


Abstract
90Y resin radioembolization is an emerging treatment in patients with liver-dominant metastatic neuroendocrine tumors (mNETs), despite the absence of level I data. The aim of this study was to evaluate the efficacy of this modality in a meta-analysis of the published literature. Methods: A comprehensive review protocol screened all reports in the literature. Strict selection criteria were applied to ensure consistency among the selected studies: human subjects, complete response data with time interval, resin microspheres, more than 5 patients, not a duplicate cohort, English language, and separate and complete data for resin-based 90Y treatment of mNET if the study included multiple tumor and microsphere types. Selected studies were critically appraised on 50 study criteria, in accordance with the research reporting standards for radioembolization. Response data (Response Evaluation Criteria in Solid Tumors) were extracted and analyzed using both fixed and random-effects meta-analyses. Results: One hundred fifty-six studies were screened; 12 were selected, totaling 435 procedures for response assessment. Funnel plots showed no evidence of publication bias (P = 0.841). Critical appraisal revealed a median of 75% of desired criteria included in selected studies. Very high between-study heterogeneity ruled out a fixed-effects model. The random-effects weighted average objective response rate (complete and partial responses, CR and PR, respectively) was 50% (95% confidence interval, 38%–62%), and weighted average disease control rate (CR, PR, and stable disease) was 86% (95% confidence interval, 78%–92%). The percentage of patients with pancreatic mNET was marginally associated with poorer response (P = 0.030), accounting for approximately 23% of the heterogeneity among studies. The percentage of CR and PR correlated with median survival (R = 0.85; P = 0.008). Conclusion: This meta-analysis confirms radioembolization to be an effective treatment option for patients with hepatic mNET. The pooled data demonstrated a high response rate and improved survival for patients responding to therapy.
Neuroendocrine tumors (NETs) are generally indolent tumors with a variable natural history of disease, arising from neuroendocrine cells throughout the body (1,2). They can be roughly divided into carcinoid and pancreatic cell tumors, and their incidence has inexplicably increased from 1.09 to 5.25 in 100,000 from 1973 to 2004 (3). The liver is the most frequent site of metastasis and the prognosis for metastatic disease is poor, with a median overall survival (OS) of 5–57 mo, often preceded by substantial morbidity such as the carcinoid syndrome (1–3).
There are various treatment options for patients with hepatic metastatic NETs (mNETs), aimed at improving quality of life, reducing symptoms, and increasing survival. The only potentially curative treatment option is surgery, which has a 10-y median OS of 42% but a median progression-free survival of only 21 mo, indicating that few patients are cured (4). Most patients are poor surgical candidates, presenting with diffuse or poorly differentiated disease (5). Inoperable patients may be evaluated for systemic therapies. Those with well-differentiated receptor-positive mNETs may be treated symptomatically with somatostatin analogs (octreotide), which have been shown to improve survival over placebo, whereas low- to intermediate-grade tumors may be treated with other systemic therapies such as streptozocin, doxorubicin, and dacarbazine, in addition to relatively newer agents including sunitinib and everolimus, both of which have been shown to improve survival over placebo (6–8). Those that are poorly differentiated or with a high Ki-67 proliferation index are typically treated with cytotoxic systemic therapies, which are usually platinum-based and may show a marked initial response, but it is usually not durable (9).
Liver-directed therapies have been widely adopted for liver-dominant disease, but external-beam radiotherapy and percutaneous ablative therapies are rarely appropriate for multifocal disease. However, similar to primary hepatocellular carcinoma, mNETs typically derive nearly all of their blood supply from the hepatic artery, whereas normal liver parenchyma mainly uses the portal vein. Cytotoxic, radioactive, or ischemia-producing agents administered intraarterially thereby target tumors preferentially, limiting systemic and hepatic toxicity.
90Y resin radioembolization has been shown to be an effective treatment for hepatic mNETs that is well tolerated, with low risk of grade 3 or higher early or late toxicity, and a superior quality of life profile (10–12). It involves injecting arteriole 30-μm-sized embolic resin (SIR-Spheres; Sirtex Medical Ltd.) or glass (TheraSphere; BTG Inc.) microspheres loaded with the β-emitting radioisotope 90Y into the tumor hepatic arterial supply. The use of this therapy is largely institution-specific, as first-line therapy with or without other modalities, as second-line therapy after another modality has failed, or as salvage therapy in patients refractory to all other treatments. In the absence of level I data, the aim of this study was to evaluate the efficacy of radioembolization for liver mNETs in a meta-analysis of the published literature.
MATERIALS AND METHODS
Search Strategy and Study Selection
To cover all of the literature, we used a meticulous systematic review procedure of the following databases: Pubmed, EMBASE, Cochrane, Scopus, and CINAHL. The initial search only used the filters “English language” and “human studies”, and the time frame included any study published before March 1, 2014. The search query included “90Y”, “radioembolization”, “liver metastases”, “neuroendocrine tumor”, “embolization”, “selective internal radiation therapy”, “internal radiation”, “intraarterial radiation”, “brachytherapy”, “microspheres”, and synonyms, derivations, permutations, and abbreviations of the above terms.
All articles with a relevant title or abstract were reviewed in full. Relevance was broadly defined to maximize the number of articles retrieved and yield from cross-referencing. All new articles retrieved from cross-referencing were also reviewed and cross-referenced. The following selection criteria were applied: human subjects, complete response data with time interval, at least 5 patients in the study group, not a duplicate cohort, English language, and if the study included multiple tumor or microspheres types it needed to have separate and complete data for hepatic mNET treated with resin microspheres.
For selected studies, the following data were retrieved: publication year, number of patients, type of radioembolic microsphere, radiographic criteria for response assessment, time after treatment to response assessment, percentage in each response category, degree of extrahepatic disease, prior therapy regimens, degree of liver tumor involvement, median overall survival, 1-y survival, activity administered, and primary site and histology of tumor. In mixed cohorts (i.e., patients with various tumor and microsphere types), only data for patients with hepatic mNET treated with resin microspheres were extracted.
Critical Appraisal
A critical appraisal of the selected studies evaluated whether they included the criteria listed in Table 1. The criteria were divided into major and minor, and studies scored 2 points for including major criteria and 1 point for minor criteria. Some of the above criteria were not applicable to each study, in which case points were not lost, but the total possible points was decreased accordingly. These criteria were developed in concordance with the research reporting standards for 90Y radioembolization (13).
Critical Appraisal According to Research Reporting Standards for Radioembolization
Statistics
Twelve radioembolization articles were analyzed with both fixed-effects and random-effects meta-analyses; effect sizes were based on logit-transformed percentage of patients with disease response and control. Outcomes were per procedure. Effects of the following moderator variables were tested with a mixed-effects model, using restricted maximum-likelihood estimation with Knapp–Hartung adjustment (14): percentage of patients with pancreatic and carcinoid mNETs and administered activity. As a check, covariate testing was performed with a 50,000-permutation test using the DerSimonian–Laird estimator. The median of the reported median survival times was estimated with a 1,000-sample bias-adjusted bootstrapped confidence interval. Statistical analyses were performed with R version 2.15.2 (www.r-project.org) using version 1.8.0 of the metafor package and version 2.3.0 of the meta package.
The critical appraisal scored each study as a percentage of total possible points. The denominator included all possible points (2 points for major criteria and 1 point for minor criteria), whereas the numerator included the total points accrued. The denominator was not the same across all studies, because some criteria were not applicable to each study.
RESULTS
Studies Selected and Critical Appraisal
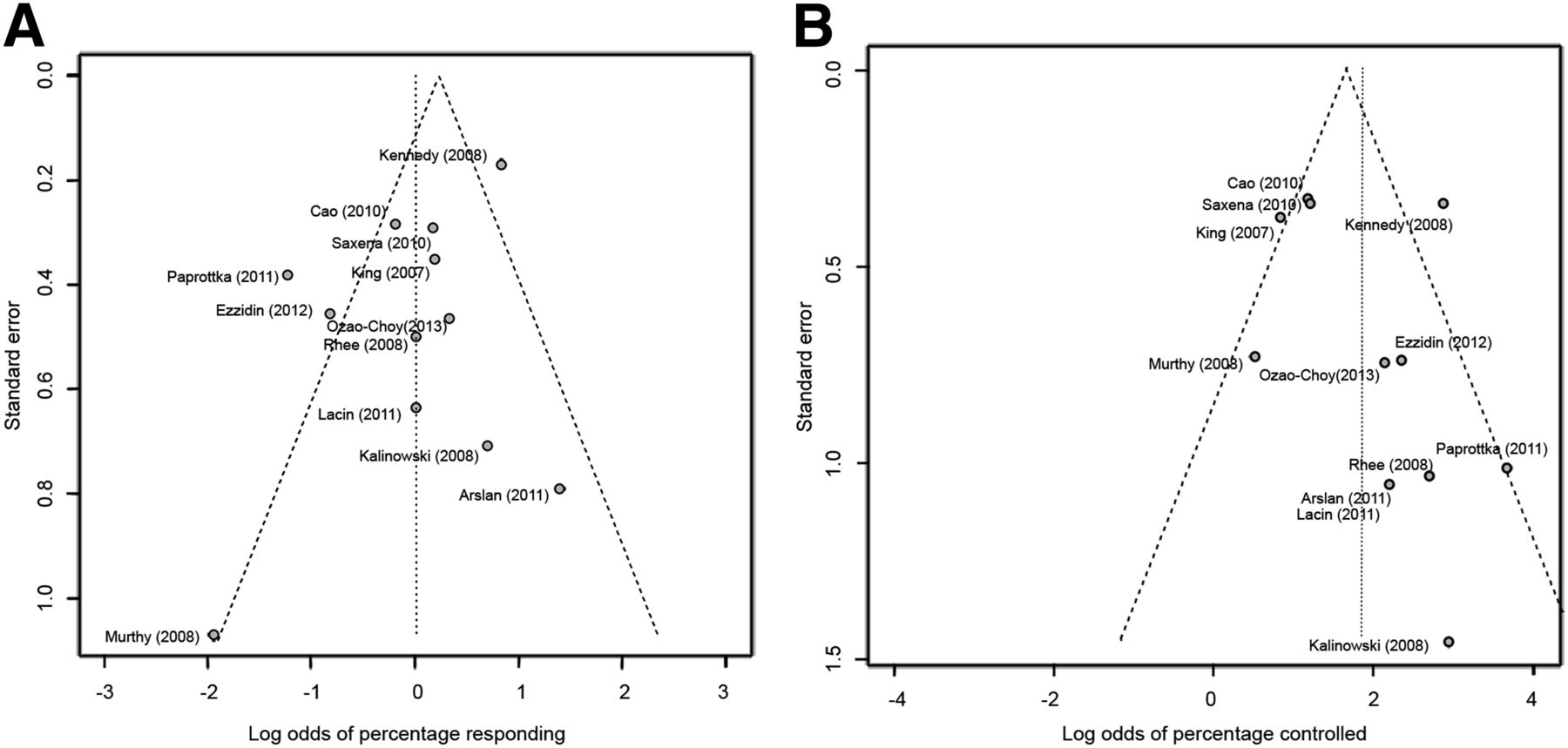
One hundred fifty-six relevant studies were reviewed in full, and 49 contained patients with hepatic mNETs treated with radioembolization. Application of the selection criteria narrowed down the selection to 12 studies (10,15–25). Most studies were excluded because they did not provide separate and complete Response Evaluation Criteria in Solid Tumors (RECIST) data specifically on hepatic mNETs treated with radioembolization. Rank-correlation tests for funnel plot asymmetry were not significant (percentage response, P = 0.841; percentage controlled, P = 0.370), demonstrating no evidence of publication bias (Fig. 1).

Funnel plots for included studies reporting on response (A) and disease control (B). No evidence of publication bias was found according to log-rank correlation (percentage response, P = 0.841; percentage controlled, P = 0.370).
From these 12 studies, 6 were retrospective, 3 were prospective, 1 was prospectively collected but retrospectively reviewed, and 2 didn’t specify. The total number of procedures with response data was 435, in 414 patients. Most studies reported their response data per patient. The largest study in the cohort including 148 patients described their response data in terms of 168 procedures, because some patients had staged procedures to treat the entire liver or retreatment of the same territories (10). According to the critical appraisal system, the median score for all studies was 75% (range, 42%–81%). The median score for the major criteria was 83%, and for the minor criteria it was 45% (Table 2).
Critical Appraisal According to Research Reporting Standards for Radioembolization
Patient Characteristics
From the 12 studies included, 8 specified the number of patients with extrahepatic metastases (median, 50%; range, 22%–63%). Eight specified the degree of liver replacement by tumor, with 4 having a median replacement of 44% (range, 32%–57%) and the other 4 reporting the percentage replacement in categories (Table 3). Treatments before radioembolization included but were not limited to surgical resection; systemic cytotoxic, targeted, or hormonal treatment; radiofrequency ablation; percutaneous ethanol injection; intraarterial bland or chemoembolization; and external-beam radiation therapy, with some studies using up to 3 of these before radioembolization. The most frequently specified were surgery in 9 studies (median, 39%; range, 17%–95%), cytotoxic chemotherapy in 8 studies (median, 45%; range, 15%–100%), and intraarterial chemoembolization in 6 studies (median, 34%; range, 10%–100%) (Table 3). Other details including age, sex, baseline laboratory values, Eastern Cooperative Oncology Group score, and time interval from NET diagnosis to 90Y radioembolization are provided in Supplemental Table 1 (supplemental materials are available at http://jnm.snmjournals.org).
Baseline Patient Characteristics and Results for Each Study Included in Meta-Analysis
Response and Survival Assessment
Very high between-study heterogeneity (I-square, 65%–74%; P < 0.0001) suggested that a fixed-effects model was not appropriate. For 90Y radioembolization with resin microspheres only, objective radiographic response rates (defined as complete response plus partial response by RECIST) (26) ranged from 12% to 80%, with a random-effects weighted average of 50% (95% confidence interval, 38%–62%) (Fig. 2). Disease control rates (defined as complete response, partial response plus stable disease) ranged from 62% to 100%, with a random-effects weighted average of 86% (95% confidence interval, 78%–92%) (Fig. 3). For percentage responding, an increase in percentage of pancreatic mNET was marginally associated with a decrease in response rate (P = 0.030), accounting for approximately 23% of the heterogeneity among studies, whereas percentage carcinoid mNETs did not have a significant effect on response rate (P = 0.198). For percentage disease controlled, neither an increase in percentage of pancreatic mNET (P = 0.178) nor percentage of carcinoid mNET (P = 0.128) had a significant effect. Administered activity (median, 1.7 GBq; range, 1.2–3.4 GBq) did not correlate with either response or control rate.
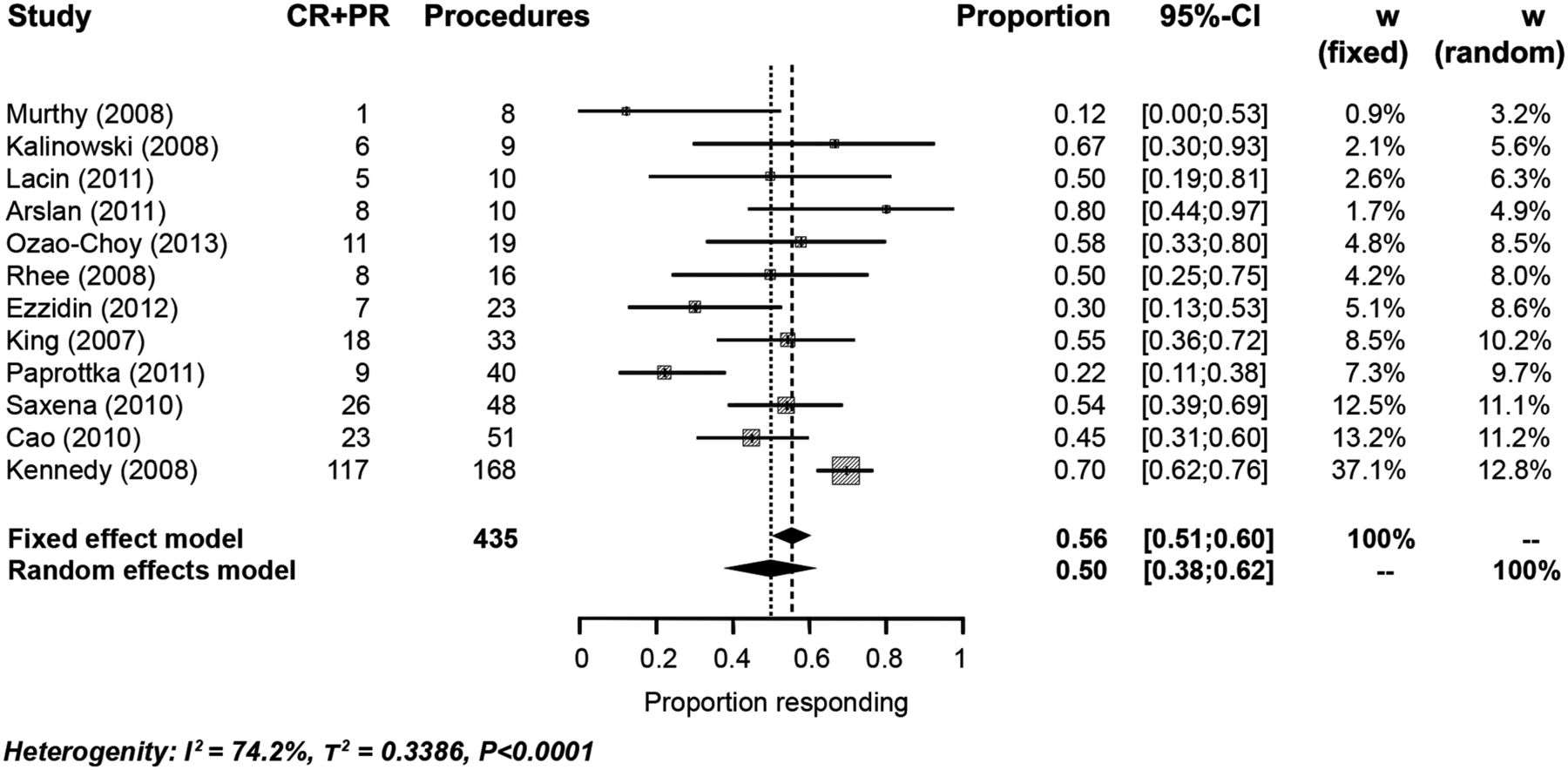
Response rates for included studies (year): complete response and partial response. Weighted average response rate according to random-effects model was 50%, with a 95% confidence interval (CI) of 38%–62%. Fixed-effect model was ruled out because heterogeneity (P < 0.0001). CR = complete response; PR = partial response; W = weighted average.

Disease control rates for included studies (year): complete response, partial response, and stable disease. Weighted average disease control rate according to random-effects model was 86%, with a 95% confidence interval (CI) of 78%–92%. Fixed-effect model was ruled out because of heterogeneity (P < 0.0001). CR = complete response; PR = partial response; SD = stable disease; W = weighted average.
Pooled survival data could not be provided for this cohort because 95% confidence intervals were not sufficiently provided. The median OS ranged from 14 up to 70 mo, with a median of 28.5 mo (95% confidence interval, 18–49.5 mo). The response rate correlated with median survival (R = 0.85; P = 0.008). Although a pooled analysis could not be calculated, the median and 1-y survival per individual study is listed in Table 3.
DISCUSSION
Radioembolization is an emerging and effective treatment for hepatic mNETs, with a superior toxicity profile (10–12). Multiple studies in the published literature have described outcomes of radioembolization for these patients. Twelve of these studies were included in our meta-analysis, with data pooled to evaluate overall efficacy. The pooled response rate of 50% and disease control rate of 86% by RECIST confirms the efficacy and validates the popularity of this treatment modality. The pooled response rates compare favorably with other therapies such as somatostatin analogs with or without interferon; older cytotoxic chemotherapeutics including dacarbazine, cisplatin, etoposide, streptozocin, and temozolomide; systemic radionuclide therapies such as peptide receptor radionuclide therapy; and newer targeted systemic therapies including everolimus and sunitinib (Supplemental Table 2).
The response rates in individual reports varied from 12% to 80%, differences resulting in part from widely differing percentages of pancreatic mNETs in each study. Our meta-analysis found a decrease in response rate with increasing percentages of pancreatic mNETs, which is consistent with previous findings and probably reflects the more aggressive nature of pancreatic NETs. In a study using bland embolization and chemoembolization, only 35.2% of pancreatic mNETs responded radiographically, whereas 66.7% of carcinoid mNETs responded (P = 0.0001) (27). In addition, previous epidemiologic studies using the National Cancer Institute Surveillance Epidemiology and End Results cancer registry that included 49,012 NETs showed that pancreatic NETs are diagnosed at a higher stage than other NET primaries (28). Despite this relationship, carcinoid mNETs were not associated with a higher response rate in our meta-analysis, which may be due in part to incomplete and inconsistent histology reporting among the source studies.
The median OS averaged 28.5 mo and ranged 14–70 mo. This wide variation may also be explained in part by the percentage of pancreatic mNETs in these studies as pertaining to response rates. The Surveillance Epidemiology and End Results database indicates that pancreatic NETs exhibit the lowest 5-y survival, compared with all other NET primaries. Small bowel primaries have nearly a 2-fold-higher 5-y survival rate (68.1%) when compared with pancreatic mNETs, likely contributing to the high survival in the Kennedy study, which had one of the largest percentages of small bowel primaries (68%) (10,28). Previous studies found a survival advantage in metastatic carcinoid, compared with pancreatic mNETs, in patients treated with other liver-directed treatments (27,29–32), but studies on 90Y radioembolization failed to find associations between primary tumor location and survival outcomes for hepatic mNETs (17,24). These studies, as well as our meta-analysis, may be underpowered to confirm this relationship.
It has been suggested that many factors, including prior surgery (33), size of target lesions (34), performance status (35,36), baseline chemistry values (35), Ki-67 index (17), presence of extrahepatic disease (16), and inability to deliver a specified dose (34), influence patient outcomes for treatment of hepatic mNETs with 90Y radioembolization. Unfortunately, despite publication reporting standards (13), publications do not conform to these standards and such clinical factors are often absent or incomplete, which limited the ability of this meta-analysis to analyze other factors potentially contributing to the pooled results. For instance, the study that included the largest database and reported some of the highest response and survival data provided little information on baseline patient characteristics (10). The critical appraisal resulted in a median score of only 75% among the 12 papers included. A higher median score of 83% was achieved when only major criteria were included, indicating that studies were slightly better at providing basic data but not sufficiently detailed to meet all criteria in the research reporting standards. Given the potential significance of these factors on outcomes, the importance of detailed reporting on patient characteristics, follow-up, treatment techniques, and outcomes cannot be stressed enough, and future authors need to become familiar with the reporting standards, which also need to be enforced by referees and editors.
This lack of comprehensive details, standardized follow-up, and inconsistency in reporting both objective response rates and survival in the source publications is the major limitation of this meta-analysis. For example, whereas 7 studies reported RECIST within 6 mo of treatment, the other studies only provided a follow-up range during which RECIST was recorded. These heterogeneous intervals may confound the response assessments. Other sources of uncertainty include large variability in the patient population of the 12 studies included in this meta-analysis—including wide variability in mNET histology, amount of extrahepatic disease and liver replacement by tumor, prior treatment regimens, and concurrent treatment regimens—as well as institution- and operator-specific variables that impact patient selection and treatment protocols (e.g., unilobar vs. bilobar treatment).
Besides the patient heterogeneity and reported details in the studies themselves, another potential limitation of any meta-analysis is publication bias. The studies included in meta-analyses are sometimes skewed toward smaller studies with unrealistically positive results. Critical appraisal of studies included in the present meta-analysis suggested they were well balanced. However, the large heterogeneity of the studies mandated use of a random-effects model, which has larger confidence intervals. In addition, inclusion of multiinstitutional studies may have resulted in inclusion of overlapping patients. However, given the limited data available in the source publications, it was not possible to identify and exclude all redundancies.
CONCLUSION
Hepatic radioembolization using 90Y resin microspheres is an effective treatment option for hepatic mNETs. The pooled data demonstrated a weighted objective response rate of 50%, disease control rate of 86%, and improved OS for patients responding to therapy. Lower response rates and survival times were associated with mNETs of pancreatic cell origin, which may be due to their more aggressive nature and advanced stage at time of diagnosis. Future studies need to comply with consensus reporting standards to contribute meaningfully to our understanding of this disease and treatment modality.
DISCLOSURE
The costs of publication of this article were defrayed in part by the payment of page charges. Therefore, and solely to indicate this fact, this article is hereby marked “advertisement” in accordance with 18 USC section 1734. Dr. Daniel Y. Sze is employed as a member of the scientific or medical advisory boards (SAB/MAB) of: Jennerex Biotherapeutics, Inc., Surefire Medical, Inc., Koli Medical, Inc., Northwind Medical, Inc., Treus Medical, Inc., RadRuard Medical, Inc., and Lunar Design and Consultant/DSMB: BTG Medical, Inc., Sirtex Medical, Inc., Covidien, Inc., and W.L. Gore, Inc. The authors did not receive financial assistance in the production of this manuscript. No other potential conflict of interest relevant to this article was reported.
Acknowledgments
We thank and acknowledge the help of Rhonda Lee in assistance with the figures and Hella Bluhm-Stieber and Marilyn Tinsley in assistance with the literature searches.
Footnotes
Published online Jul. 10, 2014.
- © 2014 by the Society of Nuclear Medicine and Molecular Imaging, Inc.
REFERENCES
- Received for publication January 24, 2014.
- Accepted for publication June 19, 2014.





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- A Novel Injectable Hydrogel Matrix Loaded With 90Y Microspheres for the Treatment of Solid Tumors
- NCCN Guidelines Insights: Neuroendocrine and Adrenal Tumors, Version 2.2018
- Radioembolization of Colorectal Liver Metastases: Indications, Technique, and Outcomes
- Reduced Periprocedural Analgesia After Replacement of Water for Injection with Glucose 5% Solution as the Infusion Medium for 90Y-Resin Microspheres
- 90Y Hepatic Radioembolization: An Update on Current Practice and Recent Developments
- Neuroendocrine Tumors, Version 1.2015