


Visual Abstract

Abstract
Our objective was to evaluate the prognostic value of somatostatin receptor tumor burden on 68Ga-DOTATOC PET/CT in patients with well-differentiated (WD) neuroendocrine tumors (NETs). Methods: We retrospectively analyzed the 68Ga-DOTATOC PET/CT scans of 84 patients with histologically confirmed WD NETs (51 grade 1, 30 grade 2, and 3 grade 3). For each PET/CT scan, all 68Ga-DOTATOC–avid lesions were independently segmented by 2 operators using a customized threshold based on the healthy liver SUVmax (LIFEx, version 5.1). Somatostatin receptor–expressing tumor volume (SRETV) and total lesion somatostatin receptor expression (TLSRE = SRETV × SUVmean) were extracted for each lesion, and then whole-body SRETV and TLSRE (SRETVwb and TLSREwb, respectively) were defined as the sum of SRETV and TLSRE, respectively, for all segmented lesions in each patient. Time to progression (TTP) was defined as the combination of disease-free survival in patients undergoing curative surgery (n = 10) and progression-free survival for patients with unresectable or metastatic disease (n = 74). TTP and overall survival were calculated by Kaplan–Meier analysis, log-rank testing, and the Cox proportional-hazards regression model. Results: After a median follow-up of 15.5 mo, disease progression was confirmed in 35 patients (41.7%) and 14 patients died. A higher SRETVwb (>39.1 cm3) and TLSREwb (>306.8 g) correlated significantly with a shorter median TTP (12 mo vs. not reached; P < 0.001). In multivariate analysis, SRETVwb (P = 0.005) was the only independent predictor of TTP regardless of histopathologic grade and TNM staging. Conclusion: According to our results, SRETVwb and TLSREwb extracted from 68Ga-DOTATOC PET/CT could predict TTP or overall survival and might have important clinical utility in the management of patients with WD NETs.
- neuroendocrine tumors
- 68Ga-DOTATOC PET/CT
- tumor burden
- prognosis
- somatostatin receptor expressing tumor volume
- total lesion somatostatin receptor expression
Neuroendocrine neoplasms (NENs) are a group of tumors of common embryologic origin but leading to a variety of clinical presentations and prognosis. The most frequent sites are the gastroenteropancreatic tract and the bronchopulmonary system. Although relatively rare, NENs have had a greatly increasing incidence in the last 30 years, and the incidence is currently estimated at approximately 5 cases per 100,000 population per year (1). According to the World Health Organization classification (based on Ki-67 percentage or number of mitoses per high-power field), NENs range from well-differentiated (WD) neuroendocrine tumors (NETs) to poorly differentiated carcinomas (2).
PET/CT imaging with a 68Ga-DOTA–labeled somatostatin analog (SSTa) is the mainstay for in vivo evaluation of somatostatin receptor expression in NETs (3,4), and almost 90% of primary grade 1 or 2 gastroenteropancreatic NETs are PET-positive because of the high somatostatin receptor expression (5). In clinical practice, 68Ga-DOTA-SSTa PET/CT has become the gold standard in the diagnosis and management of WD NETs, as it plays a major role in tumor characterization, in the assessment of disease extension, and in proper selection of patient candidates for peptide receptor radionuclide therapy (6,7). The prognostic value of 68Ga-DOTA-SSTa PET/CT imaging has been widely assessed in the literature but has been focused mainly on semiquantitative parameters such as SUV (8,9).
In several tumor models over the last few years, metabolic tumor burden on 18F-FDG PET has shown major prognostic value compared with semiquantitative parameters. Calculation of metabolic tumor burden integrates the volume of metabolically active tumor, expressed by metabolic tumor volume, and total lesion glycolysis, which is the product of SUVmean and metabolic tumor volume. Two studies (10,11) have interestingly demonstrated the prognostic utility of somatostatin receptor tumor burden (SRTB) in patients with WD NETs, obtained by measuring whole-body total lesion somatostatin receptor expression (TLSREwb) and whole-body somatostatin receptor–expressing tumor volume (SRETVwb) from 68Ga-DOTATATE PET/CT images.
Hence, the objective of this study was to evaluate the prognostic value of SRTB extracted from 68Ga-DOTATOC PET/CT in a large cohort of patients with WD NETs.
MATERIALS AND METHODS
Population
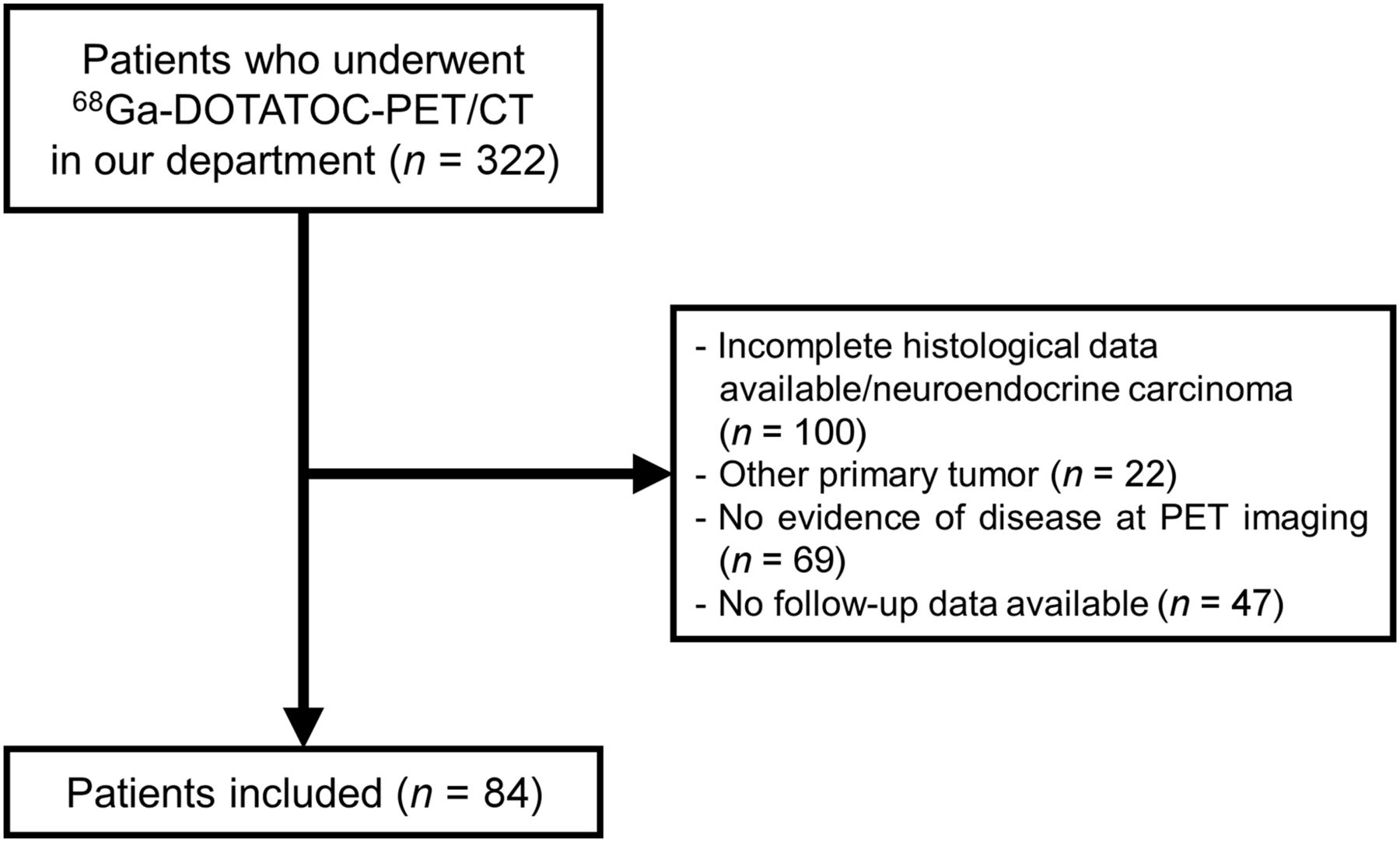
All patients (n = 322) consecutively referred for 68Ga-DOTATOC PET/CT to the Nuclear Medicine Division of “AOU Città della Salute e della Scienza,” from January 1, 2017, to January 4, 2020, were retrospectively evaluated and included if they had histologically proven grades 1–3 WD NETs, gastroenteropancreatic or bronchopulmonary NETs or an unknown primary site, 68Ga-DOTATOC PET with at least 1 positive lesion, and follow-up at least 6 mo after PET. Exclusion criteria were an age of less than 18 y, incomplete histologic data, a neuroendocrine carcinoma, concomitant metastatic neoplasia other than NET, or negative findings on 68Ga-DOTATOC PET/CT. The CONSORT diagram of the study (Consolidated Standards of Reporting Trials) is presented in Figure 1.

CONSORT diagram of study.
The study was conducted in accordance with the ethical principles set forth in the Declaration of Helsinki and was approved by the local ethical committee (approval 0004004; protocol: “NET PET Tumor Burden Study”). All enrolled patients signed an informed consent form.
Data on age, sex, TNM stage at the time of PET imaging, tumor grade according to the World Health Organization classification (12) (Ki-67 for grade 1, <3%; grade 2, 3%–20%; grade 3, >20%), functional status, and previous locoregional and systemic treatments were collected. Patients were considered treatment-naïve if they had received no previous treatment except for surgery of the primary tumor.
All patients underwent PET/CT on an analog 3-dimensional (3D) PET scanner (Philips Gemini Dual-slice EXP scanner—PET AllegroTM system with Brilliance CT scanner—Philips Medical Systems, Cleveland, OH) according to guidelines (7). The median injected tracer activity was 148 MBq (range, 92–250 MBq). After a minimal time of 45–60 min, and after a free-breathing CT acquisition for attenuation correction from the vertex to the mid thigh (5-mm slices, 40 mAs, and 120 kVp), PET data were acquired in 3-dimensional mode at 2.5 min per bed position and 6–8 bed positions per patient. The PET scans were reconstructed by ordered-subset expectation maximization (3-dimensional row-action maximum-likelihood algorithm), and the matrix size was 144 × 144 voxels, resulting in voxels of 4.0 × 4.0 × 4.0 mm. All acquisitions were corrected for attenuation, scatter, and random coincidences.
Image Analysis and SRTB Extraction
For each PET/CT scan, all 68Ga-DOTATOC–avid lesions were segmented independently by 2 nuclear medicine physicians using a semiautomatic method through freely available software (LIFEx, version 5.1; IMIV [Imagerie Moléculaire In Vivo] Lab/CEA [Le Commissariat à l’Énergie Atomique et aux Énergies Alternatives]) (13) and based on the SUV threshold method to avoid intra- and interoperator variability in manual segmentation (14,15).
The SUVmax threshold based on healthy-liver uptake was chosen. SUVmax was assessed by placing a spheric volume of interest 3 cm in diameter in the right upper lobe of the liver, as previously reported (16). For each lesion, the SRETV and TLSRE were semiautomatically extracted. TLSRE was obtained by multiplying the SRETV of each lesion by its corresponding SUVmean. A visual inspection of the resulting automated volume segmentation was performed to remove background physiologic uptake (e.g., spleen, kidney, and bladder). The same analysis was performed for each patient by both operators to evaluate reproducibility.
We classified each lesion according to its site: primary tumor, lymph node, liver, bone, or other (e.g., peritoneum and lung). Then, SRETVwb and TLSREwb, defined as the sum of SRETV and TLSRE, respectively, for all lesions in each patient, were calculated (Fig. 2). When all lesions were equal to or lower than the liver SUVmax cutoff, SRETVwb and TLSREwb were defined as equal to 0 as previously mentioned (17). We also separated the corresponding SRETVwb (primary, lymph node, liver, bone, and other) and TLSREwb (primary, lymph node, liver, bone, and other) according to each tumor site. The details of the entire process are described in Supplemental Figure 1 (supplemental materials are available at http://jnm.snmjournals.org).

68Ga-DOTATOC PET/CT in WD pancreatic NET (PET/CT [A] and PET imaging [B]) showing high uptake in all lesions (highest SUVmax, 104.4). SRTB analysis (maximum-intensity projection [C], PET/CT [D], and PET imaging [E]) highlighted SRETVwb and TLSREwb values of 249 cm3 and 4,191 g, respectively.
Statistical Analysis
Quantitative variables were expressed as median with range. The primary clinical endpoint was the time to progression (TTP), defined as the time from PET/CT imaging to the first event (progression or relapse). Because anatomopathologic confirmation of all lesions is not achievable, the TTP of the disease was based on morphologic imaging criteria or functional criteria (18). Disease progression was defined as the appearance of a new lesion or a significant increase in the size of known lesions. The secondary clinical endpoint was overall survival (OS), defined as the time from PET/CT to NET-related death. Patients were followed up until the occurrence of the primary endpoints or until October 2020.
Kaplan–Meier curves and the log-rank test were applied for survival analysis. Receiver-operating-characteristic analysis was applied to determine the best cutoff for SRETVwb and TLSREwb parameters to predict the patient’s outcome using the Youden index (19). The area under the curve, sensitivity, specificity, and accuracy were reported.
For TTP, multivariate analysis was performed by the Cox proportional-hazards regression model to estimate hazard ratios with 95% CIs, including variables that had clinical relevance or a P value of less than 0.05 in univariate analysis. Because of the low number of events, we did not perform multivariate analysis for OS.
We performed a subgroup analysis on patients with metastatic NETs at the time of PET/CT, using the same SRETVwb and TLSREwb thresholds as found for the whole cohort. Moreover, an exploratory analysis to assess the repartition of SRTB according to tumor site and progressive versus nonprogressive disease during follow-up was performed through the nonparametric Mann–Whitney U test with Bonferroni adjustment.
Interobserver agreement was evaluated for SRETVwb and TLSREwb using intraclass correlation coefficient values of between 0 and 1, with a value of more than 0.9 defining the parameter as robust (20).
All statistical tests were 2-sided, and a P value of less than 0.05 indicated a statistically significant difference. All analyses were performed on XLSTAT (version 2019.2.2; Addinsoft).
RESULTS
Among the 322 patients screened, 84 (38 male and 46 female; median age at PET, 60.5 y [range, 25–86 y]) were included in the study. The main characteristics of the patients are represented in Table 1. The pancreas was the most frequent site (39/84, 46.4%), and 40.5%, 55.9%, and 3.6% of the tumors were classified as grades 1, 2, and 3, respectively. Fifty-four (64.3%) patients had metastatic disease at the time of PET/CT, and 47 patients (55.9%) were defined as treatment-naïve.
Characteristics of Patients
SRTB
In the whole cohort, 442 lesions and subsequent volumes of interest were segmented, including primary (n = 36, 8.1%), lymph node (n = 72, 16.3%), liver (n = 185, 41.9%), bone (n = 114, 25.8%), and other sites (n = 35, 7.9%). The median SUVmax, SRETV, and TLSRE per lesion were 9.7 (range, 3.3–116.5), 4.0 cm3 (range, 0.5–1,980.3 cm3), and 24.8 g (range, 1.8–21,819.5 g), respectively. The median SRETVwb and TLSREwb were 32.4 cm3 (range, 0–3,078.7 cm3) and 338.3 g (range, 0–22,658.6 g), respectively. In 5 patients, the SRETVwb was equal to zero because the lesions were 68Ga-DOTATOC–avid but with an SUVmax lower than the liver background.
Survival Analysis
Progression was detected in 35 patients (41.7%), and 14 patients died after a median follow-up of 23 mo (range, 0–41 mo). In the entire cohort, the median TTP was 22 mo (interquartile range, from 10 mo to not reached). Ten patients underwent curative surgery of the primary tumor after PET and did not show disease relapse during the follow-up.
Univariate Analysis for TTP/OS
For SRETVwb, the area under the receiver-operating-characteristic curve was 0.83 (best cutoff, 39.1 cm3), with a sensitivity, specificity, and accuracy of 0.86, 0.76, and 0.8, respectively. For TLSREwb, the area under the curve was 0.79 (best cutoff, 306.8 g), with a sensitivity, specificity, and accuracy of 0.86, 0.74, and 0.79, respectively. A higher SRETVwb (≥39.1 cm3) and TLSREwb (>306.8 g) correlated with a significantly shorter median TTP (12 mo [95% CI, 10–23 mo] vs. not reached for both; P < 0.001) and a shorter median OS (not reached for both; P < 0.001). SUVmax was not associated with TTP or OS (P = 0.08 and P = 0.09, respectively; Fig. 3).

TTP (left) and OS (right) in patients according to SUVmax (A and B), SRETVwb (C and D), and TLSREwb (E and F).
The TNM stage at the time of PET, the Ki-67 percentage, and treatment history (naïve vs. previous line of treatment) were also significantly associated with a shorter TTP and OS (P < 0.05; Supplemental Fig. 2), whereas age, sex, and secretory syndrome were not (P = not statistically significant).
Multivariate Analysis
SRETVwb and TLSREwb were strongly correlated in our study (R = 0.916 in Pearson correlation analysis). Thus, we performed a multivariate analysis using the Cox proportional-hazards regression model including only SRETVwb (>39.1 cm3). SRETVwb was the only independent predictor of TTP (hazard ratio, 4.8 [95% CI, 1.6–14.5]; P = 0.006) regardless of TNM stage, Ki-67 percentage, and treatment history (P = 0.58, 0.85, and 0.39, respectively) (Table 2).
Univariate and Multivariate Analyses Using Cox Regression for TTP According to SRETVwb, TLSREwb, and Other Characteristics of Cohort
Subgroup Analysis in Metastasis-Positive Patients
The diagnostic performance of SRTB to predict TTP and OS was assessed according to lesion site in a subgroup of patients with metastatic disease (n = 54). Using the same threshold, Kaplan–Meier analysis revealed a significant difference, with a shorter median TTP and OS for a higher value of both SRETVwb and TLSREwb (P = 0.002 and P = 0.016, respectively; Supplemental Fig. 3). SRTB analysis according to each lesion site did not reveal any difference between patients with progressive disease and patients with nonprogressive disease (Supplemental Table 1).
Interobserver Agreement
The mean liver threshold was 5.4 ± 2.2 (range, 2.1–12.9) for operator 1 and 5.3 ± 2.0 (range, 2.1–12.2) for operator 2. The median SRETVwb and TLSREwb were 32.4 cm3 (range, 0–3,078.7 cm3) and 338.3 g (range, 0–22,658.6), respectively, for operator 1, and 32.0 cm3 (range, 0–3,100.0 cm3) and 282.0 g (range, 0–22,789.0), respectively, for operator 2. The intraclass correlation coefficients were, respectively, 0.963, 0.988, and 0.997 for liver threshold, SRETVwb, and TLSREwb.
DISCUSSION
We investigated the prognostic value of SRTB extracted from 68Ga-DOTATOC PET/CT in patients with WD NET. SRETVwb (≥39.1 cm3) and TLSREwb (≥306.8 g) were significantly associated with TTP, but at multivariate analysis, SRETVwb was an independent prognostic parameter regardless of Ki-67 percentage, TNM stage, or treatment.
Several previous studies assessed the prognostic significance of 68Ga-DOTATOC (17,21) and 68Ga-DOTATATE PET/CT (10,11,22,23) volumetric parameters in patients with NETs. In a prospective study including a large population of 184 patients with grades 1–3 NETs, Tirosh et al. reported that SRETVwb of at least 7.0 cm3 and at least 35.8 cm3 obtained by 68Ga-DOTATATE PET/CT were significantly associated with progression-free survival (PFS) and OS (P < 0.001 both), respectively (10). In another prospective study, including only grade 1 or 2 gastroenteropancreatic NETs, Toriihara et al. found that an SRETVwb of at least 11.1 cm3 and a TLSREwb of at least 146.48 g obtained by 68Ga-DOTATATE PET/CT were associated with PFS but that only SRETVwb was independently associated with PFS in a survival analysis, in accordance with our study (11). Kim et al. (17), in a retrospective study including 31 patients with unresectable or metastatic WD gastroenteropancreatic NETs undergoing 68Ga-DOTATOC PET/CT before receiving lanreotide, showed that a lower tumor-to-liver ratio, lower SUVmax, and higher SRETVwb (>58.9 cm3) were significantly associated with a shorter PFS in univariate analysis, but only tumor-to-liver ratio (hazard ratio, 3.182; P = 0.021) remained an independent factor for PFS in multivariate analysis. In our study, SUVmax was not associated with TTP, as is consistent with findings by Tirosh et al. and Toriihara et al. (10,11). One potential explanation is the differences in selection criteria. In fact, Kim et al. included a more homogeneous population of patients at an early stage of disease, most of whom had not undergone other types of treatment (87.1%, excluding surgery) (17). Although a high SUV on 18F-FDG PET/CT is positively associated with prognosis in almost all cancers, including NETs (24)—explaining the interest in using total lesion glycolysis—a lower SUVmax on 68Ga-DOTA-SSTa PET/CT is associated with poorer prognosis in patients with WD NETs (8,9,25,26). Thus, for the same SRETVwb value, patients in whom lesions with a low SUVmean—and thus a low TLSREwb value—are disclosed might tend to present a less favorable prognosis, leading to conflicting results among different studies that include different patient populations. For this reason, SRETVwb seems to be the most prognostic parameter, but its use should be validated in further prospective future studies including populations that are more homogeneous in terms of primary site, disease course, and treatment setting.
Furthermore, the proper methodology to evaluate SRTB should be considered. In our study, a customized threshold based on liver SUVmax was chosen, and to our knowledge, this was the second study in which such a segmentation method was applied to 68Ga-DOTATOC PET/CT (17). This methodology presents the advantage of being fast; hence, it could represent a useful tool in clinical practice. Interestingly, we found higher cutoffs for SRETVwb and TLSREwb than did studies assessing SRTB using 68Ga-DOTATATE, whereas the SRETVwb and TLSREwb cutoffs were consistent with the study of Kim et al., performed with the same radiopharmaceutical, 68Ga-DOTATOC (10,11,17). The literature showed that tumor uptake is higher and liver uptake lower with 68Ga-DOTATOC than with 68Ga-DOTATATE, leading to a higher tumor-to-liver ratio (27,28). Hence, we can assume that SRETVwb and TLSREwb might be lower using 68Ga-DOTATATE. These differences could also be explained by the difference in segmentation methodology. Toriihara et al. used a 50% threshold of SUVmax to segment each lesion, leading to a lower SRETVwb value, especially in patients with intense radiotracer uptake (11). An example of the impact of different segmentation methods on SRTB is reported in Supplemental Figure 4.
In addition, assessing the reproducibility and robustness of SRTB calculation is important. In our study, reproducibility between the 2 operators was excellent, with an intraclass correlation coefficient of more than 0.9 for both SRETVwb and TLSREwb. To our knowledge, no study has assessed the reproducibility of SRTB parameters on 68Ga-DOTA-SSTa PET/CT. Many studies showed that the segmentation method can impact the interoperator reproducibility of whole-body metabolic tumor volume on 18F-FDG PET/CT imaging, especially threshold methods based on 41% of SUVmax (29,30). SRTB parameters in 68Ga-DOTA-SSTa PET/CT might be more reproducible than whole-body metabolic tumor volume because of the higher signal-to-noise ratio. This point is a crucial one; studies are needed of the reproducibility and robustness of whole-body volumetric parameters in 68Ga-DOTA-SSTa PET/CT, especially between different PET systems.
Beyond the prognostic role, evaluation of changes in SRETVwb and TLSREwb (namely change in SRETVwb and change in TLSREwb) after the initiation of systemic therapy may offer promising perspectives, especially for patients treated with peptide receptor radionuclide therapy (31), and need to be assessed. However, SSA treatment or peptide receptor radionuclide therapy can modify liver uptake, as previously reported (32), impacting the calculation of SRTB. Therefore, the systematic use of the pretherapeutic liver SUVmax cutoff could be a solution to following the evolution of SRTB parameters (31,33).
Our study presents some limitations. First, it was retrospective, included a heterogenous cohort, and was conducted at a single center and on a single PET/CT scanner. Second, we included only patients with 68Ga-DOTATOC–avid lesions, and using the liver SUVmax as the cutoff, the SRETVwb was equal to zero in 5 patients. This finding is explained by the low lesion volume in these patients, which did not impact their classification as good-prognosis patients. This point is crucial, because the same assertion should not be followed in patients with a high tumor burden without 68Ga-DOTATOC uptake. In such a situation, the prognosis would be worse and 18F-FDG PET/CT should be performed (5,23,24).
CONCLUSION
In our cohort, whole-body volumetric 68Ga-DOTATOC PET/CT parameters (SRETVwb and TLSREwb) were associated with TTP and OS. SRTB could add value to conventional clinical prognostic parameters and other standard PET parameters (e.g., SUVmax) in predicting a patient’s prognosis and guiding treatment decisions, thus supporting the implementation of SRTB in clinical practice. As previously mentioned, our results remain preliminary and applicable to 68Ga-DOTATOC PET/CT but need to be validated in prospective studies and explored with other 68Ga-peptides.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
KEY POINTS
QUESTION: Can whole-body volumetric parameters extracted from 68Ga-DOTATOC PET/CT be useful in assessing the prognosis of WD NETs?
PERTINENT FINDINGS: In our cohort, whole-body volumetric 68Ga-DOTATOC PET/CT parameters (SRETV and TLSRE) were associated with TTP and OS. SRETVwb was the only independent prognostic parameter, regardless of Ki-67 percentage, TNM stage at the time of PET, and treatment history (naïve vs. previous treatments) before PET scanning.
IMPLICATIONS FOR PATIENT CARE: In the future, whole-body volumetric 68Ga-DOTATOC PET/CT parameters may add value to conventional prognostic parameters in predicting the prognosis of patients with WD NETs.
Footnotes
Published online Nov. 5, 2021.
- © 2022 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication May 28, 2021.
- Revision received October 4, 2021.





{kind=link}
{kind=link}
{kind=link}
{kind=link}