


Abstract
Lung scintigraphy is primarily used to diagnose pulmonary embolism. Ventilation imaging is often performed using 99mTc-DTPA or Technegas, an ultrafine dispersion of 99mTc-labeled carbon. Despite the common use of these radioaerosols, they have not been compared in an intraindividual study, and not with ventilation–perfusion (V/P) SPECT. The aim of the present head-to-head study was to systematically investigate differences in ventilation studies performed with 99mTc-diethylenetriaminepentaacetate (DTPA) and Technegas. Methods: Sixty-three patients, 28 without and 35 with obstructive lung disease, were examined with V/P SPECT using both 99mTc-DTPA and Technegas. V/P SPECT images were randomized and assessed independently by 2 masked physicians according to a predefined scoring system. A paired comparison was performed using the Wilcoxon signed-rank test. Results: In both obstructive and nonobstructive disease, the overall unevenness of radiotracer deposition and the degree of central deposition were more pronounced in 99mTc-DTPA than Technegas studies. Because of better peripheral penetration, the extent of reverse mismatch was less when Technegas was used. Additionally, in obstructive disease, the degree of focal deposition in distal airways was more pronounced with 99mTc-DTPA. Mismatched perfusion defects were more frequently found with Technegas in obstructive disease. Conclusion: This intraindividual comparative study shows that Technegas is the preferred radioaerosol, particularly in obstructive disease.
- pulmonary embolism
- ventilation–perfusion single-photon emission computed tomography (V/P SPECT)
- COPD
- 99mTc-DTPA
- Technegas
Lung scintigraphy allows imaging of ventilation and perfusion distribution and assessment of regional lung function in lung disease (1). Lung scintigraphy is used primarily to identify pulmonary embolism (PE), although other diseases such as pneumonia, heart failure, and obstructive lung disease may be identified (1–5). Ventilation–perfusion (V/P) SPECT improves the diagnostic accuracy for PE (6–9). V/P SPECT performed according to the state of the art also simplifies recognition of ventilation and perfusion patterns typical of other cardiopulmonary diseases (10).
Perfusion scintigraphy is most commonly achieved by microembolization with 99mTc-labeled macroaggregates of human albumin (MAA). For ventilation studies, the inert gas 81mKr and the aerosols 99mTc-diethylenetriaminepentaacetate (DTPA) and an ultrafine dispersion of 99mTc-labeled carbon (Technegas; Cyclomedica Ltd.) are currently recommended (11). 81mKr is of limited use because of its high cost and short half-life.
Previously, 133Xe was also used for ventilation studies, but this is no longer recommended according to the guidelines of the European Association of Nuclear Medicine (11).
How aerosol droplets or particles are distributed and deposited within airways and alveoli depends on their aerodynamic properties, particularly their mass median aerodynamic diameter (11). Even with the best liquid aerosol generators used with 99mTc-DTPA, the droplets have a size distribution of between 0.5 and 2 μm whereas Technegas particles are all of submicron size. Nevertheless, some studies indicate that Technegas and 99mTc-DTPA give clinical information comparable to that of 81mKr scintigraphy (12–16). However, clinical experience indicates that impaction of aerosol particles leads to hot-spot formation, particularly in patients with chronic obstructive pulmonary disease (COPD) and when aerosol particles are relatively large, as when 99mTc-DTPA is used. Technegas is therefore considered to be optimal for ventilation scintigraphy (11,17–20). However, few studies have systematically compared 99mTc-DTPA with Technegas ventilation studies (21,22). Apparently, no head-to-head comparison in humans between 99mTc-DTPA with Technegas has been published, and none has been published using V/P SPECT.
The aim of the present head-to-head study was to systematically investigate differences in ventilation studies performed with 99mTc-DTPA and Technegas in patients routinely referred for V/P SPECT mainly for diagnosis of PE and in a second group of patients with known COPD. Our hypothesis was that Technegas, because of its smaller particle size and hydrophobic properties, would have a more even distribution and better penetration within the lung parenchyma.
MATERIALS AND METHODS
Study Population
Sixty-five patients were included in this study, which was approved by the regional ethical review board.
Thirty-five of the patients were referred for a V/P SPECT examination to evaluate clinically suspected PE (n = 29), to evaluate alveolitis (n = 3), or to evaluate lung function before surgery or after transplantation (n = 3). Their mean age (±SD) was 57 ± 17 y, 51% were women, and 5 had known obstructive lung disease. Two of these 35 patients were later excluded because data had not been properly stored for reevaluation.
In addition, 30 outpatients with known COPD (age, 65 ± 6.7 y; 63% women) were consecutively recruited from the Department of Respiratory Medicine and Allergology. They had moderate to very severe COPD according to the classification of the Global Initiative of Obstructive Lung Disease (23). Their mean ratio of forced expiratory volume in 1 s and vital capacity was 0.44, within a range of 0.31–0.60. They were clinically stable and had been free from exacerbation for at least 6 wk.
The characteristics of the 63 evaluated patients are summarized in Table 1.
Patient Characteristics
Radioactive Tracer Preparation and Administration
99mTc-DTPA was prepared using a commercial kit (TechneScan DTPA; Mallinckrodt Medical BV). The 99mTc-DTPA aerosol was generated and inhaled using an UltraVent nebulizer (Mallinckrodt Medical BV) or a SmartVent aerosol generator system (Diagnostic Imaging Ltd.). The mass median aerodynamic diameter of the delivered particles from those nebulizers was 1.7 μm or less. Technegas was delivered from the Technegas generator according to the manufacturer's instructions. The size range of the Technegas primary particles and agglomerated particles is 0.005–0.2 μm (24). Inhalation in the supine position was terminated when a collimated Geiger-Müller tube monitor over the chest indicated that 30 MBq of 99mTc had been deposited in the lungs.
Perfusion SPECT was performed after intravenous injection of 100–120 MBq of 99mTc-MAA in the supine position (Technescan LyoMaa kit; Mallinckrodt Medical BV). The effective doses from V/P SPECT examinations according to this protocol are 1.5 mSv when 99mTc-DTPA plus 99mTc-MAA is used and 1.8 mSv when Technegas plus 99mTc-MAA is used (25).
V/P SPECT Acquisition
V/P SPECT was performed according to the recommended guidelines of the European Association of Nuclear Medicine (11) using the protocol of Palmer et al. (26) and Bajc et al. (7).
In short, a large-field-of-view dual-head γ-camera with a low-energy, all-purpose collimator was used. Acquisition was performed in a 64 × 64 matrix, zoomed to a pixel size of 6.8 mm with 128 projections over 360°. Sixty-four steps, each of 10-s duration, were used for the ventilation study, and 64 steps of 5-s duration were used for the perfusion study.
V/P SPECT was performed as a 1-d protocol. 99mTc-DTPA or Technegas was inhaled, and ventilation tomography followed. After that, with the patient in a carefully maintained supine position without movement, 99mTc-MAA was slowly injected intravenously. Then, perfusion tomography was performed.
Within 72 h, 60 (95%) of the 63 patients were reexamined for ventilation, using the ventilation radiopharmaceutical not used at the initial examination. The 3 remaining patients, all regarded as clinically stable (1 with COPD and 2 with alveolitis), were reexamined at 4, 6, and 7 d after the initial examination.
V/P images were reconstructed using ordered-subsets expectation maximization with 8 subsets and 2 iterations. After the ventilation background was subtracted from the perfusion tomograms, the 3 studies were adjusted for position and separately prepared for review, by an independent technologist. Attenuation correction was not used.
V/P SPECT Image Interpretation
All V/P SPECT images were independently reviewed by 2 experienced physicians. The physicians were unaware of clinical information and the type of radioaerosol that had been used. All ventilation studies were paired with the corresponding perfusion study. Accordingly, 126 sets of V/P SPECT images were reviewed in total. The order of the examinations was randomized. All sagittal, coronal, and transversal V/P SPECT images were available to the physicians.
Images were reviewed according to a predefined standardized scoring system to characterize the distribution of the ventilation radiopharmaceutical. To minimize systematic differences in the assessment, a training session was held with the 2 physicians before the study began. Ventilation images were assessed and graded using 3 qualitative parameters: unevenness of radioaerosol distribution; deposition of radioaerosol in major and intermediate conducting airways, that is, central deposition; and focal peripheral deposition in more distal airways. Each of these parameters was scored from 0 (none or normal) to 10 (very high). Thereafter, paired V/P SPECT datasets were assessed by the physicians. The extent of the mismatched (i.e., perfusion < ventilation), reverse mismatched (ventilation < perfusion), and matched (reduction in ventilation = reduction in perfusion) defects was expressed as a percentage of the total lung volume. The sum of these was used to estimate the degree of total lung function reduction.
Finally, all V/P SPECT images were reviewed according to criteria used in our clinical routine (7,10). PE was reported if there was a V/P mismatch with at least 1 segmental or 2 subsegmental defects (11). If PE was present, the extent of lung perfusion was scored as a percentage of total lung volume. Scintigraphic signs of airway obstruction were graded as 0 (none), 1 (mild, or affecting less than 20% of the total lung function), 2 (moderate, or affecting 20%−50% of the total lung function), or 3 (severe, or affecting more than 50% of the total lung function). The presence of ancillary findings such as heart failure was also described but not further analyzed in this study.
Statistics
All continuous data are expressed as mean ± SD. Paired comparison between 99mTc-DTPA and Technegas variables was performed using the Wilcoxon signed-rank test. The null hypothesis was rejected at P ≤ 0.05. The differences between 99mTc-DTPA and Technegas parameters are also illustrated in Bland–Altman diagrams, plotting differences against average. Statistics and graphing were performed using Prism 5.02 (GraphPad Software).
RESULTS
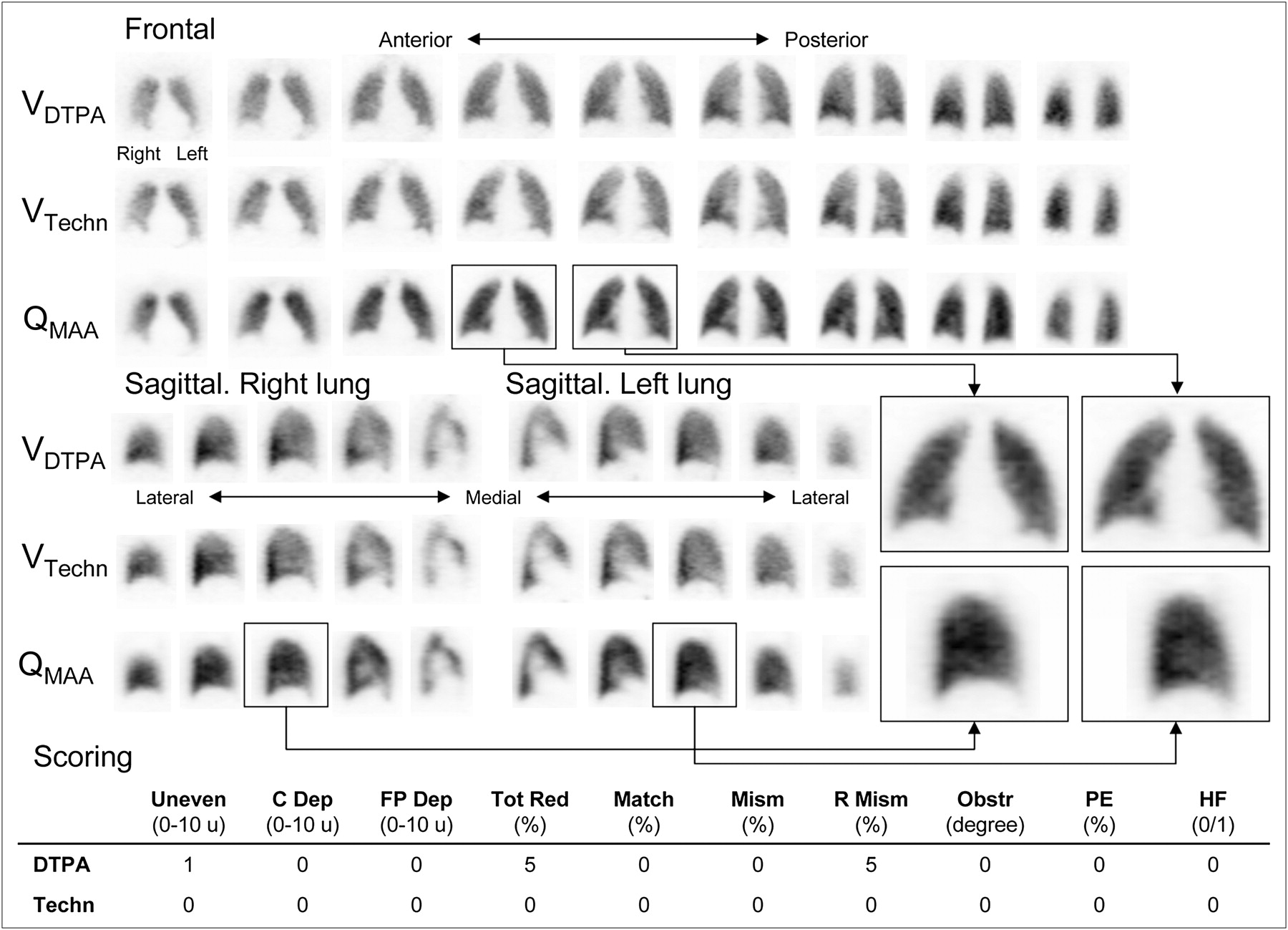
In patients with normal to near-normal ventilation patterns, even patients with PE, a close correlation was evident between 99mTc-DTPA and Technegas ventilation images (Fig. 1 and Supplemental Fig. 1A; supplemental materials are available online only at http://jnm.snmjournals.org).

In patients with normal to near-normal V/P SPECT patterns, good agreement is seen between DTPA and Technegas ventilation images. The 4 enlarged perfusion images to the right illustrate principle for construction of 2 × 2 panels used in the following images. Mean evaluation scores of 2 interpreters is shown below images. C dep = central deposition; FP dep = focal peripheral deposition; HF = heart failure; match = matched reduction/defects; mism = mismatched reduction/defects; obstr = obstruction; R mism = reverse mismatched reduction/defects; Techn = Technegas; tot red = total reduction in lung function; u = units; uneven = overall unevenness.
Both physicians identified increased alveolar epithelial leakage of 99mTc-DTPA in 3 patients. The leakage compromised the assessment of ventilation distribution (Supplemental Fig. 1B). In 2 of these patients, both physicians had difficulty with the interpretation because the quality of the 99mTc-DTPA images was poor. Interpretation difficulties were also experienced in 2 obstructive disease patients examined with 99mTc-DTPA.
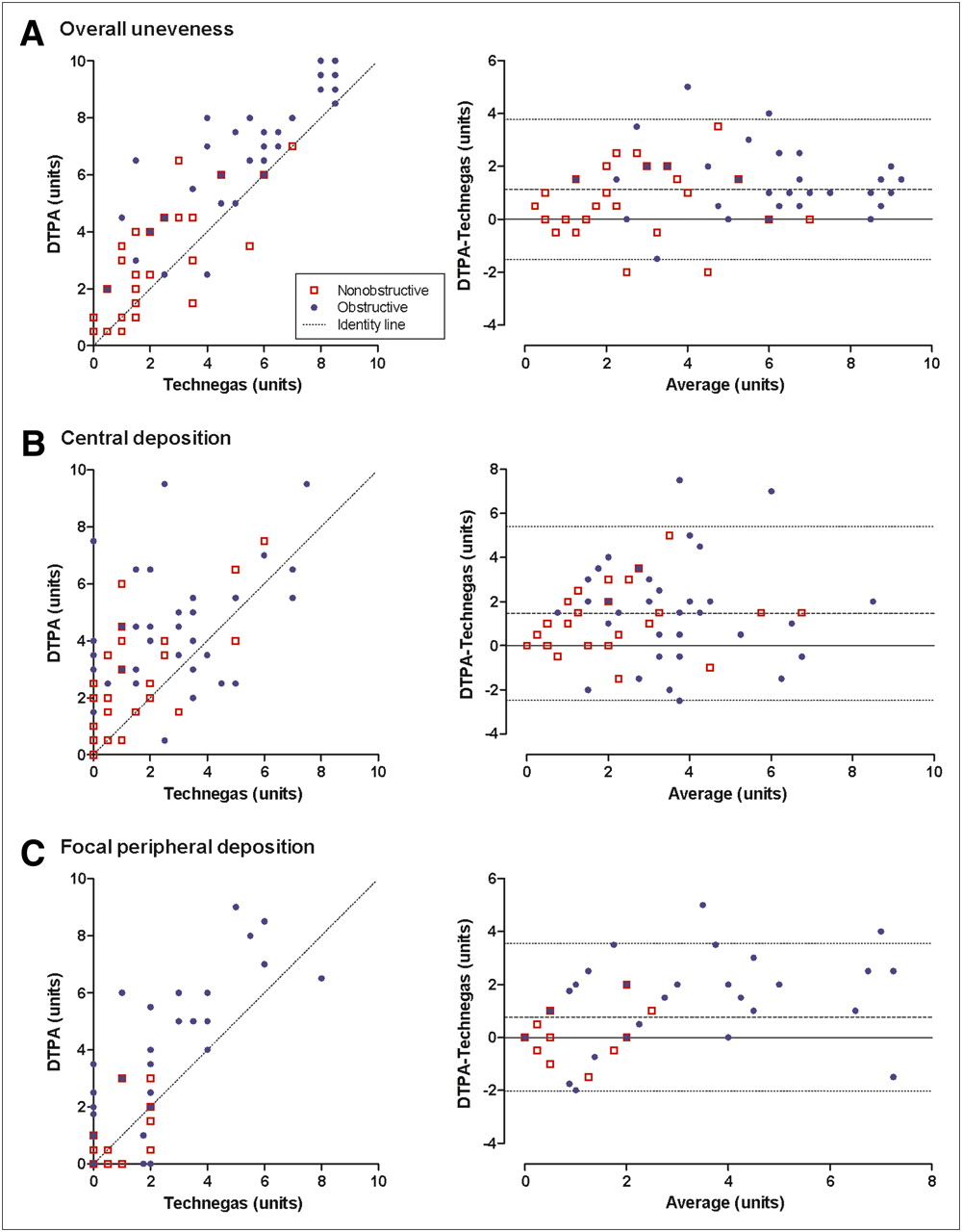
Overall unevenness of radiotracer deposition and degree of central deposition were more pronounced in 99mTc-DTPA than in Technegas studies (Figs. 2A, 2B, and 3). These differences were significant for both the nonobstructive and the obstructive groups (Table 2). The degree of focal peripheral deposition was more pronounced in 99mTc-DTPA studies and reflected the findings in the obstructive group (Fig. 2C; Table 2). The total reduction in lung function was estimated to be more severe with 99mTc-DTPA than with Technegas, particularly in the obstructive group (Supplemental Fig. 2A; Table 2). Matched defects were much more extensive among the obstructive group, whereas no difference was observed between 99mTc-DTPA and Technegas (Table 2).

Relationship between DTPA and Technegas ventilation SPECT images regarding degree of overall unevenness (A), central deposition (B), and degree of peripheral deposition (C). Right panels show difference between DTPA and Technegas scores against average score of 2 ventilation radiopharmaceuticals. Dotted lines in right panels represent 95% limits of agreement.

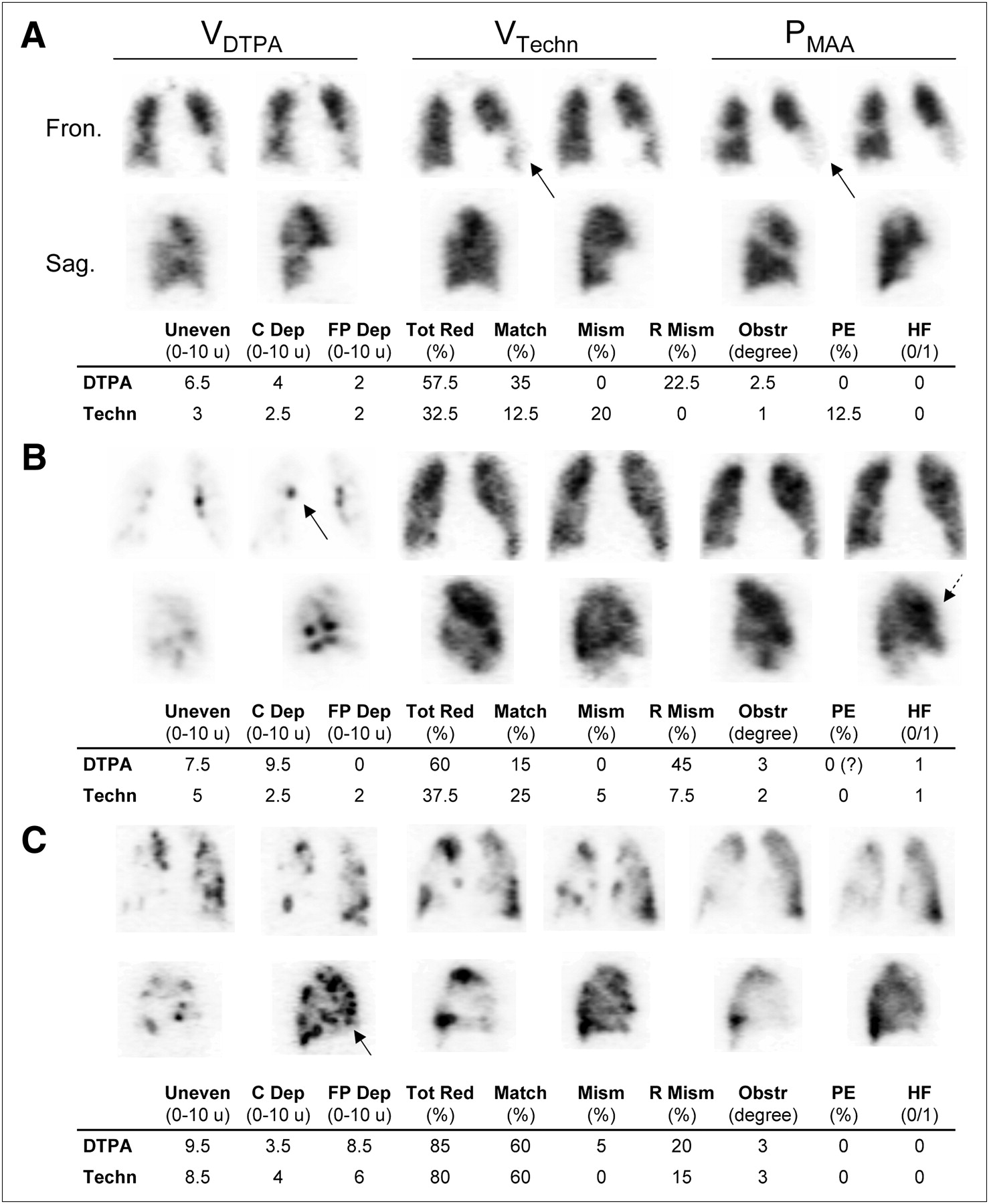
V/P SPECT images and mean interpretation scores from 3 patients with COPD. (A) Mild obstructive lung disease. Signs of pneumonia in lingular segments on CT with corresponding nearly matched reduction in V/P scans (arrows). PE is clinically suspected, as was also the case when Technegas ventilation images were used. (B) Moderate COPD and congestive heart disease. Both physicians expressed interpretation difficulties when using DTPA because of severe central deposition (solid arrow). Dashed arrow shows redistribution of perfusion to anterior parts of lungs as sign of heart failure. (C) Reduced ventilation and perfusion due to severe COPD with emphysema. Considerable peripheral deposition of ventilation radiopharmaceuticals is seen (arrow). C dep = central deposition; fron. = frontal; FP dep = focal peripheral deposition; HF = heart failure; match = matched reduction/defects; mism = mismatched reduction/defects; obstr = obstruction; R mism = reverse mismatched reduction/defects; sag. = sagittal; Techn = Technegas; tot red = total reduction in lung function; u = units; uneven = overall unevenness.
Distribution of Results from Qualitative V/P SPECT Evaluation
Reverse mismatch was significantly more extensive with 99mTc-DTPA in both groups (Supplemental Fig. 2B; Table 2).
Mismatch was observed, particularly among nonobstructive patients, because of a higher prevalence of PE (Table 2). In the obstructive group, the extent of mismatch was significantly higher when Technegas was used (Table 2.)
Among the 28 nonobstructive patients, 7 were found by both readers to have Technegas findings positive for PE. In 6 of these, PE was also diagnosed with 99mTc-DTPA. Among the 35 obstructive patients, 3 were found by both readers to have Technegas findings positive for PE (Fig. 3A). In just 1 of these, PE was also diagnosed with 99mTc-DTPA, and by only 1 of the 2 observers. In the 4 patients with signs of PE identified by both readers with Technegas only, the extent of mismatch was no more than 17%.
DISCUSSION
This intraindividual, head-to-head comparative study shows that, compared with 99mTc-DTPA, Technegas is more homogenously distributed in the lungs and has less focal deposition in both larger and smaller airways. Technegas shows fewer areas with reverse mismatch, that is, areas where ventilation appears to be lower than perfusion. In obstructive disease patients, the better peripheral penetration results in a significantly higher level of mismatched perfusion defects (P < V). In 99mTc-DTPA studies, the more uneven distribution pattern and lower peripheral penetration makes COPD patients appear to have more severe obstruction. Even in patients without any known obstructive disease, 99mTc-DTPA frequently indicates more uneven distribution and a higher degree of central focal deposition because of impaction in large airways. In patients with normal and near-normal ventilation patterns, however, there is a close correlation between 99mTc-DTPA and Technegas (Fig. 1).
For evaluating PE in patients with normal ventilation, 99mTc-DTPA has good diagnostic properties comparable to those of both krypton and xenon (16,27). This study indicated that both 99mTc-DTPA and Technegas identify the presence of PE, in nonobstructive disease patients, when the criteria set out are applied. Among patients without prior known obstructive lung disease, PE was diagnosed in 6 patients using 99mTc-DTPA and in 7 using Technegas.
In patients with compromised ventilation, however, 99mTc-DTPA has a more uneven distribution and the risk of central and focal peripheral deposition is high. These disadvantages could lead to an increased incidence of misdiagnosis and do not facilitate the diagnosis of other cardiopulmonary diseases. In 4 V/P SPECT image sets acquired using 99mTc-DTPA, the physicians experienced difficulty in interpreting the poor-quality ventilation images (Fig. 3B).
It is important to diagnose PE in patients with COPD, as PE is common in this group (28). PE accounts for up to 10% of deaths in patients with stable COPD. In the COPD patients, radioaerosol distribution was less even using 99mTc-DTPA, rendering differentiation between match and mismatch more difficult. Underestimation of mismatch may then lead to falsely negative findings for PE.
In the obstructive group, mismatches fulfilling the criteria for PE were observed only with Technegas (Fig. 3A). It is notable that the criteria were conceived and documented for patient populations in whom acute PE is clinically suspected (17). In obstructive disease patients in whom there was no such suspicion, the findings of mismatch in small areas may relate to previous episodes of PE and, as such, may be a warning sign of impending major or chronic embolism or may be a consequence of vascular remodeling in COPD. More study is required in this field.
In the absence of Technegas, consideration should be given to using the 3-dimensional V/P SPECT technique (19) even if performed with 99mTc-DTPA, as this has been shown to be superior to 2-dimensional planar imaging in diagnosing PE (6,7).
99mTc-DTPA, with its water-soluble properties, has an important role as a technique to assess epithelial integrity—a role that Technegas cannot replace. Although unaware of patient history, both physicians identified all 3 alveolitis patients on 99mTc-DTPA ventilation images.
Recent guidelines of the European Association of Nuclear Medicine emphasized that V/P SPECT with holistic interpretation should be the procedure of choice for diagnostic imaging of patients with clinically suspected PE (17). V/P SPECT, with either 99mTc-DTPA or Technegas, can be used without contraindications and gives a low radiation burden. V/P SPECT has superior sensitivity, high specificity, a nearly 100% negative predictive value, and a rate of less than 3% for nondiagnostic findings (17). The present study verifies the recommendation that Technegas, when available, should be used in patients with airway obstruction. Because the presence of airway obstruction or otherwise impaired ventilation is not always easy to predict in patients with suspected PE, Technegas may be regarded as the radioaerosol of choice for PE diagnosis.
Further studies are needed to improve the diagnosis of obstructive and comorbid diseases.
CONCLUSION
This intraindividual comparative study shows that Technegas is the preferred radioaerosol, particularly in obstructive disease patients.
Acknowledgments
We thank Berit Olsson and the other technologists at the Department of Clinical Physiology for invaluable assistance. This study was partially financed by the Region of Scania (ALF).
Footnotes
-
COPYRIGHT © 2010 by the Society of Nuclear Medicine, Inc.
References
- Received for publication December 16, 2009.
- Accepted for publication February 4, 2010.





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Comparability of Quantifying Relative Lung Ventilation with Inhaled 99mTc-Technegas and 133Xe in Patients Undergoing Evaluation for Lung Transplantation
- V/Q Scanning Using SPECT and SPECT/CT
- 68Ga PET/CT Ventilation-Perfusion Imaging for Pulmonary Embolism: A Pilot Study with Comparison to Conventional Scintigraphy