


Visual Abstract

Abstract
Fibroblast-activation protein is a promising target for oncologic molecular imaging. Studies show that fibroblast activation protein inhibitor (FAPI) radiotracers are accurate diagnostics with favorable tumor-to-background ratios across various cancers. Therefore, we performed a systematic review and metaanalysis to assess the diagnostic performance of FAPI PET/CT in comparison with [18F]FDG PET/CT, the most widely used radiotracer in oncology. Methods: We conducted a systematic search in MEDLINE, Embase, Scopus, PubMed, Cochrane Central Register of Controlled Trials, relevant trial registries, and bibliographies. The search consisted of combinations of terms for 3 topics: neoplasia, PET/CT, and FAPI. Two authors independently screened retrieved articles using predefined inclusion and exclusion criteria and extracted the data. Study quality was assessed using the criteria of QUADAS-2 (Quality Assessment of Diagnostic Accuracy Studies 2). For each study, the sensitivity, specificity, and 95% CIs were calculated to determine diagnostic accuracy for primary, nodal, and metastatic lesions. A random-effects metaanalysis was used for pooling the data, and heterogeneity was assessed (I2 index). Results: Thirty-nine studies (1,259 patients) investigating the use of FAPI PET/CT were included. On a patient-based analysis, pooled sensitivity was 0.99 (95% CI, 0.97–1.0) for the detection of primary lesions. Pooled sensitivity for nodal and distant metastases was 0.91 (95% CI, 0.81–0.96) and 0.99 (95% CI, 0.96–1.0), respectively. On a paired analysis between FAPI and [18F]FDG PET/CT, FAPI had a higher sensitivity in the detection of primary, nodal, and metastatic lesions (all P < 0.001). The differences in sensitivities between FAPI and [18F]FDG were statistically significant. In terms of heterogeneity, analyses on primary lesions were moderately affected, distant metastatic lesions were highly affected, and the nodal metastatic analyses had negligible heterogeneity. Conclusion: The diagnostic performance of FAPI PET/CT is superior to that of [18F]FDG in the detection of primary, nodal, and distant metastases. However, further studies are needed to better evaluate its utility and indication in specific cancer types and clinical settings.
PET scans are used in the diagnosis and staging of various cancers, with [18F]FDG the most widely used radiotracer (1). The glucose analog FDG utilizes the increased glucose demand of many tumors (Warburg effect); however, this can result in nonspecific uptake in glucose-avid organs or areas of inflammation (1). More recent research into the tumor microenvironment resulted in the development of fibroblast activation protein inhibitor (FAPI) radiotracers, such as [68Ga]FAPI-04 (2). This protein is a type II transmembrane serine protease that is overexpressed on cancer-associated fibroblasts, a heterogeneous population of fibroblastlike cells and a predominant component of the tumor microenvironment (2,3). These fibroblasts are implicated in several aspects of tumorigenesis, such as immunosuppression and extracellular matrix remodeling (3,4). This protein is also expressed in wound healing, in inflammatory conditions such as arthritis, in fibrosis, and in areas of extracellular matrix remodeling such as myocardial infarction and liver cirrhosis (3,5,6). Fibroblast activation protein is detected during embryogenesis and tissue remodeling but is otherwise expressed at low levels in healthy tissue (3,5). Studies show fibroblast activation protein expression on tumor cells, with increased expression correlating with poorer prognosis (7). These features make fibroblast activation protein an attractive target for oncologic imaging.
Since FAPI radiotracers were first described in 2018 (8), multiple studies have investigated their diagnostic accuracy in the detection of various cancers, reporting high accuracy and favorable tumor-to-background ratios (9,10). Comparisons are made between FAPI PET/CT, [18F]FDG PET/CT, and other imaging modalities (CT and MRI) (11,12). There are currently 4 metaanalyses investigating the diagnostic accuracy of FAPI PET (13–16). Compared with prior analyses, this current metaanalysis includes a larger number of studies, covering multiple cancer types, and directly comparing FAPI and [18F]FDG PET/CT.
This systematic review and metaanalysis synthesize the current literature on various FAPI radiotracers and the diagnostic accuracy of FAPI PET/CT in comparison with [18F]FDG PET/CT for the detection of cancers and associated metastatic lesions.
MATERIALS AND METHODS
Literature Search
We conducted this systematic review and metaanalysis in line with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines. The study protocol is registered in PROSPERO (International Prospective Register of Systematic Reviews) (CRD42021270480).
A systematic search of the literature on FAPI PET/CT was performed in November 2021 and updated in April 2022. Relevant studies were identified from the following electronic databases: MEDLINE, Embase, Scopus, PubMed, and the Cochrane Central Register of Controlled Trials. To identify trials, we searched the U.S. National Institutes of Health Ongoing Trials Register, World Health Organization International Clinical Trials Registry Platform, and the Australian New Zealand Clinical Trials Registry. The search strategy utilized medical subject headings and free-text terms centered around neoplasia, PET/CT, and FAPI. No language or publication period limitations were used in the search. Additional studies were manually retrieved through citation searches and the reference lists of included articles.
Eligibility Criteria
We applied the following criteria for study inclusion: use of FAPI PET/CT imaging for suspected or proven tumors (initial detection, staging, or recurrence detection), adult participants (≥18 y), tumor presence confirmed by reference standard (histopathologic or imaging), data available for primary outcome, and studies with ethical approval. The following were excluded: nonhuman studies, studies in fields other than oncology, case reports, review articles, editorials, letters, commentaries, and conference proceedings.
Data Extraction
All identified studies were screened using the predefined eligibility criteria by 2 investigators. Studies were screened first for inclusion or exclusion using titles and abstracts and then using full texts. A third investigator resolved any discrepancies in study inclusion and exclusion. If studies had insufficient data to construct 2 × 2 contingency tables, the corresponding authors were contacted for data before the study was excluded. If 2 or more studies by the same group had overlapping study periods and populations, the study with the largest cohort was included. In these cases, the corresponding authors were also contacted to check for any potential study overlap.
We extracted the following data: publication details, study design, study methodology, patient demographics, imaging modalities used, number of accurately diagnosed primary and metastatic lesions, number of accurately diagnosed lesions, number of inaccurately diagnosed primary and metastatic lesions, number of inaccurately diagnosed lesions, and PET radiopharmaceuticals used. If the studies did not report the raw diagnostic data, we reconstructed 2 × 2 tables from the diagnostic estimates given in the text.
Study Quality Assessment
All included studies were screened and assessed for quality using the QUADAS-2 (Quality Assessment of Diagnostic Accuracy Studies 2) criteria by 2 of the investigators independently. The risk of bias and applicability were evaluated for patient selection, index test, and reference standard, with the flow and timing domain being used only to assess bias.
Data Synthesis and Statistical Analysis
We assessed the diagnostic performance of FAPI PET/CT and [18F]FDG PET/CT for primary tumors (patient-based and lesion-based), lymph nodes, and metastases. We calculated sensitivity, specificity, and 95% CIs for each study and determined the pooled relative diagnostic accuracy of FAPI PET/CT and [18F]FDG PET/CT with a random-effects metaanalysis. Analyses were performed using a frequentist framework in R (version 4.1.2) with lme4, meta, and lmtest packages. Data were summarized and presented in paired forest plots and summary receiver-operating characteristic curves for each analysis using Revman (version 5.4, ReviewManager). Heterogeneity was evaluated using general linear models to evaluate between-study variance. Publication and any other potential biases were assessed visually using funnel plots. A P value of 0.05 or less was considered statistically significant.
RESULTS
Study Selection and Characteristics
Electronic database searches identified 1,272 articles. Duplicate screening removed 688 articles, and a further 507 articles were removed after title and abstract screening, resulting in full-text retrieval of 77 relevant articles. After full-text review, 39 studies met the inclusion criteria, constituting 1,259 patients. Nineteen studies were excluded because of insufficient data, 17 studies had overlapping populations, and 2 studies investigated only dual-tracer scans (Fig. 1).

Flowchart of study inclusions.
Study quality was assessed using the QUADAS-2 criteria (Fig. 2). The main issues in study quality were uncertainty about consecutive enrollment, lack or uncertainty of masking, lack of inclusion of all patients in the final analysis, and the use of different reference standards.

QUADAS-2 criteria assessment results for included studies. Judgments about each domain are presented as percentages, and number of studies is presented within bars.
Systematic Review
Study demographic and index test characteristics are summarized in Table 1 and Supplemental Table 1, respectively (supplemental materials are available at http://jnm.snmjournals.org). The included studies were published between 2020 and 2022. Twenty-four studies were prospective, and 15 were retrospective. More than half the studies were conducted in China. The included studies focused on gastrointestinal cancers (12,17–31), head and neck cancer (11,32–36), various cancers (9,10,37–41), lung cancer (42,43), sarcoma (44,45), breast cancer (46), lymphoma (47), multiple myeloma (48), glioblastoma (49), and liver metastases (50,51).
Study Demographics
PET/CT was used as the index test imaging modality in 34 studies, PET/MRI was used in 3 studies, and both PET/CT and PET/MRI were used in 2 studies. The studies used various FAPI ligands (FAPI-02, FAPI-04, FAPI-42, FAPI-46, DOTA.SA.FAPI, and DATA5m.SA.FAPI) and isotopes (18F and 68Ga). The injected activity of the radiotracer varied among studies (Supplemental Table 1). The most common acquisition time was 60 min (24 studies), 5 studies used acquisition times shorter than 60 min, and 10 studies used a range of acquisition times (30–113 min) (Supplemental Table 1). The FAPI scans were compared with [18F]FDG in 34 studies, MRI in 3 studies, contrast-enhanced CT in 2 studies, and a second FAPI ligand in 1 study; 2 studies had no comparator.
Metaanalysis
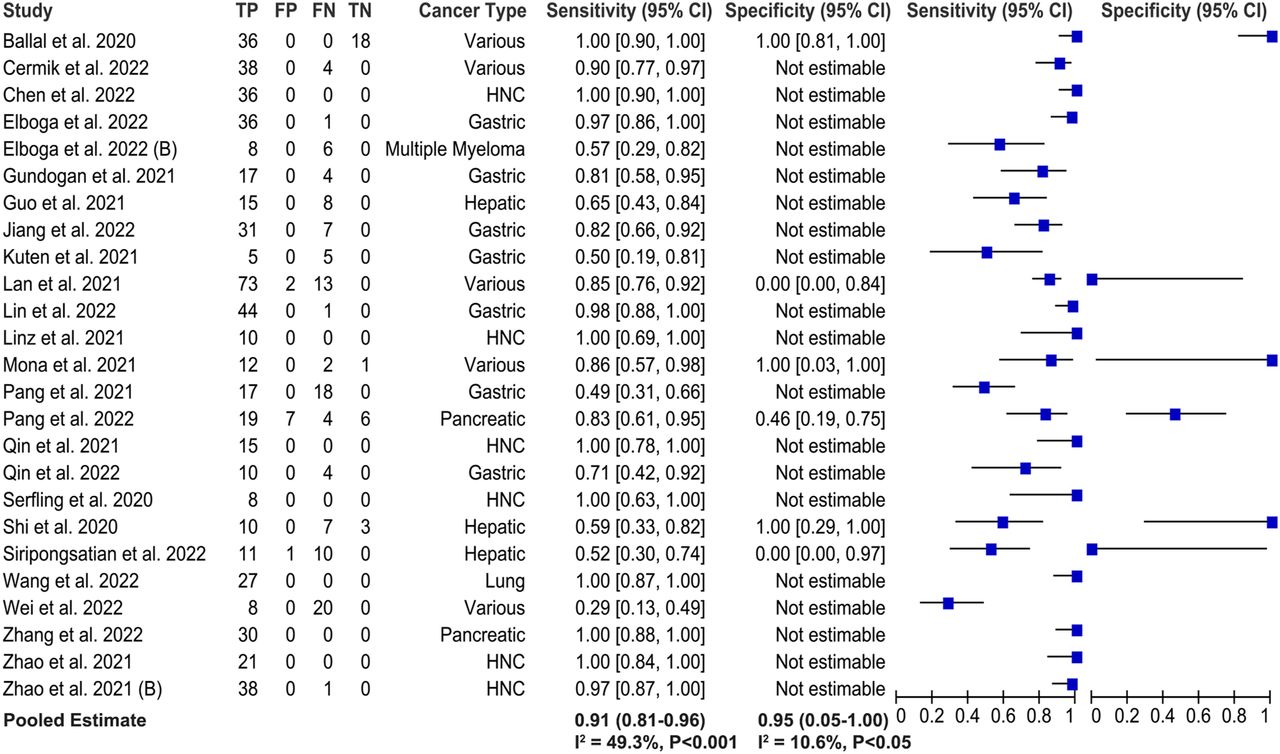
We used per-patient data for primary lesions and per-lesion data for the nodal and distant metastatic lesions. The overall pooled sensitivity of FAPI was 0.99 (95% CI, 0.97–1.00; heterogeneity index [I2] = 34.5%), 0.91 (95% CI, 0.81–0.96; I2 = 0.0%), and 0.99 (95% CI, 0.96–1.00; I2 = 96.8%) for the detection of primary, nodal, and distant metastatic lesions, respectively (Fig. 3; Supplemental Fig. 1). The overall pooled specificity of FAPI was 0.84 (95% CI, 0.28–0.99; I2 = 50.1%) for the detection of primary lesions. The forest plot in Figure 3 shows the pooled estimates of sensitivity and specificity for the detection of primary lesions. The estimated metastatic pooled per-lesion sensitivity was not reliable because of high heterogeneity (I2 = 96.8%). Forest plots for the detection of nodal and distant metastases and summary receiver-operating characteristic curves are shown in Supplemental Figures 1 and 2, respectively. The limited number of studies reporting true-negative data reduced the certainty of the pooled specificity results.

Forest plot showing random-effects estimates and individual study sensitivity and specificity for detection of primary lesions by FAPI PET/CT. FN = false-negative; FP = false-positive; HNC = head and neck cancer; TN = true-negative; TP = true-positive.
A paired analysis including studies comparing both radiotracers showed that sensitivity was higher for FAPI than for [18F]FDG in the detection of primary lesions (1.00 [95% CI, 0.95–1.00] vs. 0.91 [95% CI, 0.81–0.96]), nodal metastases (0.91 [95% CI, 0.81–0.96] vs. 0.78 [95% CI, 0.66–0.87]), and distant metastatic lesions (0.99 [95% CI, 0.96–1.00] vs. 0.73 [95% CI, 0.53–0.87]). There was a significant difference in sensitivity between FAPI and [18F]FDG in the detection of primary lesions (P < 0.001), nodal metastases (P < 0.001), and distant metastatic lesions (P < 0.001). The study estimates of sensitivity and specificity for the detection of primary lesions by [18F]FDG PET/CT are shown in Figure 4, and paired summary receiver-operating characteristic curves are shown in Figure 5. The paired analysis for primary lesions had moderate heterogeneity (I2 = 29.0% for FAPI; I2 = 49.3% for [18F]FDG), nodal metastases had negligible heterogeneity (I2 = 0.0% for both), and metastatic lesions had high heterogeneity (I2 = 96.8% for FAPI; I2 = 96.6% for [18F]FDG). The overall pooled specificity for the detection of primary lesions was higher for [18F]FDG than for FAPI (0.95 [95% CI, 0.05–1.00] vs. 0.87 [95% CI, 0.05–1.00]); however, the limited number of studies reporting true-negative data reduced the certainty of the specificity analyses. Forest plots for the detection of nodal and distant metastases are shown in Supplemental Figure 3. Funnel plot asymmetry (Supplemental Figs. 4–6) suggests slight study bias, particularly for lymph node and metastatic analyses.

Forest plot showing random-effects estimate and individual study sensitivity and specificity for detection of primary lesions by [18F]FDG PET/CT. FN = false-negative; FP = false-positive; HNC = head and neck cancer; TN = true-negative; TP = true-positive.

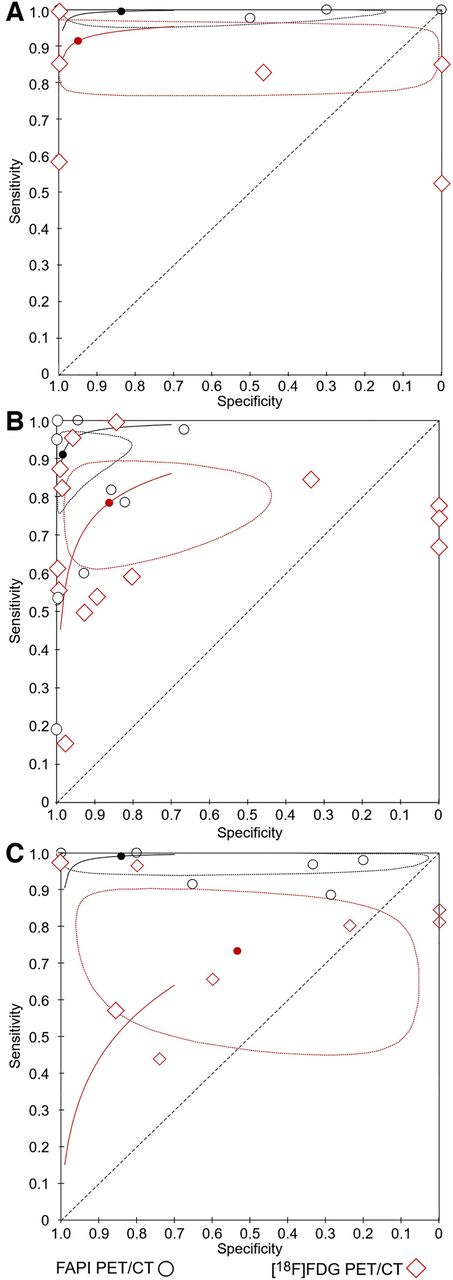
Summary receiver-operating characteristic curve analysis comparing diagnostic performance of FAPI PET/CT and [18F]FDG PET/CT for studies that reported on both tracers: primary lesions (A), nodal metastases (B), and metastatic lesions (C). Each circle represents FAPI PET/CT data, and each diamond represents [18F]FDG PET/CT data for individual study. Shaded circles represent summary points, and dotted circles show 95% CIs.
A subgroup analysis comparing FAPI and [18F]FDG PET/CT in gastrointestinal cancers demonstrated that FAPI PET/CT had a higher sensitivity (1.00 [95% CI, 0.84–0.99] vs. 0.81 [95% CI, 0.66–0.90]) and specificity (0.54 [95% CI, 0.05–0.96] vs. 0.52 [95% CI, 0.26–0.77]) than [18F]FDG PET/CT in the detection of primary gastrointestinal lesions (Supplemental Fig. 7). There was a significant difference in sensitivity between [18F]FDG and FAPI (P < 0.001), but not specificity (P = 0.42), and both analyses had high heterogeneity (I2 = 87.9% and I2 = 87.8%, respectively). FAPI PET/CT had a higher sensitivity than [18F]FDG PET/CT in the detection of nodal [0.90 (95% CI, 0.65–0.98) vs 0.64 (95% CI, 0.43–0.81)] and distant (0.99 [95% CI, 0.88–0.99] vs. 0.61 [95% CI, 0.43–0.78]) metastatic lesions in gastrointestinal cancers (Supplemental Figs. 8 and 9). Both analyses were significant (P < 0.001), and they had moderate (I2 = 57.9%) and high (I2 = 98.2%) heterogeneity, respectively.
DISCUSSION
This systematic review and metaanalysis showed that FAPI is highly sensitive in the detection of primary, nodal, and metastatic lesions. We demonstrated that FAPI is significantly more sensitive than [18F]FDG for primary, nodal, and metastatic lesions, across studies examining both radiotracers. Our analyses showed that [18F]FDG had a higher specificity than FAPI for the detection of primary lesions; however, the lack of studies reporting true-negative data reduces our confidence in pooled specificities.
Several metaanalyses investigated the diagnostic accuracy of FAPI PET/CT in the detection of oncologic lesions (13–16). Compared with previous metaanalyses, our comprehensive analysis provides an up-to-date evaluation of the diagnostic applicability of FAPI PET/CT radiotracers and a direct comparison to [18F]FDG PET/CT for primary lesions, nodal metastases, and distant metastases.
An early metaanalysis of 14 studies on [68Ga]FAPI by Sollini et al. (13) reported a patient-based pooled sensitivity and specificity of 0.99 and 0.87, respectively. On a lesion-based analysis, they reported sensitivities of 1.00 and 0.93 for the detection of primary and distant metastases, respectively. However, the results were highly heterogeneous, and the study design of the included papers prevented the calculation of pooled specificity for both primary tumors and metastases. Our lesion-based analysis for the detection of distant metastases was also heterogeneous (I2 = 96.6%). Sollini et al., however, did not report or compare [68Ga]FAPI PET/CT with [18F]FDG PET/CT or other imaging modalities (13). A metaanalysis by Roustaei et al. directly compared the detection rates of [68Ga]FAPI and [18F]FDG PET using odds ratios (OR) and risk differences for various cancers across 9 studies (14). They found that gastrointestinal tumors had the highest estimated OR (32.079; 95% CI, 4.001–257.212; P = 0.001) for the detection of primary tumors (14). For nodal and distant metastases, they found that hepatobiliary tumors (OR, 11.609) and nasopharyngeal carcinomas (OR, 77.451) had the highest ORs, respectively (14). Their analysis of different cancer types had high heterogeneity, similar to our analysis of distant metastases across various cancer types (14). Gege et al. compared [68Ga]FAPI and [18F]FDG PET/CT for the detection of peritoneal metastases, showing [68Ga]FAPI to have superior sensitivity in both patient-based analysis (98.2% vs. 55.9%, 9 studies) and lesion-based analyses (99.9% vs. 27.35, 4 studies) (15). Finally, Huang et al. analyzed the detection rates of [68Ga]FAPI in digestive system tumors in 18 studies (16), reporting a patient-based sensitivity of 0.98 and a lesion-based sensitivity of 0.97 (16), as well as a pooled sensitivity of 0.94 for the detection of nonprimary (lymph node and distant metastases) lesions (16). Specificity was statistically pooled by neither Gege et al. nor Huang et al. because of a lack of true-negative data, a common limitation in these diagnostic studies (15,16).
FAPI PET/CT appears to be a promising diagnostic radiotracer for tumors and lesions that are inconclusive on [18F]FDG imaging, such as tumors in the gut and liver with variable [18F]FDG uptake due to metabolic alterations (24). A study by Chen et al. (9) showed that [68Ga]DOTA-FAPI PET/CT had higher tumor uptake and a more favorable tumor-to-background ratio in tumors with inconclusive [18F]FDG findings.
Our metaanalysis has some limitations. First, because of the limited number of studies available on FAPI PET/CT, we included all studies that used FAPI PET/CT in an oncologic setting. These studies were heterogeneous, with various cancers and patients. As study of FAPI PET/CT continues, further analyses can be conducted on specific cancer types to better determine its diagnostic utility. Second, a small number of studies reporting true-negative data resulted in wide pooled CIs for specificity and limited conclusions on overall diagnostic accuracy. The fact that some studies also excluded patients with benign disease or included only patients who already had a confirmed malignancy highlights the need for adequate studies on patients who do not have histologic confirmation of cancer. Third, in terms of the detection of nodal and metastatic lesions, patients in some studies had already undergone treatment whereas others were treatment-naïve, which may underestimate FAPI’s ability to detect these treated lesions. Finally, many of the included studies were retrospective or focused on tumors with suboptimal [18F]FDG sensitivity, resulting in a risk of pretest selection bias.
CONCLUSION
This systematic review demonstrates that FAPI has high sensitivity in the detection of primary and nodal lesions. Additionally, the sensitivity of FAPI in the detection of primary, nodal, and metastatic lesions was significantly higher than that of [18F]FDG across various cancers. However, our findings on distant metastases were biased by high heterogeneity. Although FAPI is a promising radiotracer, the high risk of bias and study heterogeneity suggest that further trials are required to evaluate the role of FAPI in an oncologic setting and its utility alongside or over [18F]FDG PET/CT.
DISCLOSURE
This study was supported by the Department of Medicine, Dunedin School of Medicine, University of Otago Medical School, Dunedin, New Zealand. No other potential conflict of interest relevant to this article was reported.
KEY POINTS
QUESTION: What is the diagnostic accuracy of FAPI PET/CT alone and compared with [18F]FDG PET/CT for the detection of primary and metastatic lesions?
PERTINENT FINDINGS: This systematic review and metaanalysis found that FAPI has high sensitivity in the detection of primary lesions (0.99; 95% CI, 0.97–1.00), nodal metastases (0.91; 95% CI, 0.81–0.96), and distant metastases (0.99; 95% CI, 0.96–1.00). In a paired analysis, the sensitivity of FAPI was superior to that of [18F]FDG PET/CT, with statistical significance.
IMPLICATIONS FOR PATIENT CARE: These findings show that FAPI is a promising radiotracer in oncology, but further studies are required to better evaluate its indications and role.
Footnotes
Published online Jun. 8, 2023.
- © 2023 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication February 2, 2023.
- Revision received April 14, 2023.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}