


Abstract
Iodine kinetics and lesion dose per administered 131I activity (LDpA) of differentiated thyroid cancer metastases were determined using 124I PET. These data were analyzed to derive an optimized dosimetry protocol. Methods: We evaluated the time-activity-concentration curves of 37 lesions in 17 patients who had undergone thyroidectomies. LDpA determination involved 124I PET images acquired at 4, 24, 48, 72, and 96 h after intake of a capsule containing 20–40 MBq of 124I. A combination of a linear and a monoexponential or a monoexponential function only parameterized the time-activity-concentration curves. The LDpAs, calculated using data from all 5 PET time points, served as reference. The lesions were classified into 3 groups, according to potential for cure with 131I therapy: low (≤5 Gy GBq−1; n = 14), medium (between 5 and 10 Gy GBq−1; n = 9), or high LDpAs (>10 Gy GBq−1; n = 14). Using the reference approach, the differences in the empiric kinetic parameters within the LDpA groups were evaluated. The reference LDpAs were compared with those derived from only 2, 3, or 4 PET data points and from 1 adapted 2-point approach. Lin's concordance correlation coefficient (ρc) and the mean absolute percentage deviation in LDpAs were used to assess agreement between simplified and reference approaches. Results: The effective 124I half-life, linear activity–concentration rate (α), and 24-h activity concentration (CpA) (the latter 2 per administered 124I activity) differed significantly among the LDpA groups (P < 0.05). LDpAs correlated with 24-h CpAs (r = 0.94, P < 0.001). Using the 4-, 24-, and 96-h measurements, a ρc value of greater than or equal to 0.90 was found, and the mean absolute percentage deviation was less than or equal to 16%. Similar statistical values were obtained for the adapted approach, which was based on 24- and 96-h PET data points only. Conclusion: Lesion classification into LDpA groups was feasible using a single PET scan at ∼24 h. Because of the highly variable kinetics, 1 additional measurement at ∼96 h was needed to obtain a sufficiently reliable LDpA estimate. The adapted 24-96-h approach appears to be the optimal 124I protocol and is a reliable simplification of the 5-point protocol.
Several groups (1–5) have successfully used 124I PET alone and with CT to guide postsurgical treatment and, in particular, radioiodine therapy in patients with differentiated thyroid carcinoma (DTC). Preradiotherapeutic 124I PET is valuable in restaging disease; dosimetric analysis of the imaging data can identify the patients most likely to benefit from radioiodine therapy and can determine safe and effective individualized therapeutic activities of radioiodine.
Our original 124I PET dosimetry protocol entailed 5 PET measurements at 4, 24, 48, 72, and 96 h after 124I administration (2). Other 124I PET dosimetry protocols have relied on fewer measurement points. Erdi et al. (3) used a 3-point model with the first scan at ∼4 h and the last scan at ∼24 or ∼96 h after radioisotope intake. Eschmann et al. (4) relied on 4 daily scans, starting at 24 h after 124I administration. Sgouros et al. (5) generally obtained 3 PET images, at ∼4, ∼20, and ∼44 h after 124I administration; sometimes a fourth scan was acquired at 96–144 h. However, to our knowledge, no group has yet published the results of any systematic investigation to determine the number and timing of PET scans needed for an optimized protocol that provides sufficiently reliable data on lesional absorbed dose while minimizing the quantity and time range of scans. By reducing the logistical and time demands on patients and clinic staff, such a protocol would decrease inconvenience and health care costs and help make 124I PET dosimetry more widely available and user-friendly. We therefore conducted the present protocol optimization study.
MATERIALS AND METHODS
Study Design
We retrospectively compared our original 5-measurement-point 124I PET dosimetry protocol (the reference approach) with various alternative protocols, using data from fewer measurement times for accuracy in determining DTC lesional radiation doses. The comparison was made within each of 3 lesion groups, classified on the basis of potential for cure by radioiodine therapy as reflected by a low, medium, or high lesion dose per administered activity of 131I (LDpA) in Gy GBq−1. The first part of the study comprised a permutation analysis examining all evaluable alternative protocols. The second part of the study, the empiric analysis, used findings from the permutation analysis and from the reference iodine kinetic parameters to develop and assess one adapted approach, offering still greater simplicity.
Patients and Lesions
The study included 17 patients (10 women, 7 men) who had at least 1 metastatic DTC lesion. Mean (±SD) age was 56 ± 16 y (median, 53 y; range, 32–83 y). The 17 patients had a total of 37 iodine-avid metastatic lesions (19 of which involved the lymph nodes, 5 the lungs, 10 the bone, and 3 other sites). DTC histology was papillary in 12 and follicular in 5 cases. Thirteen of the 17 patients had undergone 1–7 previous radioiodine therapies (mean ± SD, 2.7 ± 1.8; median, 2), with a mean (±SD) cumulative activity of 16.9 ± 14.3 GBq (median, 14 GBq; range, 3–52 GBq). The study dosimetry took place before the first or second radioiodine therapy in 4 patients and before the third to eighth radioiodine therapy in the remaining 9 patients.
Tomograph, Acquisition, and Image Reconstruction
Tomograph
PET was performed using a scanner (ECAT EXACT HR+; CTI/Siemens) at approximately 4, 24, 48, 72, and 96 h after oral intake of a capsule containing 20–40 MBq of 124I–sodium iodide. Details on radionuclide production and calibrated activity measurement were published elsewhere (6). 124I was given when serum thyroid-stimulating hormone levels were greater than or equal to 25 μL−1 after either at least 4 wk without thyroid hormone (n = 10) or 24 h after the second of 2 consecutive daily intramuscular injections of recombinant human thyroid-stimulating hormone (Genzyme Corp.) (n = 7).
Acquisition
PET measurements were acquired in 3-dimensional mode, with scanning from the thigh or abdomen to the head using 5–8 bed positions with an emission time of 281 s each. The data were corrected for attenuation by a measured transmission scan (138 s/bed position) and standard scatter correction.
Image Reconstruction
Image reconstruction was performed after Fourier rebinning with attenuation-weighted ordered-subset expectation maximization using 8 subsets, 2 iterations, and a 5-mm gaussian filter. The resulting PET image had 256 × 256 voxels (voxel size, 1.72 × 1.72 × 2.43 mm3). In clinical applications, the image resolution expressed as full width at half maximum (FWHM) was 8 mm (6).
Determination of the Activity Concentration
The measured activity concentration was obtained using circular FWHM-sized regions of interest (ROIs) (8-mm diameter) (6). This resolution ROI technique has been proposed for determining recovery coefficients in phantom measurements needed for quantification and, therefore, should also be applied to patient data (7). For large lesions (diameter ≥ 1.5 cm), the mean activity concentration was determined by averaging the concentrations in FWHM-sized ROIs drawn in the centers of the slice with the maximum lesion activity concentration and of 2 corresponding adjacent slices (±1). The concentrations of smaller lesions (diameter < 1.5 cm) were obtained using a line profile (the mean activity concentration in the FWHM-sized ROI vs. axial distance), which was fitted with a gaussian function; the corresponding gaussian amplitude was taken as the lesion activity concentration. Images were analyzed with software (ECAT 7.2.1; CTI/Siemens).
Lesion Volume and Recovery Correction
Lesion Volume
Lesion volumes were obtained using the PET-based iterative thresholding method; the lesions were assumed to be ellipsoidal (8). An effective lesion diameter was calculated to apply the recovery correction method; that is, an effective sphere of the same volume can replace the ellipsoidal lesion volume. The mean absolute percentage deviation between CT and PET was ∼10% for lesion volumes from 0.8 to 7.5 mL and ∼15% for volumes greater than 7.5 mL (8).
Recovery Correction
For lesions of simple geometric shape, recovery effects can be corrected for by using recovery coefficients (RCs) determined in phantom measurements, as described elsewhere (6) for the study PET system. The measured activity concentration, Cmsd, can be corrected for by using the equation Ccor = Cmsd RC−1 (9). Remarkably, even for large lesions (e.g., 37-mm diameter), the 124I recovery coefficient determined for our PET system was 0.78, not unity, a phenomenon mainly associated with the complex decay scheme of the radionuclide (6). The reliability of the recovery correction depended on the lesion volume determination. Phantom measurements mimicking in vivo conditions in patients with DTC demonstrate that the maximum absolute percentage deviation between expected and measured 124I activity concentrations after applying recovery correction was about 10% for sphere volumes greater than or equal to 1 mL and about 20% for sphere volumes of 0.5 mL (6).
Parameterizing Lesional Time-Activity-Concentration Curve and Estimating Lesional Cumulated Activity Concentration (CAC)
Parameterizing the Time-Activity-Concentration Curve
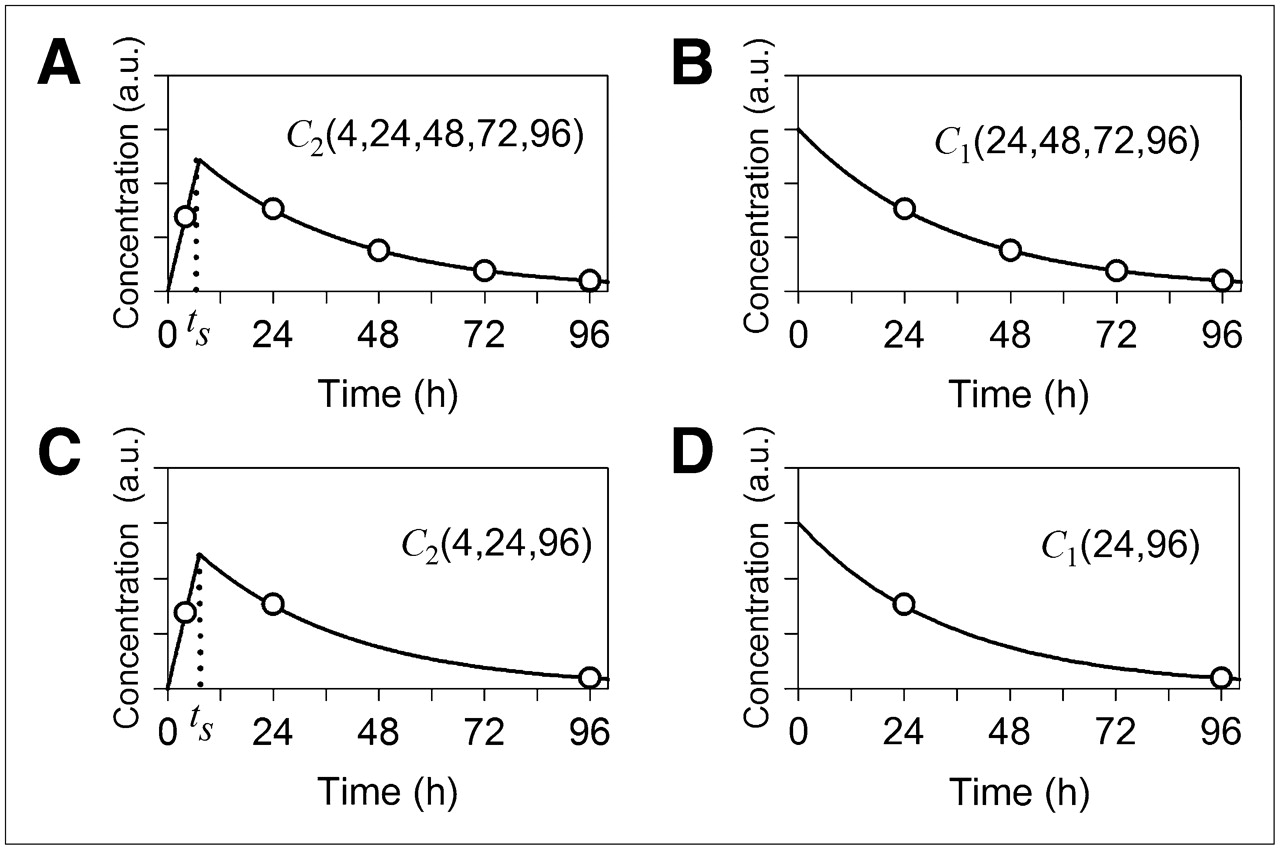
The lesional time-activity-concentration curve was parameterized to determine the CAC using 1 of 2 functional models (Fig. 1): Eq. 1
Eq. 1 Eq. 2where C0 was the (extrapolated) concentration at time zero, 124ITeff the effective half-life of 124I, and α the initial linear time-activity-concentration rate. The time, ts, indicated the point of intersection of the linear function (α·t) with the monoexponential function (Fig. 1A). The corresponding CAC was the integral of C(t) from zero to infinity. To avoid ambiguity caused by the limited number of data points, no curve-fitting procedure was used. The parameters of the functions C1(t) and C2(t) were determined algebraically: C1(t) required at least 2 points, whereas C2(t) required 3 points including the 4-h measurement (for the slope α) plus 2 later points (C0, 124ITeff). A linear regression analysis (plot of logarithm of activity concentration vs. time) was undertaken to obtain the 2 parameters, C0 and 124ITeff, in the exponential function.
Eq. 2where C0 was the (extrapolated) concentration at time zero, 124ITeff the effective half-life of 124I, and α the initial linear time-activity-concentration rate. The time, ts, indicated the point of intersection of the linear function (α·t) with the monoexponential function (Fig. 1A). The corresponding CAC was the integral of C(t) from zero to infinity. To avoid ambiguity caused by the limited number of data points, no curve-fitting procedure was used. The parameters of the functions C1(t) and C2(t) were determined algebraically: C1(t) required at least 2 points, whereas C2(t) required 3 points including the 4-h measurement (for the slope α) plus 2 later points (C0, 124ITeff). A linear regression analysis (plot of logarithm of activity concentration vs. time) was undertaken to obtain the 2 parameters, C0 and 124ITeff, in the exponential function.

Schematic representation of time-activity-concentration curves of reference approach (A) and representative alternative approaches (B–D) to estimate LDpA. a.u. = arbitrary units.
Estimating the CAC
The functional model C1 was chosen to estimate the CAC unless the 4-h PET data were included in the dataset, in which case the functional model C2 was used. Two-point models including the 4-h PET measurement were excluded from the analysis because of their inability to represent accurately the time-activity-concentration curve. In total, 21 alternatives to the reference approach were analyzed: six 2-point, ten 3-point, and five 4-point approaches; representative examples appear in Figures 1B, 1C, and 1D. The following name convention was chosen: the first symbol, C1 or C2, denoted the functional model describing the time-activity-concentration curve and the numbers in parentheses were the PET measurement time points in hours after 124I administration. For instance, C1(24,96) (Fig. 1D) is a 2-point model using 24- and 96-h PET measurements, and the time-activity-concentration curve is described by a monoexponential function. The reference approach was termed C2(4,24,48,72,96) (Fig. 1A).
Group Classification and LDpA
Group Classification
The studied lesions were classified into 3 groups, according to the likelihood of success of radioiodine therapy, based on the projected LDpA determined using the reference approach: low (≤5 Gy GBq−1), medium (>5 Gy GBq−1 to ≤10 Gy GBq−1), and high LDpA (>10 Gy GBq−1). These cut-offs were calculated on the basis of the findings of Maxon et al. (10) that minimum lesion radiation doses of 85–140 Gy are necessary to successfully treat nodal metastases and on the basis of the maximum single activity of 15 GBq found by our department.
The LDpA was calculated as follows: Eq. 3where C(t) was the 131I activity concentration corrected for the difference in physical half-lives of 124I (tracer nuclide) and 131I (therapeutic nuclide), Δ the equilibrium 131I dose constant for nonpenetrating radiation (0.11 Gy g/MBq−1 h−1) (11), Atr the tracer activity shortly after capsule administration, and ρ the tissue density (1 g/mL−1). 124I and 131I kinetics were assumed to be identical; therefore, the CAC could be transformed if the 124I lesion kinetics were known. The self-irradiation (lesion-to-lesion) absorbed dose was calculated using the MIRD formula.
Eq. 3where C(t) was the 131I activity concentration corrected for the difference in physical half-lives of 124I (tracer nuclide) and 131I (therapeutic nuclide), Δ the equilibrium 131I dose constant for nonpenetrating radiation (0.11 Gy g/MBq−1 h−1) (11), Atr the tracer activity shortly after capsule administration, and ρ the tissue density (1 g/mL−1). 124I and 131I kinetics were assumed to be identical; therefore, the CAC could be transformed if the 124I lesion kinetics were known. The self-irradiation (lesion-to-lesion) absorbed dose was calculated using the MIRD formula.
Statistics
Comparisons of alternatives to the reference approach were performed separately for each LDpA group using Lin's concordance correlation coefficients (ρc) along with 95% confidence intervals (CIs) (12) and the mean absolute percentage deviation (Δ) between the alternatives and the reference approach. The ρc value evaluates the degree to which paired measures fall on the 45° line through the origin. The compared approaches are regarded as equivalent if the ρc is above a specified threshold (agreement increases as ρc approaches 1.0). Whether agreement is excellent, moderate, or poor is a subjective decision. Partik's criteria (13) grade ρc values more than 0.95 as excellent and values more than 0.90 as very good. In the present study, approaches with ρc values of at least 0.90 were regarded as equivalent.
Differences within the LDpA groups were evaluated by the Kruskal-Wallis ANOVA on ranks, a nonparametric test, and the pairwise differences (between-group analysis) were evaluated by the Dunn test. Statistically significant differences were assumed at a P value of less than 0.05. Software (Stata 9.1; StataCorp) was used for computation.
RESULTS
Reference Iodine Kinetics and Dosimetry Data
Table 1 summarizes selected key reference kinetic variables, and Figure 2 shows examples of the reference time-activity-concentration curve and fits for each reference LDpA group. The LDpA ranged from 1.1 to 215 Gy GBq−1 (median, 7.9 Gy GBq−1; mean, 36.9 Gy GBq−1), and high intra- and interpatient variability was observed. The 24-h 124I activity concentration ranged from 2.3 to 367 kBq/mL−1 (median, 22 kBq/mL−1; mean, 77 kBq/mL−1), and the 24-h 124I lesional uptake ranged from 0.01% to 8.4% (median, 0.11%; mean, 0.56%). The lesion volume ranged from 0.7 to 28 mL (median, 1.0 mL; mean, 2.4 mL). The effective half-life, the α per administered 124I activity (RpA), and the 24-h activity concentration per administered 124I activity (CpA) showed significant differences among the LDpA groups (P < 0.002, ANOVA). Specifically, the effective half-lives, 24-h CpA, and RpA deviated significantly between the low- and high-LDpA groups (P < 0.05, Dunn test) as did the 24-h CpA and RpA between the medium- and high-LDpA groups (P < 0.05, Dunn test). The interception points, tS, showed no significant differences among the reference LDpA groups. The median (mean ± SD) interception point for all 37 lesions was 8.0 h (8.8 ± 4.2 h).
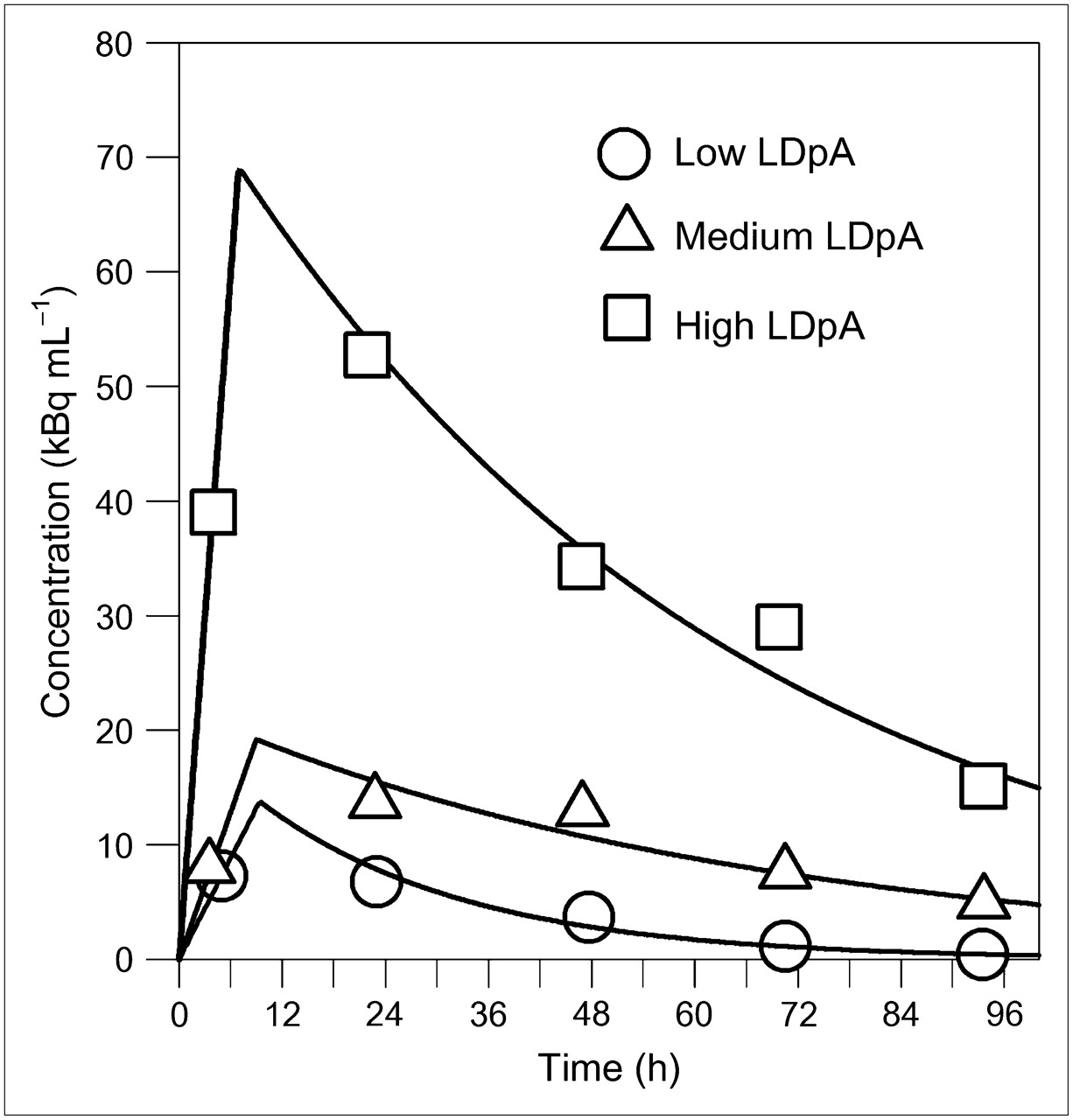
Representative examples of 124I time-activity-concentration curves of low-, medium-, and high-LDpA groups. Curves were determined using reference approach C2(4,24,48,72,96). Open circles are data taken from serial PET images.
Reference Kinetic Parameters in DTC Metastases by LDpA Group
The reference 24-h CpAs correlated well with the reference LDpAs (Pearson correlation coefficient, 0.94; P < 0.001) and therefore appeared to be a good alternative to the reference LDpA for the group classification. If the 24-h CpA values only were used, the minimum number of lesions (n = 3; lesions 12, 17, and 22) was miscategorized relative to the reference LDpA when the following reference CpA thresholds were selected: low group (n = 14), less than 0.45 kBq/mL−1 MBq−1; medium group (n = 8), 0.45–1.0 kBq/mL−1 MBq−1; high group (n = 15), greater than 1.0 kBq/mL−1 MBq−1.
Permutation Analysis
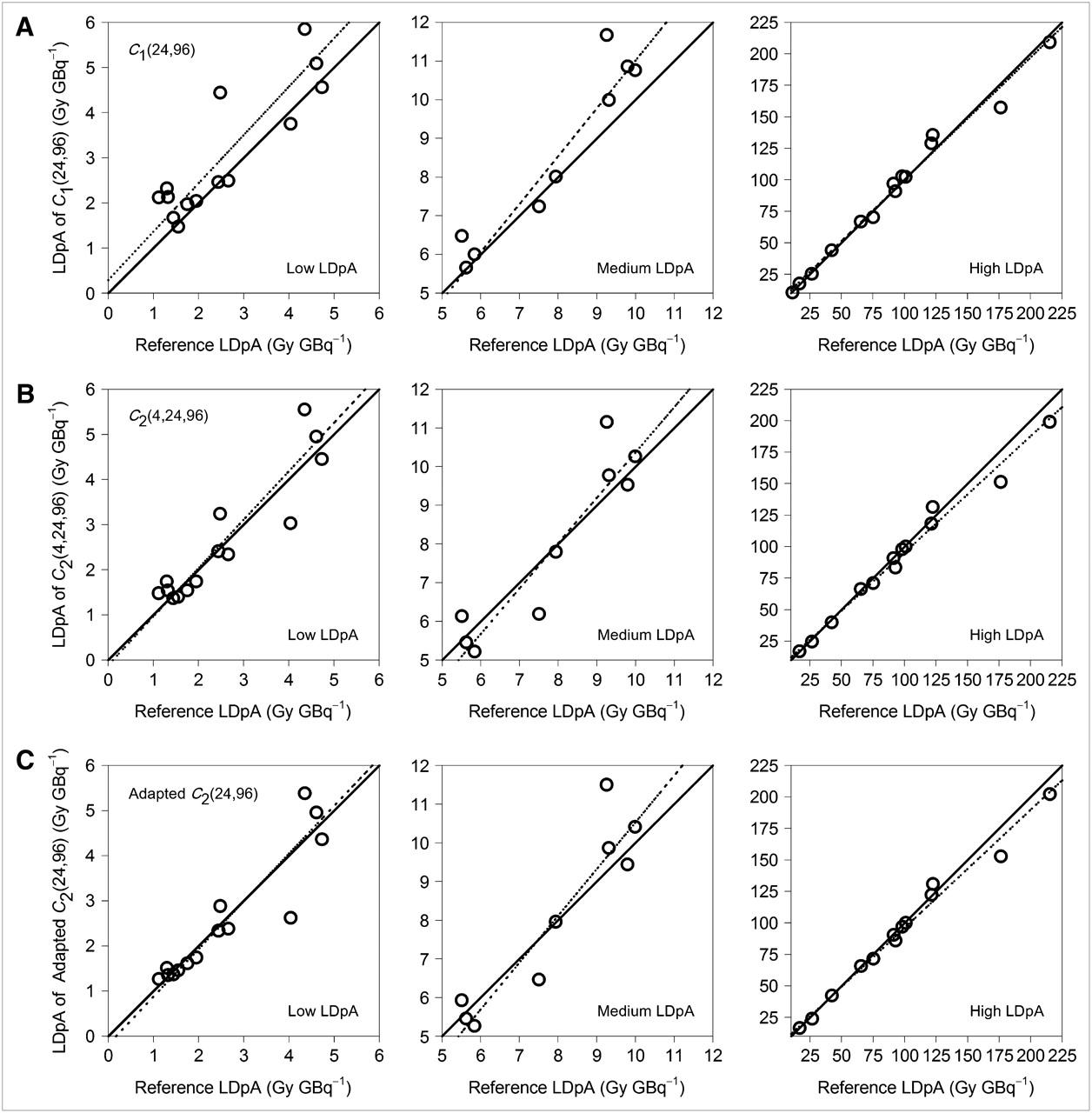
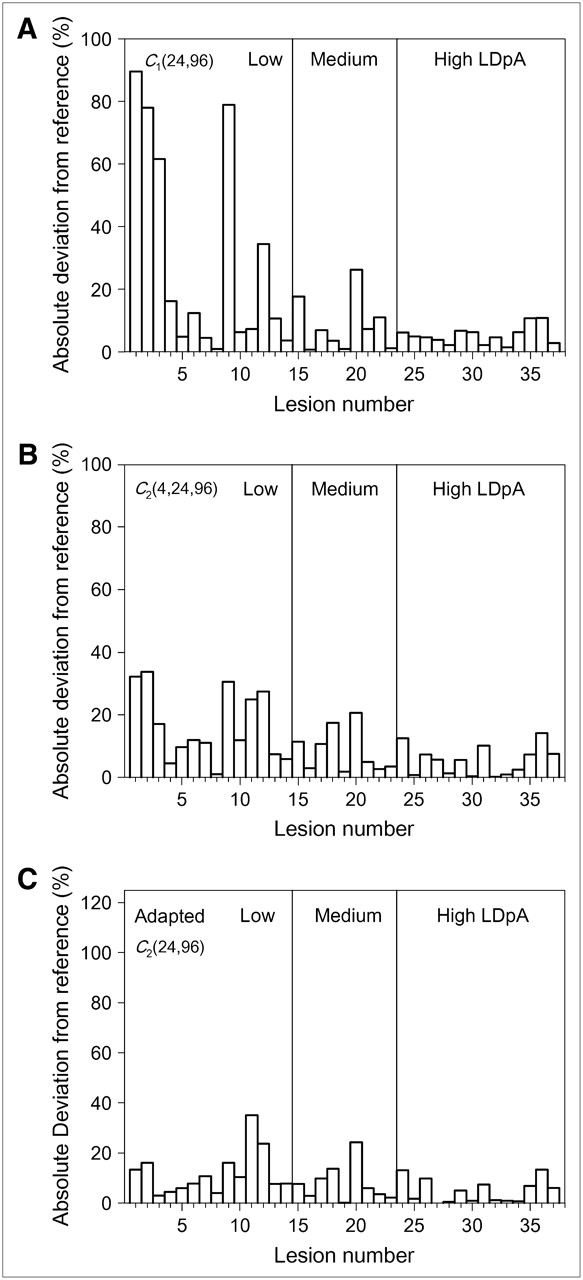
Analysis of Lin's correlation coefficients for all studied alternative approaches showed that only 2, C1(24,96) and C2(4,24,96), were of interest for protocol optimization that substantially reduced the number of PET scans. Table 2 lists Lin's coefficients and the mean absolute percentage deviations in LDpA for some representative approaches. Figure 3 shows Lin's concordance correlation plots. Figure 4 depicts the individual absolute percentage deviation in LDpA of each lesion between C1(24,96) (panel A) or C2(4,24,96) (panel B) versus the reference approach. Using C1(24,96), the mean absolute percentage deviation was 8% (maximum, 26%) for the medium-LDpA group and 5% (maximum, 11%) for the high-LDpA group, whereas the mean absolute percentage deviation of 29%, a maximum percentage deviation of 90%, and a ρc value of less than 0.90 for the low-LDpA group was unacceptable. Adding the 4-h data point, specifically using C2(4,24,96), the mean absolute percentage deviation for the low-LDpA group decreased to 16% (maximum, 34%) and the ρc value increased to 0.92. The medium-LDpA group showed an acceptable mean absolute percentage LDpA deviation for the C1(24,96) approach; however, if the 4-h data point was not considered, the ρc value was slightly less than 0.90. This finding was probably associated with the small number of lesions (n = 9) in this group. Thus, including the 4-h data point appeared to be necessary for protocol optimization, especially in the low-LDpA group, but of minor relevance to protocol optimization in the medium- and, particularly, the high-LDpA groups.

Lin's concordance correlation plots for C1(24,96) (A), C2(4,24,96) (B), and adapted C2(24,96) approaches (C), along with line of identity (solid) and reduced major axis regression line (dotted).
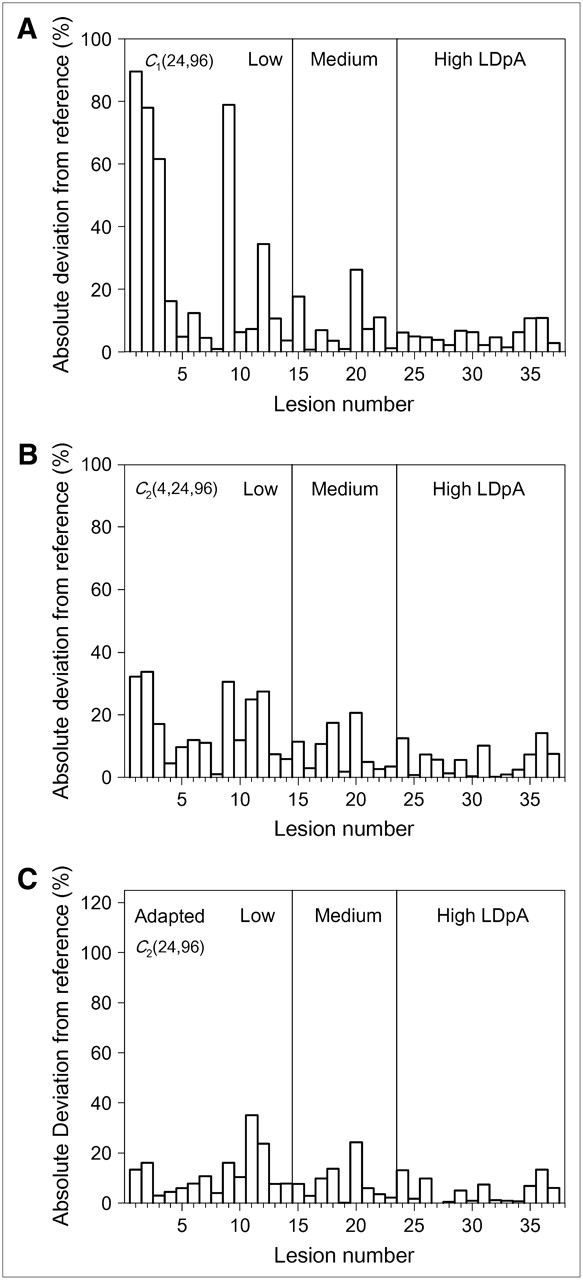
Absolute percentage deviations in LDpA for each of 37 studied lesions between C1(24,96) (A), C2(4,24,96) (B), or adapted C2(24,96) (C) versus reference approach.
Lin's Concordance Correlation Coefficients and 95% CI and Mean Absolute Percentage Deviations in LDpA (Δ in %) Between Alternative and Reference Approaches
Empiric Analysis
The permutation analysis showed that the C1(24,96) approach produced acceptable estimates of the absorbed dose for lesions that were in the high- or medium- but not in the low-LDpA group. This is because the LDpA fraction arising from the integral of C(t) from zero to ts, that is, the linear contribution to the total LDpA, was often larger for lesions in the low- than for lesions in the medium- or high-LDpA groups. To compensate for this phenomenon, a fixed interception point was chosen to estimate the linear contribution, as no significant intergroup difference was found for the interception points. Specifically, the adapted approach used data points from only 2 (24- and 96-h) PET scans and an assumed fixed interception point of 8 h (the median for all 37 lesions). The absorbed dose of this adapted 24-96-h approach was estimated using the functional model C2: Eq. 4where
Eq. 4where  is the 24-h CpA for 124I and
is the 24-h CpA for 124I and  is the effective half-life calculated from 24- and 96-h 124I PET measurements via linear regression analysis. 131ITeff is the effective half-life for 131I. The time of PET measurement at ∼24 h is designated by the symbol t24 and 131Its (≈ 124Its) is the fixed interception point of 8 h. The other symbols are defined earlier in the description of Equation 3. Table 2 lists the relevant statistical variables, and Figure 3C shows Lin's concordance correlation plots for this adapted approach. Lin's coefficients were identical with those of C2(4,24,96). Figure 4C depicts the individual absolute percentage deviation of each lesion with the adapted C2(24,96) versus the reference approach. The mean absolute percentage deviation was 12% (maximum, 35%) for the low-, 8% (maximum, 14%) for the medium-, and 5% (maximum, 13%) for the high-LDpA group.
is the effective half-life calculated from 24- and 96-h 124I PET measurements via linear regression analysis. 131ITeff is the effective half-life for 131I. The time of PET measurement at ∼24 h is designated by the symbol t24 and 131Its (≈ 124Its) is the fixed interception point of 8 h. The other symbols are defined earlier in the description of Equation 3. Table 2 lists the relevant statistical variables, and Figure 3C shows Lin's concordance correlation plots for this adapted approach. Lin's coefficients were identical with those of C2(4,24,96). Figure 4C depicts the individual absolute percentage deviation of each lesion with the adapted C2(24,96) versus the reference approach. The mean absolute percentage deviation was 12% (maximum, 35%) for the low-, 8% (maximum, 14%) for the medium-, and 5% (maximum, 13%) for the high-LDpA group.
DISCUSSION
Using the reference approach (5 PET measurement points from 4 to 96 h), the present study found broadly similar radioiodine kinetics to those observed by other groups investigating 124I PET dosimetry, albeit we noted wider ranges and higher maximum values than did those groups (3–5). Our LDpA range was 1.1–215 Gy GBq−1. Eschmann et al. (4), who used a combination of the Marinelli formula and MIRDOSE3.1 to estimate the absorbed dose, obtained an LDpA range of 10–21 Gy GBq−1 in 4 metastatic lesions in 2 patients. A mean dose range of 0.4–24.4 Gy GBq−1 (3 lesions) was reported by Erdi et al. (3) and a mean dose range of 0.08–49 Gy GBq−1 (56 lesions) by Sgouros et al. (5), who performed a point-kernel-based calculation and 3-dimensional internal dosimetry. The 124I effective half-life in metastases ranged from 6 to 80 h in the present study, 14 to 43 h in the study of Erdi et al. (3), and 22 to 65 h in the study of Eschmann et al. (4). No effective 124I half-lives were reported by Sgouros et al. (5). The present work also confirmed and extended the observation of the study of Sgouros et al. (5) (the only other published investigation of more than a handful of lesions) that in DTC metastases, LDpAs and 124I effective half-lives showed a broad variability, even within a single patient; for example, an individual could have both low- and medium-/high-LDpA lesions.
The clinical course of DTC is often favorable, and standardized radioiodine therapy is well established and frequently successful. In selected patients, an individual therapy needs to be performed at the limits, and prospective dosimetry is required. A reliable 124I dosimetry protocol necessitates multiple PET measurements over a few days. This entails substantial clinical resources and costs. The 5-d protocol (4–96 h) is certainly the most accurate among the approaches investigated. More PET data points are even more accurate, but a cost-benefit protocol implies a trade-off between accuracy and effort that should relate to the importance of the clinical decision.
The LDpAs determined in this work were subject to uncertainties. The physical errors mainly arose from the determination of the lesion volume and of the 124I activity concentrations including recovery correction. The volume was determined assuming that the lesions were ellipsoids, as more complicated shapes cannot be easily handled in a clinical setting. The error range of the volume determination was ∼10% to ∼15% (8) and the size-dependent recovery coefficients were influenced by the accuracy of the volume determination (6). Phantom measurements mimicking in vivo conditions showed that the maximum inaccuracy of the 124I activity concentration after recovery correction was ∼10% for spheres with an inner volume of 1 mL or more and ∼20% for spheres with a 0.5-mL volume (6). Other possible uncertainties are biologic factors occurring during 124I diagnostic procedures and 131I therapy. The estimated absorbed dose based on pretreatment diagnostics and the actual dose determined after therapy differ because of a faster-than-expected release of radioiodine in the immediate aftermath of radioiodine therapy (10); the reason is probably the immediate onset of therapeutic effects during 131I treatment. Finally, radioiodine distribution is known to be inhomogeneous. The inaccuracies of biologic factors are a priori unquantifiable.
In total, the estimated physics-related error range using the reference approach may total 20–30%. This error range is acceptable for an optimized 124I dosimetry protocol to provide pretherapeutic lesional absorbed dose estimates in patients scheduled for high-dose 131I therapy when 2 or more PET scans can be avoided.
Physicians are primarily interested in whether the administration of reasonable 131I activities is likely to achieve a clinically meaningful response or likely to fail. In association with the radiation dose threshold for successful treatment (5–10 Gy GBq−1 or larger), the LDpA is the key to providing this information. Our permutation analysis suggested that the 2 earliest (4 and 24 h) and the latest PET data points (96 h) provided robust estimates of the LDpA; that is, the C2(4,24,96) approach using these 3 data points yielded a ρc greater than or equal to 0.90 and a mean absolute percentage deviation less than or equal to 16% relative to the reference approach. More important, similar Lin's coefficients and absolute deviations were found for the adapted 24-96-h approach, which uses only 2 PET scans and a fixed interception point of 8 h. Thus, this 2-point protocol appears to offer the best trade-off between accuracy and effort. Especially if the clinical workload is heavy, the adapted 24-96-h approach appears to be a good alternative, as the only potential cure is either radioiodine therapy or surgery. A flow chart illustrating the optimized dosimetry protocol (i.e., the adapted 24-96-h approach) is given in Figure 5. The clinical decision to perform the 96-h measurement depends on the LDpA classification; that is, a very low 24-h CpA (low-LDpA classification) implies that radioiodine therapy is likely to fail and surgery may be more appropriate.
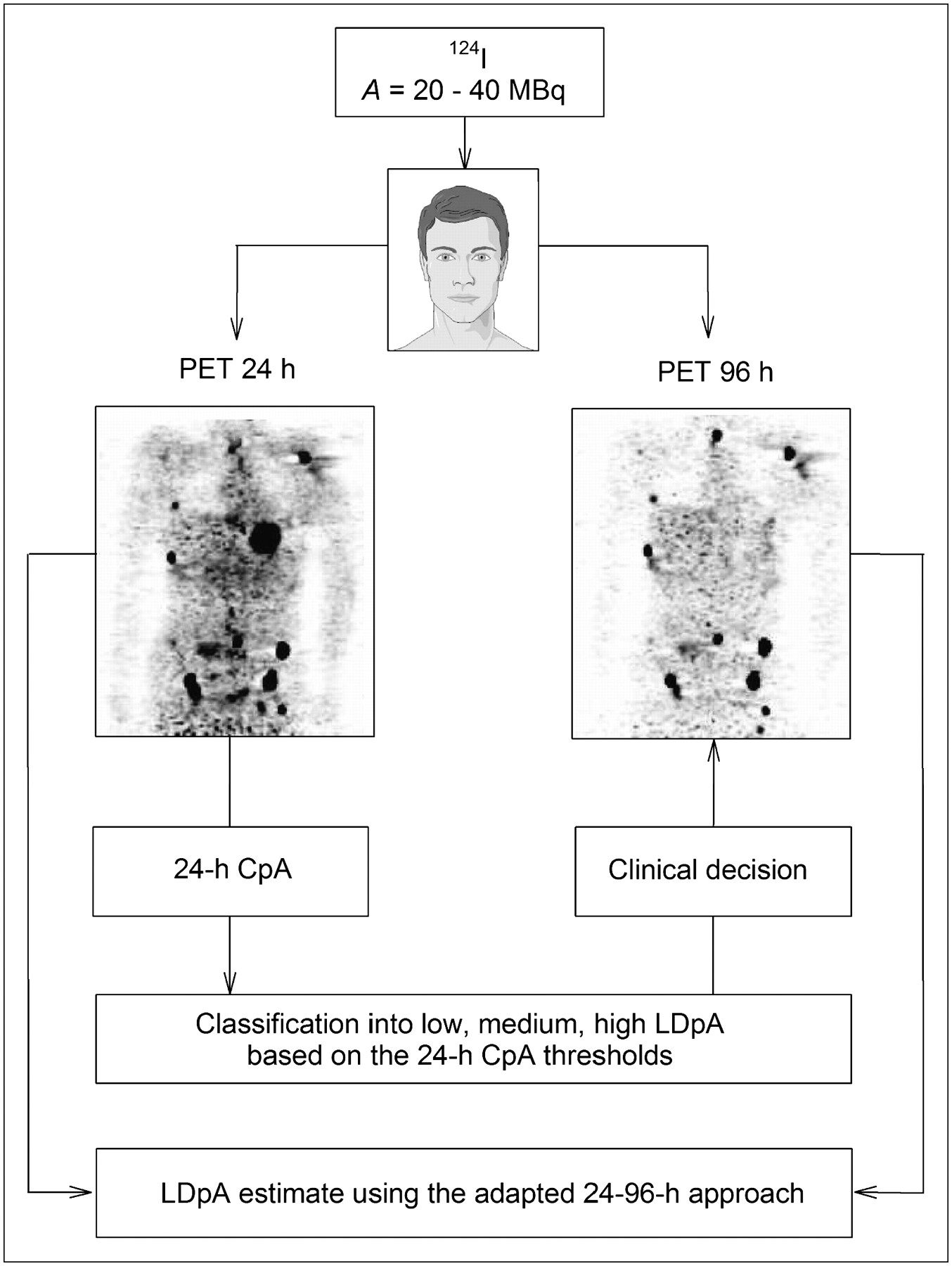
Flow chart illustrating optimized dosimetry protocol using adapted 24-96-h approach for patients with DTC undergoing 124I PET before planned radioiodine therapy. Clinical decision to perform 96-h measurement depends on LDpA classification; that is, low 24-h CpA indicates that radioiodine therapy is likely to fail.
CONCLUSION
Radioiodine kinetics and, hence, LDpA of DTC metastases showed great variability. For that reason, multiple 124I PET investigations are required. The 5-point protocol is certainly the most accurate among the approaches investigated, but the adapted 24-96-h approach using 2 points is an optimal dosimetry protocol when the clinical workload is particularly heavy, reducing logistical and time demands for patients and caregivers and clinical costs.
Acknowledgments
We are indebted to Robert J. Marlowe for critically reviewing the manuscript and for providing substantive scientific critique. We thank Dr. Annette Böckenhoff for her suggestions and guidance in the statistical analysis.
Footnotes
-
COPYRIGHT © 2008 by the Society of Nuclear Medicine, Inc.
References
- Received for publication September 10, 2007.
- Accepted for publication February 1, 2008.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- In Vivo Intralesional Positronium Lifetime Imaging of Thyroid Cancer Using Clinically Routine I-124 PET/CT
- Safety and Efficacy of Para-Aminohippurate Coinfusion for Renal Protection During Peptide Receptor Radiotherapy in Patients with Neuroendocrine Tumors
- Efficacy and Safety of 124I-MIBG Dosimetry-Guided High-Activity 131I-MIBG Therapy of Advanced Pheochromocytoma or Neuroblastoma
- Diagnostic Performance of 124I-Metaiodobenzylguanidine PET/CT in Patients with Pheochromocytoma
- Single-Time-Point Tumor Dosimetry Assuming Normal Distribution of Tumor Kinetics
- Dosimetry in Clinical Radiopharmaceutical Therapy of Cancer: Practicality Versus Perfection in Current Practice
- Appropriate Use Criteria for Nuclear Medicine in the Evaluation and Treatment of Differentiated Thyroid Cancer
- Individualized Dosimetry for Theranostics: Necessary, Nice to Have, or Counterproductive?
- Iodine Symporter Targeting with 124I/131I Theranostics
- Comparison of Empiric Versus Whole-Body/-Blood Clearance Dosimetry-Based Approach to Radioactive Iodine Treatment in Patients with Metastases from Differentiated Thyroid Cancer
- 124I PET Assessment of Response of Bone Metastases to Initial Radioiodine Treatment of Differentiated Thyroid Cancer
- High Level of Agreement Between Pretherapeutic 124I PET and Intratherapeutic 131I Imaging in Detecting Iodine-Positive Thyroid Cancer Metastases
- Dose-Response Relationship in Differentiated Thyroid Cancer Patients Undergoing Radioiodine Treatment Assessed by Means of 124I PET/CT
- Quantitative Comparison of 124I PET/CT and 131I SPECT/CT Detectability
- Assessment of Simplified Blood Dose Protocols for the Estimation of the Maximum Tolerable Activity in Thyroid Cancer Patients Undergoing Radioiodine Therapy Using 124I
- Assessment of Lesion Response in the Initial Radioiodine Treatment of Differentiated Thyroid Cancer Using 124I PET Imaging
- Dosimetry and thyroid cancer: the individual dosage of radioiodine
- Identification of a Shine-Through Artifact in the Trachea with 124I PET/CT