


Abstract
Ventilation–perfusion (V/Q) scintigraphy is established for regional assessment of lung function in a variety of diseases, including pulmonary embolism (PE). PET/CT may further improve the accuracy and utility of V/Q imaging because of its superior technical characteristics. This pilot study assessed the feasibility of performing V/Q PET/CT and compared diagnostic utility with conventional V/Q imaging in patients with clinical suspicion of PE. Methods: Ten patients undergoing conventional V/Q imaging were prospectively recruited. PET/CT V/Q imaging was performed after inhalation of 68Ga-carbon nanoparticles (“Galligas”) and administration of 68Ga-macroaggregated albumin. Blinded to the results of the other study, SPECT/CT (n = 9) or SPECT (n = 1) images and PET/CT images were graded by a predefined scoring system for scan quality. The number of matched or unmatched defects and diagnosis were also measured and compared with a final diagnosis. Results: PET image quality was equivalent or superior to SPECT in all patients, with more homogeneous radiotracer distribution for both ventilation and perfusion studies (P < 0.01). Based on conventional V/Q imaging, the diagnosis was acute PE in 2 patients and no PE in 7 patients, and the imaging results were nondiagnostic in 1 patient. The PET/CT diagnosis was concordant in 8 patients, and these studies demonstrated a similar number and distribution of matched and unmatched defects. In 1 discordant case, a patient with a SPECT/CT study that was nondiagnostic because of severe airway disease showed no PE on PET/CT. In another, the diagnosis of PE established on SPECT/CT was not reported on PET/CT 2 d later, possibly because of interval clot lysis or migration. Conclusion: This intraindividual comparative study demonstrated that V/Q PET/CT with 68Ga-labeled radiotracers can be performed in clinical practice. Compared with conventional V/Q imaging, advantages include higher-resolution, fully tomographic images with potentially better regional quantitation of lung function. The short half-life of 68Ga also enables more flexible acquisition protocols with the option of performing ventilation studies selectively on patients with abnormal perfusion. On the basis of our results, further studies are indicated to assess whether V/Q PET/CT can improve diagnostic algorithms for patients with suspected PE.
Ventilation–perfusion (V/Q) scintigraphy allows assessment of regional lung function in a variety of diseases. Most studies are performed to assess patients with suspected pulmonary embolism (PE) because presenting symptoms and signs are variable and insufficient for a clinical diagnosis. The Prospective Investigation of Pulmonary Embolism Diagnosis study (1), designed in 1983, established V/Q imaging as the standard of care at the time. V/Q imaging has improved in the past 3 decades because of major advances in image acquisition, reconstruction, and analysis techniques. The use of 99mTc-labeled carbon nanoparticles (Technegas; Cyclopharm) has improved the assessment of ventilation because of favorable imaging characteristics and small particle size, resulting in better peripheral distribution than is obtained with other aerosol techniques (2,3).
Planar scintigraphy is limited by the small number of views, with each representing a summation of data that includes overlapping lung activity. SPECT overcomes this limitation, leading to improved sensitivity, specificity, and reproducibility and a lower number of inconclusive reports (4–7). In a large prospective series, V/Q SPECT had a high negative predictive value for excluding PE (8). The advent of hybrid SPECT/CT devices further improved diagnostic accuracy by enabling anatomic characterization of scintigraphic abnormalities (9,10). The CT component also assists diagnosis by identifying nonembolic causes of the symptoms of shortness of breath and pleuritic pain that raise suspicion of PE. The causes of such symptoms include lung infection, pleural abnormalities, and bone abnormalities.
PET offers a unique opportunity to further improve the accuracy and utility of V/Q imaging. PET provides vastly superior image quality and speed compared with conventional γ-camera imaging, and is an intrinsically quantitative volumetric modality. V/Q PET/CT is now possible by substituting 99mTc with 68Ga, a positron-emitting radionuclide, using the same carrier molecules as conventional V/Q imaging. Ventilation imaging can be performed with 68Ga-carbon nanoparticles using the same synthesis device as Technegas, yielding “Galligas” (11). Perfusion imaging can be performed with 68Ga-macroaggregated albumin (68Ga-MAA). 68Ga has a short half-life of 68 min and is conveniently available on demand using a small on-site generator (12). Furthermore, all commercially available scanners are now combined with multislice CT (PET/CT), enabling detailed anatomic correlation.
We report the results of a pilot study of V/Q PET/CT performed on a cohort of patients with clinical suspicion of PE investigated with conventional V/Q imaging. The objective of this study was to assess the feasibility of performing V/Q PET/CT in a routine clinical setting and to compare the image quality and diagnostic utility with that of conventional V/Q imaging (SPECT/CT or SPECT).
MATERIALS AND METHODS
Patients
Patients with suspected PE who were referred for V/Q imaging or CT pulmonary angiography (CTPA) were approached for participation in the pilot study. Ten patients were prospectively recruited (age range, 24–70 y) over a 4-mo period from July 2010. All underwent diagnostic V/Q SPECT beforehand, 9 with contemporaneous CT using a hybrid scanner, and 2 also underwent CTPA. V/Q PET/CT was performed after the conventional modality. Pretest probability was assessed according to the score of Wells et al. (13). Two patients had a high pretest probability, 7 a moderate probability, and 1 a low probability, for PE. Table 1 provides more detailed baseline characteristics of the cohort. Exclusion criteria included age less than 18 y, pregnancy, breast-feeding, and an inability to tolerate supine positioning on the PET/CT bed. Written informed consent was provided by each patient. The research protocol (10/24) was approved by the Clinical Research Committee and the Ethics Committee at the Peter MacCallum Cancer Centre.
Summary of Patient Characteristics
68Ga Radiotracer Production
68Ga was eluted using an on-site 68Ge/68Ga generator (IDB Holland BV), purified through a method previously described (12).
Galligas was prepared using a commercially available Technegas generator (Cyclopharm). With this device, Galligas was prepared using the same technique as for Technegas production with substitution of 68Ga for 99mTc. Approximately 50 MBq of 68Ga in the form of gallium chloride were placed in the carbon crucible of the synthesis unit.
68Ga-MAA was prepared using Pulmolite (Pharmalucence Inc.). This was washed with deionized water and dispensed into three 1-mL aliquots containing MAA particles of between 250,000 and 800,000 particles. 68Ga was buffered with acetate buffer to pH 6.5 before being added to the MAA aliquot. The suspension mixture was incubated for 5 min at 70°C after the addition of 68Ga. Labeling efficacy in excess of 90% was demonstrated by comparing the activity present in the supernatant after isolation by centrifugation with the total activity of the combined sediment and supernatant, and also by measuring the amount of labeled MAA retained within a 0.22-μm Millex filter (Millipore). Analysis using a hemocytometer demonstrated no discernable differences in particle size.
Conventional V/Q Imaging
Nine patients underwent V/Q SPECT/CT using a routine clinical protocol; 1 patient was imaged at another facility using a stand-alone V/Q SPECT scanner. At our center, a 2-head SPECT/CT system fitted with low-energy, high-resolution collimators was used (Symbia T6; Siemens Medical Systems). Technegas was produced after insertion of 600–800 MBq of 99mTc-pertechnetate in the carbon crucible of the synthesis unit. After inhalation, ventilation SPECT was performed with 32 steps of 25-s duration and contour detection. A mean of 218 MBq (range, 193–255 MBq) of 99mTc-MAA was administered intravenously, and the perfusion SPECT was performed with similar parameters, except for speed, which was 15 s per step. Afterward, low-dose CT was performed (CARE Dose, 40 effective mAs; Siemens). SPECT images were reconstructed using the Flash 3D iterative algorithm (Siemens) without attenuation correction.
PET/CT
Each patient inhaled Galligas in a supine position, using the same technique as for Technegas. This inhalation took place in a room separate from the PET/CT scanner to avoid any potential contamination. The estimated inhaled activity was 10 MBq. The patient was imaged supine, with arms up and resting behind the neck. The scanner was a Discovery STE (GE Healthcare), which incorporates an 8-slice multidetector CT component. Low-dose CT was performed without intravenous contrast material (140 kVp, 40–200 mAs; Smart mA [GE Healthcare]), followed by the ventilation PET acquisition (2 or 3 bed positions of 3 min each). Without movement of the patient, a mean of 39 MBq (range, 25–60 MBq) of 68Ga-MAA was injected as a slow intravenous bolus. This dose approximates a 1:4 activity ratio between ventilation and perfusion imaging. Lung perfusion PET was performed using the same bed positions and parameters as for the ventilation study. Images were reconstructed with attenuation correction, using an ordered-subset expectation maximization algorithm.
Image Interpretation and Data Analysis
Ventilation studies were paired with the corresponding perfusion studies and reviewed on an eSoft multimodality workstation (Siemens). V/Q SPECT/CT or SPECT images and V/Q PET/CT images were reviewed by 2 experienced physicians in tandem, who did not know the results of the other examination. The images were reviewed in random order, with an interval of 1 wk between each modality, according to a predefined scoring system. First, V/Q images were characterized as normal, abnormal, or nondiagnostic. Second, 3 qualitative parameters were used as previously defined by Jogi et al. (3) to assess image quality: unevenness of radioaerosol distribution, deposition of radioaerosol in major and intermediate conducting airways (i.e., central deposition), and focal peripheral deposition in more distal airways. Each of these parameters was scored from 0 (none or normal) to 10 (very high). A paired-sample t test was used to compare the 2 groups (SPSS Statistics, version 19; IBM). Third, the number of matched and unmatched defects within each lobe was counted and characterized as segmental, subsegmental, or nonsegmental. Finally, a diagnosis of presence or absence of PE was assigned. Images were interpreted in the context of clinical history, using criteria as recommended by the guidelines of the European Association of Nuclear Medicine (14), with the addition of anatomic correlation from the low-dose CT.
A subsequent side-by-side review of any images from patients with discordant results between SPECT/CT and PET/CT was performed to identify possible reasons for the discordance. A final diagnosis was obtained after review of subsequent medical records, including clinical review and imaging.
RESULTS
All patients tolerated V/Q PET/CT without complication. In 5 patients, the PET/CT was performed on the same day as the SPECT/CT, with the interval varying between 1 and 8 d for the remaining patients.
For the qualitative parameters used to assess image quality (Fig. 1; Supplemental Table 1 [supplemental materials are available online only at http://jnm.snmjournals.org), PET ventilation imaging demonstrated a more homogeneous distribution and a lower (better) score for unevenness in each patient; the mean score for unevenness was 1.1 for PET, compared with 3.7 for SPECT (P < 0.01). Focal deposition in the peripheral airways was lower on the PET study in 2 patients, and no peripheral clumping was seen for either modality in the remaining patients (mean score, 0.4 vs. 2.7; P = 0.08). In patients with obstructive airway disease, central airway deposition was observed in both groups (mean score, 1.4 vs. 2.0; P = 0.18). PET perfusion imaging demonstrated a more homogeneous distribution than SPECT in 8 patients, with normal perfusion seen on both modalities in the remaining 2 patients (mean score, 0.4 vs. 2.7; P < 0.001). Image quality was difficult to fully define with any qualitative or quantitative parameter. Figures 2–4 present comparative images.
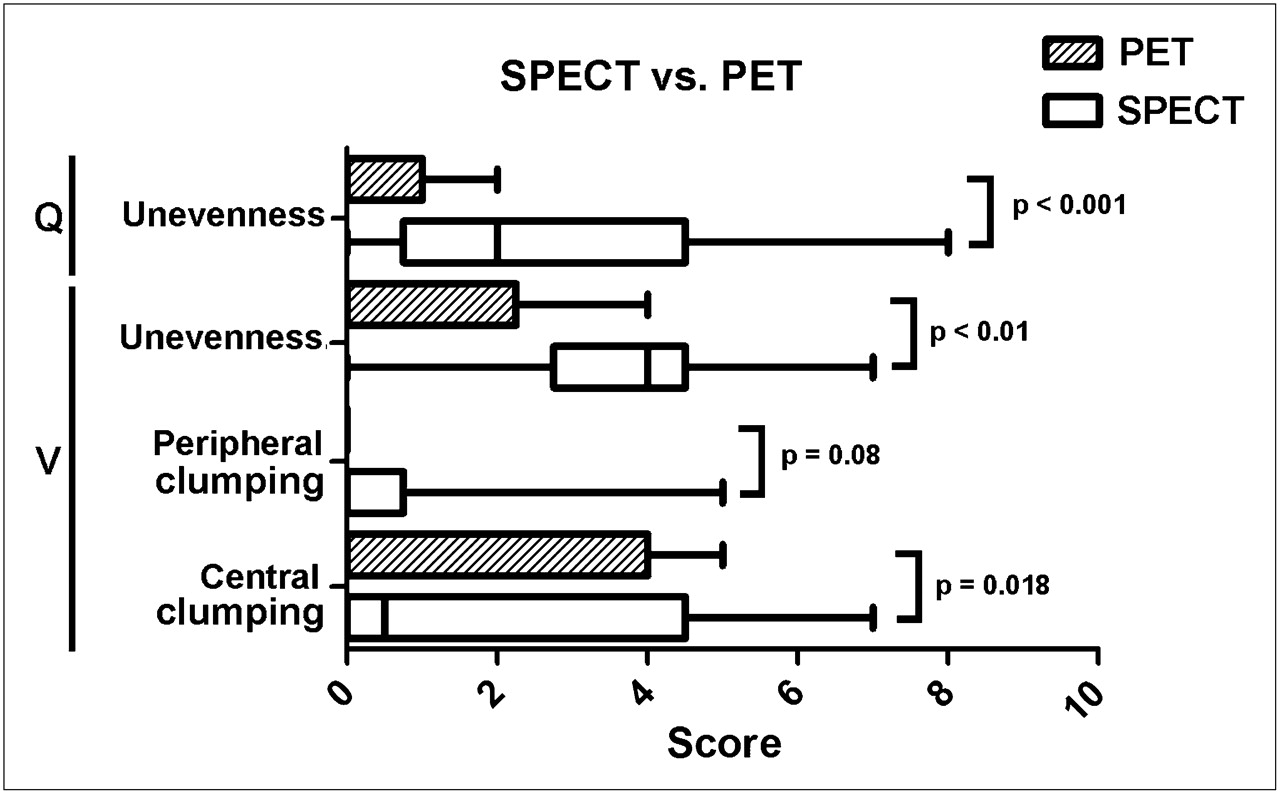
Box plot comparing qualitative image scores. Score ranges from 0 to 10, with 0 representing none or normal.

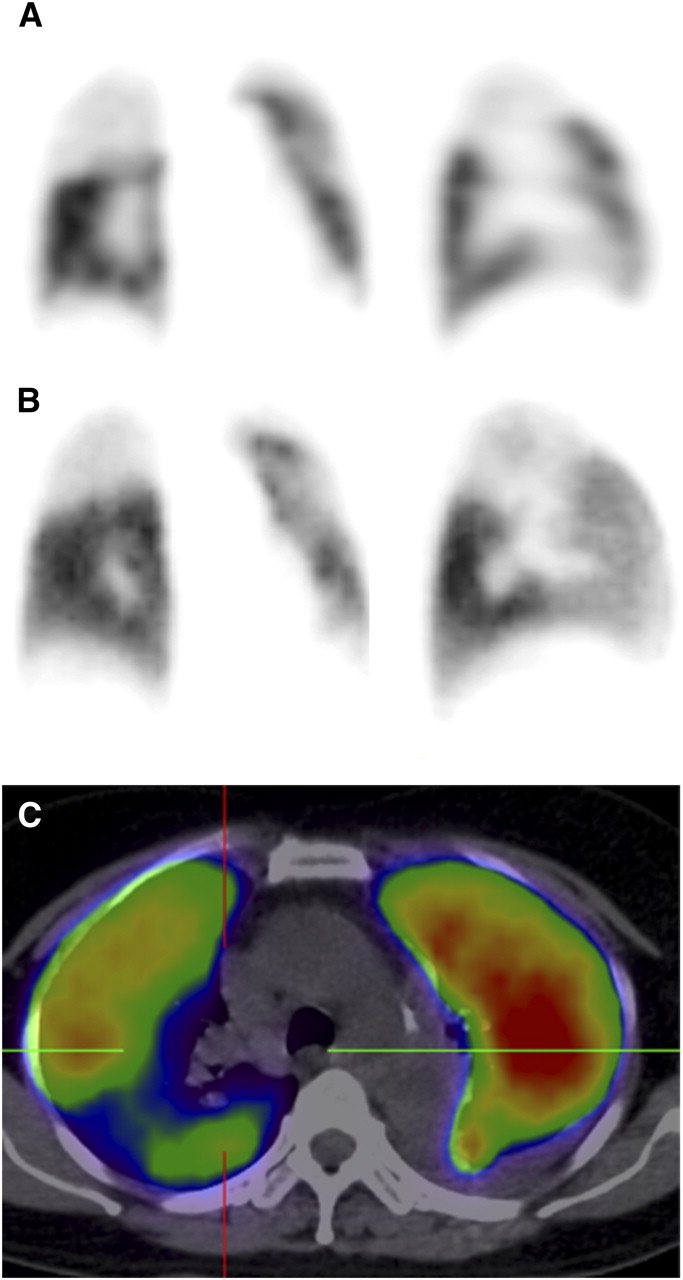
Representative coronal slice of patient 9, with severe chronic obstructive airway disease. (A) SPECT ventilation image was deemed nondiagnostic because of marked clumping and poor peripheral distribution of radiotracer. (B) PET image also demonstrates clumping, but peripheral distribution is more homogeneous, with corresponding matched changes on perfusion imaging enabling exclusion of PE with higher confidence. (C and D) Fused PET/CT (C) and low-dose CT (D) demonstrate no evidence of consolidation.

Coronal (left) and sagittal (right) SPECT (A), PET (B), and PET/CT (C) perfusion images of patient 5, demonstrating multiple segmental unmatched perfusion defects with near-normal ventilation (not shown). Diagnosis of PE was confirmed on follow-up. PET perfusion study was performed 8 d after SPECT study, accounting for resolution of some perfusion abnormalities.
Coronal and sagittal SPECT perfusion (A), PET perfusion (B), and axial PET/CT (C) images in patient with non–small cell lung carcinoma. Right upper lobe shows large unmatched perfusion defect (normal ventilation not shown). On its own, this may be interpreted as consistent with PE, but correlative CT demonstrates extensive mediastinal lymphadenopathy with extrinsic compression of right upper lobe pulmonary artery, a more likely explanation for findings than PE. Contrast-enhanced CT confirmed findings.
Three patients demonstrated normal ventilation and perfusion on both SPECT/CT and PET/CT. In 5 patients, matched and unmatched segmental or subsegmental defects were observed with a similar frequency and distribution between the 2 modalities. In the remaining 2 patients, SPECT/CT and PET/CT images were discordant. One of these patients (patient 10) had unmatched defects evident on SPECT/CT that were not visualized on PET/CT, and the other (patient 9) had severe chronic obstructive airway disease with images deemed nondiagnostic on SPECT/CT. Supplemental Table 2 summarizes the comparison between conventional V/Q imaging and PET/CT. Nonsegmental defects attributable to postradiotherapy changes or to consolidation or atelectasis were similar in number and distribution.
On the basis of conventional V/Q imaging, the diagnosis was acute PE in 2 patients and no PE in 7 patients, and the results for 1 patient were nondiagnostic (Table 2). The PET/CT diagnosis was concordant in 8 patients and discordant in 2. One case of discordance was a patient with a nondiagnostic SPECT/CT study that was interpreted as demonstrating no evidence of PE on PET/CT (patient 9). This patient had chronic obstructive airway disease and clumping of radiotracer in the proximal airways, with poor peripheral distribution, such that the SPECT interpretation in the context of a blinded reading was deemed nondiagnostic. The clinical report, however, raised the possibility of chronic PE. This case highlights the potential for interobserver disagreement in patients with low-quality images. PET/CT also demonstrated central clumping but better peripheral visualization, enabling more confident interpretation (Fig. 2). On the basis of the original clinical report, the patient was given anticoagulation therapy. A repeated V/Q study 3 wk after anticoagulation demonstrated no change in appearance, supporting the diagnosis of airway disease and the validity of the PET/CT findings.
Conventional V/Q and PET/CT V/Q Results
The other case of discordance was a patient in whom PE was demonstrated on SPECT/CT but not on PET/CT, which was performed 34 h later after initiation of anticoagulation (patient 10). On review, subtle smaller unmatched perfusion defects concordant with the prior SPECT/CT study were evident but were insufficient to allow prospective identification. Clot lysis or migration may account for the findings. This patient received anticoagulation therapy, and a repeated V/Q SPECT/CT study 4 mo later had normal findings, supporting the diagnosis of PE. Follow-up was available for all remaining patients, and the diagnosis was concordant with both the conventional V/Q finding and the PET/CT findings.
DISCUSSION
The diagnosis and management of PE remains a clinical challenge despite advances in technology. V/Q imaging and CTPA are widely used as primary diagnostic methods. Studies report high accuracies, with sensitivity and specificity greater than 90%–95% (15), but results vary widely between studies (16) and are confounded by the lack of an accurate gold standard and consequent verification bias. Moreover, there is significant interobserver disagreement as demonstrated by only moderate agreement, with a κ of 0.47 for 3-mm-collimation CTPA (17). Many practitioners fail to realize the limitations of imaging tests, leading to both overdiagnosis and a delay in treatment, particularly when there is discordance between clinical pretest likelihood and the imaging result. Indeed, among a cohort of 322 patients with a varying pretest likelihood of PE, Ranji et al. demonstrated a 25% false-positive rate for CTPA even under optimistic assumptions of accuracy (18). Accordingly, there is a need for newer imaging modalities with higher accuracy and reproducibility.
PET/CT offers an opportunity to further improve management of patients with suspected PE (19). V/Q imaging allows assessment of the functional consequences of PE, whereas CTPA enables visualization of the embolus itself. Thus, both modalities provide complementary information, and at times both are needed to reach a confident diagnosis. Even in centers that have adopted CTPA as a first-line imaging modality, many patients undergo V/Q imaging. In the Prospective Investigation of Pulmonary Embolism Diagnosis II study, 50% of eligible patients could not undergo CTPA because of renal dysfunction, critical illness, or contrast allergy. Furthermore, 6% of studies were of insufficient quality for conclusive reporting, and 1% had complications. By contrast, V/Q imaging has no absolute contraindications and anaphylaxis has not been reported.
The radiotracers used in this study, Galligas and 68Ga-MAA, are similar to their 99mTc analogs, for which there are several decades of experience. 68Ga is an ideal radiotracer for clinical use, with on-site generator-based production, short half-life, and positron emission. The concept of positron lung imaging, however, is not new, with 68Ga-labeled albumin perfusion imaging demonstrated in a canine model in 1975–1979 (20,21). 68Ga-MAA PET, analogous to 99mTc-MAA scintigraphy, is accomplished by microembolization of radiolabeled particles within pulmonary arterioles, accurately defining regional lung perfusion (22). Regional assessment of ventilation with PET has been performed with 13N-nitrogen gas washout (23), but application beyond the research setting is impractical. More recently, substitution of 99mTc by 68Ga has been successfully demonstrated as a viable radioaerosol for PET (11,24), enabling combined PET V/Q imaging (25). Galligas, analogous to Technegas, is an aerosol comprising extremely small radiolabeled solid graphite particles that are deposited in the alveolar space, enabling ventilation imaging (26,27). In a piglet study (that included a control group) of induced lobar obstruction and methacholine-induced diffuse airway obstruction, Galligas demonstrated more detailed assessment of ventilation than did Technegas (24).
The results of this study suggest that V/Q PET/CT may be a suitable alternative to conventional V/Q imaging, given image quality that is equal or superior, as was expected in view of the superior imaging resolution and radiotracer counting sensitivity of PET, compared with SPECT technology. Although improved accuracy and reproducibility ought to result from V/Q PET/CT, confirming studies will be needed. A higher specificity is advantageous, but a greater sensitivity has the potential to detect small PEs that may be of lower or no clinical significance (28). This study was limited by inclusion of only 10 patients in a population that may not be representative of clinical practice in a noncancer center. Accordingly, larger studies will be needed to determine appropriate thresholds for anticoagulation.
68Ga has a short half-life that enables more flexible imaging protocols, such as performing ventilation imaging after the perfusion study. Accordingly, if the results of the perfusion study are normal, a ventilation study would not be necessary, improving the patient journey, decreasing radiation exposure, and allowing a rapid diagnosis. The ventilation scan could still be performed on the same day by allowing a few hours for decay, without compromising diagnostic quality by spillover of activity from the prior study. On a current-generation PET/CT scanner with an extended field of view, it will be possible to complete the perfusion or ventilation component of the study in 3–6 min, compared with 15–20 min for a SPECT study. The effective radiation dose of approximately 3–5 mSv is similar between the modalities: 2 mSv for a SPECT or PET acquisition (11) plus an additional 1–3 mSv for the low-dose CT component.
The ability to noninvasively quantify pulmonary blood flow and alveolar ventilation with V/Q PET/CT has the potential to improve our understanding of pulmonary physiology in a wide spectrum of diseases (29). This technique has potential application in the presurgical evaluation of patients undergoing lung volume reduction surgery (30), in the assessment of pulmonary reserve in lung cancer patients before radiotherapy or surgery, and in the advancement of understanding about airway diseases such as chronic obstructive pulmonary disease, asthma, and interstitial pulmonary disease (9,31). Further trials to assess regional changes brought about by interventions or treatment, or merely to examine the natural history of a variety of pulmonary diseases, would be of interest.
CONCLUSION
We demonstrated that V/Q PET/CT with 68Ga-labeled radiotracers is feasible and can be incorporated into clinical practice. This technique is attractive in the context of the recent shortages in the supply of 99mTc. Compared with conventional V/Q imaging, the advantages of 68Ga-labeled V/Q PET/CT include superior image quality and faster acquisition. These may improve the outcomes of patients with suspected PE through more accurate diagnosis. In centers with access to PET/CT, rapid adoption of this new technology may be possible without an increase in cost, compared with conventional scintigraphy. The short half-life of 68Ga also enables more flexible acquisition protocols with the option of performing ventilation studies selectively in patients with abnormal perfusion or proceeding directly to CTPA to further validate suggestive abnormalities. Further study is needed to assess whether V/Q PET/CT can improve diagnostic algorithms for patients with suspected PE.
DISCLOSURE STATEMENT
The costs of publication of this article were defrayed in part by the payment of page charges. Therefore, and solely to indicate this fact, this article is hereby marked “advertisement” in accordance with 18 USC section 1734.
Acknowledgments
No potential conflict of interest relevant to this article was reported.
Footnotes
Published online Sep. 9, 2011.
- © 2011 by Society of Nuclear Medicine
REFERENCES
- Received for publication May 16, 2011.
- Accepted for publication July 14, 2011.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- A Technical Overview of Technegas as a Lung Ventilation Agent
- Single-arm prospective interventional study assessing feasibility of using gallium-68 ventilation and perfusion PET/CT to avoid functional lung in patients with stage III non-small cell lung cancer
- Correlation of 68Ga Ventilation-Perfusion PET/CT with Pulmonary Function Test Indices for Assessing Lung Function