


Abstract
Eliminating microscopic residual disease with α-particle radiation is theoretically appealing. After extensive preclinical work with α-particle–emitting 211At, we performed a phase I trial with intraperitoneal α-particle therapy in epithelial ovarian cancer using 211At conjugated to MX35, the antigen-binding fragments—F(ab′)2—of a mouse monoclonal antibody. We now present clinical outcome data and toxicity in a long-term follow-up with individual absorbed dose estimations. Methods: Twelve patients with relapsed epithelial ovarian cancer, achieving a second complete or nearly complete response with chemotherapy, received intraperitoneal treatment with escalating (20–215 MBq/L) activity concentrations of 211At-MX35 F(ab′)2. Results: The activity concentration was escalated to 215 MBq/L without any dose-limiting toxicities. Most toxicities were low-grade and likely related to the treatment procedure, not clearly linked to the α-particle irradiation, with no observed hematologic toxicity. One grade 3 fatigue and 1 grade 4 intestinal perforation during catheter implantation were observed. Four patients had a survival of more than 6 y, one of whom did not relapse. At progression, chemotherapy was given without signs of reduced tolerability. Overall median survival was 35 mo, with a 1-, 2-, 5-, and 10-y survival of 100%, 83%, 50%, and 25%, respectively. Calculations of the absorbed doses showed that a lower specific activity is associated with a lower single-cell dose, whereas a high specific activity may result in a lower central dose in microtumors. Individual differences in absorbed dose to possible microtumors were due to variations in administered activity and the specific activity. Conclusion: No apparent signs of radiation-induced toxicity or decreased tolerance to relapse therapy were observed. The dosimetric calculations show that further optimization is advisable to increase the efficacy and reduce possible long-term toxicity.
Epithelial ovarian cancer has the highest mortality rate of all gynecologic cancers and is associated with a high relapse rate (>50%) after standard therapy (1), generally located in the peritoneal cavity, and better local treatments are sought. Intraperitoneal radioimmunotherapy using β-emitting nuclides showed promising results in early trials, but randomized phase III trials with 90Y conjugated to the murine antihuman milk fat globules (HMFG1) antibody as a boost therapy failed to improve overall survival in patients with a negative second-look (2,3). Post hoc subgroup analysis indicated that an effect may be found for patients who had residual disease after primary surgery (4).
Biokinetic modeling demonstrates that α-particle therapy is needed if very small tumor clusters or single cells are to be treated effectively (5). This is based on the favorable characteristics of the α-particle, that is, a short range in tissue (<100 μm) and a high linear energy transfer that results in highly cytotoxic and localized irradiation. For α-radioimmunotherapy, the preferred clinical situation would be diseases with a small tumor volume, such as minimal residual disease in hematologic malignancies or subclinical micrometastatic disease (6).
In 2004, we initiated a dose escalation pharmacokinetic phase I study with 211At conjugated to MX35 F(ab′)2, the antigen-binding fragments of a mouse monoclonal antibody. The initial report on the pharmacodynamics demonstrated that therapeutic activities could be produced and infused (7), and we found low absorbed doses in normal organs and we found a risk that was not negligible (8). Recently, another intraperitoneal α-radioimmunotherapy study was performed by Meredith et al. using 212Pb conjugated to trastuzumab (anti–HER2-neu protein) in 18 patients with advanced HER-2–positive peritoneal growth. They concluded very low toxicity and achieved possible therapeutic doses without reaching a maximal tolerated dose (9). Here, we present mature patient data from the first 12 patients receiving intraperitoneal α-radioimmunotherapy, including toxicity and clinical long-term outcome data as well as individual absorbed dose estimates of single cells and potential microtumors.
MATERIALS AND METHODS
Study Design
A single-center study was conducted at the Department of Oncology at Sahlgrenska University Hospital, Gothenburg, Sweden. It followed good clinical practice and adhered to the Helsinki Declaration and was approved by the Regional Ethical Committee and the Swedish Medical Product Agency; accordingly, all subjects gave written informed consent. The study was designed as a 3 + 3 dose-finding study, and each dose cohort would be expanded to 6 patients if only 1 dose-limiting toxicity was recorded. If 2 dose-limiting toxicities were recorded, dose escalation would be stopped. Dose-limiting toxicity was defined as any grade 3 or 4 toxicity that could be related to the infused radioconjugate/radiation dose. Maximal tolerated dose was defined as the dose with no more than 1 dose-limiting toxicity per 6 patients and here refers to the prespecified levels of total activity (50, 100, 200, and 300 MBq) corresponding to the activity concentrations of 25, 50, 100, and 200 MBq/L given intraperitoneally to the patients in 1–2 L of 7.5% icodextrin. The starting level of administered activity was chosen to be sufficient to allow γ-scintigraphy imaging while remaining below expected tolerance limits. These calculations were extrapolated from our preclinical data (10). After 5 patients were treated, the imaging-based dosimetry indicated relatively high thyroid doses, and blocking with potassium perchlorate 200 mg twice daily was added to the protocol starting the day before treatment until 2 d after treatment. A second amendment was added after 9 patients, related to an improved labeling method to obtain the target activities (11).
Patient Inclusion and Safety Follow-up
Patients with microscopically proven epithelial ovarian cancer and who experienced a relapse and were treated with salvage intravenous chemotherapy to complete or near-complete remission were eligible. Exclusion criteria were reduced general condition (Karnofsky performance status < 80%), severe cardiovascular comorbidity, elevated liver biochemistry test, creatinine more than 3 times the upper limit of normal, and abnormal hematology. Toxicity was evaluated and recorded weekly at outpatient visits for the first 8 wk and thereafter assessed every 3 mo. When patients relapsed, they were treated and followed according to regional guidelines. The definition of disease progression included any of the following: a rise in CA125 level to more than 1.5 times the upper limit of normal (35 IU/mL), measurable disease on CT scan, or confirmed disease-related symptoms. Patients with no evidence of disease were regularly followed with laboratory testing of kidney and thyroid functions and hematology.
211At and Conjugation to the Vector
The MX35 F(ab′)2 was labeled with isolated 211At as previously described (7,11). The radiochemical purity was more than 99% as determined by methanol precipitation, and the immunoreactivity was approximately 85% according to the method described by Lindmo et al. (12).
Monoclonal Antibody
The vector was the MX35 F(ab′)2 fragment, which targets the NaPi2b (SLC34A2) cell surface glycoprotein expressed on more than 90% of human epithelial ovarian cancers (13). This murine IgG1-class mAb was developed and characterized at the Memorial Sloan Kettering Cancer Center (14) and made available to us at clinical grade.
Dosimetry
Calculations of the effective dose and absorbed dose in single cells and various potential microtumors were based on previous reports; the kinetics involved intraperitoneally infused 211At- F(ab′)2 fragments in humans (5), penetration of F(ab′)2 fragments into tissues (15), and effective dose estimation (8). Since these patients did not present with tumors detectable with imaging, individually determined activity concentration of the infused solution combined with repeat blood and intraperitoneal fluid sampling were used as model input for tumor dosimetry. The model comes with various assumptions—such as cell size, cell and microtumor shape, and antigen concentration—and deviations from these assumptions will naturally affect the results.
Statistical Analysis
Data are presented descriptively, but time to progression and survival calculations were performed with the Kaplan–Meier method using IBM SPSS Statistics, version 22, software.
RESULTS
Patient Characteristics and Treatment Compliance
Between February 2005 and February 2011, 17 patients were screened for inclusion and subjected to laparoscopy (Table 1). Three patients did not receive an intraabdominal catheter because of adherences (2 patients) or carcinomatosis. Of the 14 patients with an intraabdominal catheter, 1 was excluded because of poor distribution on 99mTc-macroaggregated albumin abdominal scintigraphy, and 1 patient experienced intestinal perforation. The remaining 12 patients (3 in each activity group) received treatment with 211At-MX35 F(ab′)2, and the activity concentration was escalated from 20 to 215 MBq/L without any dose-limiting toxicities.
Patient Characteristics
The median age was 52 y (range, 36–75 y); 10 patients had stage III disease at initial diagnosis, and a majority (7 of the 12 treated) had high-grade serous ovarian cancer. All patients were at a good performance status, with a Karnofsky score of 100. Four of the treated patients had signs of residual disease, 3 with elevated CA125 (54–70 kU/L) and 1 with biopsy-proven millimeter-sized tumor tissue found during the catheter procedure.
Toxicity
The frequency of toxicity according to the Common Toxicity Criteria, version 2.0, was low overall (Table 2). In all, there were 84 adverse events recorded during the first 8 wk in the intention-to-treat population of 17 patients (out of which 14 patients had the catheter implanted). Most patients expressed grade 1 or 2 events related to the catheter procedure, such as abdominal discomfort, swelling, and leakage. These problems generally resolved within 1 to 2 d (Fig. 1). Four patients experienced grade 1–2 fatigue between 1 and 3 d, and 1 patient experienced grade 3 fatigue (in the 200 MBq/L group) on days −1 to 3, which then declined to grade 1 and persisted for 2 wk. Six patients reported grade 1–2 nausea between 1 and 3 d, among whom 3 patients felt the discomfort before the 211At treatment, that is, after catheter implantation. One patient experienced prolonged nausea and fatigue up to 8 wk but was diagnosed with progressive disease. There was 1 grade 4 event involving a perforation of the small intestine after catheter insertion. This patient developed an abdominal infection that was treated with intravenous antibiotics and did not receive any 211At treatment.
Toxicity According to Common Toxicity Criteria, Version 2.0
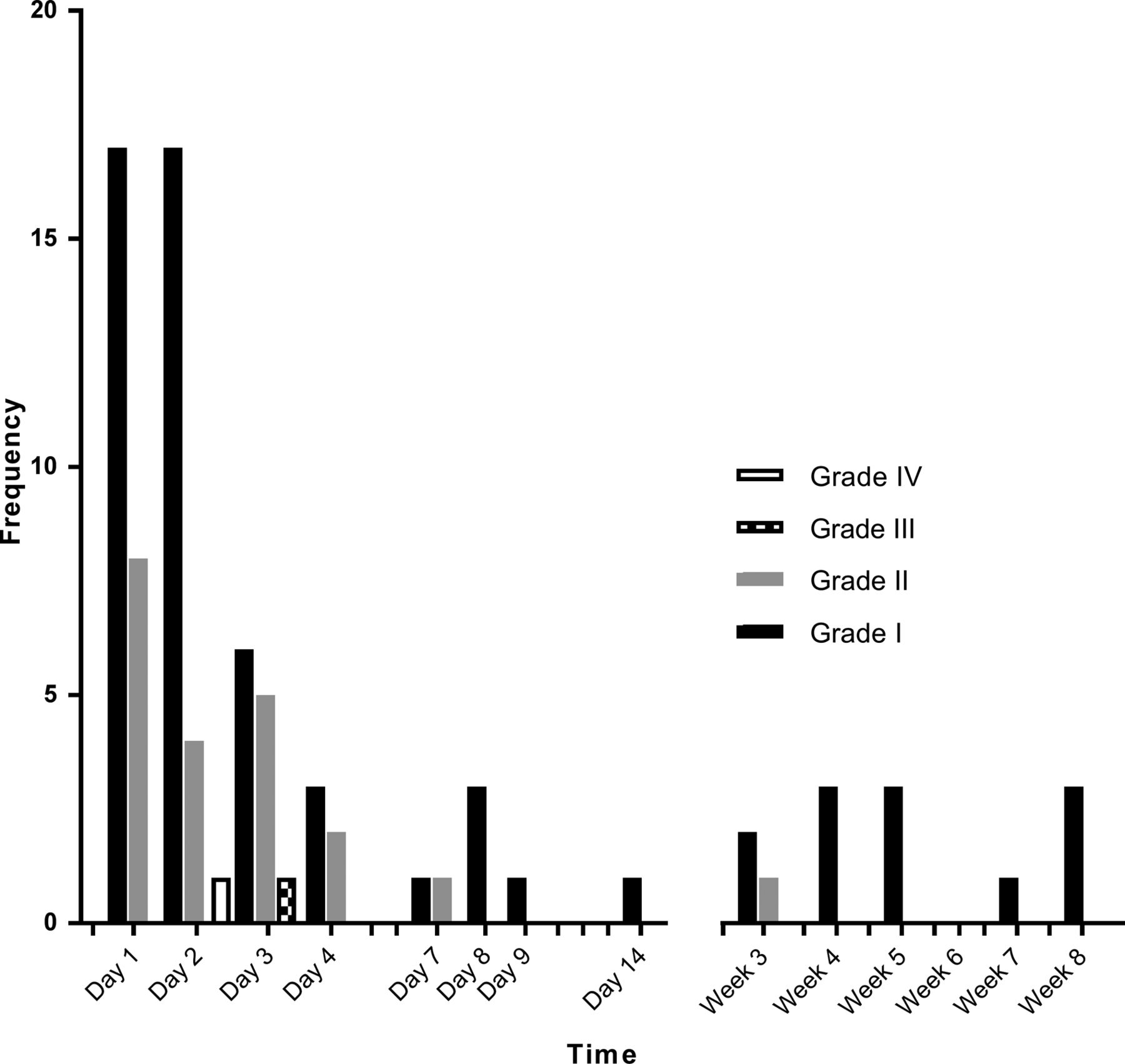
Histogram depicting on which day adverse events resolved as grouped by grade. Majority (85%) of adverse events resolved within 2 wk. Six adverse events that resolved between weeks 3 and 7 were skin-related, for example, port infection.
There were no signs of late toxicity or indication of hypothyroidism, renal failure, or bone marrow depletion. In addition, the patients were heavily treated with cytotoxic therapy after 211At treatment. Eleven patients received between 2 and 10 lines of chemotherapy, at the discretion of the physician, after α-radioimmunotherapy during periods of 6.5 mo up to 46 mo (Table 3), with no signs of impaired tolerability or enhanced bone marrow toxicity.
Clinical Outcomes After Intraperitoneal Treatment with 211At-MX35 F(ab′)2
One patient had radical surgery for a pT4N0 ileocecal mucinous adenocarcinoma 2.7 y after treatment. Histology analysis and immunostaining showed that the tumor was of intestinal origin and arose in the area where the patient had received radiotherapy for a suspected local recurrence before the 211At treatment. This patient has since been diagnosed with Lynch syndrome, and because of additional colorectal premalignant and malignant transformations, a colectomy was performed.
Efficacy
The median follow-up time was 42.5 mo for all patients and 147 mo for patients who were still alive. The median time to progression was 5 mo (range, 3.0–147+ mo) for the 12 patients treated and 9.6 mo for the 8 patients who showed no signs of disease at baseline (Table 3). Progression was based on a rising CA125 (>1.5 times the upper limit of normal) without a confirmatory CT scan but was verified in 3 cases with a CT scan or biopsy. The median overall survival was 35 mo, with 1, 2, 3-, 5-. and 10-y survival rates of 100%, 83%, 50%, 33%, and 25%, respectively. Three patients were still alive, and the remaining 9 patients all died from progressive disease.
Four patients had a longer response after chemotherapy followed by intraperitoneal 211At than in response to earlier lines of treatment (Table 3). Patients with evidence of residual disease at baseline (3 with elevated CA125 and 1 with a biopsy-proven millimeter-sized peritoneal recurrence) had a shorter response after 211At treatment but a longer remission period when administered intravenous chemotherapy after relapse. At the last follow-up, 1 patient still showed no recurrence more than 12 y after α-radioimmunotherapy. This patient had received 60 Gy in 30 fractions with external radiotherapy because of a small recurrence within the pelvis minor before 211At treatment.
Dosimetry
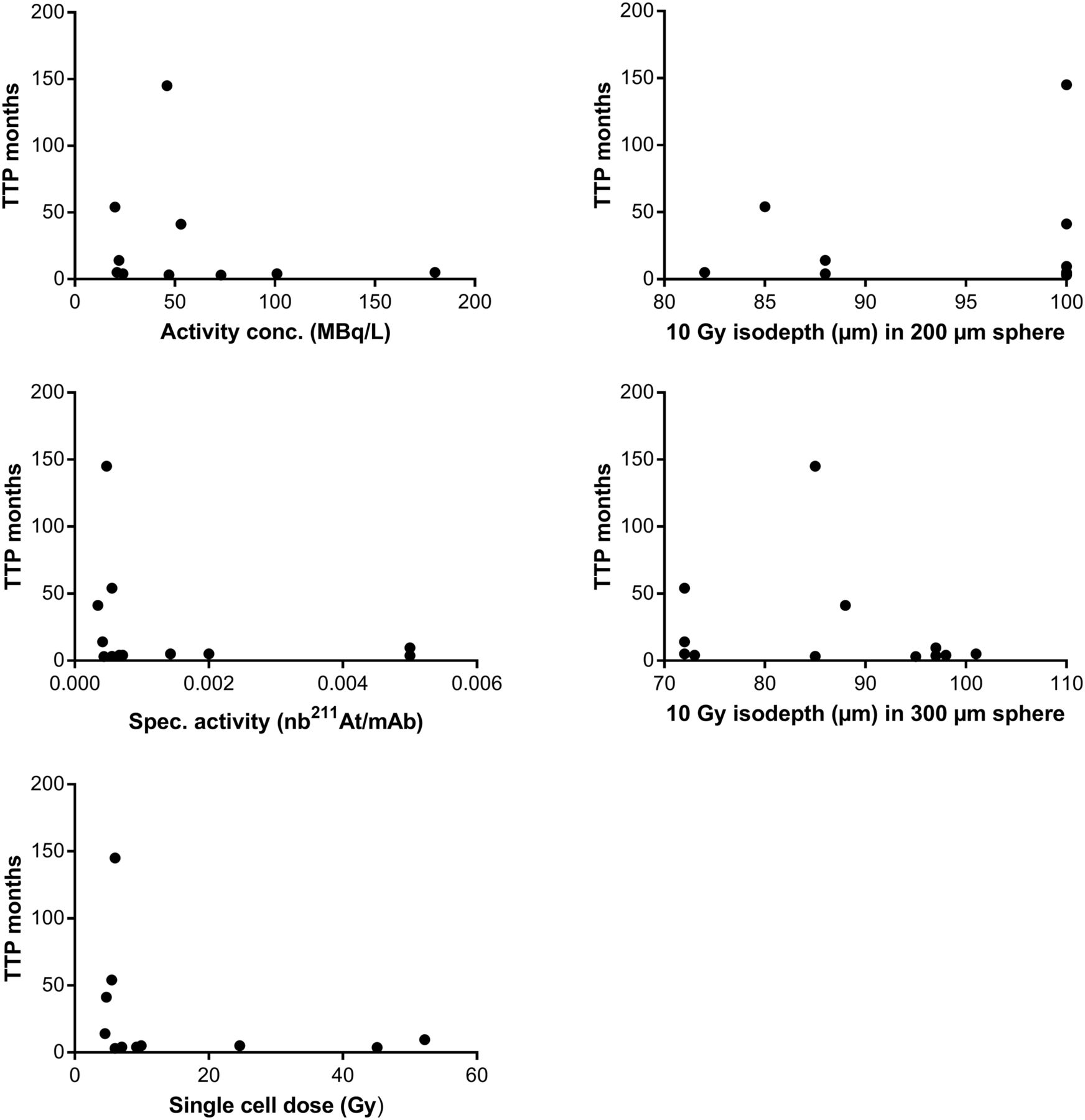
The calculation of absorbed dose to single cells and microtumors was based on the initial activity concentration of the infused solution using the models described previously (5,15). The dosimetry results are shown in Table 4. Spheres 200 and 300 μm in diameter were chosen to illustrate possible undetected avascular tumor aggregates that remained after successful chemotherapy. The first 9 patients who received treatment with a lower specific activity (between 1/700 and 1/2,900 211At/mAb) had a lower estimated dose to single cells than the last 3 patients, with higher specific activity. However, previously described modeling (5,15) predicts that a higher specific activity will result in a reduced penetration of 211At-mAbs into the tumor tissue and a lower central dose in microtumors. For several patients, high absorbed doses (approximately 10 Gy) were calculated for microtumors with diameters of up to approximately 200 μm. There were no correlations between time to progression and the estimated doses to single cells, 200- or 300-μm spheres, or activity concentration or specific activity (Fig. 2)
Calculated Individual Doses Using Specific Activity, Volume Administered, and Assumption of 7 × 105 Antigen/Cell

Correlations between time to progression (TTP, mo) and activity concentration (MBq/L), specific activity (211At/mAb), single-cell dose (Gy), and 10-Gy isodepths (μm) to 200- and 300-μm spheres showing no significant associations. nb = number.
DISCUSSION
More intense locoregional treatment of epithelial ovarian carcinoma can increase the cure rate, as argued by the effects of more aggressive debulking surgery (16) and intraperitoneal chemotherapy (17). α-particles have a high linear energy transfer and a short (<100 μm) range, making them highly cytotoxic as well as less dependent on oxygenation and cell cycle phases. However, their short range makes them likely most effective against small-scale disease. The intended clinical goal would be to treat epithelial ovarian cancer patients upfront directly after surgery using standard chemotherapy when the abdominal cavity harbors very small deposits of tumor cells. To mimic this setting, the patients included in this study had experienced disease relapse but achieved a complete or near-complete response after the second- or third-line chemotherapy.
During the initial weekly follow-up after α-radioimmunotherapy, we found no significant toxicity in the laboratory parameters—for example, a complete absence of measurable effect on leukocytes and thrombocytes. This agrees with the estimated low absorbed dose (<50 mGy) to the bone marrow (7,8). There were no signs of renal or hematologic toxicity during the subsequent lifelong follow-up, and we did not find any clinically distinct effects on the tolerability to chemotherapy on disease progression (Table 3); however, the post-211At treatments are individually managed with a range of lines and treatment periods. The first 5 patients were deliberately not blocked with potassium perchlorate, which allowed the detection of free 211At uptake in the thyroid. Thus, the subsequent patients were blocked with a significant reduction in uptake (7), but no signs of thyroid dysfunction were observed or measured in any patient at any time. Most toxicities can probably be linked to the procedure of intraperitoneal administration, that is, catheter insertion, use of opiates, and abdominal swelling by the fluid; however, a contribution of 211At treatment to low-grade fatigue and nausea cannot be ruled out (Fig. 1; Table 2). The one major complication (grade 4) was due to a small-intestine perforation after implantation of the intraperitoneal catheter, which is a known risk when performing second-look laparoscopy.
Therapeutic effect was not an endpoint in this phase I trial. Nonetheless, the outcome compares favorably with known reports of similar patients undergoing metastatic treatment with a negative second-look laparoscopy (18). Four patients had evidence of remaining active disease: 3 with slightly elevated CA125 and 1 with a suggestive finding at laparoscopy that proved to be malignant. These 4 patients showed disease progression within 4 mo after therapy. On the other end, 3 patients were still alive at this long-term follow-up assessment, 1 of whom had no evidence of disease. Compared with known predictors for long-term outcomes after intraperitoneal RIT, this outcome was not foreseen (19,20). In the current study, 4 of 12 patients treated had a longer response time after α-radioimmunotherapy than after their previous regimen. No conclusion may be drawn from this exploratory finding, but it is interesting to note that with chemotherapy, a longer response on the subsequent line than on the first-line therapy has been reported in only 3% (21) and 9% (22) of patients.
The specific activity was generally low but varied for the 2 labeling methods used (Table 1). For the last 3 patients, a new radiolabeling method that allowed a higher specific activity was used, as was believed necessary to deliver eradicative (i.e., >10 Gy) absorbed doses to single cells. However, more recently described (5,15) modeling predicts that a higher specific activity impairs the penetration of 211At mAbs into microtumors and therefore insufficiently irradiates the inner cells (Table 4). These calculated absorbed doses were estimated for microtumors with diameters of up to approximately 300 μm (Table 4). The microtumors and any radiopharmaceutical uptake on them could not be detected. The absorbed doses are instead based on various assumptions that may not entirely reflect the full biologic reality for each patient. Even if the doses are based on the individual’s activity concentration of the infused solution, the findings from the model results must be used with caution. Any deviation from the model assumptions, for example, in antigen expression, will affect the results. Although recognizing that all assumptions that are included in the models (5,15) may not be fulfilled in the individual patient, some general conclusions can be made. For example, an antibody with lower affinity or a smaller mAb fragment could improve the diffusion into microtumors and also facilitate irradiation of the inner cells of tumor deposits larger than 200 μm in diameter, but in contrast, irradiation of possible single cells might not be sufficient. The dose calculations indicate a need to further enhance the targeting vector, and a specific activity optimized to irradiate both single cells and microtumors should be sought. Alternatively, administration of a compound with high specific activity to eradicate single cells can be followed by a posttherapy cold antibody boost (15) to increase penetration.
Formally, there is room for further dose escalation, as the maximal tolerated dose was not reached. We used activity concentrations of up to 215 MBq/L without detecting any dose-limiting toxicities. A concentration of 215 MBq/L has previously been reported to be well tolerated (7,8), and this dose was confirmed in this long-term follow-up study. However, because this treatment strategy, involving radiation with a risk for secondary malignancies, aims toward the adjuvant setting, we do not think it is reasonable to escalate the dose until toxicity as with most other pharmaceuticals. It is prudent to include theoretic modeling of both long-term risks and dose levels that are needed to attain eradicative doses. In light of previous data on the risk of secondary malignancies (10) and theoretically calculated efficacy, we, for the time being, consider 200 MBq/L a reasonable activity concentration to use in further studies. Thus, we argue that the activity concentration should be carefully considered by weighing the effective dose (8) against the specific activity for a single-cell dose (5) and the penetrating ability of the vector to achieve toxic doses to both single cells and aggregates larger than 200 μm in diameter.
CONCLUSION
There were no apparent signs of radiation-induced toxicity in patients who were followed for up to 12 y, and there was no decreased tolerance to relapse therapy. The dosimetric calculations show that further optimization of the targeting vector is advisable with regard to specific activity, because escalation of the total activity and activity concentration seem doubtful, considering the effective dose.
DISCLOSURE
This work was supported by the Swedish Research Council, the Swedish Cancer Society, the King Gustav V Jubilee Clinic Research Foundation, and grants from the Swedish state under the agreement between the Swedish government and the county councils, the ALF agreement ALFGBG-435001. No other potential conflict of interest relevant to this article was reported.
Footnotes
Published online Jan. 25, 2019.
- © 2019 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication October 3, 2018.
- Accepted for publication January 3, 2019.





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Estimating the Risk for Secondary Cancer After Targeted {alpha}-Therapy with 211At Intraperitoneal Radioimmunotherapy
- Dosimetry in Radiopharmaceutical Therapy
- Biodistribution and Radiation Dosimetry of Intraperitoneally Administered 124I-Omburtamab in Patients with Desmoplastic Small Round Cell Tumors