity was 87%, and the accuracy was 79%. SPECT/CT had a sensitivity of 100%, a specificity of 94%, and an accuracy of 96%. The different sites of MAA injection in patients with extrahepatic shunting on SPECT/CT are listed in Table 2.
Detection of Gastrointestinal Shunting with Planar Imaging, SPECT, and SPECT/CT
Site of MAA Injection in Patients with Extrahepatic Shunting on SPECT/CT
Intensive nuclide deposition in the gallbladder was revealed in 4 patients by SPECT and in 6 by SPECT/CT. Two patients underwent elective cholecystectomy because the intensity of MAA deposition in the gallbladder was greater than or equal to that in the tumor.
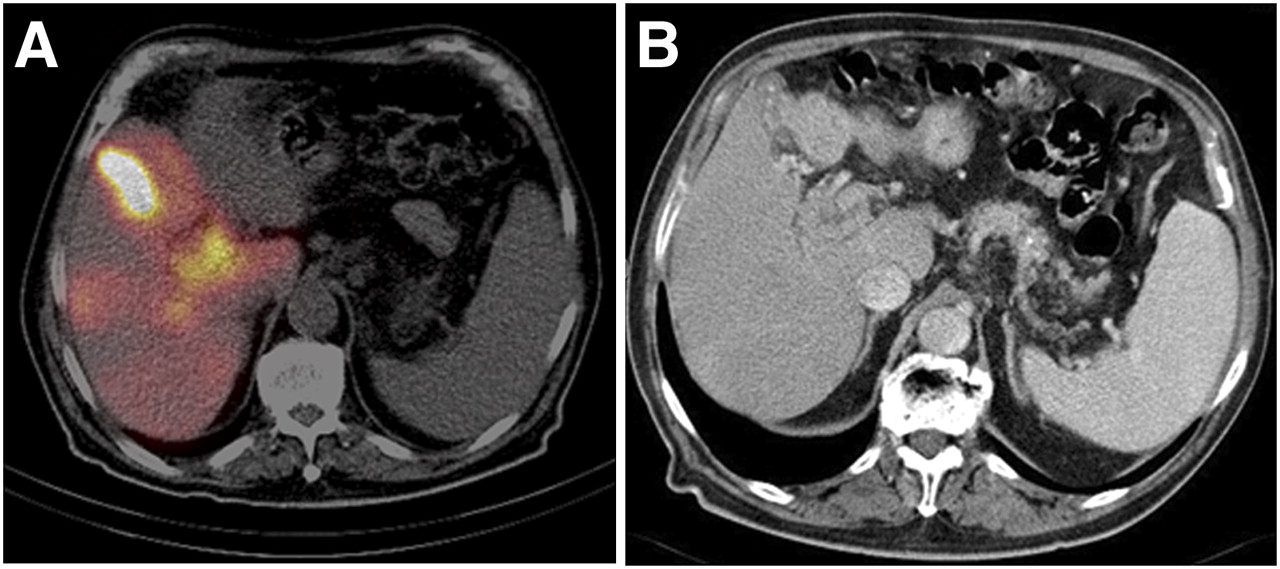
In 3 patients, MAA deposition in the liver hilum was misinterpreted as extrahepatic on SPECT/CT. Comparison of the SPECT/CT data of these 3 patients with previously acquired diagnostic contrast-enhanced CT showed that these MAA depositions were tumor uptake in portal vein tumor thrombi (Fig. 1). In 10 patients, extrahepatic MAA deposition was detected with SPECT/CT. This deposition was localized within the gastrointestinal tract in all patients. In 6 of these patients, the underlying vessel was found on repeated angiography and was coil embolized. In 2 others, the underlying vessel was detected but could not be embolized because of its small diameter. These patients were treated from a more distal catheter position. In the remaining 2 patients, no underlying artery was found on repeated angiography but MAA uptake persisted. These patients were not treated (Fig. 2). Thereby, nontarget seeding was successfully avoided.
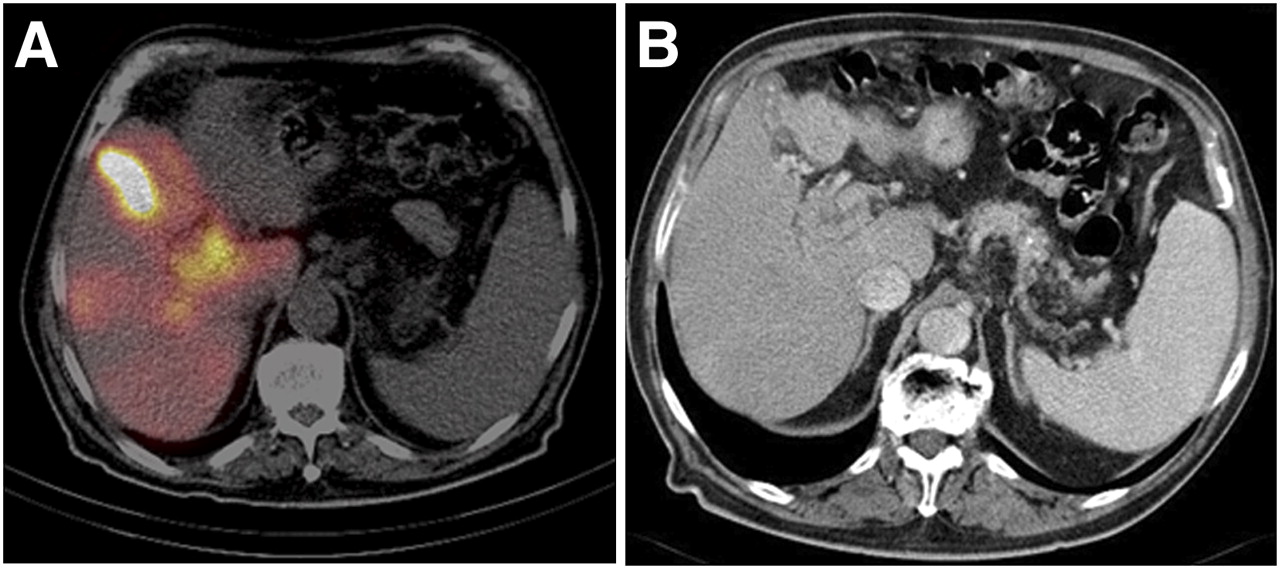
SPECT/CT and triple-phase diagnostic CT in patient with tumor infiltration of portal vein. (A) Extrahepatic MAA deposition in liver hilum is seen on low-dose SPECT/CT. (B) Triple-phase diagnostic CT reveals tumor thrombus in right branch of portal vein extending into main branch of portal vein. Finding on contrast-enhanced CT corresponds to MAA uptake on SPECT/CT.

SPECT/CT and angiography in 76-y-old man with HCC in right liver lobe. During the first angiography examination, MAA was injected into proximal right hepatic artery. No vessel leading to gastrointestinal tract was detected. (A) Strong tracer uptake (arrow) on SPECT was misinterpreted as segment 4 MAA uptake. (B) SPECT/CT localized MAA deposition (arrow) to duodenum. (C) On repeated angiography, small gastrointestinal vessel (arrow) originating from proximal right hepatic artery was detected. Repeated MAA injection was performed distally from this small vessel, and no shunting was visible on the following SPECT/CT.
No treated patient experienced gastrointestinal complications. None of the imaging modalities performed on days 30, 90, and 180 d after the treatment revealed signs of cholecystitis or pancreatitis. However, almost all patients experienced postembolization syndrome consisting of low-grade fever, loss of appetite, and fatigue for up to 6 wk after the treatment.
DISCUSSION
Our data show that SPECT with integrated low-dose CT before radioembolization with 90Y microspheres is superior to SPECT or planar imaging alone in the detection of gastrointestinal MAA deposition. Additional diagnostic contrast-enhanced CT further increases specificity in patients with portal vein thrombosis by differentiating tumor-associated MAA deposition in the portal vein from that in extrahepatic locations.
We found approximately 40% more patients with gastrointestinal MAA accumulation using SPECT/CT than with SPECT alone (16 vs. 9 of 68 examinations). Planar scanning was able to detect gastrointestinal MAA deposition in only 4 patients. Although SPECT or planar scanning is widely used before radioembolization with 90Y microspheres (9,16,17), data on their accuracy to detect gastrointestinal MAA deposition have only rarely been published. To date, the value of SPECT/CT before treatment with 90Y microspheres has been investigated only in patients with colorectal cancer, and consistent with our data, Denecke et al. found more gastrointestinal MAA uptake using SPECT/CT than using SPECT (16).
In our study, the follow-up did not show any case of gastrointestinal adverse events. Previous investigations, however, have reported gastrointestinal complications after radioembolization. Jakobs et al. published a series of 39 patients treated with 90Y microspheres and reported a patient with an actinic gastric ulcer and a patient with edematous pancreatitis, which was most likely the result of ectopic embolization via undetected vascular branches into these organ territories (2). Dancey et al. found gastrointestinal ulcers in 3 of 22 patients (3). Neither study involved SPECT/CT in the planning of radioembolization with 90Y microspheres. Although gastrointestinal complications are rare and their incidence may decrease with an increasing learning curve, according to the cited studies it may be assumed that the use of SPECT/CT in planning radioembolization with 90Y microspheres may contribute to the safety of this treatment modality. However, larger patient series are required to support this hypothesis.
The reference standard consisting of clinical and radiologic follow-up may be considered a limitation of the study. The most reliable reference standard for extrahepatic radionuclide deposition may have been endoscopy with biopsy of visually suggestive regions of the gastrointestinal wall. However, this approach would have been rather invasive and would not have included the mid and distal portions of the small intestine or any nongastrointestinal sites (e.g., the pancreas, the abdominal wall, lymph nodes). We, therefore, decided on a combination of clinical and radiologic follow-up as the standard of reference. Another limitation may be the fact that all patients with gastrointestinal MAA deposition were excluded from treatment with 90Y microspheres in this analysis if no causative gastrointestinal vessel was identified. It is not clear whether these patients would really have been affected by gastrointestinal side effects if they had been treated. Therefore, a presumably safer algorithm avoiding gastrointestinal side effects may also lead to exclusion of more patients from therapy, as other algorithms probably will.
We initially misinterpreted SPECT/CT scans in 3 patients with MAA accumulation in the liver hilum. Subsequent diagnostic contrast-enhanced CT was able to locate the tracer accumulation in the portal vein, indicating tumor invasion as a common finding in patients with advanced HCC (22). In these 3 patients, the exclusion of extrahepatic MAA deposition was important to enable radioembolization with 90Y microspheres. In view of these cases, a SPECT/CT protocol including diagnostic CT data (full-dose CT with contrast agents) may be discussed.
Occasionally, radioembolization may lead to radiation-induced cholecystitis (7,12,23). Both SPECT and SPECT/CT revealed patients with MAA depositions in the gallbladder. Unfortunately, in 2 of these patients it was not possible to position the catheter distal to the cystic artery because otherwise some parts of the tumor tissue would not have been sufficiently irradiated. In our study, these patients underwent cholecystectomy. However, we do not know if radiation-induced cholecystitis would have developed in these patients had they not undergone cholecystectomy. The risk of radiation-induced cholecystitis, when microspheres are infused from a catheter proximal to the cystic artery, has been discussed controversially. Our current approach includes prophylactic cholecystectomy in those patients in whom MAA uptake in the gallbladder wall is above the level of the nontumorous liver parenchyma. Nevertheless, dosimetric models and animal experiments are required to estimate the dose–effect relationship with regard to cholecystitis.
CONCLUSION
SPECT with integrated low-dose CT using 99mTc-MAA is beneficial in radioembolization with 90Y microspheres because it increases the sensitivity and specificity of 99mTc-MAA SPECT when detecting extrahepatic arterial shunting. The overall low risk of gastrointestinal complications in radioembolization may therefore be further reduced by SPECT/CT.
Acknowledgments
We appreciate the technical support of Wilfried Sonnenschein and Dietmar Wedeleit.
Footnotes
-
COPYRIGHT © 2009 by the Society of Nuclear Medicine, Inc.
References
- Received for publication September 23, 2008.
- Accepted for publication January 15, 2009.
In this issue





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Liver Function Changes After Technetium-99m-Macroaggregated Albumin Administration and Their Predictive Value Regarding Hepatotoxicity in Patients Undergoing Yttrium-90-Radioembolization
- A Prospective Study of Quantitative SPECT/CT for Evaluation of Lung Shunt Fraction Before SIRT of Liver Tumors
- Intraarterial Hepatic SPECT/CT Imaging Using 99mTc-Macroaggregated Albumin in Preparation for Radioembolization
- Systematic Evaluation of Tumoral 99mTc-MAA Uptake Using SPECT and SPECT/CT in 502 Patients Before 90Y Radioembolization
- Predictive Value of Intratumoral 99mTc-Macroaggregated Albumin Uptake in Patients with Colorectal Liver Metastases Scheduled for Radioembolization with 90Y-Microspheres
- From the Angio Suite to the {gamma}-Camera: Vascular Mapping and 99mTc-MAA Hepatic Perfusion Imaging Before Liver Radioembolization--A Comprehensive Pictorial Review
- Image-Guided Personalized Predictive Dosimetry by Artery-Specific SPECT/CT Partition Modeling for Safe and Effective 90Y Radioembolization
- Clinical Feasibility of Fast 3-Dimensional Dosimetry of the Liver for Treatment Planning of Hepatocellular Carcinoma with 90Y-Microspheres
- Significance of Oral Administration of Sodium Perchlorate in Planning Liver-Directed Radioembolization
- Phase III Trial Comparing Protracted Intravenous Fluorouracil Infusion Alone or With Yttrium-90 Resin Microspheres Radioembolization for Liver-Limited Metastatic Colorectal Cancer Refractory to Standard Chemotherapy
- The Significance of 99mTc-MAA SPECT/CT Liver Perfusion Imaging in Treatment Planning for 90Y-Microsphere Selective Internal Radiation Treatment