


Visual Abstract

Abstract
In patients with prostate cancer scheduled for systemic treatment, being overweight is linked to prolonged overall survival (OS), whereas sarcopenia is associated with shorter OS. We investigated fat-related and body composition parameters in patients undergoing prostate-specific membrane antigen (PSMA)–directed radioligand therapy (RLT) to assess their predictive value for OS. Methods: Body mass index (BMI, in kg/m2) and CT-derived body composition parameters (total, subcutaneous, visceral fat area, and psoas muscle area at the L3–L4 level) were determined for 171 patients scheduled for PSMA-directed RLT. After normalization for stature, the psoas muscle index was used to define sarcopenia. Outcome analysis was performed using Kaplan–Meier curves and Cox regression including fat-related and other clinical parameters (Gleason score, C-reactive protein [CRP], lactate dehydrogenase [LDH], hemoglobin, and prostate-specific antigen levels). The Harrell C-index was used for goodness-of-fit analysis. Results: Sixty-five patients (38%) had sarcopenia, and 98 patients (57.3%) had increased BMI. Relative to the 8-mo OS in normal-weight men (BMI < 25), overweight men (25 ≥ BMI > 30) and obese men (BMI ≥ 30) achieved a longer OS of 14 mo (hazard ratio [HR], 0.63; 95% CI, 0.40–0.99; P = 0.03) and 13 mo (HR, 0.47; 95% CI, 0.29–0.77; P = 0.004), respectively. Sarcopenia showed no impact on OS (11 vs. 12 mo; HR, 1.4; 95% CI, 0.91–2.1; P = 0.09). Most of the body composition parameters were tightly linked to OS on univariable analyses, with the highest C-index for BMI. In multivariable analysis, a higher BMI (HR, 0.91; 95% CI, 0.86–0.97; P = 0.006), lower CRP (HR, 1.09; 95% CI, 1.03–1.14; P < 0.001), lower LDH (HR, 1.08; 95% CI, 1.03–1.14; P < 0.001), and longer interval between initial diagnosis and RLT (HR, 0.95; 95% CI, 0.91–0.99; P = 0.02) were significant predictors of OS. Conclusion: Increased fat reserves assessed by BMI, CRP, LDH, and interval between initial diagnosis and RLT, but not CT-derived body composition parameters, were relevant predictors for OS. As BMI can be altered, future research should investigate whether a high-calorie diet before or during PSMA RLT may improve OS.
With more than 1.4 million new cases globally, prostate cancer (PC) is a major health burden (1), and androgen deprivation therapy alone or in combination with androgen receptor–targeted agents or chemotherapy is essential for treating patients with metastatic PC (2). Therapeutic options for evolving tumor biology leading to a castration-resistant tumor stage are still limited but include androgen receptor–targeted agents, for example, abiraterone and enzalutamide (3,4), or taxane-containing chemotherapies (5,6). In recent years, prostate-specific membrane antigen (PSMA)–directed radioligand therapy (RLT) has penetrated the clinical arena, demonstrating remarkable outcome benefits (7–9). For instance, the prospective VISION trial reported on a relevant improvement in overall survival (OS) when added to standard care (10), leading to recent U.S. Food and Drug Administration approval (11).
First-line therapeutic regimens used in hormone-sensitive stages, including androgen deprivation therapy, can influence body composition in PC (12–15). Body composition parameters were also tightly linked to outcome for men with castration-resistant PC (CRPC) (16). For instance, several studies have reported that overweight or obesity is favorable for prognosis in patients with CRPC, such as those receiving taxane-based chemotherapy (17–19), whereas high visceral fat is suspected of being a predictor of worse outcome (19–21). Moreover, defined as gradual skeletal muscle loss, sarcopenia still has a debatable impact on disease progression under second-line therapies such as docetaxel (19,22,23).
In the present study, the prevalence of sarcopenia and obesity in men with PSMA-targeted RLT using [177Lu]Lu-PSMA I&T was assessed. We also aimed to determine the impact of fat-related and other CT-derived body composition parameters, as well as laboratory values and clinical characteristics, on outcome.
MATERIALS AND METHODS
Patient Cohort
One hundred seventy-one CRPC patients treated with [177Lu]Lu-PSMA I&T were included in this investigation. The local ethics committee waived the need for further approval of this retrospective study (waiver 20210422 04). All patients gave written informed consent for the conducted procedures. Parts of this cohort have previously been reported (24–28), without focusing on fat-related and body composition parameters and their predictive performance for OS.
Treatment with [177Lu]Lu-PSMA I&T
The synthesis of [177Lu]Lu-PSMA I&T was previously described (28). Details on the standardized pretherapy work-up in our department were also previously published (24). In brief, blood panels including prostate-specific antigen (PSA) level, C-reactive protein (CRP), lactate dehydrogenase (LDH), and hemoglobin were collected at cycle 1, day 1, and the patient’s history was available in an electronic health database. Information on processing of blood samples and dedicated laboratory analyses was previously published (28). For treatment, we administered 6.0 GBq of [177Lu]Lu-PSMA I&T every 8 wk (maximum, 9 cycles per patient).
Assessment of Body Composition
As part of serial hybrid imaging, PSMA-directed PET along with respective CT was performed before initiation of PSMA-directed RLT, defined as baseline. CT images were assessed on a workstation equipped with syngo.via imaging software, version VB60A_HF01 (Siemens Healthineers AG). The scans were evaluated by an observer with 4 y of experience in reading PSMA-targeted PET/CT, who underwent a previous training session, and were reviewed by experienced readers, if needed. The hybrid imaging protocol was previously published (29).
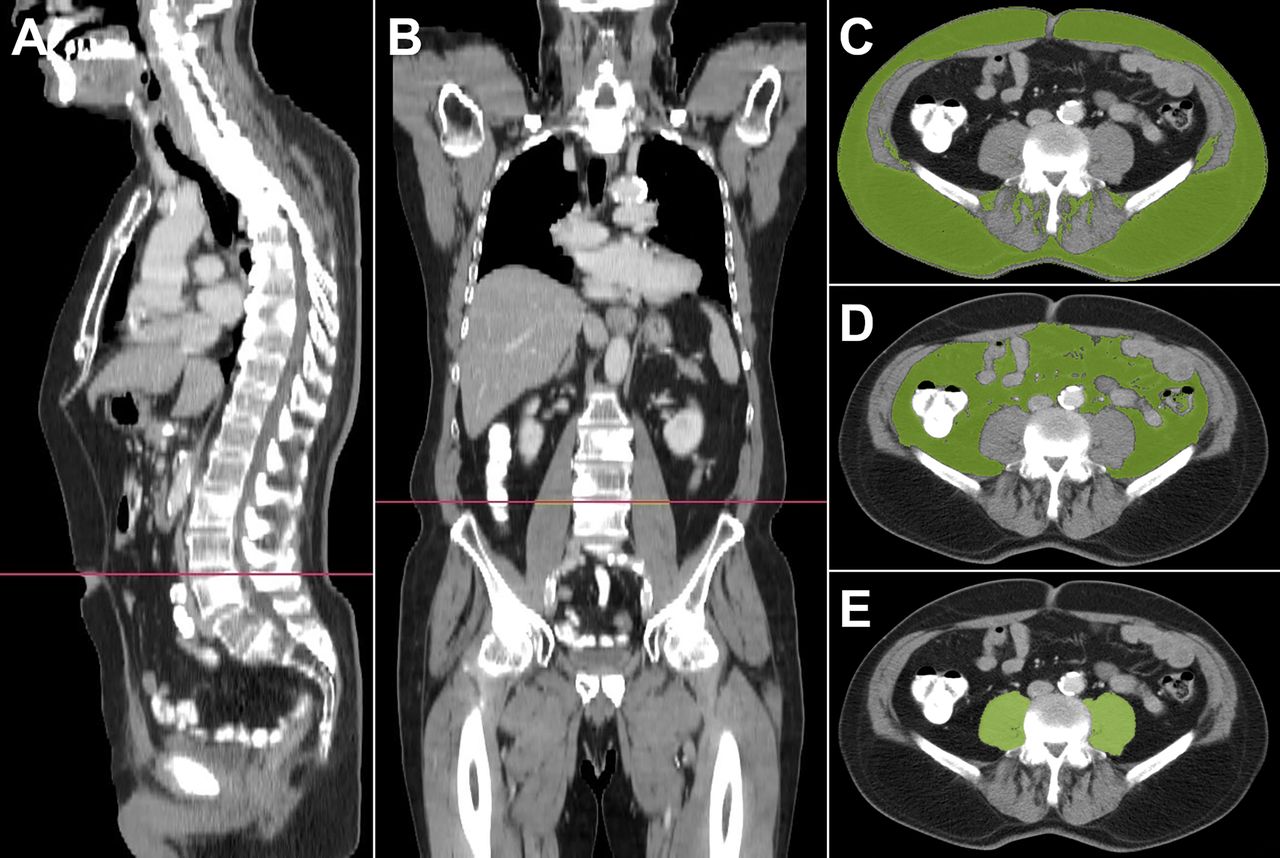
CT-based assessment of body composition was performed as previously described (23). Cross-sectional areas of different tissue compartments, including total, subcutaneous, and visceral fat areas, as well as the psoas muscle area, were segmented on axial CT scans at the level of the third and fourth lumbar vertebrae (L3–L4) by manually drawing a region of interest for each compartment and applying the respective tissue-typical Hounsfield unit threshold: −190 to −30 for adipose tissue and −29 to +150 for muscle tissue (Fig. 1). Body mass index (BMI, in kg/m2), visceral fat–to–subcutaneous fat ratio, and subcutaneous fat–to–muscle ratio were calculated. BMI was classified as normal (<25), preobese (25 ≤ BMI < 30), or obese (≥30) (30). Subcutaneous fat area, visceral fat area, and psoas muscle area were then normalized for slice thickness, and all of those parameters were also normalized for stature to derive respective indices (subcutaneous fat index, visceral fat index, and psoas muscle index [PMI], in cm2/m2). Sarcopenia was then defined as an L3 PMI of less than 5.7 cm2/m2 according to the literature (22,23).

Example of 68-y-old patient with PC. As part of hybrid imaging (PSMA PET/CT), body composition of CT was investigated. Sagittal (A), coronal (B), and axial (C–E) CT images show segmentation of separate tissue compartments at level of third and fourth lumbar vertebrae (L3–L4) applying different Hounsfield units: subcutaneous fat cross-sectional area (−190 to −30) (C), visceral fat cross-sectional area (−190 to −30) (D), and psoas muscle area (−29 to +150) (E).
Statistical Analyses
We used GraphPad Prism, version 9.3.0 (GraphPad Software), for statistical analyses. Descriptive data are presented as median and range. We defined OS as the interval from the day of the first cycle until the day of death (presented as median). Univariable Cox regression was performed with all parameters for OS after exclusion of outliers (n = 7). For multivariable analysis, we then selected significant parameters from the univariable analysis. Parallel inclusion of multiple body composition parameters in 1 model was not possible because of multicollinearity (e.g., BMI + weight + total fat area or psoas muscle area + PMI). Thus, we decided for the relevant clinical parameter BMI (as a fat-related parameter) and PMI (as an established marker of sarcopenia) in the multivariable analyses (22,23). Different Cox regression models were compared with each other and with a null model (without any parameter) using the Akaike information criterion (31) and the Harrell C-statistic (32). In this regard, a lower Akaike information criterion and a higher Harrell C value indicate a better-fit model (31,32). The hazard ratio (HR) of death and 95% CI are presented. Kaplan–Meier curves and log-rank comparison were also calculated to illustrate different survivals between high- and low-risk patients. We present median survival in months, with the HR of death and 95% CI. A P value of less than 0.05 was considered statistically significant.
RESULTS
Patient Characteristics
The median age of the 171 included patients was 71 y (range, 46–95 y), and the median Gleason score at original diagnosis was 9 (range, 5–10). The patients received a median of 2 systemic treatment lines before PSMA RLT, with 71%, 65%, 68%, and 8% of patients receiving taxane-based chemotherapy, enzalutamide, abiraterone, and 223Ra, respectively. The median baseline laboratory values were 158 ng/mL (range, 0.07–5,000 ng/mL), 0.56 mg/dL (range, 0.02–29.34 mg/dL), 268 U/L (range, 118–1,800 U/L), and 11.6 g/dL (range, 6.0–16.1 g/dL) for PSA, CRP, LDH, and hemoglobin, respectively. Men underwent a median of 2 cycles (range, 1–9) of RLT with [177Lu]Lu-PSMA I&T. The median follow-up was 7 mo (range, 1–53 mo), and the median OS was 11 mo. Ninety-four patients died during follow-up. At baseline, 73 patients (42.7%) showed a normal BMI, 56 patients (32.7%) were preobese, and the remaining 42 patients (24.6%) were obese. Sarcopenia was recorded in 65 patients (38%; Table 1). Table 1 provides a comprehensive overview of the baseline patient characteristics.
Patient Characteristics
Identification of Patients Prone to Shorter Survival Through BMI but Not CT-Derived Body Composition Parameters
Univariable Cox regression for different body composition parameters revealed total fat area (per 50 cm2; HR, 0.93; 95% CI, 0.88–0.99; P = 0.03), psoas muscle area (HR, 0.95; 95% CI, 0.91–0.99; P = 0.02), PMI (HR, 0.85; 95% CI, 0.75–0.97; P = 0.01), visceral fat index (HR, 0.99; 95% CI, 0.99–1.00; P = 0.05), BMI (HR, 0.91; 95% CI, 0.86–0.96; P = 0.001), and weight (HR, 0.97; 95% CI, 0.96–0.99; P = 0.005) as significantly associated with OS. Sarcopenia, however, failed to reach significance (P = 0.14, Table 2). Investigating clinical parameters, CRP (HR, 1.16; 95% CI, 1.11–1.20; P = 0.001), LDH (per 50 U/L; HR, 1.16; 95% CI, 1.11–1.20; P = 0.001), hemoglobin (HR, 0.71; 95% CI, 0.61–0.81; P < 0.001), PSA (HR, 1.01; 95% CI, 1.00–1.03; P = 0.04), and interval between initial diagnosis and RLT (per year; HR, 0.94; 95% CI, 0.89–0.98; P = 0.003) were significant predictors of OS. Age and Gleason score, however, were not significant (P ≥ 0.31). However, the largest improvements in the models compared with a model without parameters (null model) were seen for BMI among the body composition and fat parameters (Akaike information criterion, 728.5 vs. 738.2 in the null model; C-index, 0.64).
Univariable Cox Regression Model
The multivariable analysis included BMI, CRP, LDH, interval between initial diagnosis and RLT, hemoglobin, baseline PSA value, and PMI (C-index, 0.80). CRP (HR, 1.09; 95% CI, 1.03–1.14; P < 0.001), LDH (per 50 U/L; HR, 1.08; 95% CI, 1.03–1.14; P < 0.001), interval between initial diagnosis and RLT (per year; HR, 0.95; 95% CI, 0.91–0.99; P = 0.02), and BMI (HR, 0.91; 95% CI, 0.86–0.97; P = 0.006) remained significant predictors of OS (Table 3).
Multivariable Cox Regression
Relative to 8 mo in patients with a normal BMI, preobese men achieved a longer OS of 14 mo in Kaplan–Meier analysis (HR, 0.63; 95% CI, 0.40–0.99; P = 0.03). Similar results were recorded for obese subjects (OS, 13 mo; HR, 0.47; 95% CI, 0.29–0.77; P = 0.004 vs. normal BMI; Fig. 2). There was no significant difference in OS between preobese and obese subjects (P = 0.39). Patients with sarcopenia at baseline did not have a shorter OS than patients without sarcopenia (11 vs. 12 mo; HR, 1.4; 95% CI, 0.91–2.1; P = 0.09; Fig. 3).

Kaplan–Meier curves and log rank comparisons for patients with and without sarcopenia and treated with RLT, revealing no relevant differences in OS for men allocated to either group.

Kaplan–Meier curves and log rank comparisons for patients treated with RLT and stratified according to their BMI. Higher BMI was associated with longer median survival, in particular for obese subjects with BMI ≥ 30 kg/m2. *Compared with patients with BMI < 25 kg/m2.
DISCUSSION
Investigating fat-related and CT-derived body composition parameters along with other clinical parameters of 171 PC patients scheduled for RLT, we found that a higher BMI of at least 25 kg/m2, a lower CRP, a lower LDH, and a longer interval between initial diagnosis and RLT were significant predictors for prolonged OS. The prevalence of sarcopenia or any other CT-derived body composition parameter, however, had no relevant impact on OS in a multivariable analysis.
In the present cohort, the occurrence of sarcopenia (38%) was comparable to that in prior studies for patients scheduled for docetaxel chemotherapy (19,22). However, this prevalence is higher than reported for people aged 60–70 y in the United States and parts of Europe, with those values ranging from 5% to 13% (33). As a possible explanation, this difference may be caused by an advanced tumor biology as included in the present study, which can result in increased catabolism and malnutrition (34). In addition, RLT patients have usually undergone extensive pretreatment with androgen deprivation therapy, enzalutamide/abiraterone, and chemotherapy with docetaxel, which may also result in loss of skeletal muscle. In our investigated mCRPC patients treated with [177Lu]Lu-PSMA I&T, sarcopenia was not associated with OS, as is in line with the findings on subjects scheduled for other last-line therapies such as docetaxel chemotherapy (19). Of note, Ohtaka et al. reported a shortened OS in sarcopenic patients undergoing taxane-based chemotherapy (22). Thus, given those varying results depending on the treatment regimen, further studies are needed to corroborate our findings of no relevant impact of muscle loss on outcome by investigating other PSMA-targeted therapeutic compounds, such as [177Lu]Lu-PSMA-617 or rhPSMA-7.3 (10,35).
Investigating a large single-center experience with men treated with [177Lu]Lu-PSMA-I&T to date, we found that most of the body composition parameters were tightly linked to OS on univariable analyses, thereby demonstrating their clinical relevance in patients treated with RLT. In this regard, a rather time-consuming assessment of CT-derived body composition parameters yielded comparable results to BMI. The latter parameter, however, is easily obtainable, for example, on a first-time visit when taking the patient’s history before initiation of RLT.
In addition, BMI also achieved the highest C-index of all body composition parameters, further emphasizing the importance of this parameter in clinical routine to identify high-risk individuals experiencing treatment failure. On multivariable analysis including other relevant clinical parameters, BMI then again remained a significant predictor of OS along with CRP, LDH, and interval between initial diagnosis and RLT, whereas PMI as a CT body composition parameter failed to reach significance (Table 3). In this regard, PMI may still be prone to observer bias, but BMI as an easily obtainable clinical variable can be recorded in a standardized fashion on a first visit for RLT. Those considerations are further fueled by the fact that the recent Food and Drug Administration approval may increase the number of men anticipated for PSMA-directed RLT in the near future (36), thereby not allowing for laborious CT assessments in a busy theranostic practice. In this regard, we found that patients with a BMI of more than 25 kg/m2 showed a significantly longer OS, which corroborates previous results for CRPC patients (17,18), in particular when treated with standard docetaxel chemotherapy (19,21).
As a possible explanation, patients with higher BMIs have greater fat reserves, thereby resisting tumor-associated cachexia for a substantially longer time after starting PSMA RLT. As such, this observation may have further clinical implications, as future studies may include high-calorie diet protocols before initiation of RLT or on repeated cycles, particularly when other therapies such as docetaxel have already been applied. In this regard, the observed impact of body habitus on OS is a variable that could be modified by the referring treating physician, whereas all other clinical variables that remained significant in multivariate analyses (including blood-based values or interval between initial diagnosis and RLT) cannot be modified. Nonetheless, the most appropriate dietary control would then have to be defined, as preclinical studies have reported stronger PC growth on high-fat than high-carbohydrate diets in murine studies (37). In this regard, our study may then also pave the way for future investigations, which should assess whether underweight patients scheduled for RLT may be at higher risk for treatment failure and whether those high-risk individuals may benefit from such modified dietary protocols.
Similar to previous studies, other clinical parameters have reached significance on univariable regression analysis, including CRP, LDH, and interval between initial diagnosis and RLT (24,38,39). The assumption that patients with a high visceral fat–to–subcutaneous fat ratio exhibit shorter OS than patients with a low visceral fat–to–subcutaneous fat ratio (20,21) could not be verified in our cohort of patients undergoing RLT. Interestingly, relative to CRP, LDH, or hemoglobin, BMI or CT-derived body composition parameters such as total fat area, visceral fat area, and psoas muscle area predict OS to a lesser extent. This may be partially explained by an observer bias for CT assessment, in particular as blood-based biomarkers are analyzed following highly standardized protocols. Baseline PSA values also failed to reach significance in multivariable Cox regression. This, however, is in line with previous findings for predicting survival using [177Lu]Lu-PSMA-617 (40–42) and [177Lu]Lu-PSMA I&T (24,38).
This study has limitations, including its retrospective design and its not individually determined, but fixed activity, regimens. PSMA RLT is usually given 4–6 times (43). As a real-world dataset obtained from routine care, not all patients were able to complete all 4–6 cycles, explaining the drop-out rate of approximately 20% after every cycle. Another partial explanation is that when the first patients were included in this analysis, respective restrictions on the number of cycles were nonexistent, for example, because of the missing results of the Vision Trial (10). Nonetheless, the number of cycles is of importance, as this is also recommended by the respective guidelines (43), and thus, future investigations may include only subjects with no more than 6 cycles. Although previous studies have shown no relevant outcome differences in a matched-pair analysis comparing the 2 most widely used therapeutic radiotracers, [177Lu]Lu-PSMA I&T and [177Lu]Lu-PSMA-617 (25), future studies should determine the predictive performance of baseline BMI and body composition in other PSMA-targeted agents recently introduced for therapy, including [177Lu]Lu-rhPSMA-7.3 (35). Other studies may also incorporate sophisticated nomograms along with fat-related parameters to provide an even more refined selection of candidates who are likely to respond to treatment (44). Last, performance status, such as Eastern Cooperative Oncology Group status, should be investigated to determine the predictive value relative to BMI or CT-based body composition (45).
CONCLUSION
In CRPC patients scheduled for RLT, patients with higher BMIs showed longer OS in multivariable analyses, whereas CT-derived body composition parameters reached significance only in univariate analyses. BMI as an easily obtainable parameter was also predictive of survival, along with blood-based parameters (CRP and LDH) and time between diagnosis and initiation of RLT. Although the latter clinical variables cannot be modified by the referring physician, future studies should determine whether a preceding high-calorie diet in individuals with lower fat reserves may also improve outcome.
DISCLOSURE
This work was supported by the IZKF Wuerzburg (grant Z-02/85 to Philipp Hartrampf). Rudolf Werner and Andreas Buck received speaker honoraria from Novartis (Triple A). No other potential conflict of interest relevant to this article was reported.
KEY POINTS
QUESTION: How do body composition parameters (e.g., fat parameters, BMI, or sarcopenia) influence OS in CRPC patients undergoing PSMA RLT?
PERTINENT FINDINGS: In PC patients scheduled for RLT, sarcopenia is present in 38% of cases but is not associated with survival. However, increased fat reserves, as determined by BMI, are associated with a better outcome.
IMPLICATIONS FOR PATIENT CARE: Future studies should investigate whether alteration of BMI before treatment initiation may improve OS.
ACKNOWLEDGMENT
We thank Dr. Dirk Mügge (Adelebsen) for his statistical advice.
Footnotes
Published online Jun. 8, 2023.
- © 2023 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication December 29, 2022.
- Revision received March 21, 2023.
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.