


Abstract
Radioembolization is an established treatment modality that has been subjected to many improvements over the last decade. Developments are occurring at a high pace, affecting patient selection and treatment. The aim of this review is therefore to provide an overview of current practice, with a focus on recent developments in the field of radioembolization. Several practical issues and recommendations in the application of radioembolization will be discussed, ranging from patient selection to treatment response and future applications.
As an established treatment modality for chemoresistant, unresectable hepatic malignancies, radioembolization has expanded its applications in recent years. Radioembolization is based on the administration of 90Y-loaded microspheres in the arterial vasculature of the liver. Currently, two types of microspheres are Food and Drug Administration–approved and commercially available: resin microspheres (SIR-spheres; SirTex Medical) and glass microspheres (TheraSpheres; BTG International Ltd.). Because of preferential arterial flow, the microspheres occlude small tumor arterioles, thus selectively irradiating tumors. This review aims to give an overview of current developments in the field of 90Y hepatic radioembolization.
PATIENT SELECTION
Currently, radioembolization is indicated mainly in a palliative setting for primary and secondary hepatic malignancies, only when other (minimal) invasive or chemotherapeutic treatments have failed. Work-up for radioembolization includes clinical status, hematologic and biochemical status, anatomic assessment with CT/MR imaging, and, when appropriate, molecular imaging with SPECT/CT or PET/CT. The indications and contraindications (Table 1) need to be assessed by a multidisciplinary team (1,2). Unlike many treatment modalities, age is not a contraindication for radioembolization and has not been shown to alter prognosis (3,4).
Common Indications and Relative and Absolute Contraindications for Radioembolization
Sufficient liver function is of primary importance and is regarded as the greatest limitation (Child–Pugh score ≤ B7). Before considering radioembolization (when sufficient liver function is present), portal venous integrity, prior surgical treatments, and prior liver-directed treatments need to be evaluated. Compromised portal venous integrity is most commonly caused by a portal vein tumor thrombus (PVT), resulting in a greater dependence of the liver parenchyma on its arterial supply (5). Theoretically, after embolization a compromised portal circulation could jeopardize liver function because of ischemia or infarction, induced by the arterial occlusion. However, radioembolization has a low embolic effect, and most of the arterial tree remains patent after treatment (6,7). Radioembolization in the setting of PVT is therefore safe and can sometimes lead to complete portal vein revascularization, even in main PVT (8). In contrast to transarterial chemoembolization (TACE), PVT is not considered a contraindication. Radioembolization is an emerging indication in early-advanced hepatocellular carcinoma (HCC) (Barcelona Clinical Liver Cancer [BCLC] C, liver-dominant, Eastern Cooperative Oncology Group [ECOG] 1–2, PVT) (8). On the basis of current evidence, application of radioembolization in patients with a Child–Pugh score higher than B7 and main PVT should be weighed carefully, because of the limited potential survival benefit after radioembolization (4.5–5 mo in Child–Pugh B patients and 2.5 mo in Child–Pugh C patients vs. 2.7–4.0 mo in untreated patients) (9–12).
Prior surgical liver resection is no contraindication for radioembolization. However, surgical procedures involving the biliary tract may be a risk factor for infectious complications. The incidence of hepatic abscesses after radioembolization in patients with a normal biliary tree, or in the presence of a bilidigestive anastomosis, is fortunately low—less than 1% (Table 2) (13)—as opposed to less than 5% in the general TACE population and 48%–86% after TACE in the presence of a bilidigestive anastomosis (14,15). An aggressive prophylactic antibiotic regimen is therefore not advised (16,17). Radioembolization in the presence of a bilidigestive anastomosis seems safe but needs further attention, as liver abscesses after TACE show a high mortality rate of 11%–50% (15,18). Currently, a bilidigestive anastomosis is considered to be a relative contraindication for radioembolization, but this view is based on the available TACE literature because there is only limited evidence for radioembolization.
Current Literature on Liver Abscesses and Bilidigestive Anastomoses After Radioembolization
HEPATIC VASCULARIZATION AND ANGIOGRAPHIC CONSIDERATIONS
The standard hepatic arterial supply originates from a celiac trifurcation, from which the common hepatic artery arises. The common hepatic artery becomes the proper hepatic artery, after the gastroduodenal artery has branched off. The proper hepatic artery continues toward the hilar plate, where it splits into the right and left hepatic arteries (19). Anatomic variants of the hepatic arterial vasculature are common, and correct identification of these variants is essential as it may increase the risk of extrahepatic deposition (20). Information on arterial liver vascularization derived from preprocedural liver CT–angiography or MR imaging–angiography (e.g., with an early arterial phase) is paramount for successful angiography (19,21). Anatomic variants are frequently missed in clinical practice in the absence of a thorough evaluation of the arterial vascularization on multimodality imaging. This results in unnecessary additional angiography procedures and incomplete radioembolization treatments.
The severity of an extrahepatic deposition of microspheres depends on the affected organ and the number of displaced microspheres, and its location depends on the culprit vessel. Previously, so-called skeletonization of the hepatic arteries was advised to avoid extrahepatic depositions (2). In recent years, however, this has been debated. Skeletonization can be quite an endeavor, and new hepatic–enteric collaterals may develop after coil embolization (22). Moreover, numerous disadvantages are related to the angiography procedure itself: increased procedure complexity, additional radiation dose, potential vessel damage, and complications of coil deployment. At present, most experienced centers try to avoid coil embolization. Significant extrahepatic depositions are found mostly within the distribution of 3 distinct side-branches (Table 3): the gastroduodenal artery, cystic artery, and right gastric artery (20,21). In a recent case series of 134 patients, 68.7% did not undergo coil embolization of either the gastroduodenal artery or right gastric artery. After radioembolization with glass microspheres, 1% developed a gastric ulcer (23). On the other hand, in a case series of 247 patients treated with resin microspheres, 3.2% developed a biopsy-proven gastroduodenal ulcer, despite skeletonization (24). Potential culprit vessels need to be assessed and coiled individually. Thus, standard rigorous occlusion of all side-branches of the hepatic arteries (e.g., skeletonization) has been abandoned (23).
If an extrahepatic deposition of activity is found on pretreatment simulation with 99mTc-macroaggregated albumin (99mTc-MAA) SPECT/CT, coil-embolizing the culprit vessel, a more distal position of the catheter, or superselective catheterization, can provide a safe treatment procedure, rendering 91%–96% of the prior selected patients eligible for radioembolization (25,26). To avoid the need for a second pretreatment angiography procedure, the use of catheter-directed CT (e.g., C-arm cone-beam CT or hybrid angiography/CT) may prove indispensable. The culprit vessels can be identified during angiography and coil-embolized immediately (Fig. 1) (27). Additionally, C-arm CT can assess tumor coverage during the angiography procedure. Unenhanced tumor regions can be detected, often leading to identification of additional supplying arteries, preventing incomplete treatment. The C-arm CT provides the interventional radiologist with valuable feedback during the angiography procedure and affects the treatment plan in up to 52% of the patients (28).
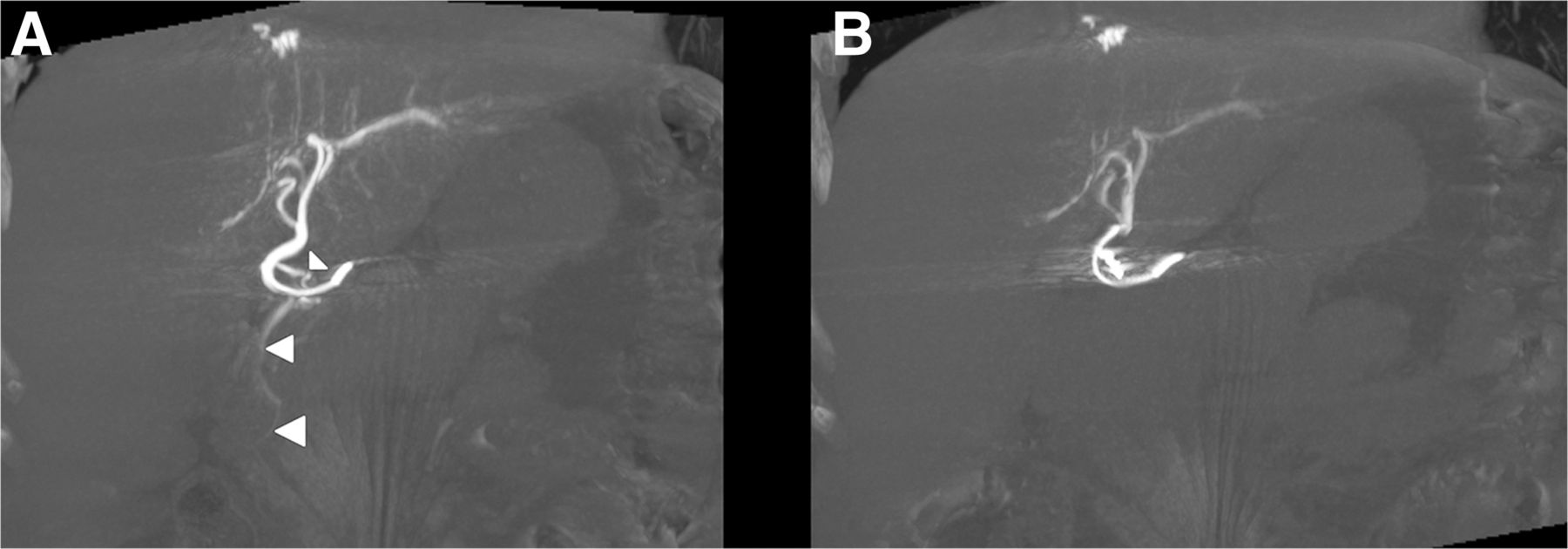
Coronal reconstructions of C-arm CT in patient before radioembolization. During angiography, catheter was positioned in proximal left hepatic artery. (A) C-arm CT illustrates arterial flow of contrast agent toward pancreatic head/duodenal region, supplied by supraduodenal artery (arrowheads), missed during digital subtraction angiography. On the basis of this additional finding, artery was occluded. (B) After coil embolization, contrast flow toward gastrointestinal tract was resolved.
PRETREATMENT IMAGING AND DOSIMETRY
Pretreatment simulation is currently based on 99mTc-MAA SPECT/CT for assessment of extrahepatic depositions and lung shunting. Lung shunting is caused by arteriovenous anastomoses or shunts in the liver parenchyma or tumor, potentially resulting in radiation pneumonitis after radioembolization (29,30). The highest tolerable lung shunt absorbed dose was defined as 30 Gy after a single treatment and up to 50 Gy after repeated treatments, in analogy with external-beam radiation therapy of the liver (31). The lung shunt fraction is usually calculated using the counts in a region of interest of the lungs, divided by the total counts in a region of interest of the lungs plus the liver (including tumor activity). However, this method is based on planar imaging and is operator- and institution-dependent. Overall, an absolute threshold (in Gy) is preferred over a relative one. Moreover, SPECT/CT leads to more accurate calculation of lung shunt absorbed dose than does planar imaging. Up to a 170% overestimation can occur when absorbed dose to the lung shunt is calculated on planar imaging compared with SPECT/CT imaging (31,32). Elschot et al. determined the lung shunt dose on planar imaging and SPECT/CT using 99mTc-MAA (150 MBq) and 166Ho-microspheres (250 MBq) (32). The true mean absorbed dose based on 166Ho SPECT/CT was 0.02 Gy. The absorbed dose was significantly overestimated by pretreatment planar imaging (99mTc-MAA, 5.5 Gy, and 166Ho, 10.4 Gy) and by 99mTc-MAA SPECT/CT (2.5 Gy). At present, no alternative for 99mTc-MAA is commercially available.
In the absence of significant extrahepatic activity, the only true dosimetric limitation left is the total absorbed radiation dose in healthy liver parenchyma, also called the nontumor dose. Little is known about the maximum tolerable nontumor dose in radioembolization. It varies between patients depending on multiple variables, including distribution of radiation within the nontumor volume. A nontumor dose limit of less than 70 Gy has been proposed (nontumor dose limit of less than 50 Gy in cirrhotic livers), although these limits seem quite arbitrarily defined and need to be confirmed in prospective studies (33). Nevertheless, pretreatment dosimetry is important to calculate the appropriate prescribed activity. Currently, 4 methods of calculating pretreatment activity are available for commercially available microspheres (Table 4) (33,34). For resin microspheres, the previously used activity calculation method was the empiric method. This method, which was based solely on tumor load, with no other patient-based factors, led to an unacceptable clinical and laboratory toxicity profile and was therefore abandoned (2,35). The second method, the body surface area method, is semiempiric and has been used safely in many clinical trials. Its main limitation is the absence of target volume in the calculation method, which can result in undertreatment (small patient with large liver) or overtreatment (large patient with small liver) (35,36). Furthermore, it does not correct for the individual intrahepatic distribution differences, calculated by the so-called tumor-to-nontumor ratio, which is to the disadvantage of patients with hyper- or hypovascular tumors. Theoretically, embedding the tumor-to-nontumor ratio in the activity calculation method for patients with hypervascular tumors will lead to a higher administered dose and higher tumor dose without compromising healthy liver tissue. The third calculation method, the so-called partition model, takes most relevant factors into account. Because the variables are acquired on 99mTc-MAA SPECT/CT before radioembolization, no additional procedures are needed (37,38). However, poorly defined tumors pose a problem for segmentation and quantification, and the overall complexity of the partition method renders its use less attractive in daily practice. For radioembolization using glass microspheres, an activity calculation method is advocated without the use of a tumor-to-nontumor ratio (34). In analogy to the discussion surrounding activity calculation for resin microspheres, the partition model based on prior 99mTc-MAA SPECT/CT has been shown feasible for glass microspheres as well (8).
Pretreatment Activity Calculation Methods
In daily practice, the body surface area method for resin microspheres and the volume-based calculation method for glass microspheres are the most commonly applied methods of calculating activity for radioembolization. Nonetheless, the partition model based on pretreatment 99mTc-MAA SPECT/CT should be preferred by nuclear physicians and interventional radiologists, because lesion-based dosimetry on pretreatment 99mTc-MAA SPECT/CT has been shown to correlate with response and survival (39–43). The aim of radioembolization is to deliver the highest possible absorbed dose to tumor cells (“tumor dose”) in order to induce apoptosis and tumor load reduction. The group of Garin et al. recently showed interesting results with the so-called partition method for treatment planning of glass microspheres. Treatment planning was based on a target tumor dose of more than 205 Gy and a nontumor dose of less than 120 Gy as calculated on 99mTc-MAA SPECT/CT. In 41 HCC patients with PVT (12/41 main branch), a median overall survival of 18 mo was found. Patients with a tumor dose of more than 205 Gy had significantly longer progression-free survival and overall survival (8). The rationale of tumor dose–response correlations has been supported by clinical studies in different settings (39,44). One should bear in mind, however, that partition modeling is based on 99mTc-MAA SPECT/CT, which is influenced by many factors, including discrepancies between 99mTc-MAA and 90Y-microsphere distribution (Fig. 2). Several alternatives to 99mTc-MAA are currently under investigation, mainly to avoid discrepancies based on morphologic differences between 99mTc-MAA and 90Y-microspheres and to improve lung shunt quantification (38).
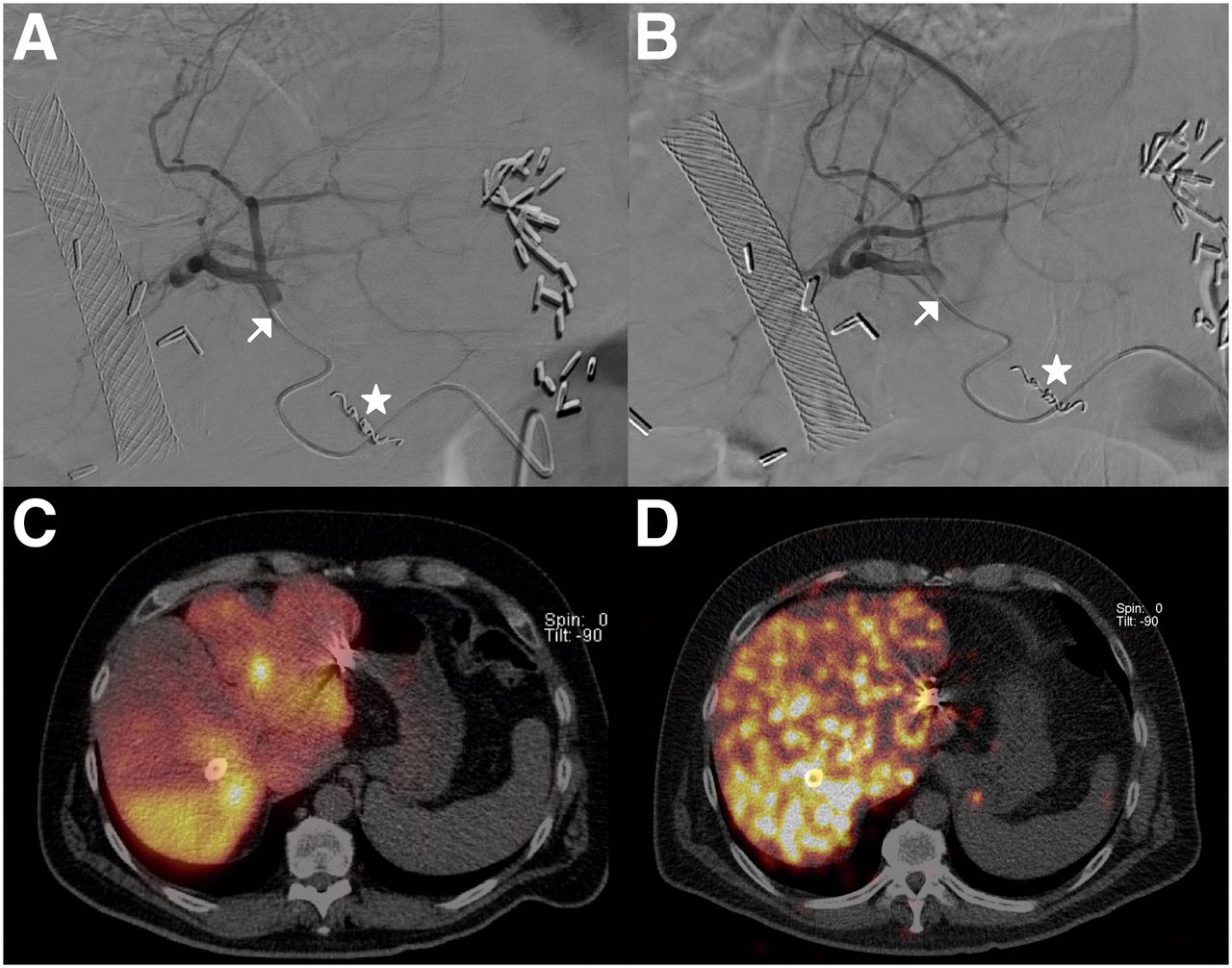
Patient with HCC recurrence in segment 7, who had previously undergone primary segmental resection with curative intent, cholecystectomy, and biliary stent placement. Gastroduodenal artery was coil-embolized (stars). Injection position is in left hepatic artery for 99mTc-MAA (A) and 90Y-resin microspheres (B) (subsequent injection position in right hepatic artery not shown). Discrepancy of distribution between 99mTc-MAA SPECT/CT (C) and 90Y PET/CT (D) can be acknowledged, with distribution in segment 4 being underestimated by 99mTc-MAA. These differences occurred even though the same 2-dimensional injection position was used in both angiographic procedures (arrows). Possible causes are the randomly shaped 99mTc-MAA vs. spheric microspheres, bolus injection 99mTc-MAA vs. intermittent injection 90Y-microspheres, in-plane (3-dimensional) catheter tip position differences, and different numbers of particles injected during scout dose, inducing differences in flow dynamics.
Because selective treatments are advocated to avoid extrahepatic deposition of activity, the prescribed activity needs to be split according to target volumes. A simple one-third (left lobe) and two-thirds (right lobe) split is used by some centers, but most centers use the pretreatment CT scan for splitting the prescribed activity according to their manual liver segmentation. The most accurate method was proposed by Kao et al., who split the dose according to artery-specific SPECT/CT-based liver segmentation, delineating an artery-specific target volume based on 99mTc-MAA distribution (37). C-arm cone-beam CT may also be used for that particular goal.
TREATMENT
During administration of resin microspheres, stasis of blood flow may occur, leading to incomplete injection of all intended microspheres. Stasis is caused by an embolic effect due to the higher number of resin microspheres (30–50 million) than of glass microspheres (4 million). The specific activity of resin microspheres (50 kBq/sphere) is approximately 50 times lower than that of glass microspheres (2,500 kBq/sphere), but this may vary by shelf-life. Although resin microspheres have a stable specific activity during a 24-h shelf-life, the specific activity (and number of microspheres) may vary for glass microspheres, having a maximum 2-wk shelf-life. It has been postulated that a more heterogeneous distribution of glass microspheres leads to a preferable toxicity profile but that, vice versa, a more homogeneous distribution of resin microspheres may lead to a preferable efficacy profile (45). The Northwestern University group in Chicago therefore advocated the use of so-called extended shelf-life glass microspheres (46). Microsphere characteristics are important to consider when analyzing dose–response relationships. It is not fully understood whether the antitumor effect is merely a radiation effect or a combination of an ischemic and radiation effect, especially in the case of resin microspheres. The embolic effect of resin microspheres sometimes leads to acute ischemic pain during injection. Recently, however, it was shown that when 5% glucose is used instead of sterile water for injection, there is less pain, less stasis, and more efficient administration. The flow dynamics during administration will be an important research topic in the coming years. Flow dynamics influence tumor targeting and the predictive value of a scout dose for dose distribution and treatment planning.
POSTTREATMENT IMAGING AND DOSIMETRY
Initially, 90Y-bremsstrahlung SPECT/CT was used after radioembolization to exclude extrahepatic activity deposition and to assess intrahepatic microsphere distribution. With 32 positrons per million decays, 90Y PET/CT imaging has gradually taken over 90Y-bremsstrahlung SPECT/CT, mainly because of new PET/CT scanners with time-of-flight technology. It allows more accurate quantification and dosimetry (47–49). Calculating tumor dose on posttreatment imaging may predict response (50–53). However, evidence was obtained in heterogeneous or small cohorts, mainly in HCC. Furthermore, the available studies differ in applied activity calculation method, used response criteria, and type of microsphere administered. Posttreatment imaging allows for detection of a heterogenic distribution of microspheres in the liver and in tumors, which correlates with partial or regional tumor response (49–51). In theory, after assessment of these parameters, additional radioembolization may be considered at an early stage, such as directly after administration of the treatment dose. However, the safety of repeated whole-liver radioembolization has not been firmly established yet (54,55).
Unfortunately, the true definition of the minimal effective tumor dose (and the maximum tolerated nontumor dose) remains a challenge. The reported tumor dose thresholds were found to be independent predictors of tumor response and survival, but lesion-based analyses on posttreatment imaging show that these numbers range widely (50,53). In a follow-up study of 56 HCC patients with 98 tumors, including a quantitative assessment on 90Y PET/CT after radioembolization with glass microspheres, lesion-based analysis yielded a mean tumor dose of 215 Gy (range, 17–555 Gy) in responders, defined as partial or complete response according to modified Response Evaluation Criteria in Solid Tumors (mRECIST), and a mean tumor dose of 167 Gy (range, 35–465 Gy) in nonresponders (53). The true minimal effective tumor dose remains unknown and needs to be further investigated for each tumor type, tumor size, and microsphere type used.
Besides tumor dosimetry, 90Y PET/CT allows early assessment of absorbed dose to healthy liver parenchyma: nontumor dose. At present, a nontumor dose of less than 70 Gy, or less than 50 Gy in cirrhotic livers, is assumed to be safe by the resin microsphere manufacturer (33). Nonetheless, a nontumor dose above these limits has been described. Using pretreatment dosimetry, a nontumor dose of less than 120 Gy on treatment planning was accepted for glass microspheres without additional toxicities (8). Like tumor dose, the maximum tolerated nontumor dose needs to be refined for baseline liver function, treatment history, tumor characteristics, and type of microsphere used.
CLINICAL OUTCOME AND TUMOR RESPONSE
In general, radioembolization is well tolerated. Mild clinical side effects usually occur within 4–6 wk after radioembolization (e.g., abdominal pain, nausea, vomiting, fatigue, and fever) (2). More serious complications (1–3 mo after radioembolization) include complications due to extrahepatic deposition of activity (e.g., gastric ulceration, pancreatitis, radiation pneumonitis) and liver decompensation. Excessive irradiation of healthy liver parenchyma leads to the most serious and life-threatening complication after radioembolization: radioembolization-induced liver disease. This is thought to be a venoocclusive disease/sinusoidal obstruction syndrome (56). Extensive sinusoidal congestion was acknowledged in liver biopsies, affecting the perivenular spaces with hepatic atrophy and necrosis around portal veins with fresh thrombus. In an early stage after radioembolization, serum markers show an induction of oxidative stress. Simultaneously, proinflammatory pathways are activated, resulting in endothelial injury with the activation of the coagulation cascade (57). Jaundice and ascites, in the absence of tumor progression or bile duct dilatation, are the main symptoms of radioembolization-induced liver disease (56,58). General risk factors for developing radioembolization-induced liver disease include prior chemotherapy, low tumor burden, high baseline bilirubin values, and cirrhotic liver disease (56,58).
Table 5 features the efficacy results of several landmark studies in the field of radioembolization.
Landmark Studies on Response and Survival in Liver Malignancies
In the intermediate and early-advanced stages of HCC (respectively, BCLC B and BCLC C), radioembolization has shown favorable outcomes compared with the currently preferred treatments (59,60). Compared with TACE, radioembolization has a similar or even better objective response rate and similar survival statistics (60). Moreover, as previously discussed, PVT and bilidigestive anastomoses are no absolute contraindication. Additionally, an ECOG performance score of at least 1 and a large tumor size (>10 cm) are currently considered a contraindication for TACE, in contrast to radioembolization (ECOG performance score ≤ 2, no tumor size limitation) (61). Radioembolization seems to effectively reduce the size of large tumors (Fig. 3), and response rates of up to 91% have been described (8).

Patient with large HCC (12 cm) in right lobe on T1-weighted MR imaging sequences in coronal plane: before radioembolization (A); tumor shrinkage after radioembolization (B); T1-weighted gadolinium-enhanced MR image with fat suppression in axial plane during arterial phase (20 s after injection), illustrating hypervascular tumor (C); large area of necrosis in tumor on same sequence after radioembolization (D).
In BCLC B or BCLC C, not suitable for TACE, the current recommendation is systemic treatment with the multikinase inhibitor sorafenib. However, these patients might benefit more from radioembolization than from sorafenib. Recently, a large study (62) showed significantly better response rates and fewer adverse events after radioembolization than after sorafenib, even after correction of confounders (Table 5); survival was similar. Patients are currently being recruited for the YES-P, SARAH, and SIRVENIB trials, in which sorafenib and radioembolization will be compared in a randomized controlled setting. The results of a phase II study in the Asia-Pacific trial indicate that combining both treatments seems beneficial, with manageable toxicities (63). This is currently under investigation in the SORAMIC trial (resin microspheres) and the STOP-HCC trial (glass microspheres). Patients who are ineligible or poor candidates for TACE are randomized into 2 groups: a group receiving sorafenib combined with radioembolization and a group receiving sorafenib alone. Even though radioembolization is currently not incorporated into the BCLC scheme and the results of the above-mentioned trials are pending, for selected patients radioembolization can be positioned between TACE and sorafenib (Fig. 4).
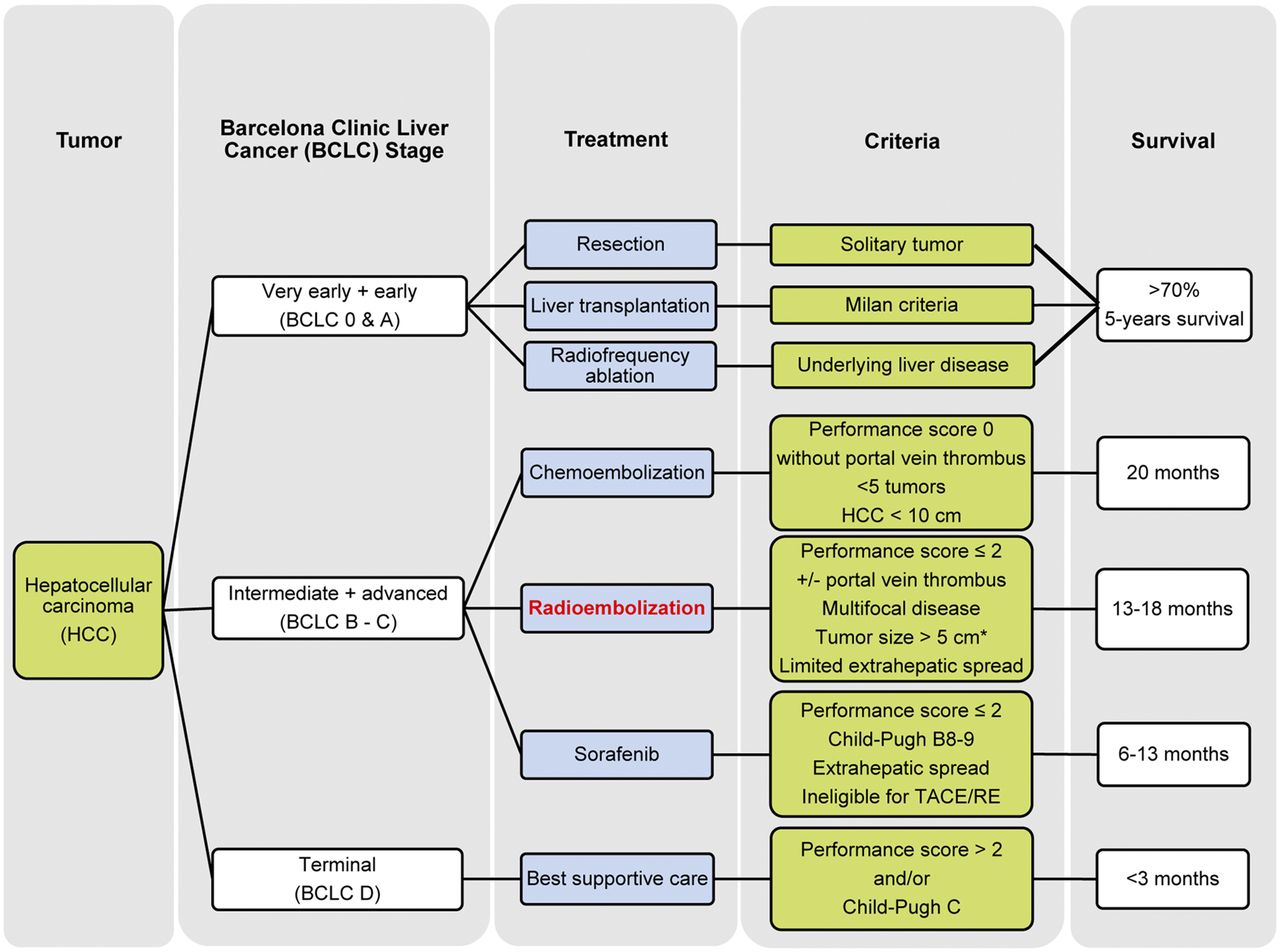
BCLC staging system with proposal for radioembolization in treatment paradigm. Because the applicability of radioembolization in intermediate- and advanced-stage HCC overlaps, these stages have been combined in this proposal. *Size of tumors has been included in this BCLC scheme; however, exact size limits need to be investigated further.
In patients with focal or limited disease, ineligible for surgical resection or radiofrequency ablation, radioembolization using glass microspheres may provide an interesting alternative: radiation segmentectomy is meant to provide an ablating radiation dose (>200 Gy) by selective or superselective catheterization. By selective targeting, necrosis is induced in a limited portion of the liver, including the tumor, thus sparing radiation to healthy liver parenchyma. Vouche et al. described a high objective response rate (88%) and median overall survival (53.4 mo) using this technique in solitary HCCs smaller than 5 cm (64). In their cohort, 33% of patients were amenable to liver transplantation after radiation segmentectomy. At pathologic examination of the native liver specimens, 100% necrosis and more than 90% necrosis were found in, respectively, 52% and 48% of patients (64). In HCC, the downstaging success rate with radioembolization is around 50% (range, 29%–67%), with a median time to downstaging of 3.1–4 mo (65). In downstaging HCC, radioembolization is a suitable alternative to TACE, but downstaging should not be restricted to HCC alone (65).
The current European Society for Medical Oncology guideline on metastatic colorectal cancer states that in patients with liver-limited disease and unresectable liver metastases failing available chemotherapeutic regimens, radioembolization using resin microspheres prolongs time to tumor progression (66). Results in heavily pretreated patients with chemoresistant metastatic colorectal cancer have been consistent over the years, making salvage treatment with radioembolization a widely accepted indication. According to a recent systematic review, treated patients have failed a median of 3 chemotherapeutic regimens before radioembolization (67). Left untreated, patients with chemorefractory liver metastases have a median survival of only 5–7 mo (68–70). Nonetheless, in this population with an overall poor prognosis, after radioembolization a mean objective response rate of 31%, median progression-free survival of 9 mo, and median overall survival of 12 mo are obtained (Table 5) (67). Several ongoing randomized controlled trials are establishing the role of radioembolization for metastatic colorectal cancer (Fig. 5). The addition of radioembolization to first-line chemotherapy regimens is being investigated in the SIRFLOX, FOXFIRE, and SIR-step trials (all using resin microspheres). After first-line failure, the EPOCH trial will randomize patients in second-line chemotherapy with or without radioembolization (glass microspheres).

Schematic of evolving application of radioembolization in metastatic colorectal cancer and current trials. At present, radioembolization is applied mainly in the salvage setting; however, many clinical trials focus on bringing radioembolization to the forefront of the metastatic colorectal cancer treatment algorithm in the first- or second-line setting.
Another relatively new application of radioembolization before surgical resection is the induction of hypertrophy of the contralateral lobe by radioembolization of the diseased lobe. After portal vein embolization, 17.5% of patients are ineligible for surgical resection because of tumor progression, and in 4.8% of patients, hypertrophy induction of the future liver remnant is insufficient (71). Compared with portal vein embolization, induction of hypertrophy by radioembolization is similar but takes longer. A degree of hypertrophy of approximately 35% (8.9%–57%) can be obtained in 3–4 mo (65). Theoretically, the main benefit of radioembolization is simultaneous tumor treatment, reducing the number of dropouts due to disease progression.
Unresectable intrahepatic cholangiocarcinoma, left untreated, has an overall survival of less than 8 mo, and with gemcitabine and cisplatin overall survival is 11.7 mo (72,73). After radioembolization, overall survival of 15.5 mo can be reached (72). Repeated radioembolization can lead to local disease control for a longer period (Supplemental Fig. 1; supplemental materials are available at http://jnm.snmjournals.org). Radioembolization before surgical resection, as in HCC and metastatic colorectal cancer, could be promising in intrahepatic cholangiocarcinoma as well. Downstaging occurs in 10%, and inducing contralateral hypertrophy seems feasible (65,72). In a small cohort combining radioembolization with chemotherapy, downstaging occurred in 22%, significant hypertrophy of the contralateral lobes was seen in all patients, and 18% were radically resected (74). In general, these results for intrahepatic cholangiocarcinoma are promising, but current literature is limited.
The heterogeneous group of neuroendocrine tumors has a lower incidence than the aforementioned tumors, though hepatic involvement in neuroendocrine tumors is common and is the greatest incriminating factor in survival (disease-free survival, 20 mo with >4 hepatic metastases, vs. 46 mo with ≤4 hepatic metastases) (75). Most patients present with multifocal hepatic disease and are ineligible for resection or radiofrequency ablation (76). Conventional treatments (i.e., somatostatin analogs) and newer biologicals (i.e., sunitinib and everolimus) improve survival, but the objective response rate is poor. Because of the hypervascular nature of hepatic metastases, neuroendocrine tumors are prime candidates for radioembolization. In a metaanalysis including 414 patients, the pooled objective response rate was 50%, disease control rate was 86%, and overall survival was 28.5 mo (Table 5) (77). Data reporting response rates based on the primary tumor origin and according to the World Health Organization histologic grading system are needed.
CONCLUSION
Hepatic 90Y radioembolization continues to develop rapidly. Clinical research is expanding indications in many different tumor types, overcoming technical angiographic challenges, fine-tuning the application of dosimetry, and optimizing quantitative imaging in daily practice.
Footnotes
Published online May 7, 2015.
Learning Objectives: On successful completion of this activity, participants should be able to (1) describe the status of the current literature regarding new indications for radioembolization; (2) describe standard hepatic vascularization, identify common routes for extrahepatic depositions, and judge when “skeletization” of hepatic arteries could be unnecessary; and (3) appraise the different methods of activity calculation and recognize the strengths and pitfalls of pretreatment and posttreatment dosimetry.
Financial Disclosure: Dr. Lam is a consultant/advisor for BTG International and a meeting participant/lecturer for SirTex Medical. The authors of this article have indicated no other relevant relationships that could be perceived as a real or apparent conflict of interest.
CME Credit: SNMMI is accredited by the Accreditation Council for Continuing Medical Education (ACCME) to sponsor continuing education for physicians. SNMMI designates each JNM continuing education article for a maximum of 2.0 AMA PRA Category 1 Credits. Physicians should claim only credit commensurate with the extent of their participation in the activity. For CE credit, SAM, and other credit types, participants can access this activity through the SNMMI website (http://www.snmmilearningcenter.org) through July 2018.
- © 2015 by the Society of Nuclear Medicine and Molecular Imaging, Inc.
REFERENCES
- 1.↵
- 2.↵
- 3.↵
- 4.↵
- 5.↵
- 6.↵
- 7.↵
- 8.↵
- 9.↵
- 10.
- 11.
- 12.↵
- 13.↵
- 14.↵
- 15.↵
- 16.↵
- 17.↵
- 18.↵
- 19.↵
- 20.↵
- 21.↵
- 22.↵
- 23.↵
- 24.↵
- 25.↵
- 26.↵
- 27.↵
- 28.↵
- 29.↵
- 30.↵
- 31.↵
- 32.↵
- 33.↵
- 34.↵
- 35.↵
- 36.↵
- 37.↵
- 38.↵
- 39.↵
- 40.
- 41.
- 42.
- 43.↵
- 44.↵
- 45.↵
- 46.↵
- 47.↵
- 48.
- 49.↵
- 50.↵
- 51.↵
- 52.
- 53.↵
- 54.↵
- 55.↵
- 56.↵
- 57.↵
- 58.↵
- 59.↵
- 60.↵
- 61.↵
- 62.↵
- 63.↵
- 64.↵
- 65.↵
- 66.↵
- 67.↵
- 68.↵
- 69.
- 70.↵
- 71.↵
- 72.↵
- 73.↵
- 74.↵
- 75.↵
- 76.↵
- 77.↵
- 78.
- 79.↵
- 80.↵
- Received for publication March 12, 2015.
- Accepted for publication April 25, 2015.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- PET/CT and SPECT/CT imaging of 90Y hepatic radioembolization at therapeutic and diagnostic activity levels: anthropomorphic phantom study
- Lung Dose Measured on Postradioembolization 90Y PET/CT and Incidence of Radiation Pneumonitis
- A Pilot Study on Hepatobiliary Scintigraphy to Monitor Regional Liver Function in 90Y Radioembolization
- Optimization of Image Reconstruction for 90Y Selective Internal Radiotherapy on a Lutetium Yttrium Orthosilicate PET/CT System Using a Bayesian Penalized Likelihood Reconstruction Algorithm
- Insights into the Dose-Response Relationship of Radioembolization with Resin 90Y-Microspheres: A Prospective Cohort Study in Patients with Colorectal Cancer Liver Metastases