


Abstract
Despite the fact that several studies have been published regarding the prognostic factors of neuroendocrine tumors (NETs), there are some cases in which available data are not sufficient to predict disease progression and to define a correct therapeutic approach. To our knowledge, the role of maximum standardized uptake value (SUVmax) as a prognostic factor has never been studied in NET patients. Therefore, we prospectively investigated whether 68Ga-[1,4,7,10-tetraazacyclododecane-1,4,7,10-tetraacetic acid]-1-NaI3-octreotide (68Ga-DOTANOC) PET SUVmax could be used as an accurate noninvasive marker for disease prognosis. Methods: Forty-seven patients with NETs were studied with 68Ga-DOTANOC PET. All patients underwent a baseline visit and laboratory and radiologic examinations. Follow-up was performed in all cases. Results: SUVmax was significantly higher in patients with pancreatic NET and in those with well-differentiated NETs. Moreover, SUVmax was significantly higher in patients with an elevated expression of 2A-somatostatin receptor. During the follow-up, the disease was stable or presented a partial response in 25 patients, and in 19 cases the disease progressed. The patients with stable disease or a partial response had an SUVmax significantly higher than did those in the progressive disease group, with the best cutoff ranging from 17.9 to 19.3. At univariate and multivariate analysis, the significant positive prognostic factors were well-differentiated NET, an SUVmax of 19.3 or more, and a combined treatment with long-acting somatostatin analogs and radiolabeled somatostatin analogs. Conclusion: We demonstrated, for the first time to our knowledge, that 68Ga-DOTANOC PET SUVmax correlates with the clinical and pathologic features of NETs and is also an accurate prognostic index.
Neuroendocrine tumors (NETs) are a rare and heterogeneous group of neoplasms originating from the neural crest. The main localization of NETs is in the gastroenteropancreatic tract, lung, and, rarely, ovary and thymus (1). Although NETs are generally slow-growing, the outcome of the disease is extremely variable. Several studies have been published regarding the prognostic factors of the disease, such as the localization of the primary tumor, grade of differentiation, proliferation index, presence of somatostatin receptors (SSTRs), and tumor stage at the time of diagnosis (2–8). However, there are some cases in which the available data are not sufficient to predict the disease progression and, consequently, to plan a correct therapeutic approach.
In recent studies (9–11) in limited patient populations, it has been suggested that 68Ga-[1,4,7,10-tetraazacyclododecane-1,4,7,10-tetraacetic acid] (DOTA)-peptide PET is useful in diagnosing NETs (i.e., visualization, initial staging, and detection of relapse) and in evaluating the possibility of planning radiolabeled therapy. 68Ga-DOTA-peptides (DOTA-d-Phe1,Tyr3-octreotide, DOTA-[1-NaI3]-octreotide [DOTANOC], and DOTA-d-Phe1,Tyr3-octreotate) are new PET tracers that specifically bind to SSTRs overexpressed on the surface of NET cells. Although studies of direct comparison of these tracers have not yet been performed, 68Ga-DOTANOC seems to be the most promising peptide for the broader SSTR subtype affinity (binding to SSTR2, SSTR3, and SSTR5) and has an acceptable dosimetry (12,13).
It is well known that in PET studies using metabolic tracers, such as 18F-FDG, the maximum standardized uptake value (SUVmax) reflects the rate of the tracer metabolism and represents a parameter for detection of the metabolic activity of neoplastic lesions. Several authors reported that 18F-FDG PET SUVmax was a predictor of patient survival and therapeutic response in different forms of solid and hematologic neoplasms (14–16).
When ligand tracers (such as 68Ga-DOTA-peptides) are used, the biologic significance of SUVmax corresponds to the receptor availability on the cell surface. Because NET lesions overexpress SSTRs, 68Ga-DOTA-peptides are particularly relevant for the assessment of these tumors that cannot be visualized easily on 18F-FDG PET scans because of their slow metabolism. 68Ga-DOTANOC PET is relevant not only for diagnostic purposes but also as a noninvasive tool to demonstrate the receptor expression status of tumor cells, which is crucial in the selection of candidate patients for somatostatin analog therapy.
Information regarding the role of the 68Ga-DOTANOC PET SUVmax in patients with NET is lacking. In the present article, we prospectively investigated whether the determination of this index may be useful as a prognostic marker in NET patients.
MATERIALS AND METHODS
Among the 47 subjects who underwent 68Ga-DOTANOC PET from September 2006 to May 2008, we studied those with histologic confirmation of a NET, presenting disease at both 68Ga-DOTANOC PET and CT scans, and who had been treated with somatostatin analogs or surgery only or were not treated at all before PET.
All patients underwent physical examination, and their clinical history was taken with the aim of investigating the putative clinical features of the functioning tumors. Laboratory and radiologic examinations were performed to evaluate the localization of the tumor and to stage the disease (7,8).
Tissue for the evaluation of the Ki67 index was available in 33 patients (70.2%), and the expression of SSTR type 2A (SSTR2A) was evaluated in 14 patients (29.8%). The patients were divided into 2 groups according to a Ki67 cutoff value of 5% (17). NETs were classified as functioning when clinical symptoms associated with an increase of serum peptide levels were present and as nonfunctioning when these symptoms were lacking.
The enrolled patients underwent a clinical check-up and a CT scan every 3 mo during the first year and every 6 mo thereafter. In the follow-up period, according to the Response Evaluation Criteria in Solid Tumors, the patients were categorized into stable disease, partial response (PR), and progressive disease (PD) groups. Surgical and medical procedures (long-acting somatostatin analog therapy with Sandostatin LAR [30 mg; Novartis Oncology] or Lanreotide Autogel [120 mg; Ipsen] every 28 d or radiolabeled therapy) were also recorded.
Immunostaining Method
Multiple paraffin sections (thickness, 4 μm) were collected, and the slides were processed by immunohistochemistry using a non–biotin-amplified method (Novolink; Novocastra Laboratories). Briefly, the sections were dewaxed, rehydrated, and subjected to the proper antigen-retrieval treatment. After the sections were cooled at room temperature, endogenous peroxidase activity was inhibited using a methanol/H2O2 solution (0.5%) for 20 min. The sections were then washed in phosphate-buffered saline (pH 7.2–7.4), covered by polyclonal anti-SSTR2A antibody (BIOTREND; Chemikalien GmbH), and incubated overnight in a moist chamber at room temperature. The sections were then washed in phosphate-buffered saline and treated using Novolink reagents according to the instructions of the manufacturer.
Optimization of Immunostaining Technique
A serial section of a specific tissue macroarray made up of 1 normal pancreas and 2 neoplastic samples comprising 2 pancreatic NETs positive to the Octreoscan (Covidien) test (one characterized by optimal tissue preservation, the other poorly fixed) was used to define the best combination between dilution and antigen-retrieval treatment. The section was warmed at 98°C in a water bath using citrate buffer, pH 6.0, or Tris–ethylenediaminetetraacetic acid buffer, pH 9.0, for 20–40 min. The best treatment schedule resulted in a final dilution of 1:12,000 with citrate buffer at pH 6.0 and for 20 min at 98°C. Serial sections of the same tissue macroarray were used in each batch of slides to standardize immunohistochemistry-immunopositive staining.
Scoring System
The immunostaining evaluation considered membranous and cytoplasmic patterns.
Cytoplasmic membrane immunoreactivity was assessed using a semiquantitative score—the so-called quick score—incorporating both the percentage of positive tumor cells and staining intensity, as suggested by Reiner et al. (18). At each field (100×), the percentage and intensity score were attributed according to the following cutoff values: percentage, ≤1% = score 0, >1% ≤ 25% = score 1, >25% ≤ 50% = score 2, >50% ≤ 75% = score 3, and >75% = score 4; and intensity, weak = score 1, moderate = score 2, and strong = score 3. The product of percentage and staining intensity mean values was grouped as follows: <4 = low and ≥4 = high.
68Ga-DOTANOC PET
68Ga-DOTANOC was synthesized by the Radiopharmacy of the Nuclear Medicine Unit of S. Orsola-Malpighi Hospital. 68Ga was eluted from a 68Ge/68Ga generator, and DOTANOC was labeled with 68Ga following the procedure described by Zhernosekov et al. (19).
68Ga-DOTANOC PET scans were obtained using a dedicated hybrid PET/CT scanner (Discovery LS; GE Healthcare) for patients who had fasted for 6 h (68Ga-DOTANOC, intravenous injected dose, 185 MBq; uptake time, 60 min). PET emission images were recorded for 4 min per bed position; CT images were used for nonuniform attenuation correction (acquisition parameters, 140 kV, 90 mA, 0.8 s; tube rotation, 5-mm thickness). PET images were acquired from the skull base to the middle of the thigh.
PET results were evaluated by 2 experienced nuclear medicine specialists unaware of the results of the other imaging modalities. The final report was based on the agreement of the 2 reviewers.
Any localization with a greater intensity than background that could not be explained by physiologic activity (pituitary gland, spleen, liver, adrenals, kidneys, and urinary bladder) was considered to indicate SSTR expression.
SUVs
The SUVmax was calculated by measuring the maximal concentration of the labeled tracer in a region of interest and correcting it for patient body weight and injected dose (SUVmax = maximum activity concentration/[injected dose/body weight]) (20).
For each PET scan, the SUVmax was measured by choosing a region of interest that included the lesion presenting the highest tracer uptake. For large tumors, the region of interest was moved over several sites within the mass to ensure that the true SUVmax was obtained. All images were corrected for scatter, randoms, dead time, and decay. Images were reconstructed with a 2-dimensional ordered-subset expectation maximization iterative algorithm (2 iterations, 28 subsets).
Ethics
All patients gave their written informed consent to participate in the study. The study protocol was approved by the Senior Ethical Committee of the Department of Clinical Medicine of the University of Bologna and was performed according to the Helsinki Declaration for human studies.
Statistics
Mean, SD, median, range, and frequencies were used to describe the data. The data were analyzed by 1-way ANOVA. The distribution of the SUVmax was tested for normality by the Kolmogorov–Smirnov test; it showed a significant positive skewness and was log-transformed before analysis (P = 0.006 and P = 0.692 before and after transformation, respectively). The effects and their 95% confidence intervals (CIs) were estimated as antilog transformations of the analyzed data and were expressed as percentages after simple contrast had been applied. Progression-free survival was estimated by means of the Kaplan–Meier actuarial test, and the putative prognostic factors were tested by univariate and multivariate Cox regression; the hazard ratios, together with their 95% CIs, were also estimated. P = 0.05 and P = 0.10 were chosen as the cutoff values for entering or exiting, respectively, variables in the multivariate analysis. The area under the receiver-operating-characteristic curve was evaluated to determine the accuracy of the SUVmax at diagnosis in predicting the progression of the disease. The best prognostic cutoff value was estimated by a maximum likelihood ratio method (21). SPSS software (version 16.0; SPSS Inc.) was used to analyze data. Two-tailed P values less than 0.05 were considered statistically significant.
RESULTS
Patient Characteristics
Forty-seven patients (27 men and 20 women; median age, 62.8 y; age range, 40–80 y) with NETs were studied. Twenty-three patients (48.9%) had a NET of the pancreas, 18 (38.3%) had a gastrointestinal NET, and 6 (12.8%) had a NET of the lung.
Sixteen patients (34.0%) had a functioning NET: 2 insulinomas, 3 gastrinomas (Fig. 1), 1 glucagonoma, 1 VIPoma, and cases of carcinoid syndrome. In the remaining 31 (66.0%), the tumor was nonfunctioning. Six of the 47 patients (12.8%) had multiple endocrine neoplasia type 1.

Transaxial 68Ga-DOTANOC PET/CT scans of 62-y-old woman with multiple hepatic secondary NET lesions (gastrinoma). SUVmax of lesion with highest uptake was 41. At follow-up, patient showed partial response (PRRT plus somatostatin analogs).
At pathologic evaluation, 42 patients (89.4%) had a well-differentiated neuroendocrine carcinoma, whereas 5 (10.6%) had a poorly differentiated neoplasia. The mean Ki67 index (available in 33 patients) was 5.0% (range, 0.5%−19.0%); 20 of 33 patients (60.6%) had a Ki67 of 5% or less, and 13 of 33 patients (39.4%) had a Ki67 greater than 5%.
Of 14 patients, 8 (57.1%) had a low score of expression of SSTR2A, and the other 6 (42.9%) had a high score.
According to the TNM classification, 4 patients (8.5%) had stage I or II disease, 5 (10.6%) had stage III, and 38 (80.9%) had stage IV.
SUVs of 68Ga-DOTANOC
The mean values and the respective SD of the SUVmax among the different groups of patients are reported in Table 1.
Mean Values and Respective SD of SUVmax Among Different Groups of Patients
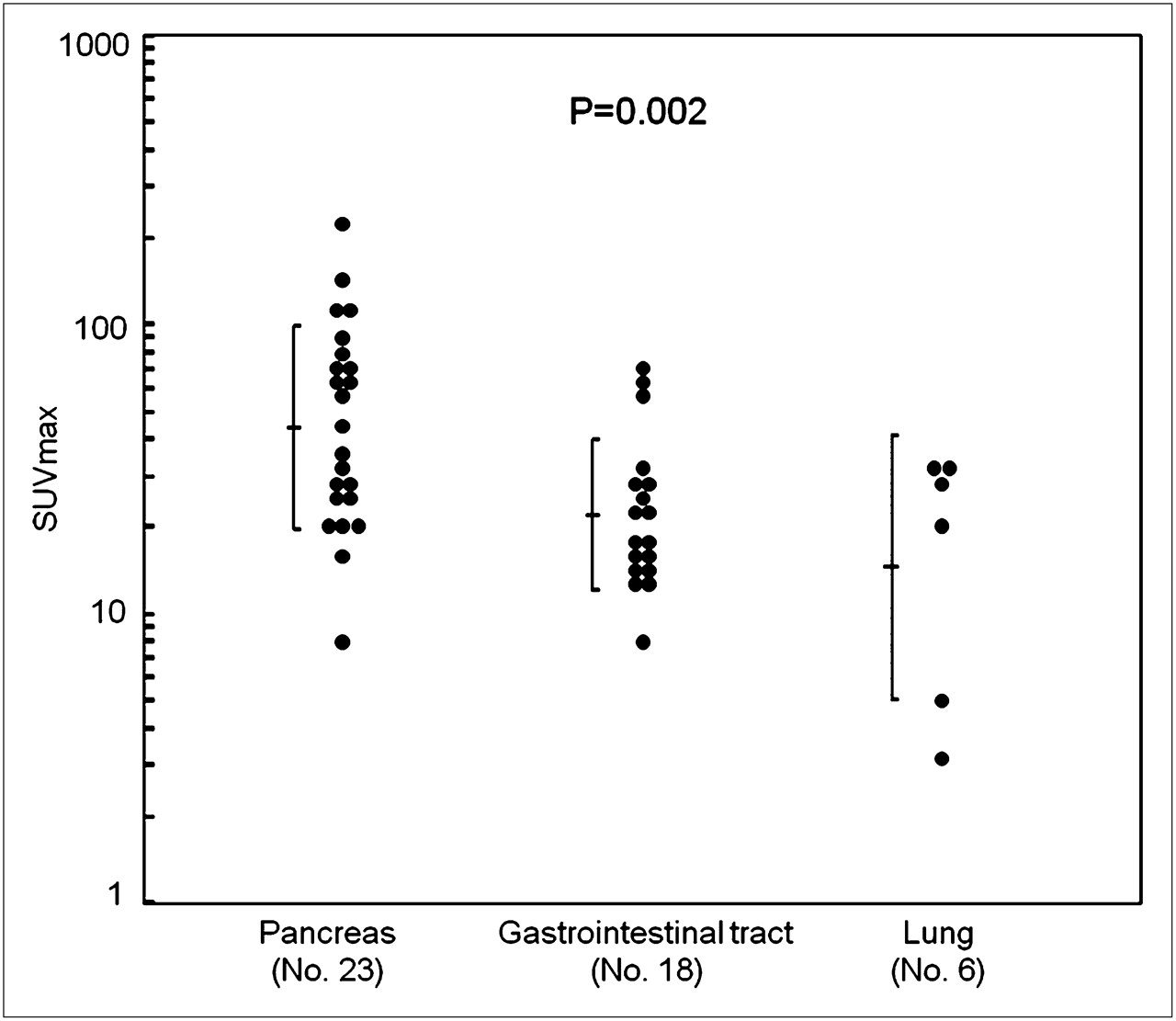
The SUVmax was significantly higher in patients with pancreatic NETs than in patients with gastrointestinal NETs (P = 0.006) and lung tumors (P = 0.003) (Fig. 2). Otherwise, we did not find any significant difference in the SUVmax between gastrointestinal and lung endocrine tumors (P = 0.255).
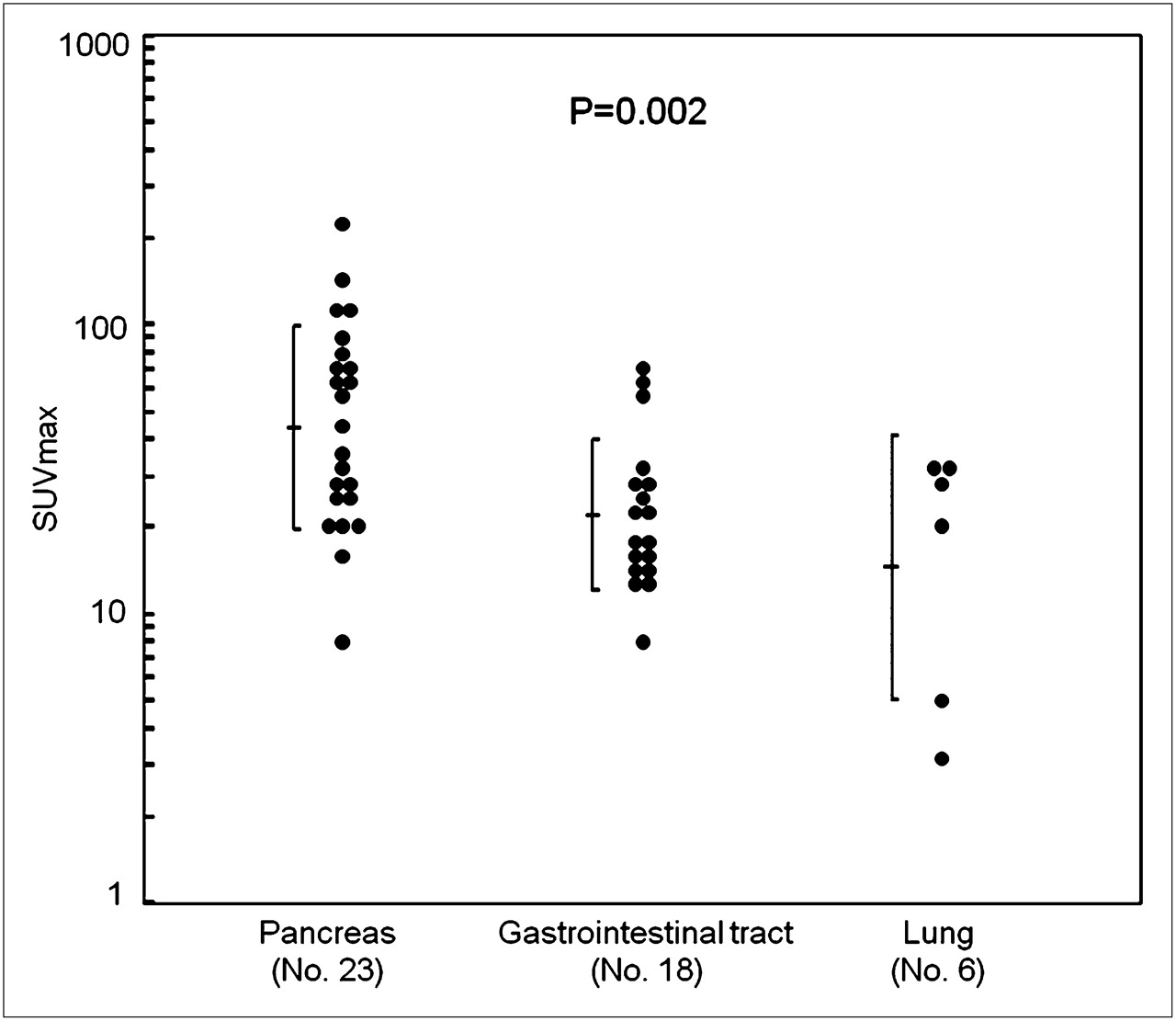
Distribution of SUVmax in 43 patients with NETs according to primary tumor site. Mean ± SD values are also shown. Significant value among 3 groups was calculated by ANOVA.
We also found no significant differences in the mean values of the SUVmax between functioning NETs and nonfunctioning tumors (P = 0.214) and between patients with and those without multiple endocrine neoplasia type 1 syndrome (P = 0.370). Furthermore, the SUVmax did not correlate with the stage of the disease (P = 0.217).
Regarding the pathology of the disease, SUVmax was significantly higher in patients with well-differentiated neuroendocrine carcinomas than with poorly differentiated carcinomas (P = 0.036), whereas no correlation was found between the SUVmax and the Ki67 (P = 0.842).
Finally, the SUVmax was significantly higher in patients with a high expression of SSTR2A than with a low SSTR2A expression.
Follow-up
Forty-four of the 47 patients were evaluated for a mean period of 11.1 mo (range, 2–24 mo); 2 patients were lost at follow-up, and 1 patient underwent radical surgery. Twenty-four of the 44 patients were treated with long-acting somatostatin analogs (Sandostatin LAR [30 mg] every 28 d or Lanreotide Autogel [120 mg] every 28 d), and 19 had a combined treatment with both long-acting somatostatin analogs and peptide receptor radionuclide therapy (PRRT). One patient with an insulinoma refused any treatment during the follow-up period.
During the follow-up, 25 patients (56.8%) had stable disease or a PR (mean, 12.4 mo; range, 3–24 mo); in 19 (43.2%), the disease progressed (mean, 9.3 mo; range, 2–18 mo). The mean time to disease progression was 15.7 mo (95% CI, 13.2–18.3 mo) (Fig. 3), and the probability of stable disease or a PR at 6 and 12 mo was 85.6% ± 5.4% and 52.3% ± 8.6%, respectively
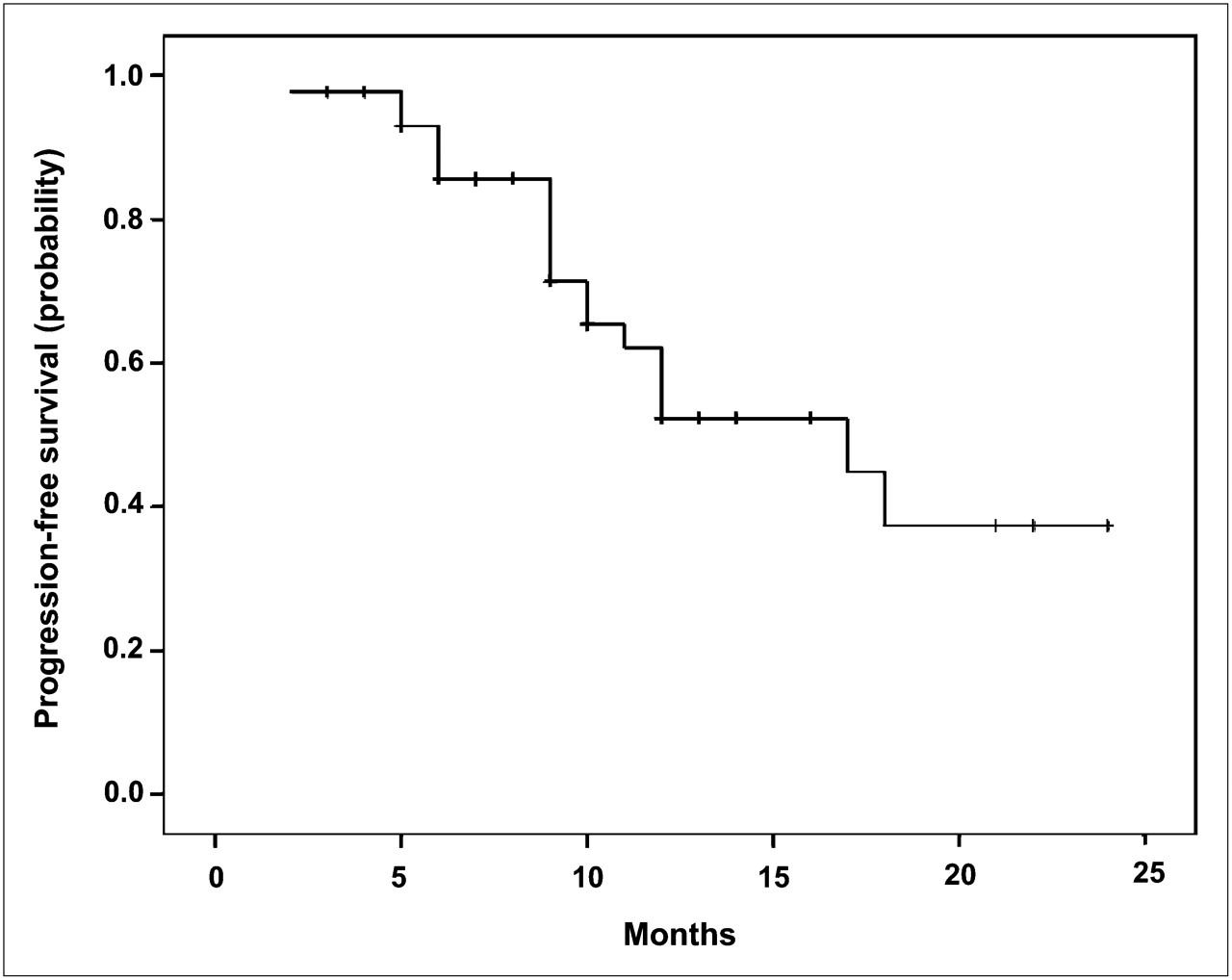
Plot of Kaplan–Meier estimates for progression-free survival among 44 patients with NETs. Mean time until disease progression was 15.7 mo (95% CI, 13.2–18.3 mo), and probability of stable disease or PR at 6 and 12 mo was 85.6% ± 5.4% and 52.3% ± 8.6%, respectively.
As reported in Table 1, the patients with stable disease or a PR had an SUVmax significantly higher than did the PD group (P = 0.001).
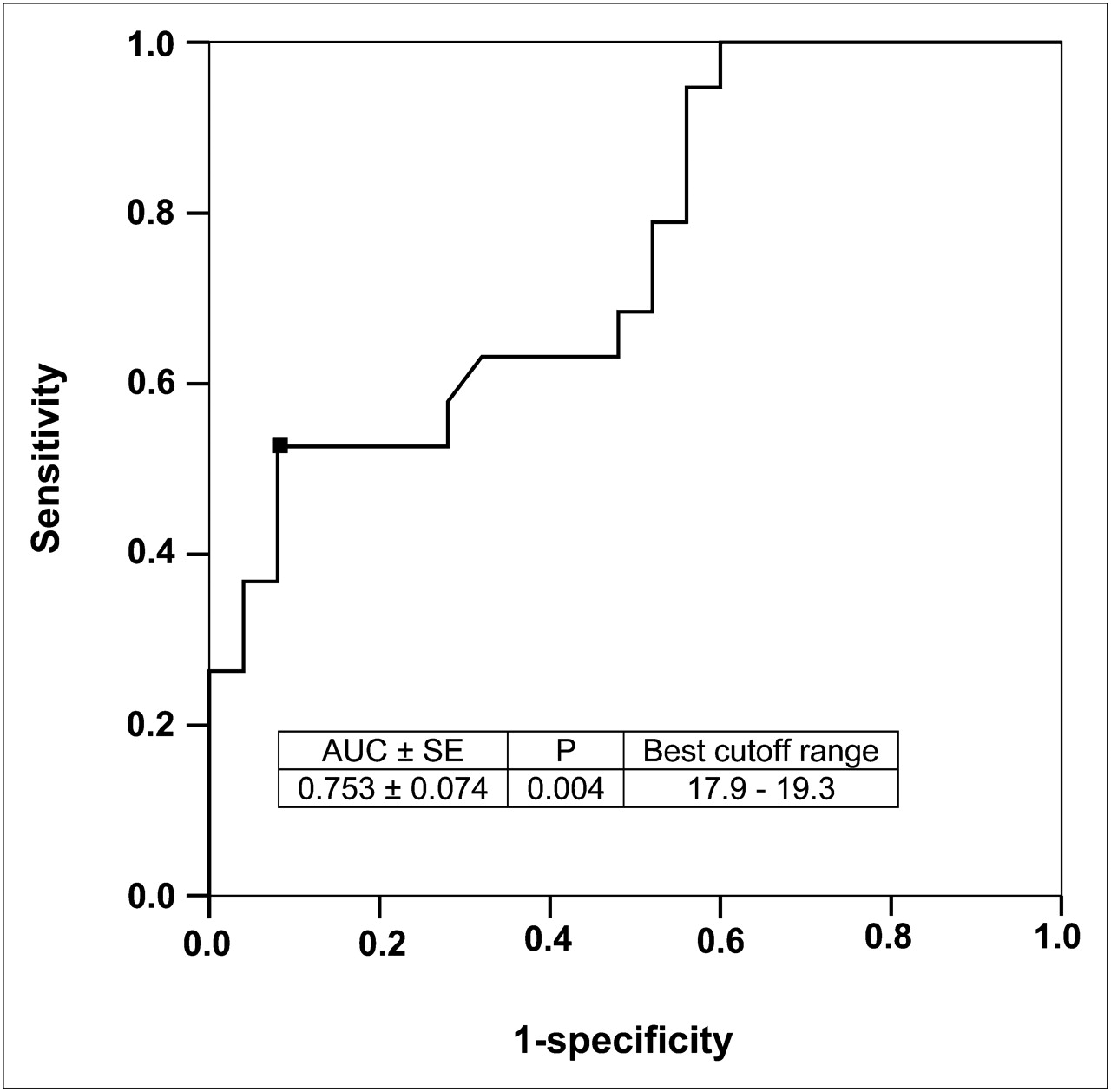
The receiver-operating-characteristic curve of the SUVmax in predicting patients who had PD is shown in Figure 4. The SUVmax was quite accurate (area under the curve ± SE, 0.753 ± 0.074; P = 0.004), and the best cutoff ranged from 17.9 to 19.3. The sensitivity and specificity obtained using the best cutoff values were 52.6% (10/19) and 92.0% (23/25), respectively.

Receiver-operating-characteristic curve of SUVmax in predicting patients who had PD. Sensitivity and specificity obtained using best cutoff were 52.6% (10/19) and 92.0% (23/25), respectively. AUC = area under the curve.
Prognostic Factors
The putative prognostic factors on time to progression evaluated in 44 patients are shown in Table 2. At univariate analysis, the significant positive prognostic factors were the following: well-differentiated NET (P = 0.002), SUVmax of at least 19.3 (P < 0.001; Fig. 5), and a combined treatment with long-acting somatostatin analogs and radiolabeled somatostatin analogs (P = 0.011; Fig. 6). These 3 prognostic factors, previously identified at univariate analysis, were also confirmed at multivariate analysis. In addition, the stage of the disease entered the procedure, with a P value near statistical significance (P = 0.052).

Plot of Kaplan–Meier estimates for progression-free survival among 44 patients with NETs according to SUVmax (SUVmax ≥ 19.3, SUVmax ≤ 17.6; P < 0.001, Mantel–Cox test).
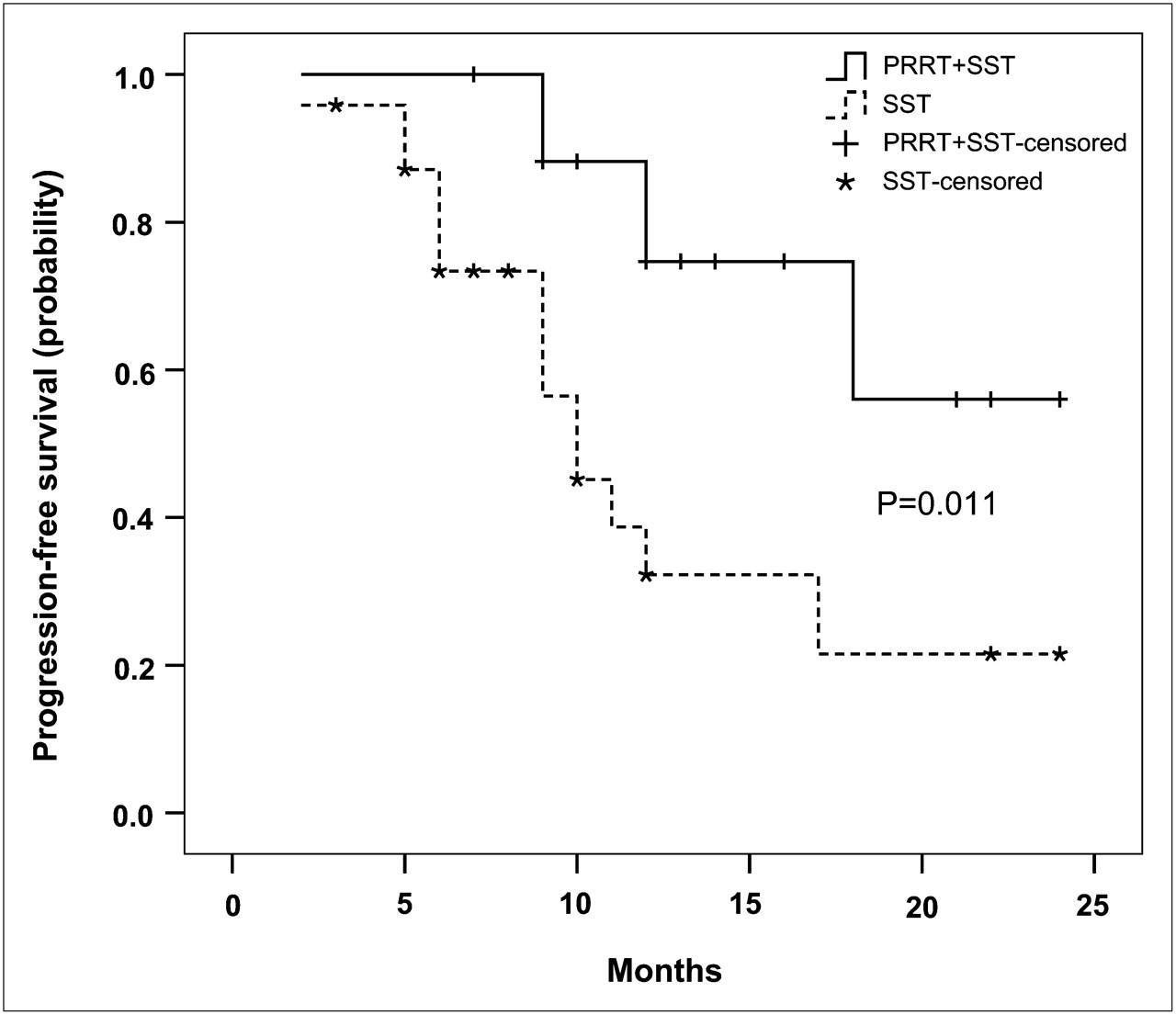
Plot of Kaplan–Meier estimates for progression-free survival among 43 patients (1 patient without therapy was excluded) with NETs according to treatment. P = 0.011, Mantel–Cox test. SST = somatostatin analogs; PRRT = radiolabeled therapy.
Effect of Various Clinical, Radiologic, and Histologic Findings on Progression-Free Survival in 44 Patients with Endocrine Tumors
DISCUSSION
68Ga-DOTA-peptide PET is a technique for the visualization, initial staging, and detection of recurrent disease and for planning radiolabeled therapy in NETs (22).
In the last few years, several authors have compared 68Ga-DOTA-peptide PET with the other imaging techniques usually used in NET patients—such as Octreoscan, CT, and MRI—and they evaluated the sensitivity and specificity of these imaging modalities (10,11).
However, only recently have researchers directed their attention to the evaluation of the SUVmax measured on PET scans. In particular, Miederer et al. (23) correlated the SUVmax with the cell membrane–based SSTR2 immunohistochemistry score in 17 patients with NETs and found a significant correlation between membranous SSTR2 expression determined by immunohistochemistry and tumor uptake of the SSTR2 analog 68Ga-DOTATOC expressed as SUV.
In the present article, we evaluated the SUVmax measured on the 68Ga-DOTANOC PET scan in a group of patients with NETs to correlate this quantitative value with the clinical findings, immunohistochemical findings, and time to progression of the disease during follow-up.
First, we found that the SUVmax was significantly higher in patients with pancreatic NETs than in those with gastrointestinal or lung NETs. This finding was in agreement with what had recently been reported by O'Toole et al. (24). The authors found a higher messenger RNA level expression of SSTR2 and SSTR5 in pancreatic than in gastrointestinal NETs. In fact, 68Ga-DOTANOC was reported to present a high affinity for SSTR2, SSTR3, and SSTR5 (12,13).
Data on the SSTR2A expression at immunohistochemical staining were available in a subgroup of patients (14). In cases presenting a higher score of SSTR2A, we also observed a statistically significant higher SUVmax. This finding is reinforced by the report of Asnacios et al. (25), who pointed out a significant correlation between the immunohistochemical positivity for SSTR2 and the positivity at Octreoscan. These results suggest the possibility of using a quantitative variable, such as the SUVmax, instead of a qualitative one, such as Octreoscan.
In our series, the SUVmax was higher in patients with functioning NETs than in those with nonfunctioning endocrine tumors. Up to now, these data have been controversial; some authors have reported a low expression of SSTRs in nonfunctioning endocrine tumors (26), whereas Jais et al. did not observe any significant differences between functioning and nonfunctioning tumors (27). Our results were also in agreement with those already published by Ezziddin et al. (28), who found positive Octreoscan results more frequently in patients with functioning NETs than in those with nonfunctioning lesions, although the results did not reach statistical significance. The observed higher expression of SSTR reflects the high differentiation of the functioning tumors.
We did not find a statistically significant correlation between SUVmax and different stages of disease at CT, possibly because of the high proportion of stage IV patients in our series. Moreover, SUVmax is useful for a better characterization of the tumor and not for the staging of it. In fact, regarding histologic findings, we reported a significantly higher SUVmax in patients with well-differentiated endocrine carcinomas than in those with poorly differentiated endocrine carcinomas. These data reflect how the expression of SSTR2, SSTR3, and SSTR5 correlates to the degree of differentiation of the neoplastic tissue, and they further confirm the previous results of Papotti et al. (29), who used immunohistochemical procedures, and Ezziddin et al. (28), who found this correlation using Octreoscan.
We also found a significantly higher SUVmax in patients with stable disease and in those with a PR at follow-up. The best cutoff for the differentiation between patients with stable disease or a PR at follow-up and patients with PD ranged from 17.6 to 19.3; values higher than 19.3 permitted the selection of patients with a slow disease progression.
We also demonstrated how the SUVmax correlated with time to progression at both univariate and multivariate analysis, and we found that an SUVmax of 19.3 or more could be considered an index of a better prognosis. This is a new finding because previously only Asnacios et al. (25) had stated that a positive Octreoscan result may select those patients with low disease progression.
Finally, we found that patients who underwent both somatostatin analog treatment and PRRT had a better prognosis than those who were treated with somatostatin analogs alone, confirming the positive role of PRRT in the treatment of chronic NETs (30).
CONCLUSION
We have demonstrated, for the first time to our knowledge, that the SUVmax, measured at 68Ga-DOTANOC PET, correlated with the clinical and pathologic features of NETs. In fact, we observed that the SUVmax was significantly higher in patients with pancreatic endocrine tumors and in those with well-differentiated carcinoma.
Regarding the correlation of time to progression, we can consider the SUVmax and the degree of differentiation to be important prognostic indices, even if our data have to be confirmed in future studies, possibly multicenter, based on a large series of patients.
Footnotes
-
COPYRIGHT © 2010 by the Society of Nuclear Medicine, Inc.
References
- Received for publication May 28, 2009.
- Accepted for publication December 2, 2009.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- [18F]FDG PET/CT-Avid Discordant Volume as a Biomarker in Patients with Gastroenteropancreatic Neuroendocrine Neoplasms: A Multicenter Study
- High Tumor Uptake on 18F-FDOPA PET/CT Indicates Poor Prognosis in Patients with Metastatic Midgut Neuroendocrine Tumors: A Study from the Groupe detude des Tumeurs Endocrines and ENDOCAN-RENATEN Network
- 68Ga-DOTATATE PET in Restaging and Response to Therapy in Neuroblastoma: A Case Series and a Mini Review
- 68Ga-DOTATATE PET in Restaging and Response to Therapy in Neuroblastoma: A Case Series and a Mini Review
- Prognostic Value of Whole-Body PET Volumetric Parameters Extracted from 68Ga-DOTATOC PET/CT in Well-Differentiated Neuroendocrine Tumors
- Semiautomatic Tumor Delineation for Evaluation of 64Cu-DOTATATE PET/CT in Patients with Neuroendocrine Neoplasms: Prognostication Based on Lowest Lesion Uptake and Total Tumor Volume
- Quantitative 68Ga-DOTATATE PET/CT Parameters for the Prediction of Therapy Response in Patients with Progressive Metastatic Neuroendocrine Tumors Treated with 177Lu-DOTATATE
- Somatostatin Receptor Imaging and Theranostics: Current Practice and Future Prospects
- 64Cu-DOTATATE PET/CT and Prediction of Overall and Progression-Free Survival in Patients with Neuroendocrine Neoplasms
- Current Concepts in 68Ga-DOTATATE Imaging of Neuroendocrine Neoplasms: Interpretation, Biodistribution, Dosimetry, and Molecular Strategies
- Comparison of the Impact of 68Ga-DOTATATE and 18F-FDG PET/CT on Clinical Management in Patients with Neuroendocrine Tumors
- The Impact of 68Ga-DOTATATE PET/CT Imaging on Management of Patients with Neuroendocrine Tumors: Experience from a National Referral Center in the United Kingdom
- Prognostic Value of 68Ga-DOTANOC PET/CT SUVmax in Patients with Neuroendocrine Tumors of the Pancreas
- 64Cu-DOTATATE PET for Neuroendocrine Tumors: A Prospective Head-to-Head Comparison with 111In-DTPA-Octreotide in 112 Patients
- Quantitative and Qualitative Intrapatient Comparison of 68Ga-DOTATOC and 68Ga-DOTATATE: Net Uptake Rate for Accurate Quantification
- Unexpected Sensitivity of sst2 Antagonists to N-Terminal Radiometal Modifications
- Radiopeptide Imaging and Therapy in Europe
- Incidence of Increased 68Ga-DOTANOC Uptake in the Pancreatic Head in a Large Series of Extrapancreatic NET Patients Studied with Sequential PET/CT
- Volume-of-Interest Assessment of Oncologic Response Using 18F-FDG PET/CT: A Phantom Study