


Several neurodegenerative disorders exhibit pathologic aggregation of the tau protein in the brain and are therefore summarized under the term tauopathies (1). Alzheimer disease (AD) is considered a tauopathy because, in addition to extraneuronal β-amyloid plaques, it is characterized by pathologic tau aggregation in the form of intraneuronal neurofibrillary tangles (2). In other tauopathies—including progressive supranuclear palsy, corticobasal degeneration, and some other disorders of the spectrum of frontotemporal lobar degenerative disorders—tau pathology may occur as the leading form of protein aggregation abnormality (3). The disappointing results of antiamyloid therapy approaches in AD (4,5) and the onset of novel anti-tau therapeutic concepts (6,7) have increased interest in the in vivo detection of tau pathology, which has been limited to postmortem examinations so far.
Several PET tracers for cerebral tau deposits have been developed, and some have already been applied in vivo to patients with neurodegenerative disorders. The most widely used tracers are 18F-AV-1451, 18F-THK5351, and 11C-PBB3 (8,9). More recently, tracers such as 18F-MK-6240, 18F-RO6958948, 18F-PI-2620, and 18F-JNJ64349311 have been introduced, and further compounds are under evaluation (10–12). Although some of these compounds are already being tested in clinical trials (up to phase 3), all of the available tracers can currently still be considered in an exploratory stage and the available literature is still limited.
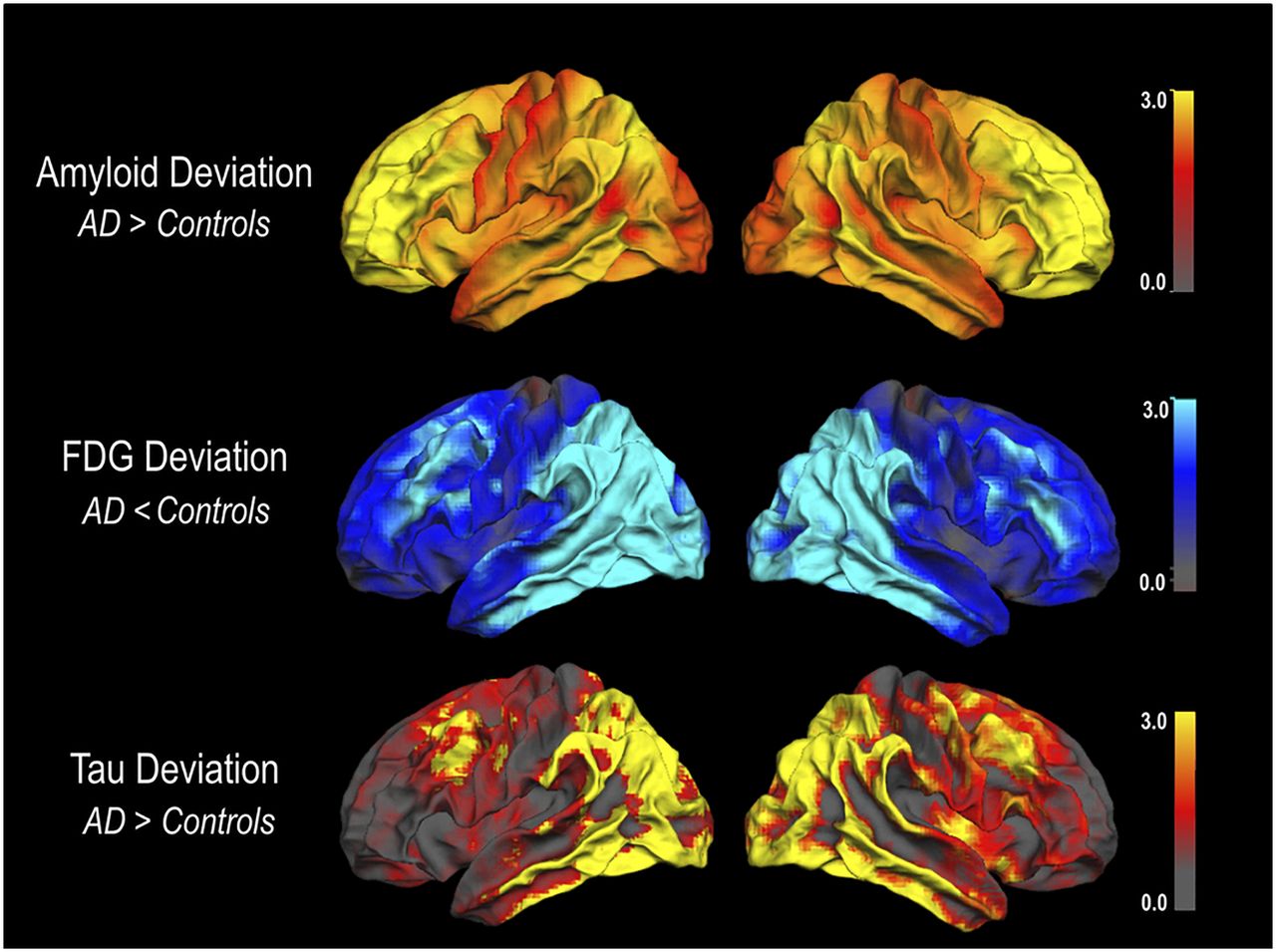
In several studies, a strong similarity between the distribution of tau tracer retention in the brain and the extent of hypometabolic abnormalities (as measured with 18F-FDG PET) has been observed (Fig. 1) (13–16). Furthermore, these studies statistically demonstrated an inverse quantitative relationship between tau deposition and metabolism. While underscoring the hypothesis that tau pathology may be causally involved in the development of neuronal dysfunction, this upside-down similarity between the two methods raises the question of whether tau PET has additional clinical value over established 18F-FDG PET.
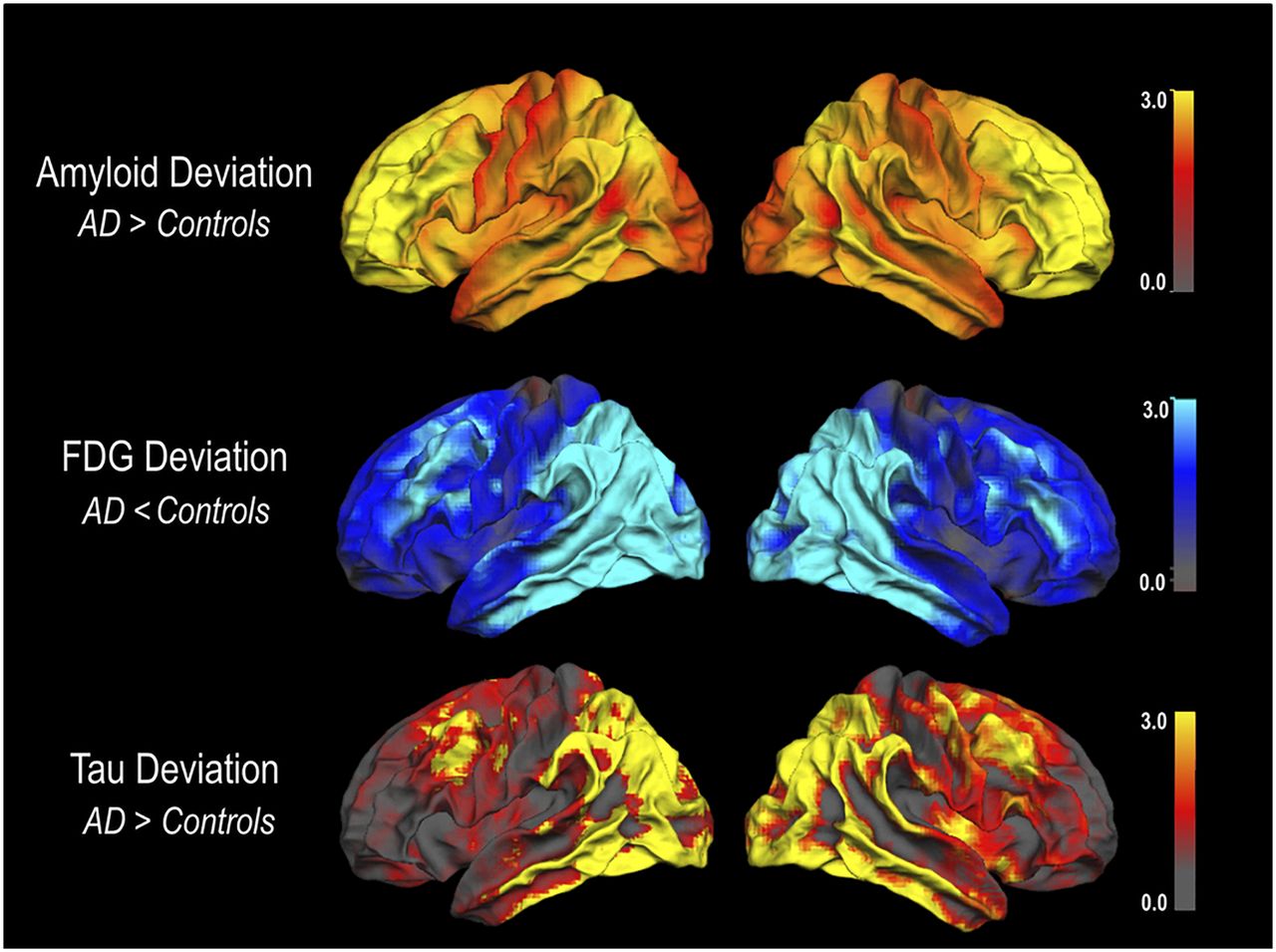
Spatial correspondence of mean 18F-FDG deviation and mean tau deviation but not amyloid deviation in patients with AD. Deviation images were projected on lateral surface of left and right hemispheres using FreeSurfer. (Reprinted with permission of (13).)
STATUS OF TRACER VALIDATION
18F-FDG PET imaging has proven to have high diagnostic value at relatively low costs in the assessment of neurodegeneration (17–21). The tracer is broadly available, and automated analytic approaches and international guidelines are established (20,21).
In contrast, validation and standardization of tau tracers is far less advanced. This may stem not only from the novelty of the tracers but also from the complexity of tau as a target itself. Tau deposition can occur in different splicing isoforms (3R vs. 4R), different primary forms of fibrous assembly (paired helical vs. straight filaments), and different aggregation states (neurofibrils, pretangles, mature tangles, and coiled bodies, among others). Moreover, tau can be found in different cellular locations (intraneuronal, intraglial) and macroscopic anatomic locations (basal ganglia, cortex) (22,23). This variance in the appearance of tau pathology hampers the development and evaluation of tau imaging tracers.
Recently developed tau tracers have been promising insofar as in vitro analyses suggested distinct binding to tau pathology in the absence of relevant binding to amyloid (8). Furthermore, in vivo tracer retention patterns showed good agreement with the expected distribution of tau pathology (2,24). However, considerable between-tracer differences in regional capture of tau pathology may exist in AD (25–27) and in non-AD tauopathies such as corticobasal degeneration or progressive supranuclear palsy. Additionally, some evidence questions the specificity of currently available tau tracers. This refers to non-tau pathology such as TDP-43 and to off-target binding, which has been observed in vivo for several of the tracers in various regions (basal ganglia, brain stem, choroid plexus, and extracerebral structures) (24,28,29).
Elevated binding to melanin and monoaminooxydase may explain some of the off-target binding (30–32). Particularly worrisome are recent findings demonstrating a potential contribution of monoaminooxydase-B binding to tau PET imaging not only in subcortical but also in cortical brain regions (33). Such a contribution by unspecific binding could hamper quantitative assessment, particularly in longitudinal tau PET studies.
In summary, comparability between existing tau tracers is currently not warranted. To gain critical insight into the differential sensitivity and specificity of the currently available tracers, further evaluation is required, particularly with regard to systematic in vivo or postmortem cross validation. Corresponding studies are currently under way.
POTENTIAL FOR EARLY DIAGNOSIS
The value of 18F-FDG PET for early diagnosis of AD, particularly regarding short-term prediction of conversion to AD-type dementia in patients with mild cognitive impairment, has been repeatedly demonstrated (20,34,35). Similar data are not yet available for tau PET imaging. Supporting current hypothetical disease models, some studies suggest that tau pathology may be detected subsequent to elevated amyloid pathology by means of amyloid PET (36). Others suggest that mesial temporal tau aggregation may exist in some healthy elderly subjects in the absence of amyloid pathology, but the pathologic relevance of these findings is yet unclear (24). Regarding the obvious similarity between 18F-FDG PET and tau PET findings documented so far, similar sensitivities with regard to early detection may be expected. However, preliminary data from our and other groups (directly comparing 18F-FDG and tau PET in patients with mild cognitive impairment and AD) suggest that tau abnormalities may be somewhat more pronounced than hypometabolic changes and possibly can be detected earlier (Fig. 2) (37). Also, hot lesions in tau PET may be more salient than cold lesions in 18F-FDG PET.

Clearly abnormal tau PET findings but barely abnormal 18F-FDG PET findings in 66-y-old man with mild cognitive impairment and cerebrospinal fluid values indicative of AD pathology. Axial slices of SUV ratio images are shown for 18F-AV-1451 and 18F-FDG PET. Global maximum intensities were set to 100 for scaling.
POTENTIAL FOR DIFFERENTIAL DIAGNOSIS
The valuable role of 18F-FDG PET in differential diagnosis of neurodegenerative disorders has repeatedly been demonstrated, including various forms of dementias, movement disorders, and atypical Parkinsonian syndromes (38,39). In a similar vein, tau PET imaging shows specific patterns of tau tracer retention in typical and atypical variants of AD and other tauopathies (14,15,40–43). However, unlike 18F-FDG, tau PET at the same time provides insights on underlying neuropathology, which may allow tauopathies (e.g., corticobasal degeneration or progressive supranuclear palsy) to be distinguished from non-tauopathies (e.g., multiple-system atrophy).
POTENTIAL AS A BIOMARKER IN CLINICAL TRIALS
For 18F-FDG PET, a reliable association between hypometabolism and the type and severity of cognitive deficits has been demonstrated (44,45). This association qualifies 18F-FDG PET as a valuable tool to track clinical progression. However, 18F-FDG PET results may be affected by functional processes such as diaschisis or compensatory effects. In this respect, tau imaging may more directly mirror the extent and progression of neuropathology. Moreover, as a major advantage over amyloid PET, tau tracer uptake may better track cognitive decline than does amyloid deposition, as expected from neuropathologic studies. Most importantly, tau PET may be used for the selection of patients in future therapeutic trials directed toward the removal of tau pathology (7). Results from tau PET may also serve as a surrogate endpoint in clinical trials, since tau PET may reflect more proximal processes in the cascade of neurodegeneration than does hypometabolism. Tau PET could therefore surpass 18F-FDG PET as a “reasonably likely surrogate endpoint” in clinical trials (46).
CONCLUSION
Tau imaging represents an exciting, novel approach aiming to assess a basic pathology of neurodegeneration in vivo. Although similarities between patterns of hypometabolism and tau tracer deposition have been documented, tau imaging certainly offers more than just upside-down 18F-FDG PET information. An added clinical value of tau PET over the well-established 18F-FDG PET can be expected but remains to be proven. Preliminary data indicate that tau imaging could be slightly more sensitive than 18F-FDG PET in detecting the onset of neuronal injury in early stages of AD. Tau PET may also have advantages with regard to differential diagnosis. In addition to measuring the extent and localization of pathology, tau PET may allow differentiation between tauopathies and non-tauopathies. These questions may gain relevance with the advent of anti-tau therapy trials. Specific monitoring of anti-tau treatment may also represent a most important future application for tau PET. Although tau PET imaging certainly holds great potential in various diseases and in different domains spanning from early and differential diagnosis to disease monitoring, many questions, particularly with regard to validation of the tracers, still remain open. Much more needs to be learned about the variability of the signal due to unspecific contributions, across different tracers, and in different disease populations.
DISCLOSURE
Thilo van Eimeren received speaker and consulting honoraria and/or research support from AVID Radiopharmaceuticals and Eli Lilly. Alexander Drzezga received speaker and consulting honoraria and/or research support from AVID Radiopharmaceuticals, Eli Lilly, GE Healthcare, Siemens Healthcare, and Piramal. No other potential conflict of interest relevant to this article was reported.
Footnotes
Published online May 10, 2017.
- © 2017 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication April 4, 2017.
- Accepted for publication May 5, 2017.





{kind=link}
{kind=link}