


Abstract
We determined whether the addition of the angiotensin-receptor blocker valsartan to an angiotensin-converting enzyme (ACE) inhibitor improves cardiac sympathetic nerve activity and left ventricular function in patients with congestive heart failure (CHF). Methods: Thirty-two patients with CHF (left ventricular ejection fraction [LVEF] < 40%; mean, 33% ± 6%) were treated with an ACE inhibitor and a loop diuretic. Sixteen patients (group A) were randomized to additionally receive valsartan (40–80 mg/d), and the remaining 16 patients (group B) continued their current regimen. Patients were studied before and 6 mo after treatment. The delayed heart-to-mediastinum count ratio (H/M ratio), delayed total defect score (TDS), and washout rate (WR) were determined from 123I-metaiodobenzylguanidine images. The left ventricular end-diastolic volume (LVEDV) and LVEF were determined by echocardiography, and New York Heart Association (NYHA) functional class was estimated. Results: Before treatment, TDS, H/M ratio, WR, LVEDV, LVEF, and NYHA functional class were similar in both groups. After treatment in group A, TDS decreased from 37 ± 8 to 31 ± 9 (P < 0.001), H/M ratio increased from 1.66 ± 0.23 to 1.81 ± 0.23 (P < 0.001), and WR decreased from 47% ± 9% to 39% ± 10% (P < 0.01). In addition, the LVEDV decreased from 193 ± 36 mL to 169 ± 51 mL (P < 0.005), and LVEF increased from 32% ± 7% to 41% ± 13% (P = 0.0005). In group B, these parameters did not change significantly. NYHA functional class improved in both groups (in group A, from 3.3 ± 0.5 to 1.7 ± 0.6 [P < 0.0005]; in group B, from 3.3 ± 0.5 to 2.4 ± 0.6; [P < 0.005]). The improvement was significantly greater in group A than in group B (P < 0.05). Conclusion: The addition of valsartan to an ACE inhibitor improves cardiac sympathetic nerve activity, left ventricular function, and symptoms in patients with CHF.
Despite considerable advances in pharmacologic therapy for congestive heart failure (CHF), mortality rates for CHF remain high, with approximately 50% of patients dying within 5 y of diagnosis (1). Angiotensin-converting enzyme (ACE) inhibitors increase survival when introduced at any stage of CHF (2–7). ACE inhibitors are believed to act principally by blocking the formation of angiotensin II (A-II), a potent vasoconstrictor and cardiovascular growth stimulator that may contribute to increased impedance to left ventricular ejection and cardiac remodeling (8,9). However, growing evidence supports an important role for non-ACE-mediated enzymatic pathways in the conversion of angiotensin I to A-II (10,11). Consequently, A-II production may persist despite ACE inhibition, and the efficacy of these drugs may be attributed, in part, to increased concentrations of bradykinin due to the inhibition of the kininase that mediates its breakdown (12).
Angiotensin-receptor blockers (ARBs) inhibit the angiotensin type 1 receptor and exert hemodynamic effects similar to those of ACE inhibitors in the setting of CHF (13,14). The ARB valsartan has beneficial hemodynamic and hormonal effects in patients with CHF taking standard doses of ACE inhibitors (15). The Valsartan in Heart Failure Trial (Val-HeFT) reported that the addition of valsartan significantly improves New York Heart Association (NYHA) functional class, left ventricular remodeling, left ventricular ejection fraction (LVEF), and signs and symptoms of heart failure (16).
Myocardial imaging with 123I-metaiodobenzylguanidine (MIBG), an analog of norepinephrine, is a useful tool for detecting abnormalities of the myocardial adrenergic nervous system in patients with CHF (17–19). Several reports have suggested that the treatment of heart failure can improve cardiac sympathetic nerve activity based on cardiac MIBG scintigraphy in patients with CHF (20–22). However, there are no reports using cardiac 123I-MIBG scintigraphy to evaluate the effects of the addition of ARB to an ACE inhibitor in patients with CHF. This study was performed to determine whether valsartan can improve cardiac sympathetic nerve activity, left ventricular function, and symptoms in patients with CHF.
MATERIALS AND METHODS
Study Population
Thirty-two patients, 19 men and 13 women (mean age, 68 ± 12 y; age range, 42–88 y), with CHF were included in the study. A detailed history and physical examination were obtained before inclusion in the study. Chest radiography, standard electrocardiography, echocardiography, and 201Tl and 123I-MIBG scintigraphy were performed on all patients. Patients were in NYHA functional class III or IV at the time of enrollment and had an echocardiographic LVEF < 40% (mean, 33% ± 6%). The causes of CHF were old myocardial infarction (n = 16), idiopathic dilated cardiomyopathy (n = 10), and valvular disease (n = 6). All patients were being treated with an ACE inhibitor and a loop diuretic (Table 1).
Demographics and Clinical Characteristics
Patients were excluded from the study if they had primary operable valvular heart disease, congenital heart disease, unstable angina, recent acute myocardial infarction, primary hepatic failure, or active cancer. The study was approved by the ethics review board of our institution, and written informed consent was obtained from all patients.
Study Protocol
Sixteen patients (group A) were randomized to additionally receive valsartan (40–80 mg/d), and the remaining 16 patients (group B) continued their current drug regimen. We performed a series of examinations before and 6 mo after treatment. In this study, no patient received a β-blocker.
123I-MIBG Imaging
The method used for 123I-MIBG imaging has been described previously (20). The 123I-MIBG was obtained commercially (Daiichi-Radioisotope Laboratories). Patients were injected intravenously with 123I-MIBG (111 MBq) while upright. Anterior planar and SPECT images were acquired 15 min after injection and again 4 h later. SPECT was performed with a dedicated single-head imaging system (Millennium MPR; General Electric Medical Systems). The energy, uniformity, and linearity were continuously corrected. Images were acquired for 40 s at 32 steps over a 180° orbit and were recorded at a digital resolution of 128 × 128 from the anterior planar 123I-MIBG image.
From anterior planar delayed 123I-MIBG images, the heart-to-mediastinum count ratio (H/M ratio) was determined. Washout rate (WR) was calculated by the following equation: {([H]-[M])early − ([H]-[M])delayed}/([H]-[M])early × 100 (%), where [H] = mean count per pixel in the left ventricle and [M] = mean count per pixel in the upper mediastinum. In our laboratory, the normal range for the delayed H/M ratio is 2.00–2.80 and the normal range for WR is 22%–32%.
The myocardial delayed SPECT images for each patient were divided into 20 segments. The short-axis images at the basal, middle, and apical ventricular levels were divided into 6 segments. The apical segment of the vertical long-axis image was divided into 2 segments. Regional tracer uptake was assessed semiquantitatively using a 4-point scoring system (0 = normal uptake, 1 = mildly reduced uptake, 2 = moderately reduced uptake, and 3 = severely reduced uptake). The total defect score (TDS) was calculated as the sum of the scores for all 20 segments.
Interobserver variability was determined in a masked manner by 2 independent observers, who had no knowledge of the clinical status and medication of the patients. The interobserver correlation was represented by r = 0.90 (P < 0.001).
Echocardiography
Echocardiographic measurements were performed using standard methods in a masked manner before and 6 mo after treatment. Two independent and experienced echocardiographers who had no knowledge of the study performed all measurements. Left ventricular end-diastolic volume (LVEDV) and LVEF were calculated using the modified Simpson method (23).
Data Analysis and Statistics
Statistical analysis was performed using StatView (Abacus Concepts) for Macintosh (Apple Computer, Inc.). Numeric results are expressed as the mean ± SD. Comparison of baseline data between 2 groups was by the χ2 test. The differences between continuous variables were evaluated using the unpaired t test. Changes in NYHA functional class were assessed using the Wilcoxon matched-pairs signed rank test. The effects of chronic treatment were assessed within groups by the paired t test and between groups by ANOVA. A value of P < 0.05 was considered statistically significant.
RESULTS
The hemodynamic characteristics of the 2 groups did not differ significantly. Before treatment, TDS, H/M ratio, WR, LVEDV, LVEF, and NYHA functional class were similar in both groups.
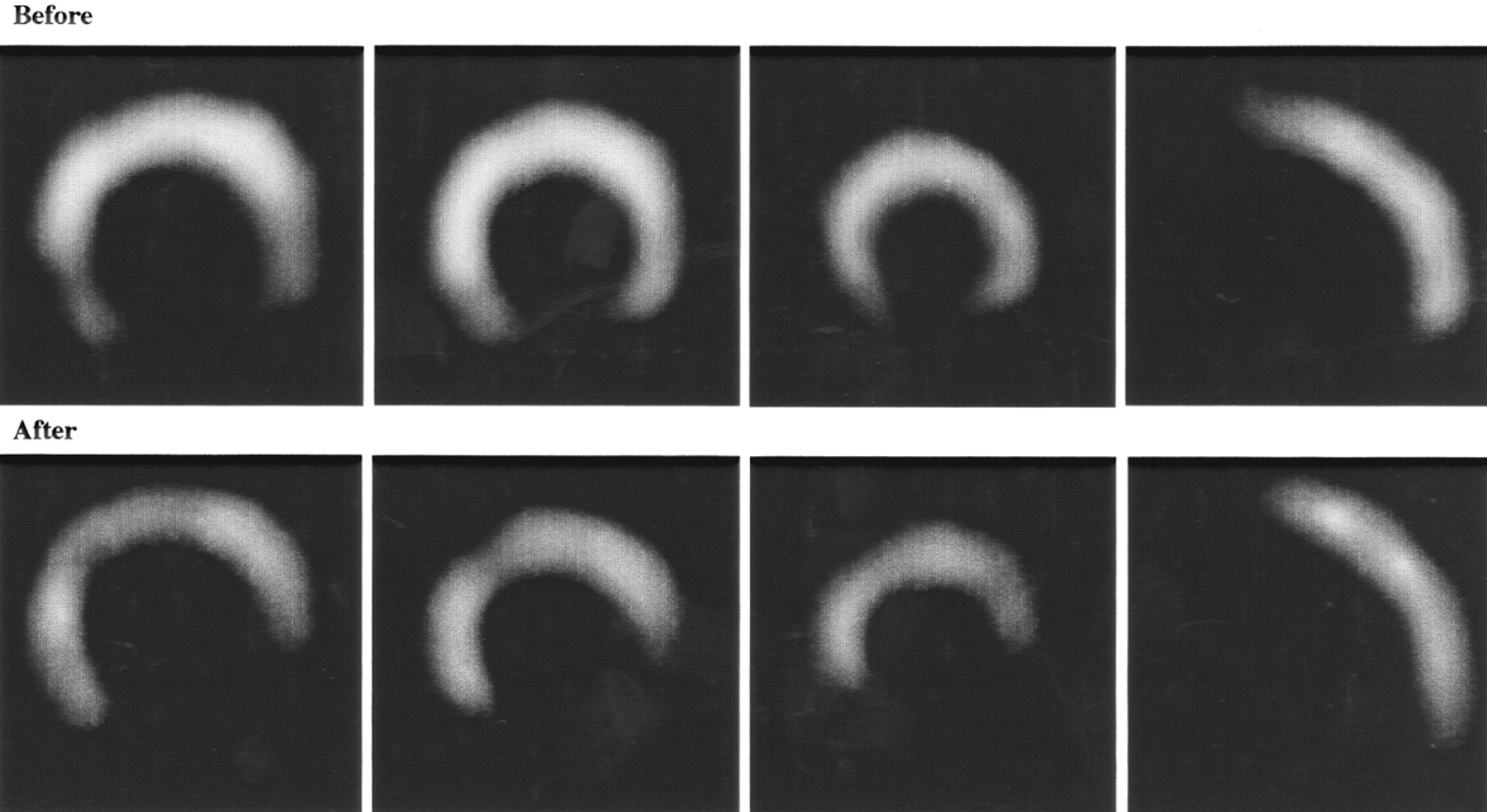
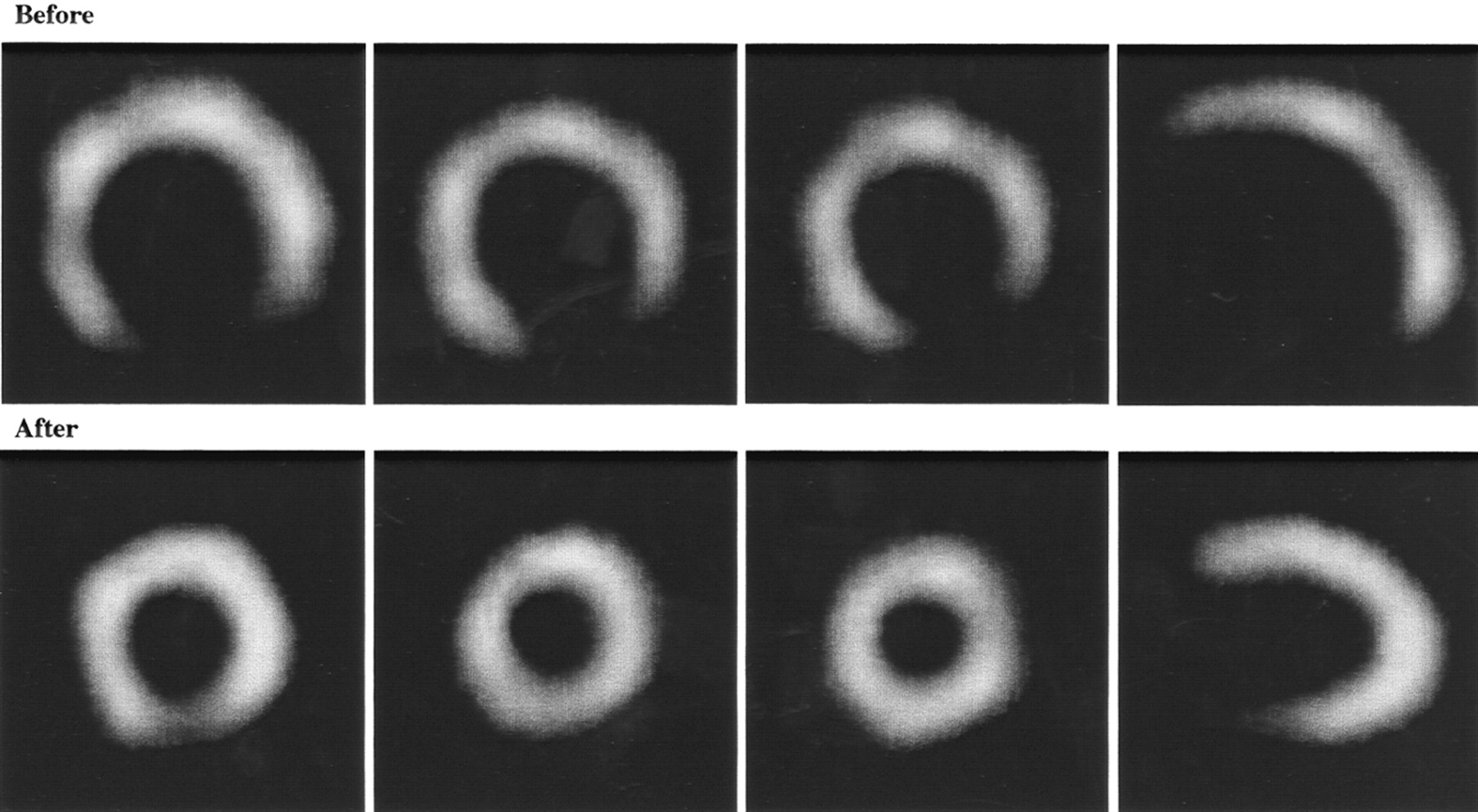
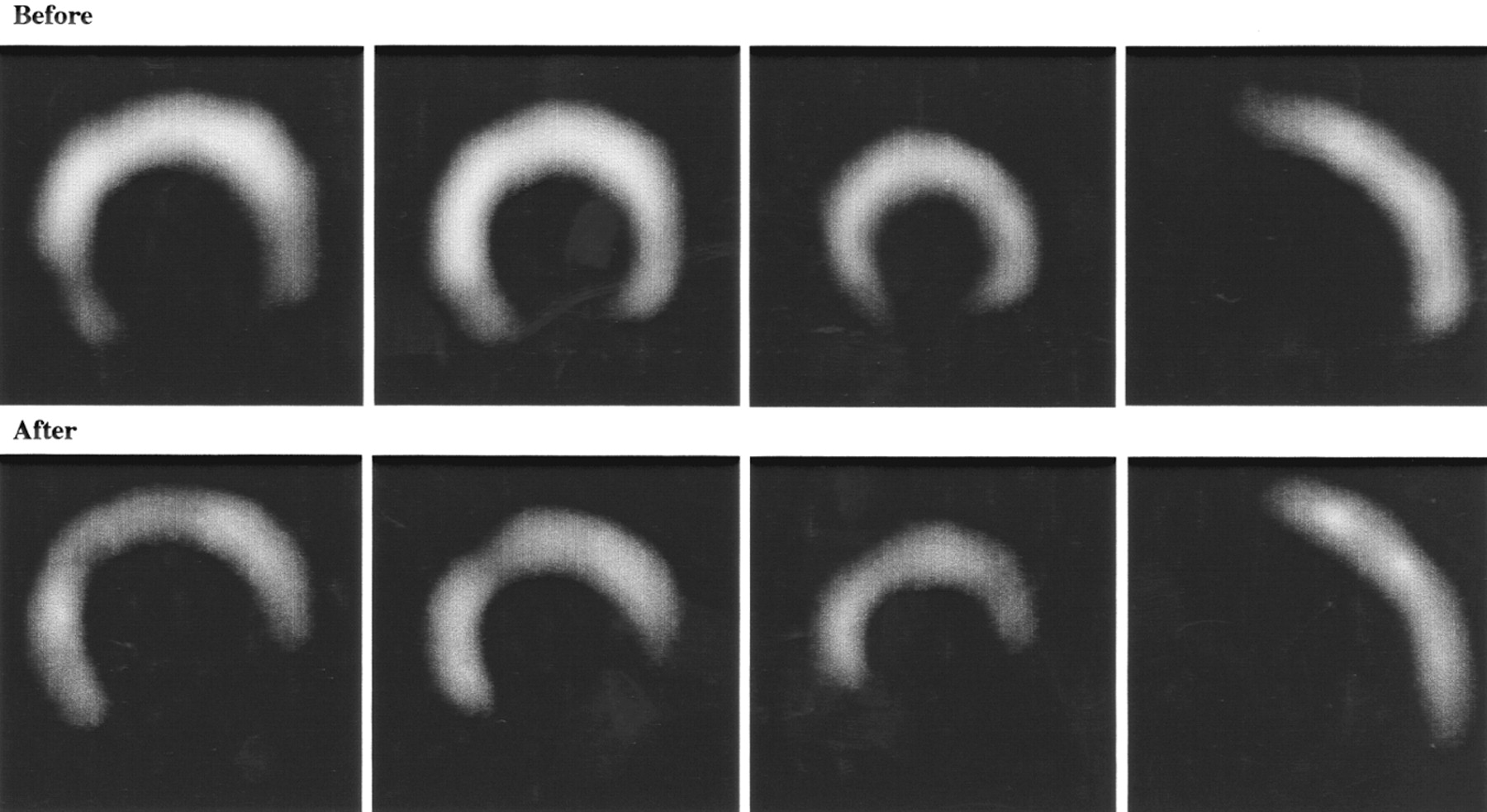
TDS, H/M ratio, and WR are reported in Table 2. In group A, the TDS decreased significantly after 6 mo (31 ± 9), compared with the baseline value (37 ± 8) (P < 0.001). In contrast, in group B, there were no significant differences between the values at baseline and after 6 mo of treatment. In the segmental analysis in both groups, though TDS tended to improve the uptake of the inferior wall, the improvement was not statistically significant. In group A, the H/M ratio increased significantly after 6 mo (1.81 ± 0.23), compared with the baseline values (1.66 ± 0.23) (P < 0.001). In contrast, in group B, there were no significant differences between the values at baseline and after 6 mo of treatment. In group A, the WR decreased significantly after 6 mo (39% ± 10%), compared with the baseline values (47% ± 9%) (P < 0.01). In contrast, in group B, there were no significant differences between the values at baseline and after 6 mo of treatment. Furthermore, after 6 mo of treatment, the WR was significantly lower in group A than in group B (P < 0.005). Representative 123I-MIBG images from both groups before and after treatment are shown in Figures 1 and 2.

Representative SPECT 123I-MIBG images from patient treated with addition of valsartan to ACE inhibitor.
Representative SPECT 123I-MIBG images from patient treated with ACE inhibitor.
Changes in TDS, H/M Ratio, and WR for 123I-MIBG Imaging in Patients with CHF
LVEDV and LVEF are reported in Table 3. In group A, the LVEDV decreased significantly after 6 mo (169 ± 51 mL), compared with the baseline value (193 ± 36 mL) (P < 0.005). In contrast, in group B, there were no significant differences between the values at baseline and after 6 mo of treatment. In group A, the LVEF after 6 mo of treatment (41% ± 13%) increased significantly from the baseline value (32% ± 7%) (P = 0.0005). In contrast, in group B, there were no significant differences between the values at baseline and after 6 mo of treatment.
Changes in LVEDV, LVEF, and NYHA Functional Class in Patients with CHF
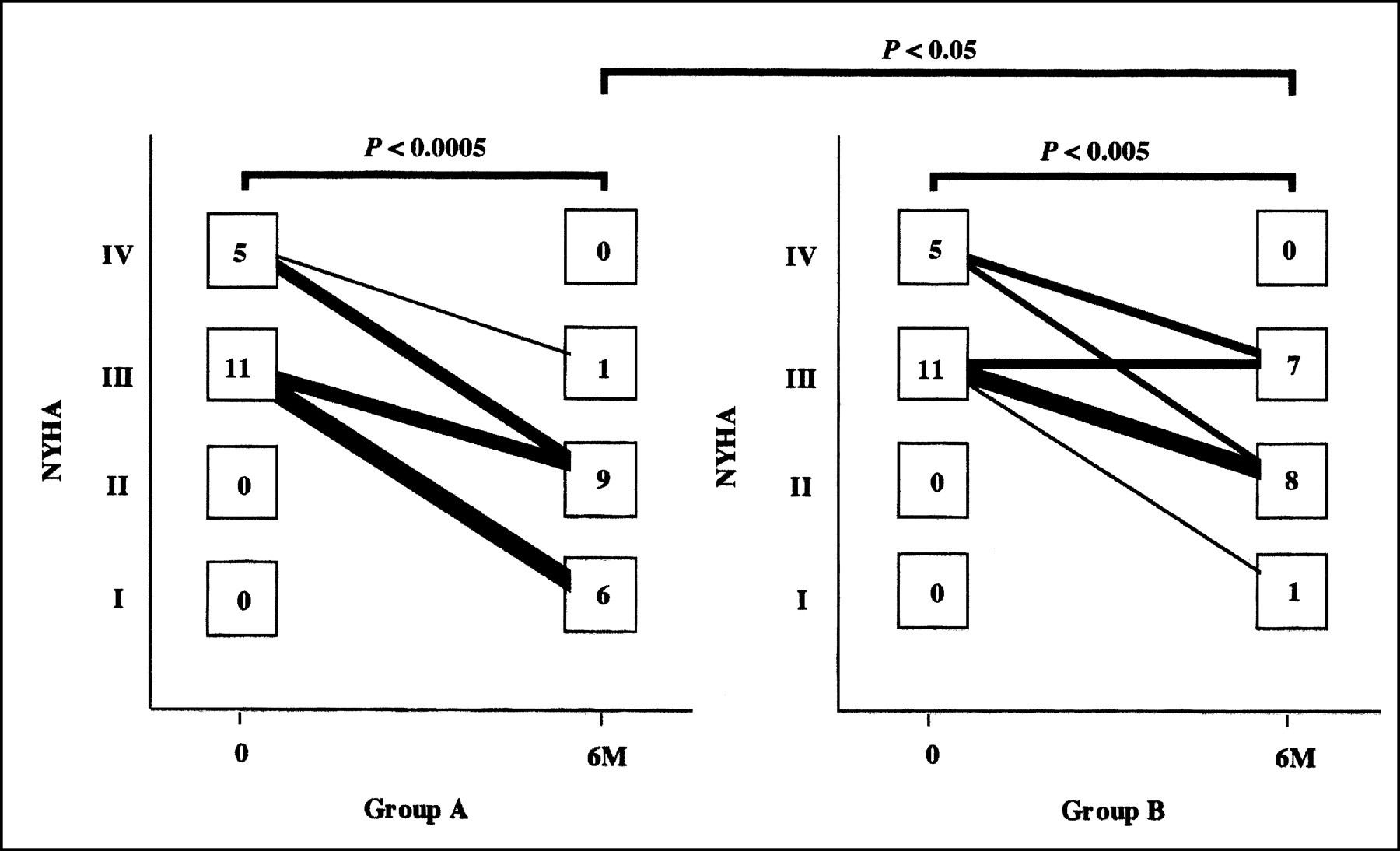
The NYHA functional class of the patients is shown in Table 3 and Figure 3. Patients in both groups showed functional improvement after 6 mo of treatment, compared with the baseline values (in group A, from 3.3 ± 0.5 to 1.7 ± 0.6, P < 0.0005; in group B, from 3.3 ± 0.5 to 2.4 ± 0.6, P < 0.005). After treatment, the NYHA functional class was better for the patients of group A than the patients of group B (P < 0.05).
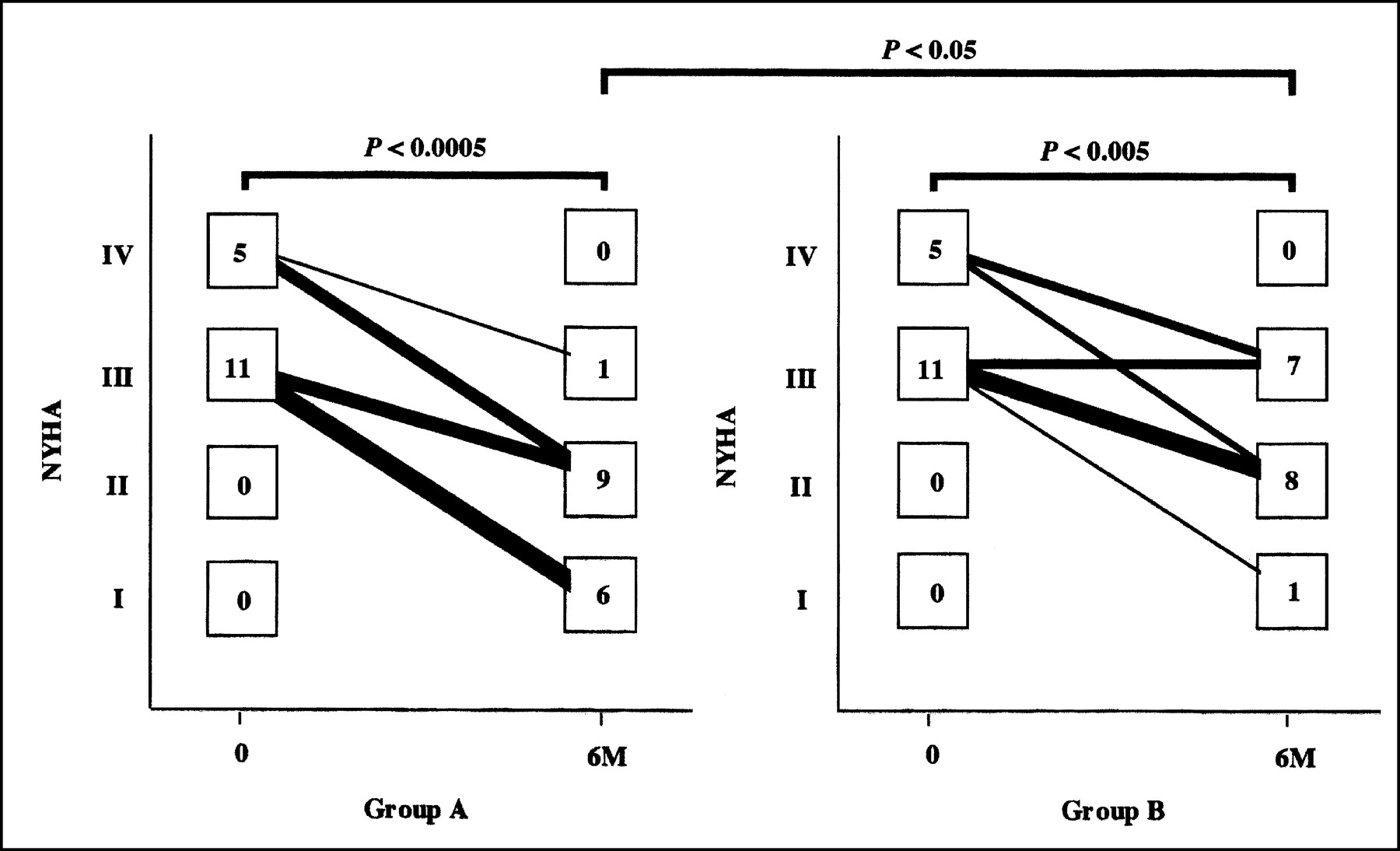
Changes in NYHA functional class in groups A and B during treatment. 6M = after 6 mo of therapy.
DISCUSSION
The potential adverse effects of angiotensin on cardiovascular function make its inhibition an attractive therapeutic approach to heart failure. Although ACE inhibitors were designed to decrease circulating and tissue concentrations of A-II, recent evidence suggests that current therapeutic regimens using ACE inhibitors do not adequately suppress A-II production (15). Whether this pharmacologic failure is related to inadequate dosing or frequency of ACE inhibitor administration or to the activity of non-ACE-mediated pathways of A-II production (10,11) remains uncertain. The present study raises the possibility that ACE inhibitors are exerting their favorable effects through an alternative mechanism. Therefore, the strategy of providing more complete blockade of angiotensin with valsartan for the treatment of heart failure appears rational.
The growth-promoting and apoptotic effects of A-II have been well documented (24,25) and may contribute to the structural remodeling that promotes the progression of heart failure (26–28). A long-term increase in the LVEF has been identified as a marker of beneficial left ventricular remodeling that is manifested as a reduced chamber volume (29). This structural effect is associated with an improvement in survival (30). Val-HeFT (16) documented that the addition of valsartan significantly improves cardiac function and reduces mortality and morbidity in patients with heart failure. In this study, left ventricular volume and cardiac function were significantly improved by adding valsartan to standard ACE inhibitor therapy. Moreover, in our study, the addition of valsartan also improved the symptoms of heart failure, as measured by changes in the NYHA functional class.
Cardiac 123I-MIBG, an analog of norepinephrine, can be used to detect abnormalities of the myocardial adrenergic nervous system in patients with CHF (17–19). Because activation of the renin-angiotensin system in the setting of CHF facilitates cardiac norepinephrine release, treatment with ACE inhibitors may affect cardiac sympathetic activity (31,32). Several reports have suggested, on the basis of cardiac 123I-MIBG scintigraphy in patients with CHF, that ACE inhibitor therapy can improve cardiac sympathetic nerve activity (21,22). However, no reports have been published on the use of cardiac 123I-MIBG scintigraphy to evaluate the effects of combined ARB and ACE inhibitor therapy in patients with CHF. In this study, we used 123I-MIBG scintigraphy to examine whether valsartan could improve cardiac sympathetic nerve activity in patients with CHF, and we found that the TDS, H/M ratio, and WR improved with the addition of valsartan to standard ACE inhibitor therapy.
On the basis of cardiac 123I-MIBG scintigraphy, our study showed that an ACE inhibitor alone could not improve cardiac sympathetic nerve activity, although previous reports had indicated that this treatment did result in an improvement (21,22). However, in the patients of our study, cardiac function was relatively low and the symptoms of heart failure were more severe than in the previously reported patients; therefore, the improvement in cardiac sympathetic nerve activity brought about by an ACE inhibitor might not be recognizable. Because of the results of our study and the previous reports, we consider that the renin-angiotensin system should be more completely blocked by combined ARB and ACE inhibitor therapy in patients with severe CHF.
In this study, delayed MIBG images were used to determine the TDS and H/M ratio. There are 2 types of norepinephrine and MIBG uptake. Uptake-1 (neuronal uptake), which takes place even if the concentration of norepinephrine or MIBG is low, depends on sodium and adenosine triphosphate and is suppressed by tricyclic antidepressants. Uptake-2 (extraneuronal uptake), which takes place only when the concentration is high, represents simple diffusion and is unaffected by tricyclic agents (33,34). Early images result from both uptake-1 and uptake-2 (35,36), whereas delayed images are less dependent on uptake-2 and therefore reflect the status of cardiac sympathetic nerve activity more accurately. Furthermore, since the neuronal accumulation of MIBG reached a peak value 4 h after its administration, the neuronal uptake of norepinephrine can be evaluated accurately if MIBG imaging is performed at that time (36). For these reasons, we used delayed MIBG imaging in this study.
Recently, it has been reported that aldosterone is produced in the ventricles of the failing human heart (37) and that the aldosterone synthase gene is expressed in cardiac tissue (38). Furthermore, it has been reported that aldosterone induces the expression of ACE messenger RNA in cultured neonatal cardiocytes (39). Activation of the renin-angiotensin-aldosterone system is known to prevent myocardial uptake of norepinephrine (20,31,32,40). Therefore, we believe that it is important to more completely inhibit the renin-angiotensin-aldosterone system by adding valsartan to an ACE inhibitor in patients with severe CHF.
CONCLUSION
The TDS, H/M ratio, and WR determined by 123I-MIBG scintigraphy were significantly improved after 6 mo of addition of valsartan to ACE inhibitor therapy. In addition, echocardiographic parameters improved with this treatment. These findings indicate that the addition of valsartan to an ACE inhibitor can improve cardiac sympathetic nerve activity and cardiac function in patients with CHF.
Acknowledgments
The authors thank Takayoshi Honjo, Akira Nakaya, Hiromitsu Takahashi, Hiroyuki Takada, and Takehiro Ishikawa for their technical assistance.
Footnotes
Received Oct. 7, 2002; revision accepted Feb. 13, 2003.
For correspondence or reprints contact: Shu Kasama, MD, Second Department of Internal Medicine, Gunma University School of Medicine, 3-39-15, Showa-machi, Maebashi, Gunma 371-0034, Japan.
E-mail: s-kasama{at}bay.wind.ne.jp
REFERENCES
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Comparative effects of long-acting and short-acting loop diuretics on cardiac sympathetic nerve activity in patients with chronic heart failure
- Introduction to Cardiac Neuronal Imaging: A Clinical Perspective
- 123I-MIBG SPECT for Evaluation of Patients with Heart Failure
- Cardiac 123I-MIBG Imaging for Clinical Decision Making: 22-Year Experience in Japan
- Assessment of cardiac sympathetic activity by MIBG imaging in patients with heart failure: a clinical appraisal
- Prognostic Value of Serial Cardiac 123I-MIBG Imaging in Patients with Stabilized Chronic Heart Failure and Reduced Left Ventricular Ejection Fraction
- Predicting the Need for an Implantable Cardioverter Defibrillator Using Cardiac Metaiodobenzylguanidine Activity Together with Plasma Natriuretic Peptide Concentration or Left Ventricular Function
- Additive Effects of Spironolactone and Candesartan on Cardiac Sympathetic Nerve Activity and Left Ventricular Remodeling in Patients with Congestive Heart Failure
- Long-Term Nicorandil Therapy Improves Cardiac Sympathetic Nerve Activity After Reperfusion Therapy in Patients with First Acute Myocardial Infarction
- Effects of Intravenous Atrial Natriuretic Peptide on Cardiac Sympathetic Nerve Activity and Left Ventricular Remodeling in Patients With First Anterior Acute Myocardial Infarction
- Effects of torasemide on cardiac sympathetic nerve activity and left ventricular remodelling in patients with congestive heart failure
- Comparative effects of valsartan and enalapril on cardiac sympathetic nerve activity and plasma brain natriuretic peptide in patients with congestive heart failure
- Effects of candesartan on cardiac sympathetic nerve activity in patients with congestive heart failure and preserved left ventricular ejection fraction
- Dobutamine Stress 99mTc-Tetrofosmin Quantitative Gated SPECT Predicts Improvement of Cardiac Function After Carvedilol Treatment in Patients with Dilated Cardiomyopathy
- Effects of Intravenous Atrial Natriuretic Peptide on Cardiac Sympathetic Nerve Activity in Patients with Decompensated Congestive Heart Failure