


Abstract
The purpose of this study was to evaluate the ability of 18F-FDG PET to characterize adrenal lesions in patients with proven or suspected cancers. Methods: A retrospective analysis was performed on 50 adrenal lesions in 41 patients, whose PET scans were done to evaluate the primary or metastatic disease. CT had shown 50 adrenal lesions in 41 patients and MRI had revealed 13 lesions in 10 patients. There were 34 patients with proven malignancy (28 lung cancer, 3 thyroid cancer, 2 colorectal cancer, and 1 lymphoma) and 7 with lung nodules. Of the 50 lesions, 18 were eventually determined to be malignant either by histopathology (n = 7) or by follow-up (n = 11). The remaining 32 lesions were proven or assumed to be benign by histopathology (n = 4) or clinical follow-up (n = 28). Unlike previously published reports, PET was interpreted as positive if the uptake was equal to or greater than that of the liver. Results: No malignant lesion yielded a negative result on PET. Most lesions (13/18) showed significantly higher FDG uptake than that of the liver. In the remaining 5 lesions (2 metastases from neuroendocrine tumor, 2 early metastases, and 1 necrotic metastasis), FDG uptake was equal to or slightly higher than that of the liver. Of the 32 benign lesions, there were 2 lesions with uptake equal to or slightly higher than that of the liver, 3 with uptake less than the liver but more than the background, and 27 with uptake of the background. MRI identified 3 of the 13 lesions as false-positives but FDG PET correctly identified all 3 as benign. The other 10 adrenal lesions accurately diagnosed by MRI were also characterized by PET. FDG PET for characterization of adrenal lesions showed a sensitivity of 100%, a specificity of 94%, and an accuracy of 96%. Conclusion: FDG PET showed excellent diagnostic performance in differentiating adrenal lesions detected on CT or MRI. Because FDG PET has the additional advantage of evaluating the primary lesions as well as metastases, it could be cost-effective and the modality of choice for the characterization of adrenal lesions, especially in patients with malignancy.
Because adrenal adenomas are relatively common (2%–9%) in the general population, an incidental detection of such lesions poses a diagnostic challenge in patients with malignancy (1–4). Among high-resolution anatomic imaging techniques, CT is used as the first-line diagnostic modality for screening and determining the nature of the adrenal lesions, and MRI is often performed to further characterize indeterminate masses seen on CT. Recently, 18F-FDG PET has also shown great potential in differentiating malignant from benign adrenal lesions in patients with proven malignancy or in patients with incidentally detected adrenal tumors on CT or MRI studies (5–7).
With more experience in the evaluation of the adrenal lesions using FDG PET, it has been noted that benign adrenal adenomas can have increased FDG uptake leading to false-positive results on PET (6). In previous studies, the scan was interpreted as positive if the FDG uptake was greater than background or blood-pool activity in the adrenal lesion. Unlike previously published reports, we have adopted different diagnostic criteria to interpret PET studies (6,7). There might be a potential advantage to this approach by increasing the specificity of FDG PET without compromising its sensitivity. This study was undertaken to evaluate the ability of FDG PET and these new criteria in characterizing adrenal lesions in patients with proven or suspected cancers.
MATERIALS AND METHODS
Fifty adrenal lesions detected on CT scans from 41 patients (17 women, 24 men; age range, 42–84 y; mean age, 63 ± 12 y), on whom PET scans were obtained to evaluate the primary or metastatic disease, were retrospectively reviewed for this study. In 10 patients, MRI done to characterize the lesions seen on CT revealed 13 lesions. Because not all MRI studies were available for our review, the interpretation of magnetic resonance images was based on reports from referring physicians. There were 34 patients with proven malignancy (28 lung cancer, 3 thyroid cancer, 2 colorectal cancer, and 1 lymphoma) and 7 with indeterminate lung nodules. A final diagnosis of the adrenal lesions was based on a histopathologic examination of the specimen or clinical follow-up. An adrenal lesion detected on follow-up imaging was considered benign if no change had been seen in the size of the lesion for at least 6 mo, and it was considered malignant if the size of the adrenal lesion had increased or decreased after treatment or a new adrenal lesion had developed.
PET imaging was performed using a C-PET scanner (ADAC UGM, Philadelphia, PA). This scanner acquires data in 3-dimensional mode without septa. The intrinsic spatial resolution of the system is 5-mm full width at half maximum in the center of the field of view. The patients fasted for at least 4 h and the serum glucose level was < 140 mg/dL in all patients. PET scanning was initiated 60 min after intravenous administration of 2.516 MBq (0.068 mCi)/kg of FDG. Sequential overlapping scans were acquired to cover the neck, chest, abdomen, and pelvis. Transmission scans using a 137Cs point source were interleaved between the multiple emission scans to correct for nonuniform attenuation correction (8). The images were reconstructed using ordered subset expectation maximization, an iterative reconstruction algorithm (9).
FDG PET images were qualitatively evaluated on a high-resolution computer screen by 2 nuclear medicine physicians who were unaware of other clinical or imaging information. Special attention was paid to FDG uptake in the adrenal glands. In cases of disagreement, final decision was made by consensus. The scan was considered negative for malignancy if the degree of FDG uptake in the adrenal region was less than the uptake in the liver at the same coronal section. Conversely, it was considered positive if the uptake in the lesion was equal to or greater than uptake in the liver. On the basis of past experience, we have noted that visual assessment of the suspected lesions may be just as effective as semiquantitative analysis using the standardized uptake value (SUV) in differentiating active from inactive disorder. Therefore, the SUV was not used to differentiate a benign lesion from a malignant adrenal lesion. Furthermore, it was often difficult to generate a region of interest over the lesions that were not visualized on PET scan.
RESULTS
The size of the 50 lesions on CT scans ranged from 0.5 to 4.2 cm, with a mean size of 2 ± 1 cm. Of the 50 lesions, 18 were determined to be malignant by surgery (n = 3), percutaneous biopsy (n = 2), autopsy (n = 2), or follow-up (n = 11). All 18 malignant lesions showed positive FDG uptake on PET scans. Thirty-two lesions were known or subsequently proven to be benign by surgery (n = 2), percutaneous biopsy (n = 2), or follow-up for a period of time not less than 6 mo (n = 28). All except 2 benign lesions showed negative FDG uptake on PET scans (Table 1).
FDG PET Findings Versus Final Conclusions on Adrenal Lesions
Most malignant lesions (13/18) showed significantly higher FDG uptake than that of the liver (Fig. 1). In the remaining 5 lesions with FDG uptake equal to or slightly higher than that of the liver, there were 2 metastases from neuroendocrine tumor of the lung (Fig. 2), 2 early, small metastases from lung cancer that were not seen on previous CT scans, and 1 necrotic metastasis, also from lung cancer. Of the 32 benign lesions, there were 2 lesions with uptake equal to or slightly higher than that of the liver (Fig. 3), 3 with uptake greater than the background but less than the liver (Fig. 4), and 27 with uptake equal to that of the background. FDG PET for characterization of adrenal lesions showed a sensitivity of 100%, a specificity of 94%, and an accuracy of 96%.
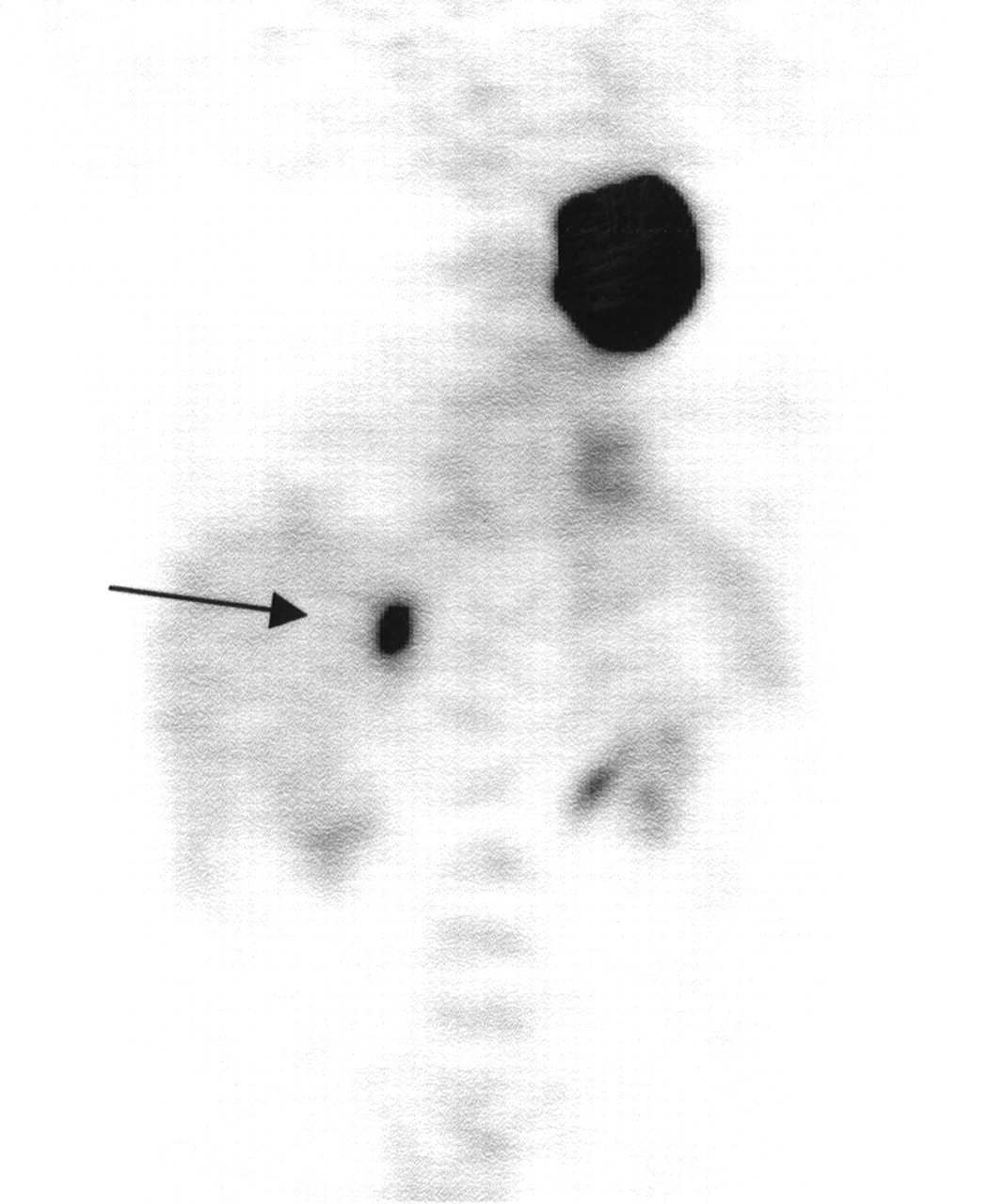
Coronal view of FDG PET shows intense FDG uptake in large primary cancer of left upper lung. Lesion in right adrenal gland (arrow) shows significantly higher FDG uptake than that of liver and was confirmed as metastasis from lung cancer by surgery.

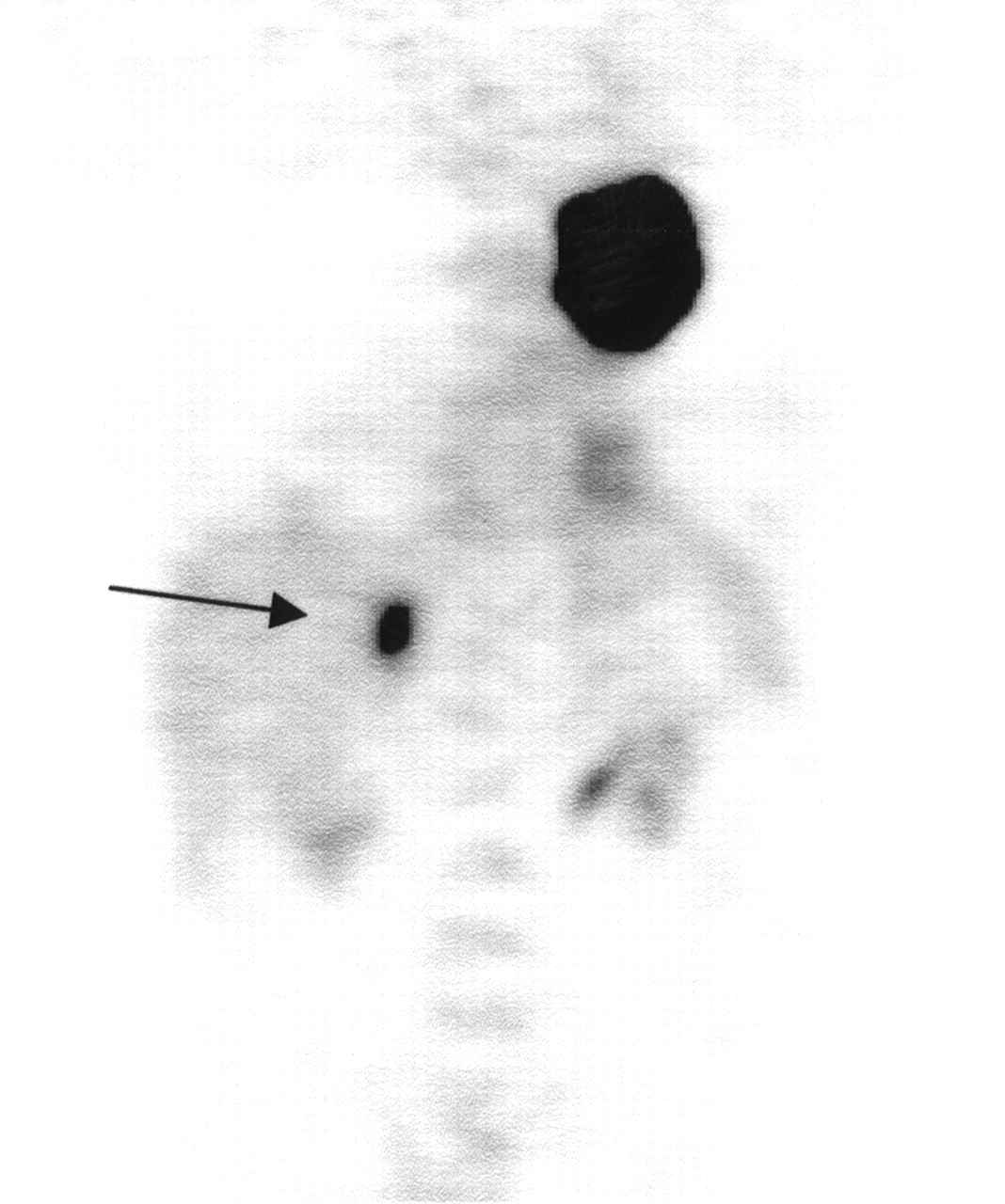
Coronal view of FDG PET shows small, round focus with FDG uptake equal to or slightly higher than liver in right adrenal gland (arrow). Patient has history of neuroendocrine tumor in right upper lobe of lung. Lesion in adrenal gland underwent surgery and was proven to be metastatic cancer with neuroendocrine differentiation.
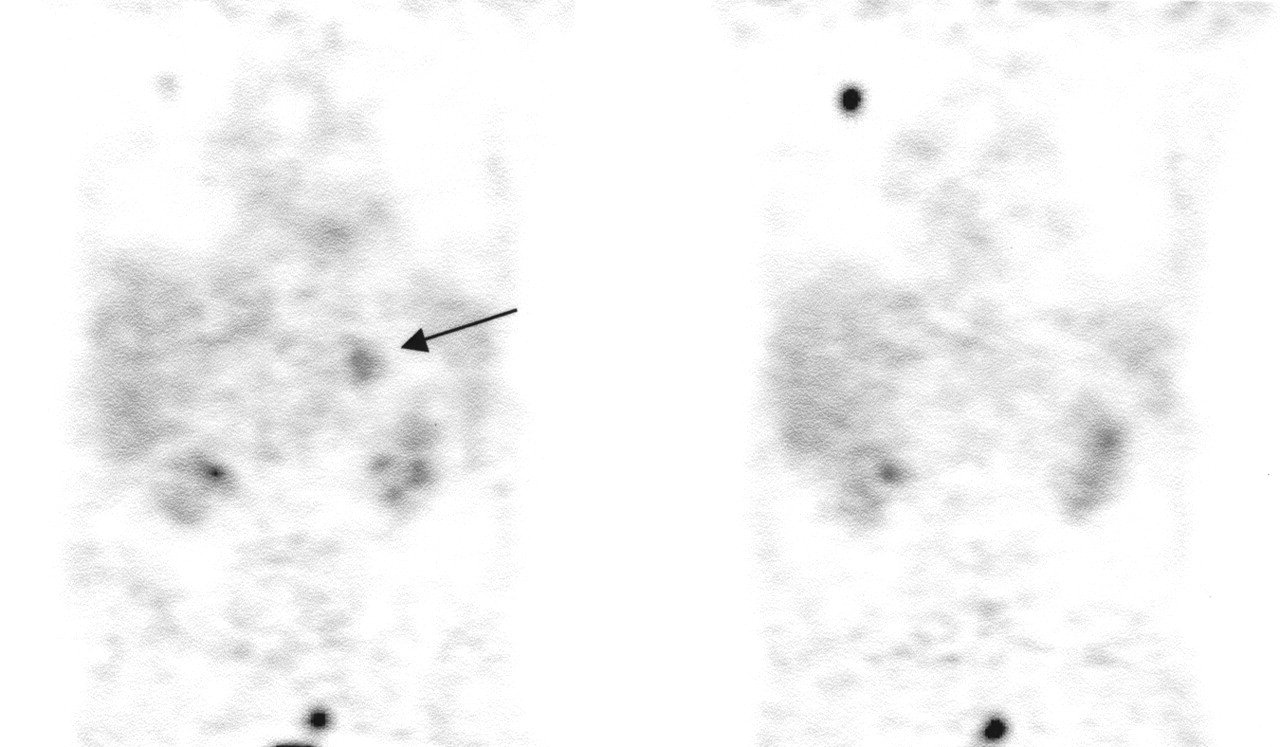
Patient with newly diagnosed lung cancer in right upper lung. Coronal views of FDG PET show focus of intense FDG uptake in right upper lung corresponding to lung cancer. There is another focus with FDG uptake slightly higher than that of liver in left adrenal gland (arrow). Lesion in adrenal gland was biopsied for staging purpose and turned out to be benign adenoma.

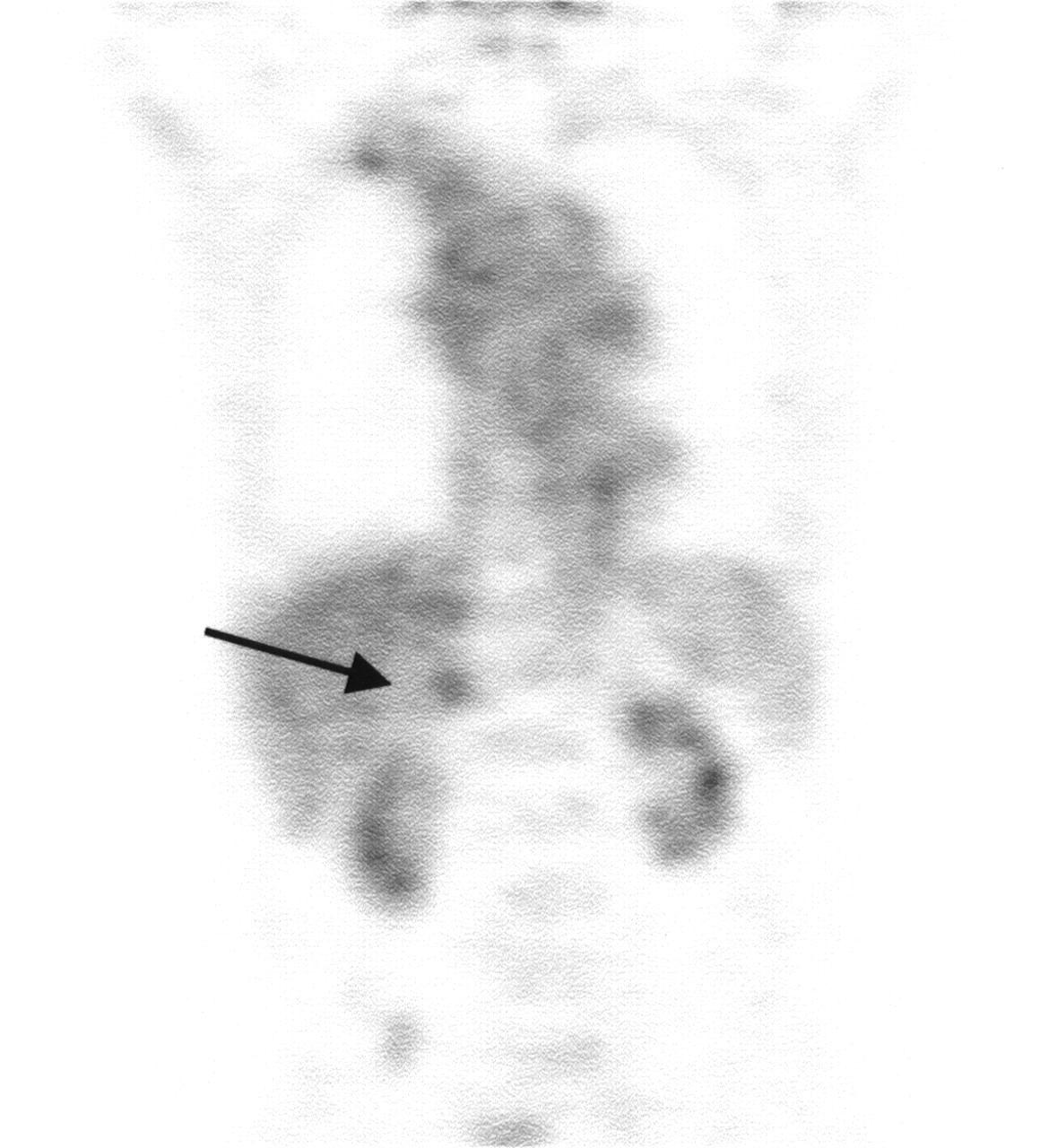
Patient with history of medullary thyroid cancer. Coronal view of FDG PET shows focal area with FDG uptake less than that of liver in left adrenal gland (arrow). Lesion measured 3.5 cm on CT scan and did not change for 15 mo on follow-up. MRI showed findings that are diagnostic of benign adenoma.
Using the criteria adopted in this study, excellent agreement was made between the 2 observers in the interpretation of FDG PET scans. For 2 of the 50 lesions, the 2 observers disagreed on the grade of the uptake of the adrenal lesions at initial reading. However, consensus between the observers was easily reached on these 2 lesions at the time of the second review.
Of 13 lesions in 10 patients on whom MRI was performed for further characterization of indeterminate adrenal lesions on CT, there were 4 true-positives, 6 true-negatives, and 3 false-positives. FDG PET accurately diagnosed all 13 lesions (Table 2). MRI interpretation based on reports from referring physicians had sensitivity, specificity, and accuracy of 67%, 100%, and 77%, respectively, for correctly identifying a benign lesion from a malignant lesion. MRI showed excellent specificity when characterizing a benign lesion. However, MRI criteria for differentiating benign from malignant lesions may differ among institutions. Because of the limited sample size of patients who underwent MRI and the lack of access to magnetic resonance images from different institutions in this study, the performance assessment of MRI might not be as accurate as that of FDG PET.
Results on 13 MRI Lesions in Comparison with FDG PET Results on Same Lesions
DISCUSSION
Approaches for diagnosis and management of adrenal lesions differ among institutions (10–14). Most adrenal masses are likely to be benign, even in patients with cancer (4,15). Therefore, it is essential to differentiate benign and nonfunctioning lesions from those with hormonally active or malignant lesions so that appropriate treatment strategies can be initiated.
CT scanning is considered most important in evaluating adrenal masses. Lipid within adenomas causes a low attenuation value on CT, and such an attenuation value has been extremely helpful in differentiating a benign adenoma from a malignant lesion (16–19). Delayed enhanced CT could help by analyzing the washout patterns seen in adrenal lesions. Adenomas may show mild enhancement and rapid washout, whereas metastases may show marked, fast enhancement and slower washout (20–22). Chemical shift MRI is most commonly used among different magnetic resonance techniques and appears to be highly accurate in the diagnosis of benign adenomas. Any lipid-containing tissue would show a signal loss caused by cancellation of the signal from fat and water. It should be noted, however, that rare adrenal cortical carcinomas or metastases from hepatoma, renal cell carcinoma, or liposarcoma could give the same lipid signal loss seen in adenomas (23–25). McNicholas et al. (26) reported excellent diagnostic performance using CT and MRI to identify intracellular lipid. In their study, 36% of adrenal masses were characterized by unenhanced CT scans and 60% more were characterized by MRI using a chemical shift sequence, leaving only 4% of the patients to undergo invasive percutaneous biopsy procedures.
Unlike CT and MRI, FDG PET is based on increased glucose metabolism in malignant lesions. Boland et al. (5) reported that FDG PET distinguished benign adrenal lesions from metastatic lesions with 100% sensitivity and specificity. Erasmus et al. (6) evaluated 33 adrenal masses in 27 patients with bronchogenic carcinomas. PET was interpreted as positive when FDG uptake in the adrenal mass was higher than background activity. The sensitivity for detecting metastasis was 100% and the specificity was 80%. In their prospective study, Maurea et al. (7) considered adrenal FDG uptake to be abnormal when it was higher than blood-pool and background activities. All malignant lesions showed abnormally increased uptake. In benign lesions, no abnormally increased FDG uptake was observed, except for 1 benign pheochromocytoma. It is known that most pheochromocytomas, either benign or malignant, are metabolically active and thus accumulate FDG, although uptake is found in a greater percentage of malignant than in benign pheochromocytomas (27).
We also encountered benign adenomas showing a variable degree of FDG uptake, which could cause false-positive results on PET. Therefore, we decided to use new criteria to interpret scans so that the specificity of FDG PET would improve without compromising sensitivity. Using these criteria, no malignant lesion showed a negative result, giving a sensitivity of 100%. In 5 of 18 malignant lesions, FDG uptake was only equal to or slightly higher than that of the liver. These included 2 metastases from neuroendocrine tumors, 2 early, small metastases, and 1 necrotic metastasis. As previously reported, a neuroendocrine tumor could have lower FDG uptake than typically is seen in a malignant tumor (28). The sizes of the lesions could explain why the early metastases and necrotic metastasis showed relatively less intense FDG uptake than most of the malignant lesions. Of the 32 benign lesions, there were 2 adenomas with uptake equal to or slightly higher than that of the liver. It is unknown why some adenomas show variable FDG uptake. Overall, we achieved the high specificity of FDG PET without compromising sensitivity by using these criteria.
Of the 13 lesions identified by MRI, 3 were false-positives, but FDG PET correctly identified all 3 false-positives as benign. The other 10 adrenal lesions accurately diagnosed by MRI were also characterized as such by PET. Hence, FDG PET can play a role in further differentiation of indeterminate adrenal masses on MRI. MRI was not performed for 2 lesions that were determined by FDG PET as being false-positive. Thus, we were not able to determine whether MRI could have correctly diagnosed these lesions.
Our results indicate that if a lesion shows FDG uptake less than that of the liver, or shows uptake that is significantly higher than the liver, the study can be interpreted with high confidence unless the patient has pheochromocytoma, which can be excluded by biochemical markers. If the lesion in the adrenal gland shows uptake equal to or slightly higher than that of the liver on FDG PET, the study can be read as indeterminate because either benign or malignant lesions can show this degree of FDG uptake. In this situation, an additional imaging study should be performed for further characterization of the lesion, especially when it is the only area of suspicious metastasis identified through an FDG PET scan.
CONCLUSION
FDG PET showed excellent diagnostic performance in differentiating malignant from benign adrenal lesions in patients with proven or suspected malignancy. The additional advantage of imaging the whole body could make FDG PET the diagnostic modality of choice for the evaluation of adrenal lesions in patients with cancer. However, prospective studies are needed to further validate the role of FDG PET in characterizing adrenal lesions. Considering the outstanding specificity of MRI for adrenal adenomas, this technique can play a role in further differentiation of indeterminate lesions on FDG PET.
Footnotes
Received Apr. 16, 2001; revision accepted Aug. 21, 2001.
For correspondence or reprints contact: Abass Alavi, MD, 110 Donner Bldg., Division of Nuclear Medicine, Hospital of the University of Pennsylvania, 3400 Spruce St., Philadelphia, PA 19104.
REFERENCES
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Management of incidental adrenal tumours
- Appropriate Use Criteria for 18F-FDG PET/CT in Restaging and Treatment Response Assessment of Malignant Disease
- Assessment of incidental and clinically unsuspected fluorodeoxyglucose-avid foci detected on oncological positron emission tomography/CT
- Utilisation of combined 18F-FDG PET/CT scan for differential diagnosis between benign and malignant adrenal enlargement
- AME Position Statement on adrenal incidentaloma
- Guidelines on the radical management of patients with lung cancer
- Management of Adrenocortical Carcinoma
- Adrenal incidentaloma: evaluation and management
- PET/CT assessment of clinically unsuspected, incidental FDG-avid lesions in oncological patients
- Adrenal Masses in the Cancer Patient: Surveillance or Excision
- PET Evaluation of Lung Cancer
- 18F-FDG PET/CT in the Evaluation of Adrenal Masses
- Management of patients with adrenal cancer: recommendations of an international consensus conference
- 18F-FDG PET in Evaluation of Adrenal Lesions in Patients with Lung Cancer
- Characterization of the Normal Adrenal Gland with 18F-FDG PET/CT
- Imaging of Adrenal Incidentalomas with PET Using 11C-Metomidate and 18F-FDG
- American Society of Clinical Oncology Treatment of Unresectable Non-Small-Cell Lung Cancer Guideline: Update 2003
- Application of a Neural Network to Improve Nodal Staging Accuracy with 18F-FDG PET in Non-Small Cell Lung Cancer
- PET in the follow-up of differentiated thyroid cancer