


The value of in vivo peptide receptor targeting for imaging and treating oncologic patients is well accepted and implemented in clinical practice. A prime example is somatostatin receptor (SSTR)–targeted peptide receptor radionuclide therapy (PRRT), which relies on an image-and-treat approach (theranostics), a rapidly evolving clinical concept in patients with neuroendocrine tumors (NETs).
SSTR agonists are internalized after high-affinity ligand receptor binding and have historically been used for in vivo SSTR receptor targeting. This mechanism is considered an essential step in in vivo receptor targeting using SSTR agonists (Fig. 1). The evolving PET/CT technology and the optimization of radiopharmaceutical chelation for effective somatostatin analog development opened the door to [68Ga]Ga-DOTA0-Tyr3-octreotate ([68Ga]Ga-DOTATATE) PET/CT. In 2016, [68Ga]Ga-DOTATATE received Food and Drug Administration approval for SSTR imaging, followed by [68Ga]Ga-DOTATOC and [64Cu]Cu-DOTATATE in 2019 and 2020, respectively. SSTR-based PRRT was explored by the phase 3 NETTER-1 trial, a first-in-humans prospective multicenter randomized clinical trial comparing [177Lu]Lu-DOTATATE (4 cycles, 7.4 GBq/cycle) with high-dose octreotide in 229 patients with progressive low-grade midgut NETs.

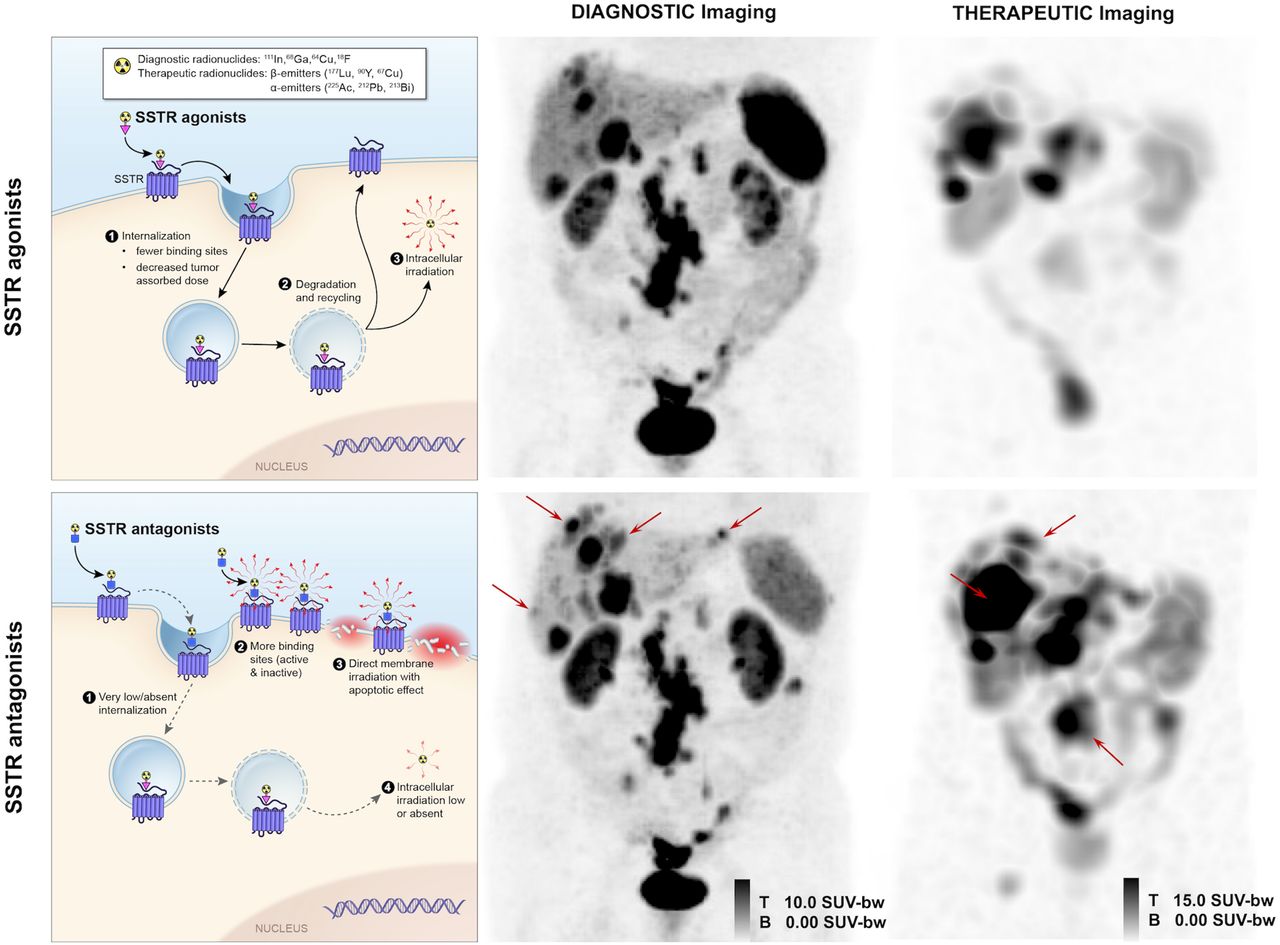
(Left) Mechanism of action of radiolabeled SSTR agonists and antagonists for theranostics application. SSTR agonists are internalized after binding to SSTR2, with consequent accumulation of radioactivity in cell. In contrast, SSTR antagonists bind more effectively to receptors on cell membrane, with near absence of internalization and direct membrane damage. (Middle) Head-to-head comparison between PET images (anterior maximum-intensity projection; SUVmax range, 0–10) of [68Ga]Ga-DOTATOC (SSTR agonist) and [68Ga]Ga-NODAGA-JR11 (SSTR antagonist) in patient with low-grade NET, showing more lesions (arrows, particularly in liver) for [68Ga]Ga-NODAGA-JR11 than for [68Ga]Ga-DOTATOC. (Right) Direct comparison of posttreatment SPECT images (anterior maximum-intensity projection; SUVmax range, 0–15) after [177Lu]Lu-DOTATOC (cycle 1) and [177Lu]Lu-DOTA-JR11 (cycle 2) performed within 10-wk interval. Tumor activity concentration at 24 h after injection is ∼30% higher with antagonist (arrows) than with agonist even though administered activity of 177Lu is ∼50% less for antagonist than for agonist (3.9 vs. 7.4 GBq). B = bottom; bw = body weight; T = top.
The NETTER-1 trial significantly improved progression-free survival with [177Lu]Lu-DOTATATE, with a hazard ratio of 0.18 (95% CI, 0.11–0.29; P < 0.0001) (1). However, 5 y after the last patient randomization, there was no statistically significant difference in median overall survival between the [177Lu]Lu-DOTATATE arm (48 mo; 95% CI, 37.4–55.2) and the control arm (36.3 mo; 95% CI, 25.9–51.7) despite a clinically significant improvement of the quality of life and progression-free survival in the [177Lu]Lu-DOTATATE arm (1). Concerning treatment safety, only 3 of 111 patients (3%) of the [177Lu]Lu-DOTATATE arm showed treatment-related severe adverse events during long-term follow-up, and 2 patients (2%) developed myelodysplastic syndrome, one of whom died 33 mo after randomization. No new cases of myelodysplastic syndrome or acute myeloid leukemia were reported during long-term follow-up. At present, the NETTER-2 trial is ongoing to determine whether [177Lu]Lu-DOTATATE prolongs progression-free survival in grade 2 or 3 gastroenteropancreatic NETs as first-line treatment in combination with long-acting octreotide (NCT03972488). A recent metaanalysis including more than 1,200 patients treated by [177Lu]Lu-DOTATATE (1–8 cycles, 3.7–10 GBq/cycle) revealed a disease control rate (proportion of complete response, partial response, minor response, and stable disease) of 74.1% (95% CI, 67.8%–80%) and a disease response rate (proportion of complete response, partial response, and minor response) of 29.1% (95% CI, 20.2%–38.9%) (2). This evidence contributed to the inclusion of [177Lu]Lu-DOTATATE in the therapeutic algorithms proposed by leading international societies as an effective and safe treatment option for NETs. Recently, a novel SSTR-agonist radioligand, [64Cu]64Cu-SARTATE, was compared with [68Ga]Ga-DOTATATE, showing higher uptake and retention resulting in high-contrast diagnostic images upward of 24 h (3). [67Cu]Cu-SARTATE, the therapeutic counterpart of [64Cu]Cu-SARTATE, is currently being evaluated (NCT04023331).
Over the years, novel data have emerged for SSTR antagonists. The application of SSTR antagonists was initially discouraged because of lack of internalization. Despite these initial considerations, it was later found that a higher percentage of SSTR antagonists than of agonists was bound in animal and human models. This can be attributed mainly to the functional interaction of SSTR antagonists with a larger variety of SSTR conformations, allowing binding of both activated and inactivated SSTRs (Fig. 1) (4,5). Slow dissociation of antagonist receptor binding and minimal internalization are also thought to play a role in tumor detection. Further, SSTR antagonists are more chemically stable and hydrophobic than SSTR agonists, with a consequent longer duration of action and stabilization in a lipid-rich environment (4).
From a theranostic point of view, the high target-to-background ratio and prolonged in vivo tumor binding obtained with radiolabeled SSTR antagonist have been of paramount importance in promoting the use of SSTR antagonists over SSTR agonists. Compared with [68Ga]Ga-DOTATATE in NETs, both [68Ga]Ga-NODAGA-LM3 and [68Ga]Ga-DOTA-LM3 demonstrated a significantly higher detection of liver metastases (202 vs. 235, P = 0.01, and 196 vs. 261, P = 0.02, respectively) and overall lesions (339 vs. 395, P = 0.002, and 372 vs. 447, P = 0.02, respectively), with a higher tumor-to-liver ratio of matched lesions in both arms (P = 0.00). There was no significant difference in detection of primary tumors (17 vs. 19, P = 0.16, and 13 vs. 15, P = 0.16, respectively), lymph node metastases (24 vs. 27, P = 0.18, and 29 vs. 32, P = 0.18, respectively), bone metastases (31 vs. 46, P = 0.11, and 126 vs. 126, P = 1.00, respectively), or other lesions (65 vs. 68, P = 0.32, and 8 vs. 13, P = 0.10, respectively) (6). In another comparative study, [68Ga]Ga-DOTA-JR11 detected more liver (552 vs. 365, P = 0.001) but fewer bone (158 vs. 388, P = 0.02) metastases than 68Ga-DOTATATE, but with comparable primary tumor detection (20 vs. 24, P = 0.50) and overall detection rate (835 vs. 875, P = 0.15) and with equal lymph node (43 vs. 43), pleural (51 vs. 51), and peritoneal (2 vs. 2) metastases (7). Similarly, in 12 gastroenteropancreatic NET patients, [68Ga]Ga-NODAGA-JR11 demonstrated a significantly higher overall sensitivity (94% with 50 μg and 88% with 15 μg of [68Ga]Ga-NODAGA-JR11) compared with [68Ga]Ga-DOTATOC (15 μg, 59.2%, P < 0.001, for both doses of [68Ga]Ga-NODAGA-JR11) (8).
Radioligand SSTR antagonists have been documented to bind a higher percentage of SSTRs than do agonists (Fig. 1), increasing targeting even for tumors with low SSTR expression (4,5). This would be clinically important in high-grade NETs, poorly differentiated neuroendocrine carcinoma, and certain non-NETs (breast carcinomas, renal cell carcinomas, and non-Hodgkin lymphomas) (9). For these reasons, there has been increasing interest in SSTR antagonists. In humans, 2 theranostic pairs of JR11 (i.e., [68Ga]Ga-DOTA-JR11/[177Lu]Lu-DOTA-JR11 and [68Ga]Ga-NODAGA-JR11/[177Lu]Lu-DOTA-JR11) have already been investigated (10,11). However, the safety profile of SSTR antagonists for PRRT requires further consideration and optimization. Severe hematotoxicity was observed compared with SSTR agonists at doses equivalent to or greater than that to red marrow. In a recent phase I clinical trial (12), 4 of 4 patients who received 2 cycles of [177Lu]Lu-satoreotide-tetraxetan (also known as [177Lu]Lu-DOTA-JR11) and an estimated bone marrow dose of at least 1.44 Gy developed grade 4 thrombocytopenia (and grade 3/4 neutropenia) and 57% developed grade 4 myelosuppression, but none of the patients with a bone marrow dose of 1.08 Gy or less experienced grade 4 thrombocytopenia or neutropenia. Therefore, the therapeutic protocol was revised to lower the bone marrow dose from 1.5 to 1 Gy and, subsequently, halve the dose in cycle 2. However, the hypothesis that the activity concentration in red marrow is comparable to that in blood (11) could probably be reconsidered, as SSTR antagonists may have specific binding in red marrow, also supporting a dedicated dosimetry based on posttherapeutic SPECT/CT imaging.
[68Ga]Ga-DOTA/NODAGA-LM3 and [177Lu]Lu-DOTA-LM3 represent another attractive SSTR-antagonist–based theranostic pair with high tumor binding and preliminary favorable dosimetry (13). Furthermore, radiolabeling of SSTR antagonists with α-emitters would provide a joint benefit from the biologic characteristics of the antagonists and the physical properties of the α-emitters, with potential therapeutic advantages even in patients refractory to treatment with β-emitter–labeled somatostatin analogs.
In conclusion, published literature strongly suggests that SSTR antagonists are characterized by no cellular internalization but a strong binding capacity to SSTR receptors, suggesting a higher efficacy than SSTR agonists that undergo cellular internalization and have weaker SSTR binding. These unique characteristics of SSTR antagonists are now shifting clinical focus toward the use of radiolabeled SSTR antagonists to improve the diagnostic sensitivity (with some concerns at the bone level (7)) and therapeutic efficacy of SSTR-based PRRT. Although SSTR antagonists have been optimized at the diagnostic level, therapeutic applications must be further investigated. Decreasing administered activities, encouraging dosimetry, and increasing duration between PRRT cycles to limit hematotoxicity while preserving therapeutic efficacy should be further researched. Patients with multiple liver metastases and those with poorly differentiated NETs could be suitable candidates for promising new clinical investigations. Thus, SSTR antagonists currently represent a novel paradigm in theranostics that will undoubtedly revolutionize diagnostic and therapeutic management of NETs. We hope these discoveries will ultimately improve the clinical outcomes of patients with these rare tumors.
DISCLOSURE
This work was supported by the Intramural Research Program of the National Institutes of Health, Eunice Kennedy Shriver National Institute of Child Health and Human Development. No other potential conflict of interest relevant to this article was reported.
Footnotes
Published online Feb. 9, 2023.
- © 2023 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication January 4, 2023.
- Revision received February 2, 2023.
In this issue





{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.