


Abstract
Patients with mild cognitive impairment (MCI) represent a risk population for progressing to dementia of the Alzheimer type (DAT). However, clinical criteria do not ensure reliable individual prognosis in these patients. The objective of this longitudinal, prospective study was to examine the value of 18F-FDG PET of cerebral glucose metabolism and of genetic susceptibility, as defined by an APOEε4–positive genotype, with regard to the early diagnosis of DAT in patients with MCI. Methods: In 30 patients with the diagnosis of MCI (16 female, 14 male; age, 70 ± 8 y), baseline and follow-up examinations (mean observation period, 16 mo) were performed. In all patients, the APOE genotype was assessed and cerebral glucose metabolism was evaluated at baseline using cranial 18F-FDG PET. Individual PET data were screened for findings suggestive of Alzheimer’s disease (AD), with the help of an automated computer program. After stereotactical normalization of the PET images, this program performs an observer-independent statistical comparison with an age-matched reference database (n = 22). Results: In 43% of all MCI subjects, a PET scan suggestive of AD pathology according to our predefined criteria was observed at baseline (PET+); 57% of all MCI patients were carriers of the APOE ε4 allele (e4+). In 40% of all patients, progression of symptoms within the observation period justified the clinical diagnosis of probable DAT at the time of follow-up reevaluation. Statistical evaluation revealed the best results for PET with regard to early diagnosis of DAT in MCI patients (sensitivity, 92%; specificity, 89%). Classification according to the APOE genotype was significantly less successful (sensitivity, 75%; specificity, 56%). However, a combination of both diagnostic tests allowed early diagnosis with either very high specificity (PET+ AND e4+: sensitivity, 67%; specificity, 100%) or very high sensitivity (PET+ OR e4+: sensitivity, 100%; specificity, 44%). Conclusion: 18F-FDG PET of cerebral glucose metabolism is a valuable diagnostic tool for the prediction of clinical outcome in individual MCI patients. Results are superior to the exclusive assessment of the APOE genotype. A combination of both functional imaging and genotyping may allow an early high-risk or low-risk stratification of patients with either very high sensitivity or very high specificity. This may be valuable, for example, for patient selection in scientific studies.
Mild cognitive impairment (MCI) is used as a diagnostic classification concept for patients with a decline of cognitive performance, which is more pronounced than expected age-related changes but not sufficient for the diagnosis of dementia (1). Longitudinal studies have shown that a substantial proportion of MCI patients subsequently progress to dementia of the Alzheimer type (DAT) (2). Thus, MCI populations include a portion of patients with predementia Alzheimer’s disease (AD). The interest in prediction of prognosis is continuously increasing with emerging new therapeutic options (3, 4). However, in patients selected by clinical criteria alone, the clinical syndrome of MCI may be caused by many other underlying conditions, such as cerebrovascular disease or depression, so that the prognosis of individual MCI patients is highly variable (5).
Several diagnostic procedures have been suggested to improve the prediction of prognosis in MCI patients. 18F-FDG PET assessment of cerebral glucose metabolism is a measure of synaptic activity and can identify the presence and localization of neurodegenerative processes in the brain. It has been shown to be a valuable aid in the diagnosis of dementing disorders. Criteria have been established and validated for differential diagnosis of dementia and early detection of AD using PET (4, 6–11). Some studies have also been performed in patients with MCI, and characteristic abnormalities have even been found in healthy individuals who progressed to DAT later on (12–17). In a recent study by our group, characteristic abnormalities of baseline cerebral glucose metabolism have been detected in a group analysis of MCI patients who showed progression to DAT within 1 y (14). Therefore, it is evident that the analysis of metabolic abnormalities in patients with MCI could play an important role in the prediction of the clinical course and in the selection of patients with more uniform underlying pathology for targeted research projects, such as specific drug trials.
18F-FDG PET only captures one aspect of AD pathology in MCI patients. The prognostic accuracy may be increased by a combination of parameters that illuminate the disease process from different angles. In this context, it appears particularly promising to combine the results derived from functional imaging with diagnostic information on the predisposition for the disease. With regard to AD, the apolipoprotein E (APOE) ε4 allele has been identified as a major susceptibility gene. Homozygous and heterozygous carriers of the ε4 allele have an increased risk of progressing to DAT (18). In studies on the genetic predisposition of nonfamiliar AD, the APOE genotype has been shown to have a relatively high predictive value (19). However, less data have been collected on the contribution of genetic assessment to the diagnosis of AD at the stage of MCI. Generally, the exclusive assessment of the APOE genotype in the diagnosis of AD is expected to be limited because 50% of AD patients are ε4 negative and some carriers of the ε4 allele will never progress to DAT, even at a very old age (20). In a few studies the possible benefit of a combination of neuroimaging with genetic risk factors has been advocated (19–21). A very recent retrospective study explicitly encouraged the combination of 18F-FDG PET and APOE genotyping for the prediction of dementia in MCI patients (16).
Thus, the objective of the current prospective study was to determine the diagnostic value of 18F-FDG PET and the APOE genotype in patients with MCI with regard to the progression to DAT. Analysis was performed for each predictor separately and for a combination of both parameters. For analysis of the PET data, a well-established observer-independent program (NEUROSTAT; University of Michigan) was used to minimize observer bias.
MATERIALS AND METHODS
Inclusion and Exclusion Criteria
The study was set up in a prospective design. In a previous study of our group on MCI, we observed a conversion rate to DAT of 36% within 12 mo (14). On the basis of these results, we planned to recruit at least 30 patients according to comparable inclusion criteria to gather a reasonable number of converters (>10 patients). To be able to finish the entire study within a time period of 2 y, we defined a follow-up period of 15 mo.
Patients were recruited consecutively from the research unit for cognitive disorders at the Technical University of Munich, Munich, Germany. They were referred for diagnostic evaluation by general practitioners, neurologists, or psychiatrists or other institutions. The baseline diagnostic work-up included an interview with the patient and informant; medical, psychiatric, and neurologic examinations (performed by an experienced psychiatrist); routine blood screening; and APOE genotyping. Cranial MRI was performed to assess structural brain abnormalities and cranial 18F-FDG PET was used to determine cerebral metabolism.
Inclusion Criteria.
Participants had to meet the established diagnostic criteria for MCI, defined by Petersen et al., that have been evaluated in previous studies (22). These criteria include subjective complaints, performance of 1.5 or more SDs below the age norm on the Consortium to Establish a Registry for Alzheimer’s Disease (CERAD) delayed verbal recall test, a Clinical Dementia Rating (CDR) score of 0.5, and preserved basic activities of daily living (ADL) (23). Patients were included in the study after informed consent had been obtained.
Exclusion Criteria.
Patients were not included in the study if they met diagnostic criteria for manifest dementia or for any other functional psychiatric disorder, including major depression, or if they showed any characteristic symptoms of diseases or abnormalities sufficient to cause memory impairment, such as normal pressure hydrocephalus, Parkinson’s disease, or progressive supranuclear palsy. Patients were also excluded if they showed any major structural abnormalities or signs of major vascular pathology in MRI, such as status after infarction, extensive leucoencephalopathy or atrophy, intracerebral aneurysm or arteriovenous malformation. The National Institute of Neurological Disorders and Stroke–International Association for Research and Teaching in Neurosciences (NINDS–AIREN) criteria were used to exclude relevant ischemic processes causing cognitive impairment in the patients (24). Furthermore, other extracerebral causes possibly influencing neuropsychologic function, such as psychotropic medication (e.g., antidepressants, neuroleptics) or substance abuse, were excluded.
The aim of using these rather stringent inclusion and exclusion criteria was to ensure that neurodegeneration was the most probable underlying cause of cognitive decline in the selected population and, thus, to obtain a high conversion rate to DAT as demonstrated in a previous study of our group using these criteria (14).
Neuropsychologic Evaluation
All patients underwent neuropsychologic evaluation including the CERAD neuropsychologic battery (performed by an experienced neuropsychologist) (23, 25–27). For this study, a German version of the CERAD neuropsychologic battery was used for which normative data have been published (28). The CDR was used for analysis of the overall severity of cognitive impairment (29, 30). Performance on ADL was assessed.
Routine Blood Screening and APOE Genotype
Routine blood screening included a standard serologic chemistry group, full blood cell count, blood glucose, vitamin B12 and folic acid levels, thyroid hormone levels, as well as serologic tests for syphilis and Lyme borreliosis and revealed no major abnormalities. For determination of the APOE genotype, DNA was extracted according to standardized procedures and apolipoprotein polymorphism was assessed by a polymerase chain reaction–based assay, simultaneously using 2 distinct restriction enzymes, as described previously (31). For further analysis, subjects were divided in APOE ε4-allele carriers and noncarriers; all ε4-allele–positive subjects were pooled together, as done in previous studies (32, 33).
MRI
At the time of initial evaluation, structural MRI was performed on all patients to exclude major structural abnormalities or vascular lesions—that is, no cortical infarction, <25% white matter lesions and no lacunes in the basal ganglia. Patients underwent examination on a 1.5-T Magnetom Symphony (Siemens) scanner using a standardized imaging protocol consisting of axial T2-weighted turbo-spin-echo images (repetition time [TR], 4,510 ms; echo time [TE], 104 ms; 19 slices; voxel dimensions, 0.6 × 0.5 × 6.0 mm), coronal T1-weighted spin-echo images (TR, 527 ms; TE, 17 ms; 19 slices; voxel dimensions, 0.9 × 0.9 × 6.0 mm), and T2-weighted gradient-echo images (TR, 725 ms; TE, 29 ms; 19 slices; voxel dimensions, 0.7 × 0.7 × 6.0 mm).
18F-FDG PET
18F-FDG PET was performed at the time of initial clinical evaluation. All subjects received 370 MBq 18F-FDG at rest with the eyes closed. Subjects were positioned with the head parallel to the canthomeatal line within the gantry. Thirty minutes after injection, PET was performed under standard resting condition (eyes closed in dimmed ambient light) using a Siemens 951 R/31 PET scanner (CTI). A sequence of 3 frames of 10 min was started and later combined into a single frame. Image data were acquired in 2-dimensional mode with a total axial field of view of 10.5 cm and no interplane gap space. Attenuation correction was performed by a standard ellipse-fitting method.
Image Analysis
For image analysis, a Sun workstation (Sun Microsystems Inc.) was used. Automated analysis of the 18F-FDG PET images was performed using a standard diagnostic routine (NEUROSTAT) in our laboratory. This method has been described previously in detail and has been evaluated for clinical and scientific use in patients with dementia and other cerebral disorders (34–37).
Briefly, rotational correction and centering of the dataset were performed in 3 dimensions, followed by realignment to the anterior commissure–posterior commissure line. To adjust the individual’s brain to the proportional grid system, proposed by Talairach and Tournoux, linear scaling and nonlinear warping of the data were performed, resulting in a standardized image set with a uniform voxel size of 2.25 mm (38).
Subsequently, the individual normalized brain activity of each patient was compared with a reference normal database consisting of 22 age-matched healthy control subjects by means of a z score. PET scans in the group of healthy volunteers had been performed on the same scanner and under the same conditions as those used for the patients. z scores were calculated pixel by pixel. A high, local z score represents a reduced local glucose metabolism in the patient relative to the control mean. A z-score threshold of >1.64 (1 tail) corresponding to a P value of 0.05 (1 tail) was applied for demarcation of significant abnormalities. This statistical threshold previously proved to be suitable for the diagnosis of DAT using the applied statistical tool (34, 35). Three-dimensional stereotactic surface projections (3D-SSP) of the z scores were then generated to allow visualization of abnormalities.
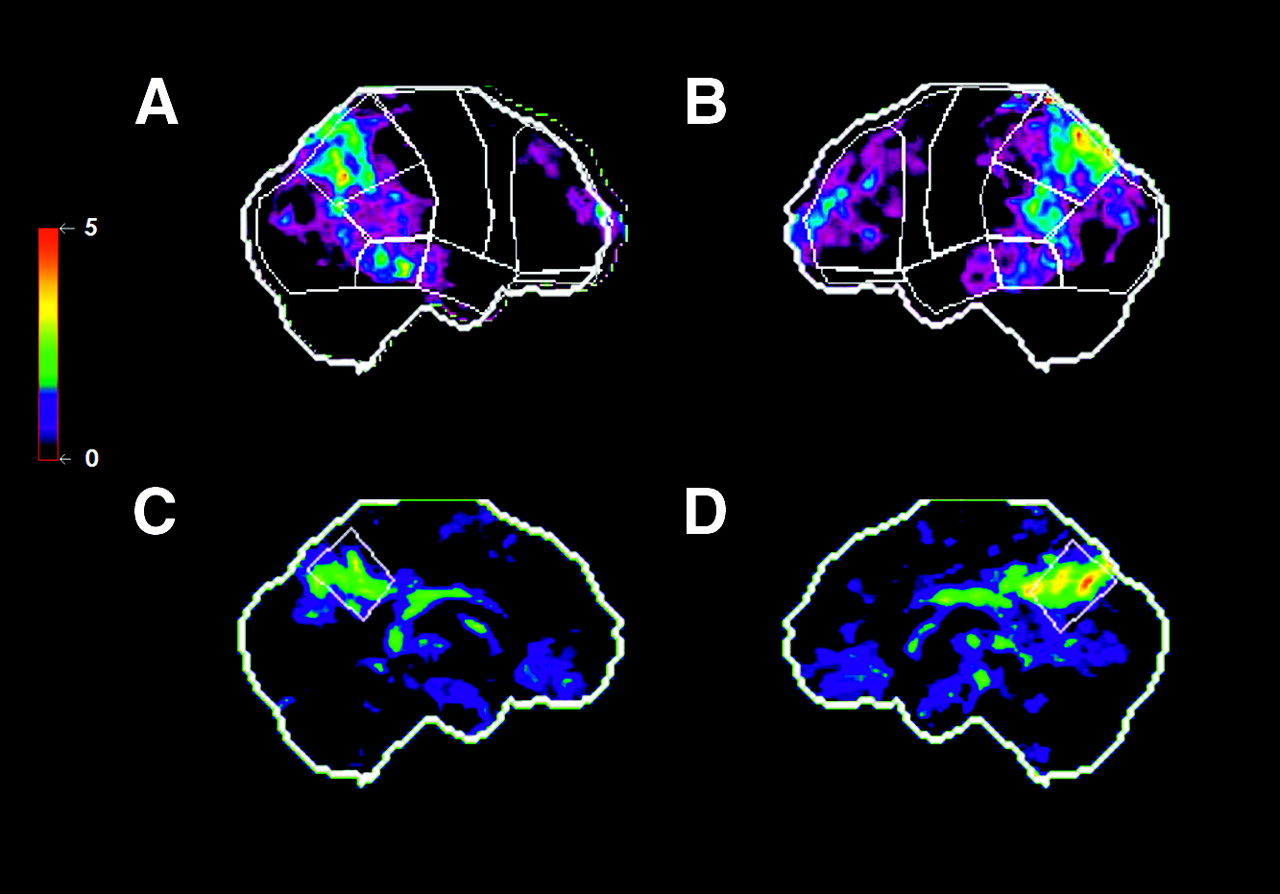
A predefined set of 20 surface regions of interest (ROIs) was then placed automatically onto the 3D-SSP z-score images, covering the entire brain. The ROIs were defined to reflect functional divisions of the cerebral lobes, and each hemisphere was divided into the following regions: orbitofrontal, prefrontal, premotor, central, parietal superior and inferior, occipital, temporal anterior, temporal posterior, and posterior cingulate (Fig. 1). The results from the ROI analysis were not averaged together; each ROI was assessed individually. As demonstrated previously, this approach allowed observer-independent attachment of significant regional hypometabolism to predefined brain regions (36, 39). With this automated routine, the significance of cerebral metabolic deviations could be examined using the z score and the extent of the abnormalities could be assessed via the number of affected cortical regions.
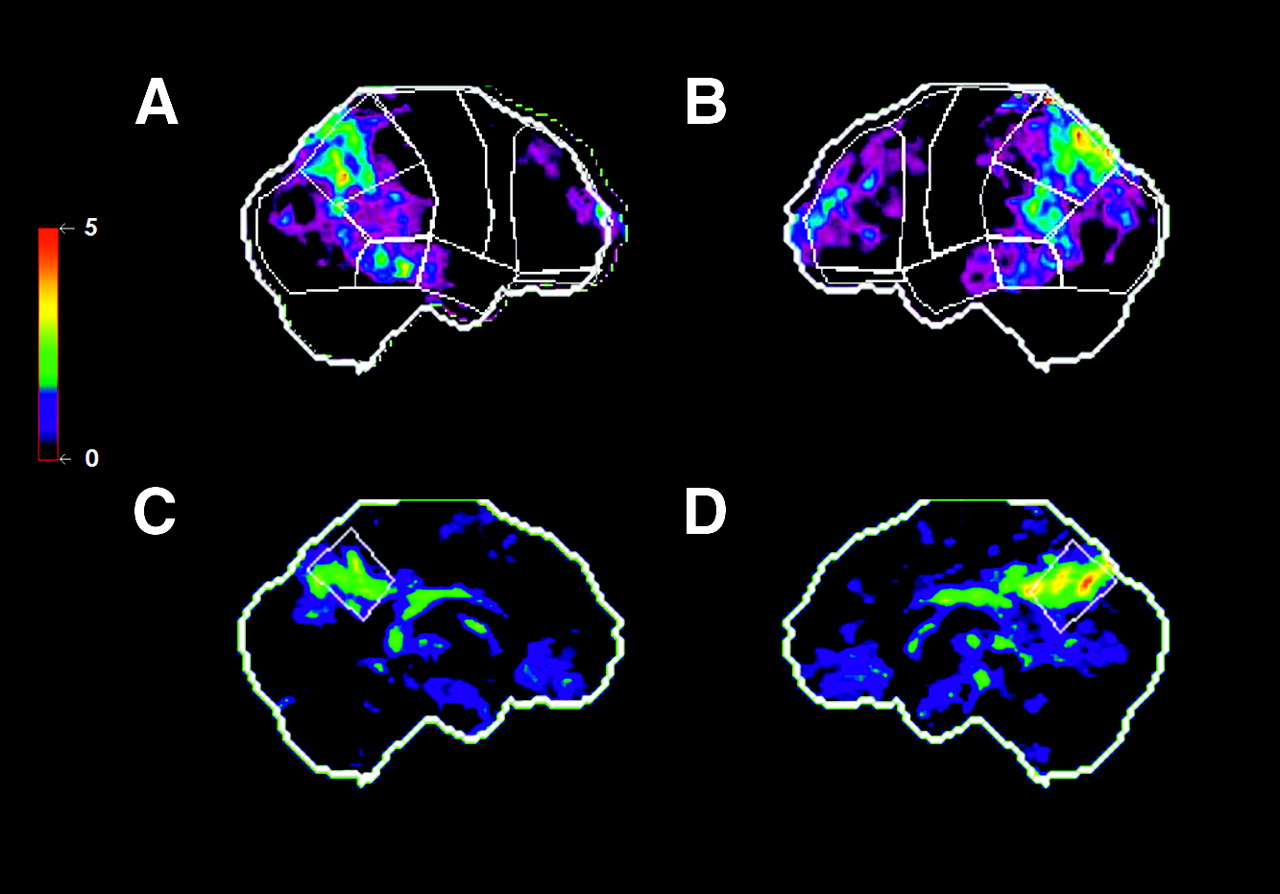
Baseline 18F-FDG PET findings in MCI patient who showed clinical progression to DAT within 16 mo. Surface projections of statistical abnormalities (z scores) as compared with healthy control population are displayed. Predefined anatomic surface ROIs are depicted in white color. Significant hypometabolism in bilateral temporoparietal and frontal cortex and in the posterior cingulate cortex is apparent. (A) Right lateral. (B) Left lateral. (C) Left medial. (D) Right medial.
Classification of PET Findings
In a previous study, we performed a group analysis of cerebral glucose metabolism in MCI patients who had been selected according to criteria similar to those used in the current study. In this analysis, characteristic abnormalities of cerebral glucose metabolism were detected already at the baseline PET examination in the group of MCI patients who showed conversion to DAT within 12 mo. Affected areas included brain regions typically involved in AD, such as bilateral para/hippocampal cortex, inferior prefrontal cortex, temporal cortex, inferior parietal cortex, and posterior cingulate cortex. Similar key regions for differential diagnosis and early detection of dementia using PET have been established in several other studies on diagnostic criteria (6–11,16). Particularly, the posterior cingulate cortex has been discussed as showing early abnormalities in AD. On this background, individual MCI patients were systematically screened for typical abnormalities using the NEUROSTAT automated image analysis procedure. The detection of significant hypometabolism (as compared with a control population) in surface ROIs covering the posterior cingulate cortex accompanied by cortical hypometabolism in at least unilateral temporoparietal areas was determined as suggestive of early AD, based on findings of earlier studies (14). According to this strategy, PET baseline results were classified as suggestive or not suggestive for AD, blinded for the later outcome of the patients and blinded for other clinical baseline information.
Follow-Up Assessment
To be able to finish the entire study within 2 y, we planned to perform the follow-up examination at 15 mo after initial diagnostic assessment. We tried to establish a tight personal relationship of patients with the research center and the responsible physician to ensure good compliance with regard to the readmission for follow-up examination. If patients did not show up independently, they were actively contacted. In the follow-up examination, the complete diagnostic work-up—including an interview with the patient and an informant; medical, psychiatric, and neurologic examinations; and the battery of neuropsychologic examinations—was repeated. No additional clinical evaluation of the patients was performed between baseline and follow-up examination. Impairment of cognitive performance and a decline in performance of ADL resulting in a CDR score of ≥1 were used as a measure for progression to manifest dementia. The diagnosis of probable DAT was established according to previously defined criteria (40). All physicians involved in the clinical diagnosis were unaware of the PET results and the APOE genotype of the patients to avoid any observer bias.
Statistical Evaluation
For statistical evaluation of the data, we performed a receiver-operating-characteristic analysis (ROC analysis). We calculated sensitivity, specificity, accuracy, and corresponding confidence intervals (CI) for each of the methods (APOE genotype assessment and PET) relating to the emergence of DAT in MCI. With regard to the prospective approach of the study, we also calculated positive and negative predictive values (PPV and NPV, respectively) for both tests. A χ2 test was used to assess differences in distribution of categoric attributes such as age and sex. In a previous study, the combined use of APOE genotyping and PET for prediction in MCI has been advocated (16). Thus, we separately evaluated 2 different combined applications of the tests to assess the potential additional value of a combined diagnostic strategy: (a) PET AND APOE: Only subjects with AD-suggestive PET findings and ε4–positive APOE genotype were classified as test positive. Subjects without suspect findings or with suspect findings in 1 test only, were classified as test negative. (b) PET OR APOE: All subjects with a suspect finding in either one of the tests (PET positive or ε4–positive APOE genotype) were regarded as test positive (including subjects with positive findings in both tests). Only subjects with inconspicuous findings in both PET and genotype assessment were classified as test negative.
RESULTS
Patient Characteristics at Baseline
On the basis of the inclusion and exclusion criteria, 30 individuals (16 female, 14 male) were included in the study. The mean age at baseline examination was 70 ± 8 y and the mean age at onset of memory problems was 68 ± 8 y. This resulted in a mean duration of symptoms of 2.6 ± 2 y. The mean time of formal education was 11.6 ± 3.4 y. Formal education was defined as years of school attendance plus years of apprenticeship, technical school, college, and university (Table 1).
Characteristics of MCI Patients (n = 30)
All participating individuals complained of memory problems of gradual onset at initial evaluation. Some patients mentioned additional minor problems with language, such as word-finding difficulties. Slight problems in time orientation and subtle insecurities with orientation in new surroundings were also reported.
All patients had a memory performance of at least 1.5 SDs below their age norm on the CERAD neuropsychologic delayed verbal recall test and a CDR score of 0.5 (as required by the inclusion criteria). Most subjects also showed subnormal results in other memory-related tasks, including immediate verbal recall and delayed verbal recognition. Delayed nonverbal recall, however, was within normal limits in most patients. The mean score on the Mini-Mental State Examination (MMSE) at baseline was 26.9 ± 1.9 points, with the majority scoring >1.5 SDs below their cognitively healthy age-matched peers. According to the definition of subtypes of MCI of Petersen et al., 25 patients fulfilled criteria of a “multiple domains” type of MCI, generally including memory deficits, and 5 patients showed isolated memory impairment corresponding to an “amnestic type” of MCI (41). No patients with a single “nonmemory domain type” of MCI were included in the study.
Neuropsychologic Reevaluation
As a consequence of the preestablished tight relationship of patients with the research center and the relatively small number of patients overall, no dropouts occurred. No patients died within the observation period. However, some patients had to be actively contacted for the follow-up examination; thus, the observation period showed some variation and the originally planned follow-up period of 15 mo expanded to a mean of 16 ± 2 mo.
In 12 (40%) participants, deterioration of clinical symptoms justified the clinical diagnosis of DAT at the time of follow-up examination. In 18 of the 30 MCI patients (60%), the diagnostic status at the follow-up examination revealed minor or no changes; thus, they still were diagnosed as MCI. Patients who progressed from MCI to DAT were slightly older than patients whose diagnostic status did not change; however, they showed no significant difference with regard to educational level. The duration of symptoms did not differ between the groups. The mean MMSE at baseline was significantly lower in the progressive group compared with nonprogressive patients; furthermore, progressive patients showed a significant decline of the MMSE value within the follow-up period. A χ2 test revealed no significant difference in the distribution of male and female patients in the 2 groups (Table 1). At the baseline evaluation, 9 of the 12 progressive patients were classified as a having the multiple domains subtype of MCI and 3 were classified as having the amnestic type of MCI. In the group of the 18 clinically stable patients, 16 patients fulfilled criteria of a multiple domains subtype and 2 patients had the amnestic type.
APOE Genotype
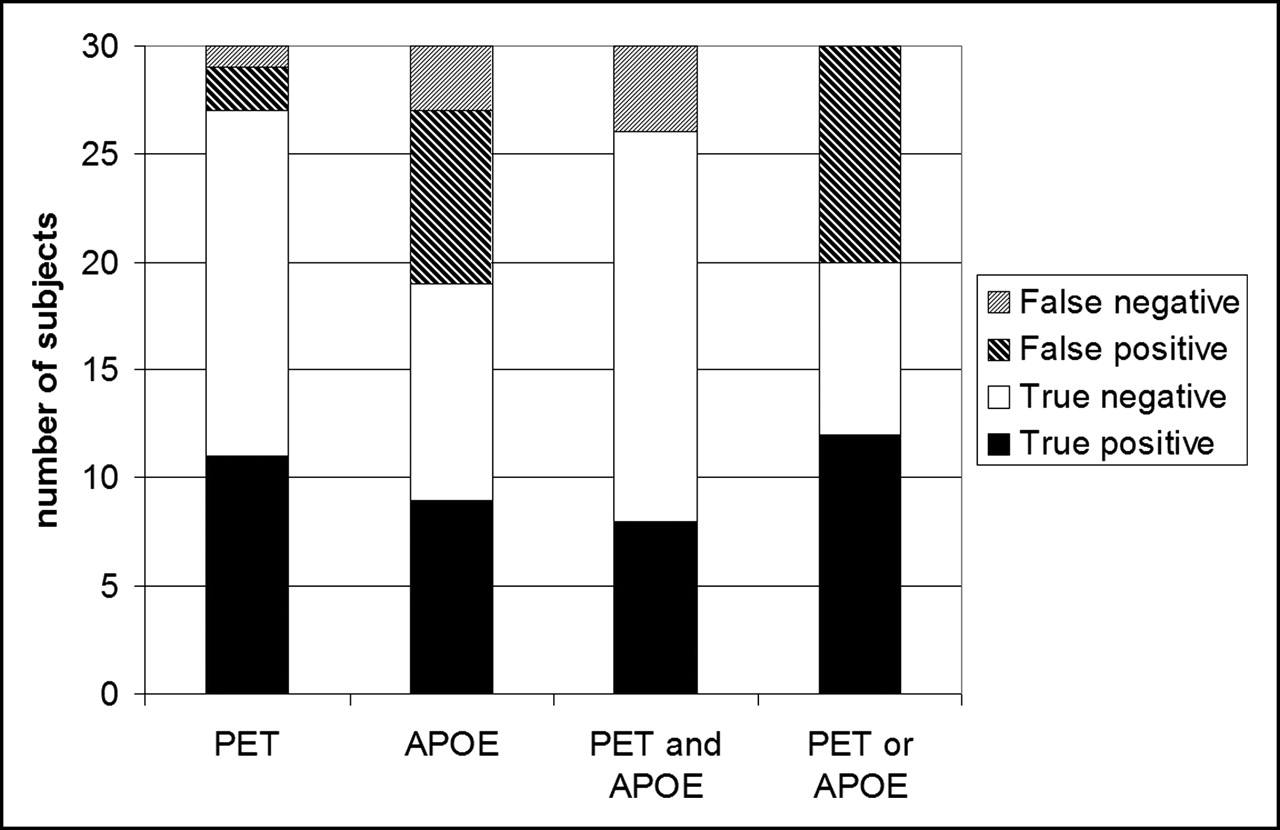
Analysis of the APOE genotype at baseline revealed that 17 (57%) of all MCI patients were carriers of the APOE ε4 allele (APOE ε4 positive). Four of these patients (13%) were homozygous for the ε4 allele. Thirteen (43%) of all MCI patients did not carry a copy of the ε4 allele (APOE ε4 negative). In 9 of the 17 APOE ε4–positive patients, progression to clinical DAT was documented within the observation period. Three of the 4 homozygous ε4 carriers showed progression to DAT. In contrast, 10 of the 13 APOE ε4–negative patients remained clinically stable (Fig. 2). The statistical evaluation revealed a sensitivity of 75% (95% CI, 43–94), a specificity of 56% (CI, 31–79), and a test accuracy of 63%. A PPV of 53% and a NPV of 77% were calculated for APOE genotype (homo- and heterozygous) with regard to the emergence of DAT in the MCI patients studied (Table 2; Fig. 3). A χ2 test revealed no significant difference in the distribution of ε4–positive and ε4–negative genotype on progressive and nonprogressive patients (Table 1).
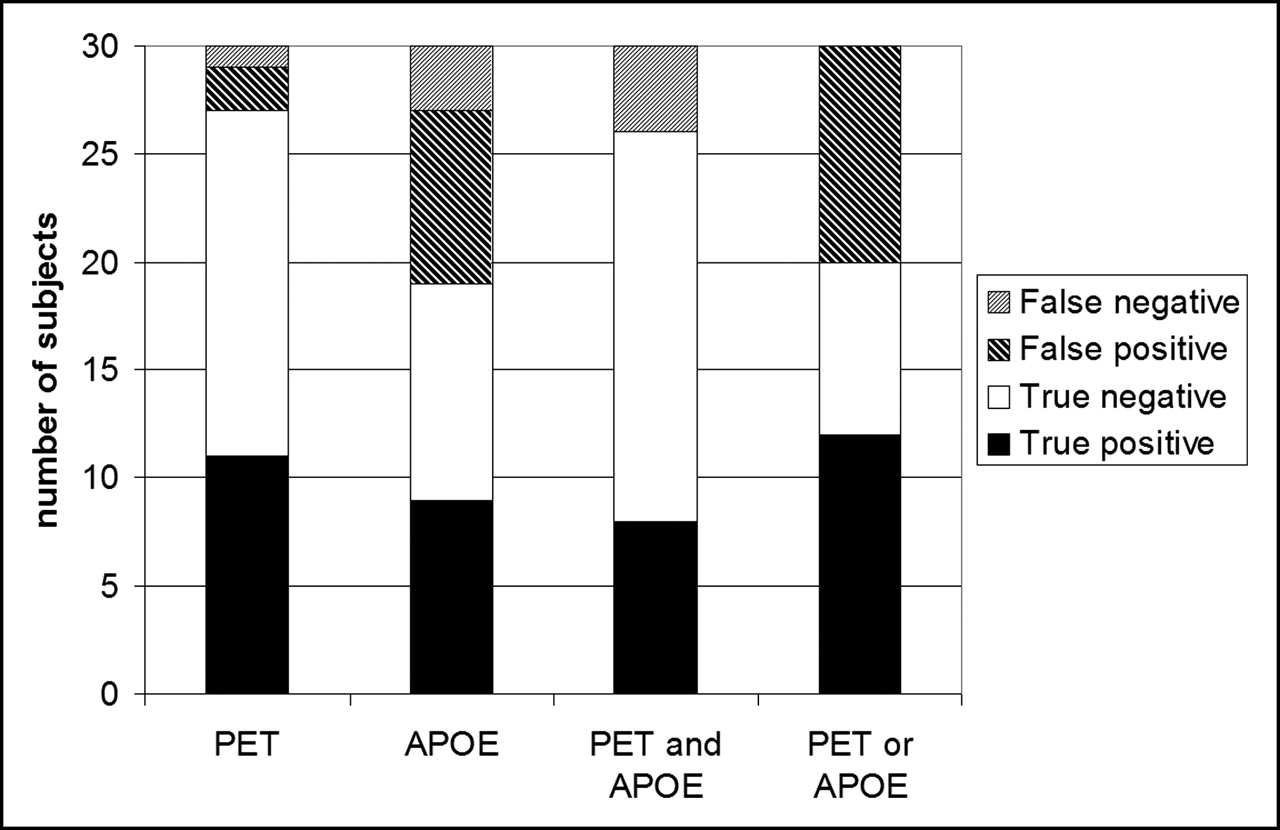
Correct prediction concerning emergence of DAT in MCI patients. True- and false-positive and -negative findings of PET, APOE genotype, and combined PET/APOE classifications. PET: MCI patients with Alzheimer-suggestive PET scan at baseline were classified as test positive; APOE: MCI patients with APOE ε4–positive genotype were classified as test positive; PET and APOE: MCI patients with Alzheimer-suggestive PET scan and APOE ε4–positive genotype at baseline were classified as test positive; PET or APOE: MCI patients with Alzheimer-suggestive PET scan or APOE ε4–positive genotype were classified as test positive.
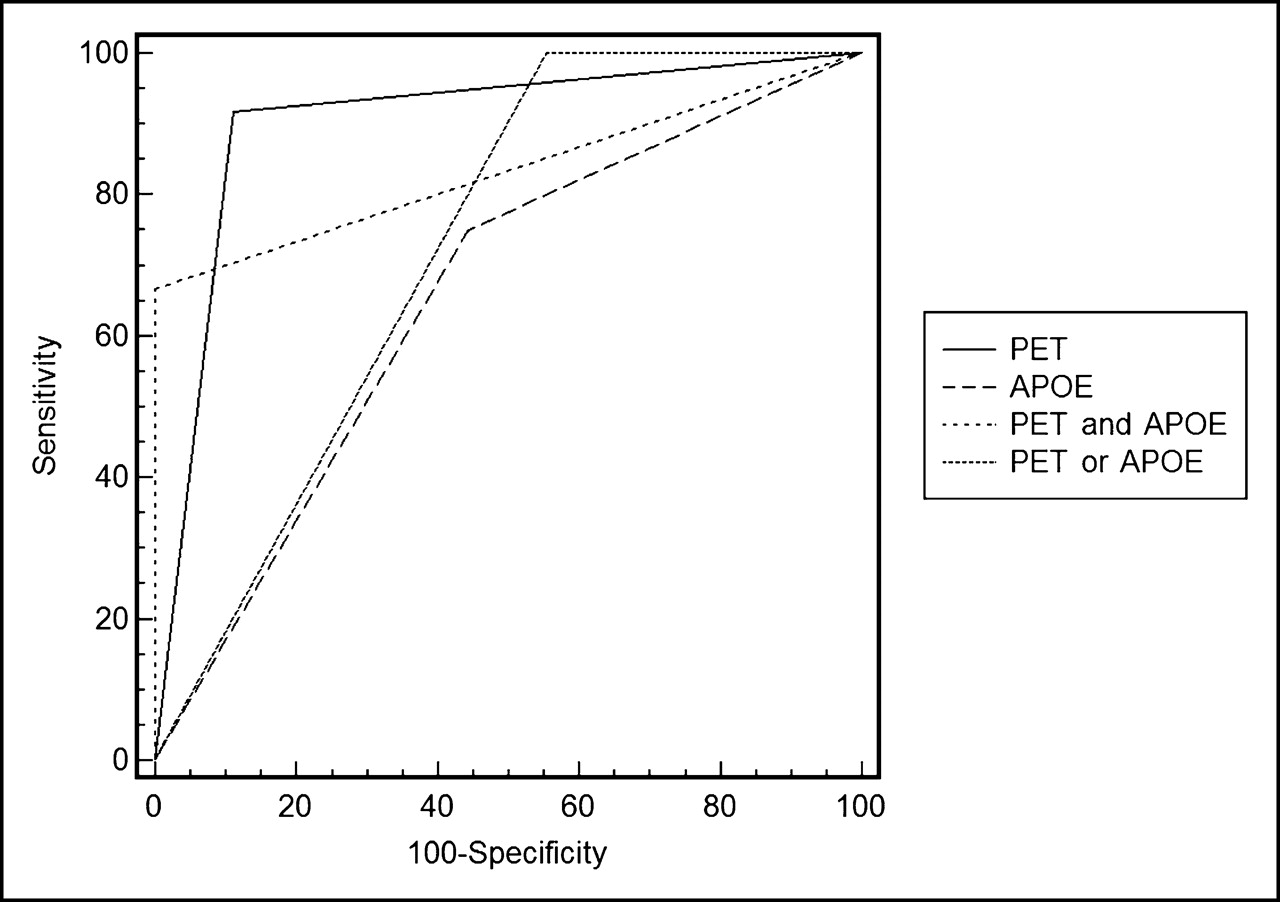
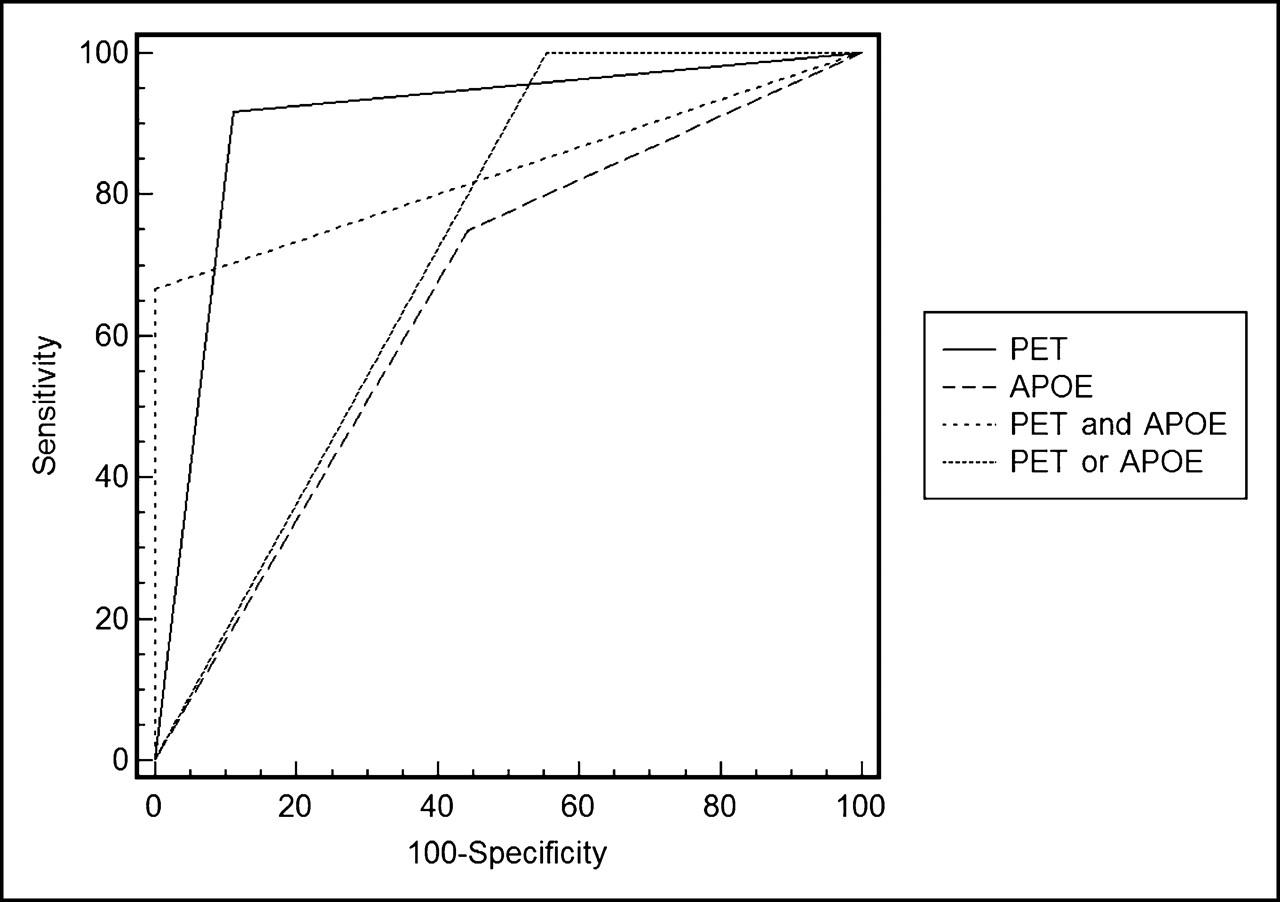
ROC analysis for PET, APOE genotyping, and combined approaches. PET: MCI patients with Alzheimer-suggestive PET scan at baseline were classified as test positive; APOE: MCI patients with APOE ε4–positive genotype were classified as test positive; PET and APOE: MCI patients with Alzheimer-suggestive PET scan and APOE ε4–positive genotype at baseline were classified as test positive; PET or APOE: MCI patients with Alzheimer-suggestive PET scan or APOE ε4–positive genotype were classified as test positive.
Statistical Evaluation
PET
In 13 (43%) of all MCI subjects, a PET scan suggestive for AD according to our predefined criteria was observed at baseline (PET positive), and 17 (57%) patients did not show AD-suggestive abnormalities (PET negative). Eleven of the 13 PET-positive patients proceeded to manifest DAT during the observation period and 16 of the 17 PET-negative patients remained clinically stable (Fig. 2). Thus, the statistical analysis revealed a sensitivity of 92% (CI, 62–99), a specificity of 89% (CI, 65–98), and a test accuracy of 90%. A PPV of 85% and a NPV of 94% were calculated for PET relating to the identification of MCI patients who did or did not progress to probable DAT (Table 2; Fig. 3). The χ2 test revealed a highly significant difference in the distribution of AD-suggestive and -nonsuggestive PET findings on progressive and nonprogressive patients (Table 1).
Combination of PET and APOE Genotyping
In 8 of all MCI patients (27%), AD-suggestive PET abnormalities in combination with ε4–positive APOE genotype (homo- and heterozygous) were detected (+/+); another 8 patients showed nonsuggestive PET findings at baseline and were ε4 negative (−/−). All patients with normal PET together with ε4–negative genotype remained clinically unchanged within the observation period, and all patients with AD-suggestive PET abnormalities and concurrent ε4–positive APOE genotype progressed to DAT. In 14 patients (46%), either normal PET in the presence of ε4–positive APOE genotype (−/+) or ε4–negative APOE genotype and AD-suggestive PET (+/−) was found. In only 4 of these 14 patients (29%) with discordant findings was progression to probable DAT observed (Fig. 2). For PET+ AND APOE+ analysis, a sensitivity of 67% (CI, 35–90), a specificity of 100% (CI, 81–100), a test accuracy of 87%, a PPV of 100%, and a NPV of 82% were calculated. Statistical evaluation of PET+ OR APOE+ analysis revealed a sensitivity of 100% (CI, 73–100), a specificity of 44% (CI, 22–69), a test accuracy of 67%, a PPV of 55%, and a NPV of 100% (Table 2; Fig. 3).
Comparison of ROC Curves
In the ROC analysis, the following areas under the curve (AUC) were calculated for the different diagnostic approaches: 0.90 for PET, 0.65 for APOE genotyping, 0.83 for combined PET AND APOE analysis, and 0.72 for PET OR APOE analysis. In pairwise statistical comparisons of the ROC curves, the AUC for PET analysis was found to be significantly greater than the AUC for APOE genotyping (P = 0.024; CI, 0.03–0.47), confirming the higher accuracy of the PET analysis. No significant differences between all other AUCs were detected (Fig. 3).
DISCUSSION
Recently, existing and potentially upcoming therapeutic options for AD are being discussed. For these therapies it is essential to start treatment at an early stage of the disease (42). This has raised interest in a more precise characterization of risk populations, such as MCI for treatment studies, and in the early diagnosis of AD in these populations. For the current prospective study, we tried to evaluate the diagnostic value of 2 noninvasive complementary prognostic tools—that is, APOE genotyping as a marker of genetic predisposition and 18F-FDG PET as a marker of actual pathology (cerebral metabolic changes). A prognostic value in MCI has been previously attributed to both diagnostic procedures (13, 21,36, 43). However, so far, only very limited data have been collected on the actual prognostic value for the individual patient. Thus, in the current study, individual diagnostic classification was constituted at baseline using PET, APOE genotyping, and combinations of both. Statistical evaluation was performed at the point of follow-up, depending on the clinical outcome by that time.
Following this approach, our study revealed the highest test accuracy for PET (90%), interpreted by means of automated image analysis, with regard to division of MCI patients into those who would or would not progress to DAT within the observation period. These relatively high values may be attributed to the largely observer-independent analytic approach of the image data. Previous studies were able to demonstrate that the applied statistical tool, which is based on a comparison with a normal database, can significantly improve diagnostic reading of brain PET data compared with observer-dependent approaches (34–36).
The assessment of the prognostic value of the APOE genotype in the current study revealed a considerably lower test accuracy and lower predictive values compared with PET analysis. The particularly low PPV can be explained by the relatively high number of false-positive findings. In 44% of MCI patients who did not progress to DAT within the observation period, the APOE ε4–positive genotype was found. However, it cannot be excluded that some of these patients will progress to DAT later on and longer observation periods are required to clarify this point. Generally, the NPVs detected in this study must be interpreted with caution with regard to possible later conversion of MCI patients to DAT. A large epidemiologic follow-up study showed continuous conversion rates of >10% every 2 y in MCI patients in a 10-y follow-up study. However, in that study, a significant proportion (>50%) of MCI patients also remained stable or improved within the observation period (44). With regard to this heterogeneity of the MCI population, the value of diagnostic tools such as APOE genotyping and PET in terms of long-term outcome remains to be evaluated.
Several studies advocate a combination of different diagnostic strategies to enhance predictive accuracy (12, 17,19, 45). For example, Bottino and Almeida concluded in their study that the validity of the ε-4 allele as a risk factor for AD in patients with MCI can be enhanced by neuroimaging (45). Only recently, Mosconi et al. concluded in a retrospective analysis that 18F-FDG PET in combination with the APOE genotype may improve prediction of the conversion to DAT in MCI (16). Therefore, we decided to evaluate prognostic approaches combining the evidence resulting from genetic assessment and 18F-FDG PET. These combined approaches allowed an early diagnosis of DAT in MCI patients with either very high sensitivity (patients with suspect PET findings OR APOE ε4–positive genotype were classified as test positive) or very high specificity (patients with suspect PET findings AND ε4–positive genotype were classified as test positive). Thus, combinations of both diagnostic parameters would possibly allow defining MCI subgroups with a very high or very low risk for the emergence of DAT in the immediate future. This could be useful, for example, for patient stratification in treatment studies. However, overall test accuracy of these combined strategies remained significantly lower than values calculated for PET alone, limiting their clinical applicability.
In the current study, more than one third of the MCI patients had proceeded to manifest DAT at the date of follow-up examination, and more than half did not show progression to dementia. These results confirm that MCI patients, even when selected carefully after clear inclusion criteria, represent a very heterogeneous group with regard to prognosis. Although the number of patients examined was relatively small, the results further underline that clinical and neuropsychologic inclusion criteria alone do not guarantee the selection of a homogeneous patient population. In our population, MCI patients who converted to DAT within the observation period were significantly older and showed significantly lower values in the baseline MMSE evaluation. However, these differences were valid only between the groups of progressive or nonprogressive patients and would not facilitate individual prognosis at baseline. It appears important to take the prognostic diversity of MCI into account when MCI patients are included in drug treatment and prediction studies. In this context, PET and assessment of the APOE genotype may be a valuable complement to neuropsychologic and other clinical assessment.
The conversion rate observed in the current study (40%) was higher than the conversion rates reported in many other epidemiologic studies, ranging between 2% and 31% per year (2). This may be a consequence of the stringent selection process, which excluded all diagnosable cerebral or systemic causes of cognitive impairment. Therefore, the patient sample was enriched with predementia AD. This enrichment is also reflected in the high overall frequency of the APOE ε4 allele (57%). With regard to these facts, the MCI population selected in our study represents a group with a high a priori risk of progressing to DAT later on and the validity of this study must be restricted to this type of highly selected population. Statistical values must be regarded preliminary and cannot be uncritically transferred to the MCI population in general. If, for example, the relatively high prevalence of 40% DAT in MCI, as found in our study, would be statistically normalized to an assumptive value of 15%, the PPV of PET would fall from 85% to 59%, whereas the NPV would rise from 94% to 98%. Nevertheless, we believe that the results of the present study are plausible and promising and inspire the need for further studies with longer follow-up periods and larger patient samples. It remains important to examine the value of PET in combination with other diagnostic criteria in further studies. Information on cerebral metabolism may be crucial for correct interpretation of other biomarker results, as shown for the APOE genotype in the current study.
CONCLUSION
In the current study, observer-independent evaluation of individual 18F-FDG PET data has been shown to have a high predictive accuracy relating to the progression of MCI to DAT within a 16-mo observation period. Results were significantly superior to the exclusive assessment of APOE genotype. A high percentage of progressive MCI patients has been shown to carry the APOE ε4 allele; however, the prognostic value of genetic assessment alone was demonstrated to be comparatively low. A prognosis based on a combination of both functional imaging and genotyping may allow an early high-risk or low-risk stratification of patients with either very high sensitivity or very high specificity. This may be valuable, for example, with regard to patient selection for clinical trials and scientific studies. However, in the current study, combined strategies remained statistically inferior to exclusive analysis of PET data.
Acknowledgments
We thank Brigitte Dzewas and Coletta Kruschke for their technical assistance and the radiochemistry group for their reliable supply of radiopharmaceuticals. We are obliged to Denise Lee for the very careful review of the manuscript. We also thank Regina Hollweck, PhD, Department of Medical Statistics and Epidemiology, Technische Universität München, for her advice and support in the statistical analysis.
Footnotes
Received Apr. 6, 2005; revision accepted Jul. 11, 2005.
For correspondence or reprints contact: Alexander Drzezga, MD, Nuklearmedizinische Klinik und Poliklinik, der Technischen Universität München, Klinikum rechts der Isar, Ismaninger Strasse 22, 81675 München, Germany
E-mail: a.drzezga{at}lrz.tu-muenchen.de
REFERENCES
In this issue





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- A New Dawn
- 18F-FDG PET Imaging in Neurodegenerative Dementing Disorders: Insights into Subtype Classification, Emerging Disease Categories, and Mixed Dementia with Copathologies
- Predicting the Progression of Mild Cognitive Impairment Using Machine Learning: A Systematic, Quantitative and Critical Review
- VGF in cerebrospinal fluid, when combined with conventional biomarkers, enhances prediction of conversion from mild cognitive impairment to Alzheimers Disease
- Is Tau Imaging More Than Just Upside-Down 18F-FDG Imaging?
- Diagnostic Value of 18F-FDG PET/CT Versus MRI in the Setting of Antibody-Specific Autoimmune Encephalitis
- Inclusion criteria provide heterogeneity in baseline profiles of patients with mild cognitive impairment: comparison of two prospective cohort studies
- Predictive value of APOE-{varepsilon}4 allele for progression from MCI to AD-type dementia: a meta-analysis
- Magnetic resonance spectroscopy in the prediction of early conversion from amnestic mild cognitive impairment to dementia: a prospective cohort study
- Comparing predictors of conversion and decline in mild cognitive impairment
- Tarot decks and PET scans: Predicting the future of MCI
- Comparison of 18F-FDG and PiB PET in Cognitive Impairment
- Effect of APOE genotype on amyloid plaque load and gray matter volume in Alzheimer disease
- Fluorodeoxyglucose-Positron-Emission Tomography, Single-Photon Emission Tomography, and Structural MR Imaging for Prediction of Rapid Conversion to Alzheimer Disease in Patients with Mild Cognitive Impairment: A Meta-Analysis
- Multicenter Standardized 18F-FDG PET Diagnosis of Mild Cognitive Impairment, Alzheimer's Disease, and Other Dementias
- Positron emission tomography imaging in dementia
- Maternal family history of Alzheimer's disease predisposes to reduced brain glucose metabolism
- Role of Neuroimaging in Alzheimer's Disease, with Emphasis on Brain Perfusion SPECT
- 18F-FDG PET Database of Longitudinally Confirmed Healthy Elderly Individuals Improves Detection of Mild Cognitive Impairment and Alzheimer's Disease