


Abstract
Radioiodine therapy with 131I is used for treatment of suspected recurrence of differentiated thyroid carcinoma. Pretherapeutic 124I PET/CT with a low activity (∼1% of 131I activity) can be performed to determine whether uptake of 131I, and thereby the desired therapeutic effect, may be expected. However, false-negative 124I PET/CT results as compared with posttherapeutic 131I SPECT/CT have been reported by several groups. The purpose of this study was to investigate whether the reported discrepancies may be ascribed to a difference in lesion detectability between 124I PET/CT and 131I SPECT/CT and, hence, whether the administered 124I activity is sufficient to achieve equal detectability. Methods: Phantom measurements were performed using the National Electrical Manufacturers Association 2007 image-quality phantom. As a measure of detectability, the contrast-to-noise ratio was calculated. The 124I activity was expressed as the percentage of 131I activity required to achieve the same contrast-to-noise ratio. This metric was defined as the detectability equivalence percentage (DEP). Results: Because lower DEPs were obtained for smaller spheres, a relatively low 124I activity was sufficient to achieve similar lesion detectability between 124I PET/CT and 131I SPECT/CT. DEP was 1.5%, 1.9%, 1.9%, 4.4%, 9.0%, and 16.2% for spheres with diameters of 10, 13, 17, 18, 25, and 37 mm, respectively, for attenuation- and scatter-corrected SPECT versus point-spread function (PSF) model–based and time-of-flight (TOF) PET. For no-PSF no-TOF PET, DEP was 3.6%, 2.1%, 3.5%, 7.8%, 15.1%, and 23.3%, respectively. Conclusion: A relatively low 124I activity of 74 MBq (∼1% of 131I activity) is sufficient to achieve similar lesion detectability between 124I PSF TOF PET/CT and 131I SPECT/CT for small spheres (≤10 mm), since the reported DEPs are close to 1%. False-negative 124I PET/CT results as compared with posttherapeutic 131I SPECT/CT may be ascribed to differences in detectability for large lesions (>10 mm) and for no-PSF no-TOF PET, since DEPs are greater than 1%. On the basis of DEPs of 3.5% for lesion diameters of up to 17 mm on no-PSF no-TOF PET, 124I activities as high as 170 MBq may be warranted to obtain equal detectability.
After resection for differentiated thyroid carcinoma, 131I is used as primary treatment to ablate remnant thyroid tissue and potential residual tumor tissue. Treatment with 5.5–7.4 GBq of 131I is indicated if metastases are suspected (1). The administered 131I activity is generally empiric and non–patient-specific, since the uptake and hence the therapeutic effectiveness of radioiodine in metastatic lesions is usually not known beforehand. Posttherapeutic 131I SPECT/CT or whole-body scintigraphy is routinely performed to assess tumor uptake. Up to 50% of empirically treated patients show no uptake on posttherapeutic imaging (2). To predict whether uptake of radioiodine, and hence a desired therapeutic effect, may be expected, pretherapeutic imaging with a low activity is performed.
Several pretherapeutic imaging strategies have been suggested to optimize patient-specific treatment activity and to prevent unnecessary 131I therapy. 131I whole-body scintigraphy with a low, nontherapeutic 131I activity (half-life, 8 d) can be used for pretherapeutic imaging (3). However, diagnostic low-activity 131I scintigraphy does not adequately predict the results of posttherapeutic high-activity 131I scintigraphy (4). Moreover, septal penetration by the high-energy (364 and 637 keV) γ-photons negatively affects the image quality of 131I SPECT and scintigraphy, making 131I less suitable for diagnostic purposes. The medium-energy (159 keV) γ-emitter 123I has also been suggested for pretherapeutic imaging, and studies investigating the potential of 123I yielded good results (5). However, because of the short half-life of 123I (13.2 h), a large fraction of the administered activity has already decayed before uptake maximizes and imaging is performed.
Alternatively, 124I, with a half-life of 4.2 d, has been proposed for pretherapeutic imaging and assessment of treatment response. Several groups have reported promising results using 124I as a diagnostic agent (6,7). 124I is a positron emitter and can be imaged using PET, with resolution, sensitivity, and quantitation superior to those obtainable with the use of 131I in scintigraphy or SPECT. Relatively low activities of 20–74 MBq are used for diagnostic 124I PET imaging (8–13).
Unfortunately, clinical experience has shown that 124I PET/CT does not always predict uptake of 131I reliably, and discrepancies between posttherapeutic 131I SPECT/CT and pretherapeutic 124I PET/CT have been reported by several groups (8–13). More specifically, in some cases 124I PET/CT images showed no uptake whereas 131I SPECT/CT images did. An example from a study we performed (unpublished data, 2013) is shown in Figure 1 (14). These false-negative 124I PET/CT results as compared with 131I SPECT/CT may be ascribed to a difference in lesion detectability between 124I PET/CT and 131I SPECT/CT.

Two example THYROPET patients (14) in whom 124I PET/CT was false-negative as compared with 131I SPECT/CT. In first patient, 124I PET/CT (A and C) was performed at 2 min per bed position 24 h after oral administration of 74 MBq of 124I using Gemini (Philips) and line-of-response row-action maximum-likelihood reconstruction without TOF correction (no-PSF no-TOF); in second, 131I SPECT/CT (B and D) was performed in 21 min 7 d after oral administration of 7,400 MBq of 131I using Symbia T2 (Siemens) and fast low-angle shot 3-dimensional attenuation-corrected reconstruction (no-SC 6i8s). Arrows indicate metastatic lesions.
The purpose of this study was to investigate whether the reported discrepancies may be ascribed to a difference in lesion detectability between 124I PET/CT and 131I SPECT/CT and, hence, whether the administered 124I activity is sufficient to achieve equal detectability. This was done by establishing the 124I activity, expressed as percentage of 131I activity, at which the contrast-to-noise ratio (CNR) was equal for both modalities.
MATERIALS AND METHODS
Phantom
To compare lesion detectability on 131I SPECT/CT and 124I PET/CT images, acquisitions of the International Electrotechnical Commission–National Electrical Manufacturers Association 2007 phantom (PTW Freiburg GmbH) were performed with varying activities. The phantom is torso-shaped and has a lid holding refillable thin-walled spheres 10, 13, 17, 22, 28, and 37 mm in diameter. Separate phantoms were used for the 124I and 131I experiments. The phantoms were filled only once, and different activity concentrations were obtained by leaving the activity to decay. This approach decreases measurement errors in comparison with refilling the phantom. Two phantoms were used for detectability analysis; one with activity in the background compartment and one without.
Clinically, large variations may occur in lesion-to-background ratios. Rubello et al. measured the lesion-to-background ratio with a γ-probe during radioguided surgery and obtained a mean lesion-to-background ratio of 11.4 (15). Therefore, we used 2 phantoms with different background concentrations to capture both extremities: no background (1:0) and a high background concentration (10:1). The activity in the spheres ranged from 1.8 × 104 to 4.6 Bq/mL for 124I and from 9.1 × 105 to 3.9 × 102 Bq/mL for 131I. The initial activities are shown in Supplemental Table 1 (supplemental materials are available at http://jnm.snmjournals.org). The activity in the phantoms was chosen such that it could be used to effectively compare lesion detectability in the range around the expected minimum detectable activity (MDA). In total, 45 124I PET studies were performed over 50 d, and 42 131I SPECT studies were performed over 90 d.
Scanners and Acquisitions
A Biograph mCT time-of-flight (TOF) PET/CT scanner (Siemens Healthcare) with TrueV (axial field of view, 21.6 cm) was used to acquire PET data. 124I images were acquired using a 435- to 650-keV energy window at 4 min per bed position, in accordance with the clinical protocol (14). Three bed positions were used to ensure that sensitivity was uniform along the entire length of the phantom in the axial direction.
A dual-head Symbia T16 SPECT/CT system (Siemens Healthcare) was used to acquire SPECT data. The BiCore high-energy collimator (Siemens Healthcare) that was used has 8,000 holes, a hole length of 59.7 mm, a hole diameter of 4.0 mm, and septal thickness of 2.0 mm. For all 131I acquisitions, 128 projections were acquired on a 128 × 128 grid with a 4.8 × 4.8 mm pixel size. In accordance with the clinical protocol, a 25-s acquisition time per view was used, resulting in a total acquisition time of 26 min.
Reconstruction
PET images were reconstructed to create 200 × 200 × 316 voxel images with a 4.07 × 4.07 × 1.50 mm voxel size. The reconstruction incorporated a 124I prompt γ-correction (16) and a randoms correction by adding the gaussian-filtered randoms-sinogram to the forward projection during the iterative reconstruction (17). Two reconstruction methods were used to obtain PET images.
The first method was ordered-subset expectation maximization 3-dimensional reconstruction incorporating TOF information (TrueX) with point-spread function (PSF) model–based resolution recovery and CT-based attenuation and scatter correction, using 4 iterations and 21 subsets in accordance with the clinical protocol. A gaussian postreconstruction filter was applied with a full width at half maximum of 5 mm. This method will be referred to as the PSF TOF method.
The second method was ordered-subset expectation maximization 3-dimensional reconstruction with attenuation correction, scatter correction, no TOF modeling, and no PSF model–based resolution recovery. As advised by the vendor, 4 iterations and 24 subsets were used and a gaussian postreconstruction filter was applied with a full width at half maximum of 5 mm. This reconstruction method will be referred to as the no-PSF no-TOF method.
SPECT images were reconstructed to create 128 × 128 × 80 voxel images with a 4.8 × 4.8 × 4.8 mm voxel size. The Siemens fast low-angle shot 3-dimensional reconstruction algorithm was applied, incorporating attenuation correction and resolution recovery using distance-dependent PSFs. Three reconstruction methods were used to obtain SPECT images. The first method used 6 iterations with 8 subsets and triple-energy-window scatter correction (SC 6i8s), the second method used 6 iterations with 8 subsets and did not incorporate scatter correction (no-SC 6i8s), and the third method used 30 iterations with 8 subsets and triple-energy-window scatter correction (SC 30i8s). Reconstruction with 6 iterations and 8 subsets was performed to allow comparison with the clinical trial running at our hospital (14), and reconstruction with 30 iterations and 8 subsets was included for increased contrast recovery at the cost of increased image noise (18,19).
Quantitative Analysis
Detectability Equivalence Percentage (DEP)
As a measure of detectability, we calculated CNR for each sphere using where CH is the mean voxel value in the sphere volume of interest (VOI), CB is the mean voxel value in the background VOI, and
where CH is the mean voxel value in the sphere volume of interest (VOI), CB is the mean voxel value in the background VOI, and  is the SD in the background VOI.
is the SD in the background VOI.
Three-dimensional VOI masks were created on the basis of the sphere coordinates determined from the coregistered CT image. The position of the spheres in the CT image was determined automatically using a Hough-transform–based circle detection method (20). The background VOI was defined as the entire phantom minus the sphere VOIs. To eliminate the influence of partial-volume effects on the background measurement, a 2-cm margin around the spheres and the phantom edges was subtracted from the background VOI by means of binary erosion.
To assess the difference in sphere detectability between 124I PET/CT and 131I SPECT/CT, 124I activity was expressed as the percentage of 131I activity required to achieve the same CNR. This metric was defined as DEP. For example, a DEP of 1% indicates that the same CNR is obtained on the 124I PET/CT image as on the 131I SPECT/CT image if the 124I activity is 1% of the 131I activity. For each sphere size and sphere-to-background ratio, DEP was determined by calculating the average ratio of the CNR curves (CNR vs. activity) for the 2 isotopes and multiplied by 100 to obtain a percentage. To reduce the influence of noise on the calculated DEPs, regression analysis of the curves was performed. Cubic spline fits of the activity as a function of the sphere CNR were performed and plotted in the log–log domain, because the range of the curves was several orders of magnitude. The mean ratios were calculated over the largest possible interval at which CNR data were acquired for both isotopes and in which CNRs were greater than 1. For the phantom without activity in the background compartment, CNRs for which the mean pixel value of the background VOI was less than 1 were not used for the regression analysis.
MDA
False-negative 124I PET/CT results as compared with 131I SPECT/CT occur when 124I is below MDA and 131I is above MDA. Therefore, MDA was calculated using the Rose criterion (21). The Rose criterion states that a lesion is no longer visible when the CNR of the lesion falls below a certain threshold, which can be used to determine the MDA. Because the Rose criterion has been validated for use in 2 dimensions only, we calculated the CNR of the (2-dimensional) central slice through the spheres. The detectability measure K2D was obtained by correcting CNR for lesion size according to where CNR2D is CNR in 2 dimensions, CH,2D is the mean voxel value in the 2-dimensional sphere region of interest (ROI), CB,2D is the mean voxel value in the 2-dimensional background region of interest, σB,2D is the SD in the 2-dimensional background region of interest, and N is the number of pixels in the lesion region of interest. A K2D threshold of 8 was used to determine MDA (22,23). MDA was defined as the activity at which the K2D-versus-activity curve intersected with the threshold. Regression analysis of the K2D-versus-activity curves with cubic splines was performed to reduce the influence of noise.
where CNR2D is CNR in 2 dimensions, CH,2D is the mean voxel value in the 2-dimensional sphere region of interest (ROI), CB,2D is the mean voxel value in the 2-dimensional background region of interest, σB,2D is the SD in the 2-dimensional background region of interest, and N is the number of pixels in the lesion region of interest. A K2D threshold of 8 was used to determine MDA (22,23). MDA was defined as the activity at which the K2D-versus-activity curve intersected with the threshold. Regression analysis of the K2D-versus-activity curves with cubic splines was performed to reduce the influence of noise.
RESULTS
Figures 2 and 3 show typical 124I PET/CT and 131I SPECT/CT National Electrical Manufacturers Association phantom images for different activities. The sphere CNR was calculated and plotted as a function of activity, as shown in Figure 4 and in Supplemental Figures 1 and 2 for the phantom with and without background activity, respectively. Defined as the average ratio between 124I and 131I activity to achieve the same CNR, DEP was calculated for each combination of PET and SPECT reconstruction methods and for each sphere size (Tables 1 and 2).
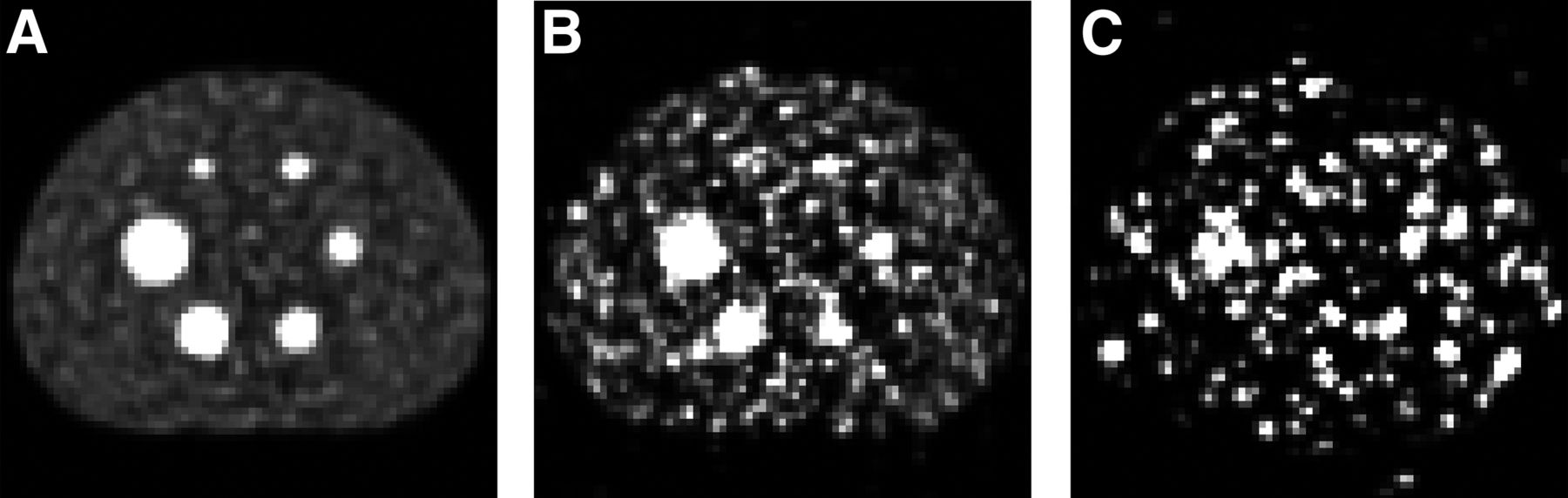
Typical 124I PET/CT images of phantom with activity in background compartment reconstructed using PSF TOF method showing central slice through spheres for 2.2 × 104 Bq/mL (A), 9.3 × 102 Bq/mL (B), and 6.5 × 101 Bq/mL (C). Maximum of gray scale is 5 times mean pixel value of image.
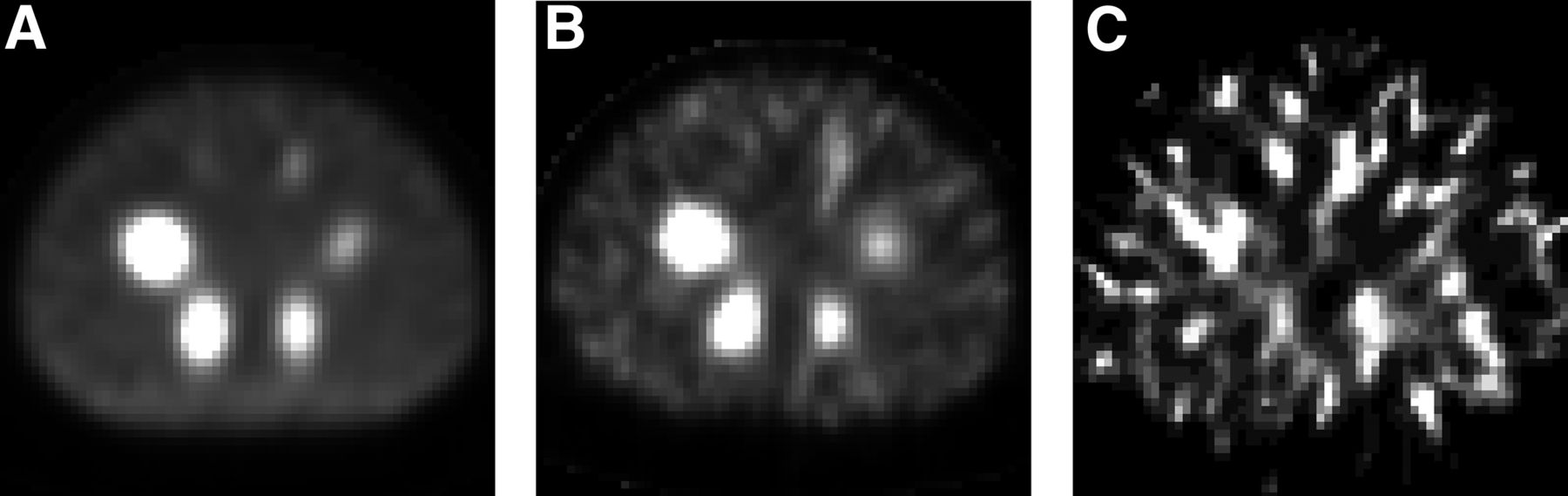
Typical 131I SPECT/CT images of phantom with activity in background compartment reconstructed using SC 6i8s method showing central slice through spheres for 9.1 × 105 Bq/mL (A), 4.5 × 104 Bq/mL (B), and 2.2 × 103 Bq/mL (C). Maximum of gray scale is 5 times mean pixel value of image.
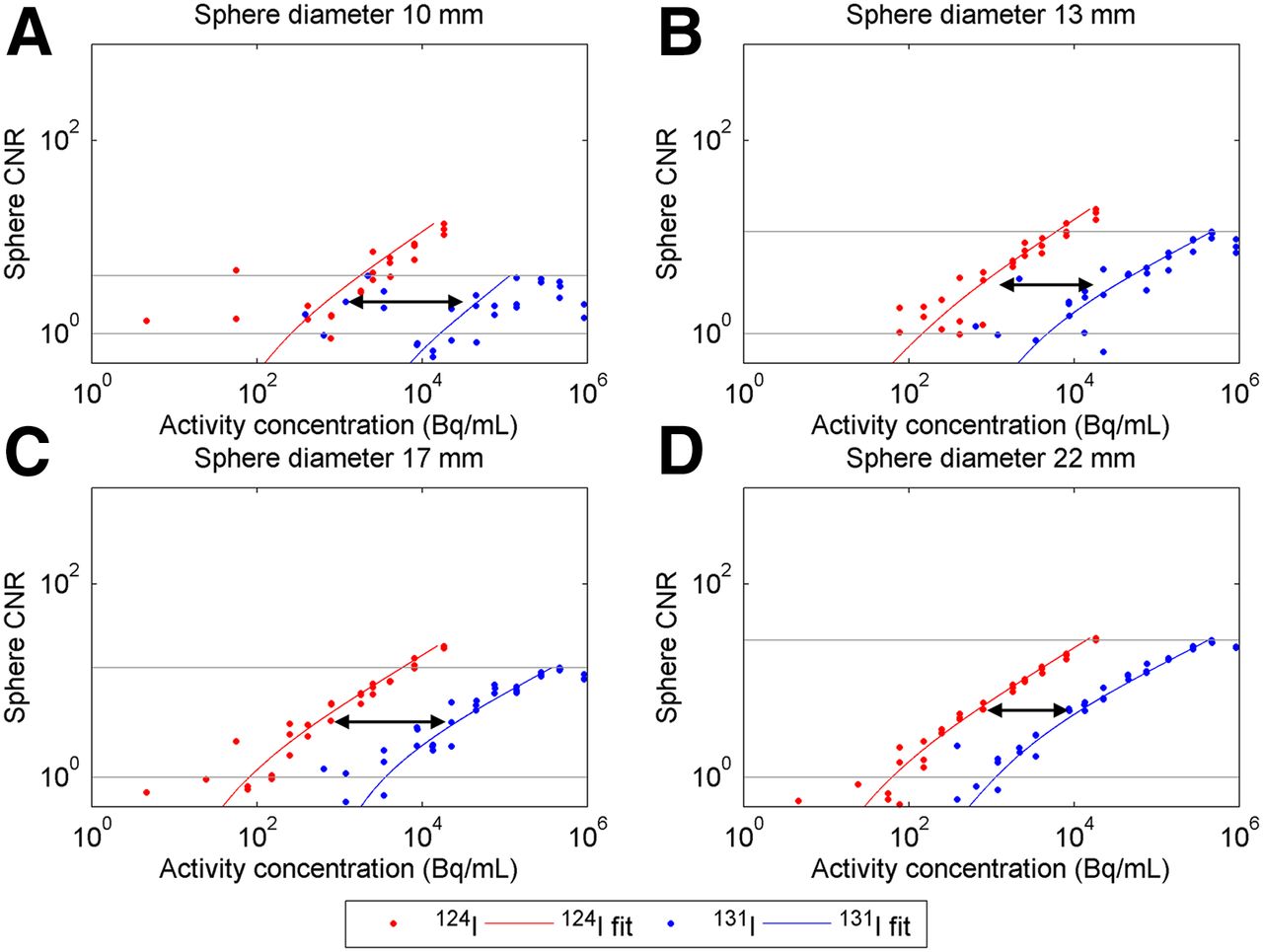
Sphere CNR as function of activity for 124I (red) and 131I (blue) phantom with background for spheres with diameters of 10 mm (A), 13 mm (B), 17 mm (C), and 22 mm (D). DEP is determined by calculating ratio of curves, which is graphically represented as horizontal shift of curves (arrows). Gray lines denote interval in which average ratio between curves was determined. Reconstruction was with PSF TOF for PET and SC 6i8s for SPECT.
DEPs for Phantom with Background
DEPs for Phantom Without Background
In general, because lower DEPs were obtained for smaller spheres, a relatively low 124I activity was sufficient to achieve similar lesion detectability between 124I PET/CT and 131I SPECT/CT. Furthermore, DEP depends on reconstruction method. DEP was higher for no-PSF no-TOF PET reconstruction than for PSF TOF reconstruction. Furthermore, DEP was slightly higher for SC 6i8s than for no-SC 6i8s and lower for SC 30i8s than for the other SPECT reconstruction methods. Differences in DEP between PSF TOF and no-PSF no-TOF reconstruction were smaller for the phantom without activity in the background compartment. In general, DEPs were slightly smaller for the phantom without activity in the background compartment.
Table 3 shows the MDA for the phantom with activity in the background compartment. The MDA of 124I was lower for PSF TOF reconstruction than for no-PSF no-TOF reconstruction. Similarly, for the 13- and 17-mm spheres, the MDA of 131I was lower for SC 6i8s than for no-SC 6i8s. However, for the 10-, 22-, and 28-mm spheres, the MDA of 131I was higher for SC 6i8s than for no-SC 6i8s. The MDAs of SC 30i8s were larger than for the other SPECT reconstruction methods.
MDAs for Phantom with Background
DISCUSSION
A relatively low 124I activity of 74 MBq (∼1% of 131I activity) was sufficient to achieve similar lesion detectability between 124I PSF TOF PET/CT and 131I SPECT/CT for small spheres (≤10 mm), since the reported DEPs were close to 1%. False-negative 124I PET/CT results as compared with posttherapeutic 131I SPECT/CT may be ascribed to differences in detectability for large lesions (>10 mm) and for no-PSF no-TOF PET since DEPs were greater than 1%.
The results showed that DEP was lower for smaller spheres, indicating that smaller spheres are relatively more easily detected on PET than on SPECT. This can be explained by the fact that the resolution of 124I PET images (∼5 mm) generally is higher than that of 131I SPECT images (∼15 mm). Therefore, differences in CNR are large in spheres that measure between 5 and 15 mm.
Activities frequently used in clinical practice and studies are 74 MBq of 124I and 7,400 MBq of 131I; thus, the administered 124I activity is approximately 1% of the administered 131I activity. However, because different scan delays are used after administration, it is necessary to correct for physical decay during the delay. The 124I PET and the 131I SPECT acquisitions are usually performed 24 h and 7 d after administration, respectively, so that at scanning time the 124I activity is approximately 1.5% of the 131I activity if we correct for physical decay. Tables 1 and 2 show that for some sphere sizes and reconstruction algorithms, DEP is less than 1.5%. Therefore, for small spheres (≤10 mm) on PSF TOF PET, a 74-MBq 124I activity is sufficient to achieve similar detectability between low-activity 124I PET/CT and high-activity 131I SPECT/CT. This shows that false-negative results on low-activity 124I PSF TOF PET/CT, as compared with posttherapeutic high-activity 131I SPECT/CT, are not likely caused by differences in the detectability of small lesions. A significant number of lesions seen in clinical practice are expected to be smaller than 10 mm (24). For larger lesions (>10 mm) and no-PSF no-TOF PET, DEP generally is greater than 1.5%, and a 74-MBq 124I activity is not sufficient to achieve similar detectability between low-activity 124I PET/CT and high-activity 131I SPECT/CT. Reported discrepancies, such as the example shown in Figure 1, may therefore be caused by differences in detectability.
The administered 124I activity is a factor that should be considered when our results are compared with those of other studies. Several clinical studies have been performed with 124I activities lower than 74 MBq (8,9,11). The probability of a false-negative 124I PET/CT result as compared with posttherapeutic 131I SPECT/CT considerably increases with lower 124I activities. When 25 MBq of 124I and 7,400 MBq of 131I are administered, the ratio of 124I to 131I activity is approximately 0.5% when corrected for physical decay. Since this is lower than the reported DEPs, discrepancies are more likely to occur as a result of differences in detectability.
An activity of 90 MBq is sufficient to achieve similar detectability for lesion diameters of up to 17 mm on PSF TOF PET, with DEPs up to 1.8%. On the basis of DEPs of 3.5% for lesion diameters of up to 17 mm on no-PSF no-TOF PET, 124I activities as high as 170 MBq may be warranted to obtain equal detectability. However, a limiting factor for high pretherapeutic activities may be thyroid stunning, although stunning due to 124I is controversial, and the origin and existence of stunning still are a hotly debated issue (25).
Discrepancies between 124I and 131I distribution in tissue as a consequence of differences in uptake and washout may be influenced by additional factors not assessed in this study. First, unlike phantoms, thyroid tumors or thyroid cancer metastases are inhomogeneous structures consisting of cancer cells, blood vessels, and connective tissue with different iodine concentrations, inducing partial-volume effects that may affect the measured contrast. Second, iodine uptake may be influenced by whether patients are prepared using thyroid hormone withdrawal or using recombinant human thyroid-stimulating hormone stimulation of iodine uptake. Third, cell damage as a consequence of delivered dose of activity may influence retention time and therefore cause differences in physiologic washout properties between 124I and 131I. Washout of 131I is expected to be faster in damaged cells (24). Fourth, the contrast of 131I lesions may increase when scanning is delayed: background activity may clear more quickly than tumor activity, and contrast in the images may therefore, contraintuitively, increase over time (10). In clinical practice, one of the few adjustable parameters that influence activity is the delay between administration and acquisition. However, the timing of the 131I SPECT/CT acquisition still is a matter of debate in the literature. In fact, Salvatori et al. stated that “perfect timing” probably does not exist because of differences in 131I kinetics in different patients and in different metastases (26). A delay of 7 d for this study was chosen to allow washout of background activity (27). Similar to 131I, 124I uptake differs significantly among metastases, although peak uptake is generally observed about 24 h after administration (28,29). Therefore, a delay of 24 h was used for the 124I PET/CT acquisition.
The purpose of this study was not to investigate the impact of physiologic factors but to quantitatively compare lesion detectability on 124I PET/CT and 131I SPECT/CT images. It may not be accurate to assume that physical decay is the only factor affecting the ratio of 124I to 131I activity, and interpretation of the results depends on this assumption. However, the measured DEPs do not depend on physiologic factors. To our knowledge, phantom measurements that compare the detectability of 124I and 131I quantitatively have not been published before.
CNR values lower than 1 were not used for the regression analysis and calculation of DEP. These values are inherently noisy because of the low number of counts. Furthermore, rounding errors occurred through conversion to the DICOM format when the mean voxel value in the background compartment was lower than 1. Consequently, for low activities in the phantom without background activity, SD in the background compartment was underestimated and CNR overestimated. Therefore, these data points (mean background VOI < 1) were not used to determine DEPs and MDAs.
Diagnostic 131I SPECT/CT with 37–150 MBq of 131I can also be performed for pretherapeutic imaging (3). However, this study showed that false-negative diagnostic scans as compared with posttherapeutic scans may be ascribed to the difference in administered activity and that false-negative results are likely, especially for smaller lesions with high MDAs.
False-negative 124I PET/CT results as compared with 131I SPECT/CT occur when 124I is below MDA and 131I is above MDA. The MDAs of 131I and 124I were therefore determined for the different reconstruction methods. The MDA of 131I was higher for SC 6i8s reconstruction than for no-SC 6i8s reconstruction for some sphere sizes (10, 22, and 28 mm). MDAs were not necessarily lower for images obtained with scatter correction, possibly because of the additional noise introduced in the reconstruction by the scatter projections. Unfortunately, no 131I MDAs could be obtained for the 37-mm spheres because not enough data were available for low CNRs.
DEPs were lower for 30i8s than for 6i8s SPECT reconstruction, because generally lower CNRs were obtained for 30i8s than for 6i8s. The cause was the increase in background noise with number of iterations, which lowered CNR. Therefore, the 124I activity expressed as a percentage of 131I activity required to achieve the same CNR (i.e., DEP) was lower for 30i8s than for 6i8s.
On the basis of the coregistered CT data, the sizes of the lesions in Figure 1 are 5 and 7 mm (Fig. 1B) and 12 mm (Fig. 1D). DEP for the 10-mm sphere was between 1.3 and 3.4, depending of the lesion-to-background ratio (Tables 1 and 2), so that a relatively low 124I activity of 74 MBq (∼1% of 131I activity) may not be sufficient to achieve similar detectability. The false-negative 124I PET/CT results as compared with 131I SPECT/CT may therefore be ascribed to differences in detectability. Unfortunately, no DEPs were calculated for sphere diameters smaller than 10 mm. In general, discrepancies between 124I PET/CT and 131I SPECT/CT depend on many factors, and this study showed that the dose of 124I activity should be chosen carefully.
CONCLUSION
A relatively low 124I activity of 74 MBq (∼1% of 131I activity) is sufficient to achieve similar lesion detectability between 124I PSF TOF PET/CT and 131I SPECT/CT for small spheres (≤10 mm), since the reported DEPs are close to 1%. A 124I activity of 90 MBq is sufficient to achieve similar detectability for lesion diameters of up to 17 mm on PSF TOF PET, with DEPs of up to 1.8%. False-negative 124I PET/CT results as compared with posttherapeutic high-activity 131I SPECT/CT may be ascribed to differences in detectability for large lesions (>10 mm) and for no-PSF no-TOF PET, since DEPs are greater than 1%. On the basis of DEPs of 3.5% for lesion diameters of up to 17 mm on no-PSF no-TOF PET, 124I activities as high as 170 MBq may be warranted to obtain equal detectability.
DISCLOSURE
The costs of publication of this article were defrayed in part by the payment of page charges. Therefore, and solely to indicate this fact, this article is hereby marked “advertisement” in accordance with 18 USC section 1734. No potential conflict of interest relevant to this article was reported.
Acknowledgments
We thank Dr. Dennis Brian Martin Dickerscheid for providing the phantom.
Footnotes
Published online Oct. 22, 2015.
- © 2016 by the Society of Nuclear Medicine and Molecular Imaging, Inc.
REFERENCES
- Received for publication June 30, 2015.
- Accepted for publication October 9, 2015.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Tumor Dose-Response Relationship of [131I]MIBG Therapy in Patients with Neural Crest Tumors by Means of [124I]MIBG PET
- Diagnostic Performance of 124I-Metaiodobenzylguanidine PET/CT in Patients with Pheochromocytoma
- 18F-NaF PET/CT of Obese Patients on a Lutetium-Yttrium Oxyorthosilicate PET/CT System: Patient Dosimetry, Optimization of Injected Activity, and Acquisition Time
- Technical Advances in Image Guidance of Radionuclide Therapy
- THYROPET Study: Is It Biology or Technology That Is the Issue?
- Reply: THYROPET Study: Is It Biology or Technology That Is the Issue?