


Abstract
Acute allograft rejection remains a major complication after liver transplantation. We report a semiquantitative imaging method of detecting acute allograft rejection with 18F-FDG PET. Methods: Syngeneic and allogeneic transplanted rats, with or without immunosuppressive treatment, were subjected to serial PET. Autoradiography of the liver was conducted in both the syngeneic and the allogeneic rats. Results: A significant increment of 18F-FDG accumulation in liver allografts was observed by PET on day 2. The 18F-FDG signal was concentrated in the area where inflammatory cells around the vessels were detected by autoradiography. Allotransplanted rats treated with an immunosuppressive agent displayed a marked decrease in hepatic 18F-FDG uptake, compared with allotransplanted rats that were not treated. Conclusion: 18F-FDG PET may be a valid method for facilitating the development of protocols to diagnose graft rejection and to monitor the efficacy of immunosuppressive therapy.
Liver transplantation has become an effective therapy for patients with acute or chronic end-stage liver disease. Allograft rejection remains a major complication after transplantation, although tacrolimus-based immunosuppression has contributed to allograft survival (1,2). Liver biopsy is the gold standard routinely used to diagnose liver graft rejection and to monitor the efficacy of immunosuppressive therapy (3). However, this procedure is invasive and associated with some risk of morbidity and mortality, and rejection that is focal or patchy is subject to false-negative results because of the limited sampling site (3,4). Therefore, many attempts (5,6) have been made to develop noninvasive approaches to globally assess liver graft rejection, but none of these is in widespread clinical use.
18F-FDG is a glucose analog and is taken up by cells with increased metabolism such as cancer and activated immune cells. It is possible that 18F-FDG accumulates strongly in acute liver rejection. However, no studies have described 18F-FDG uptake under liver allotransplantation. 18F-FDG PET with an appropriate animal model is a useful approach to clarify whether 18F-FDG may enable noninvasive evaluation of acute liver rejection and immunosuppressive treatment efficacy. Thus, we performed 18F-FDG PET on rat models of orthotopic liver transplantation with or without treatment.
MATERIALS AND METHODS
Animals
Adult male Lewis rats (RT1l; Shizuoka Laboratory Animal Center) weighing 210–250 g were used as recipients, and Lewis or DA rats (RT1a; Shizuoka Laboratory Animal Center) of the same weight range, as donors. Orthotopic liver transplantation was performed (7). Tacrolimus (Astellas Pharma) was suspended in distilled water and injected intramuscularly from day 0 or 2 until day 8 once a day at a dose of 1 mg/kg of body weight. The animal experiments were approved by the Committee of Care and Use of Laboratory Animals of Fujita Health University and the National Institute of Radiologic Sciences.
18F-FDG PET
18F-FDG (37 MBq; Nihon Medi-Physics) was intravenously injected into liver-transplanted rats (nonfasting) under anesthesia. At 50 min after injection, a 10-min emission scan was started using a small-animal PET system (Inveon; Siemens Medical Solutions) under 1% isoflurane anesthesia. Images were reconstructed using filtered backprojection (a ramp filter with a cutoff frequency of 0.5) with attenuation correction. Tracer uptake was quantified as standardized uptake values (SUVs). Circular regions of interest (3.9 mm in diameter) were manually drawn on 3 parts of the liver in each rat, and the mean SUV in each region of interest was measured. The mean SUVs of each rat were independently used for statistical analysis. The data were expressed as mean ± SD and were analyzed by ANOVA with a Student-Newman-Keuls multiple-comparison test.
Autoradiography and Hematoxylin–Eosin Staining
After the PET scans, the rats were sacrificed, and the livers were removed and quickly frozen in an optimal-cutting-temperature compound. Dried sections (20 μm thick) were exposed to an imaging plate (Fuji Film) for 2 h. Sequential sections (5 μm thick) were stained with hematoxylin and eosin for histologic evaluation (8).
RESULTS
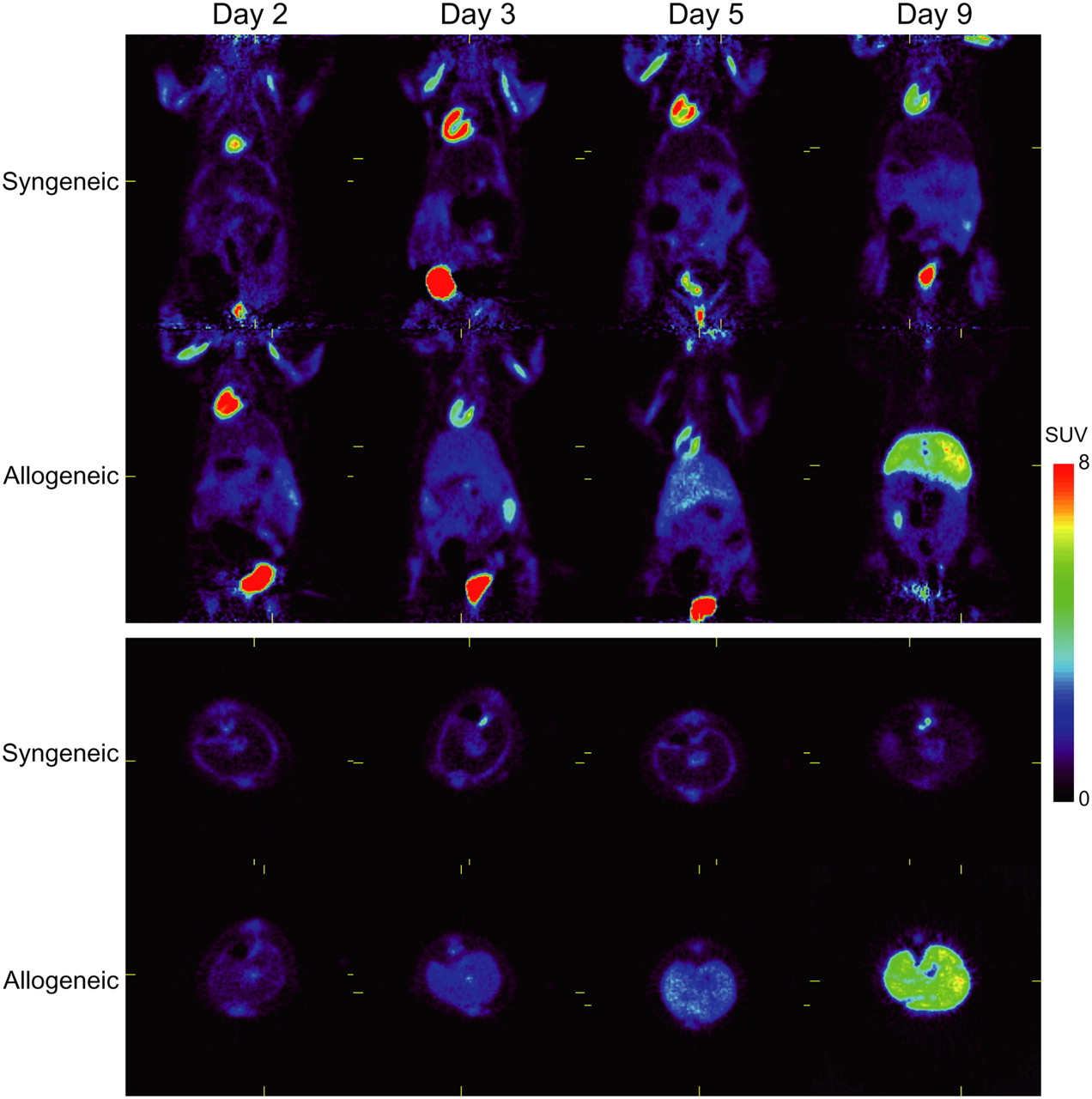
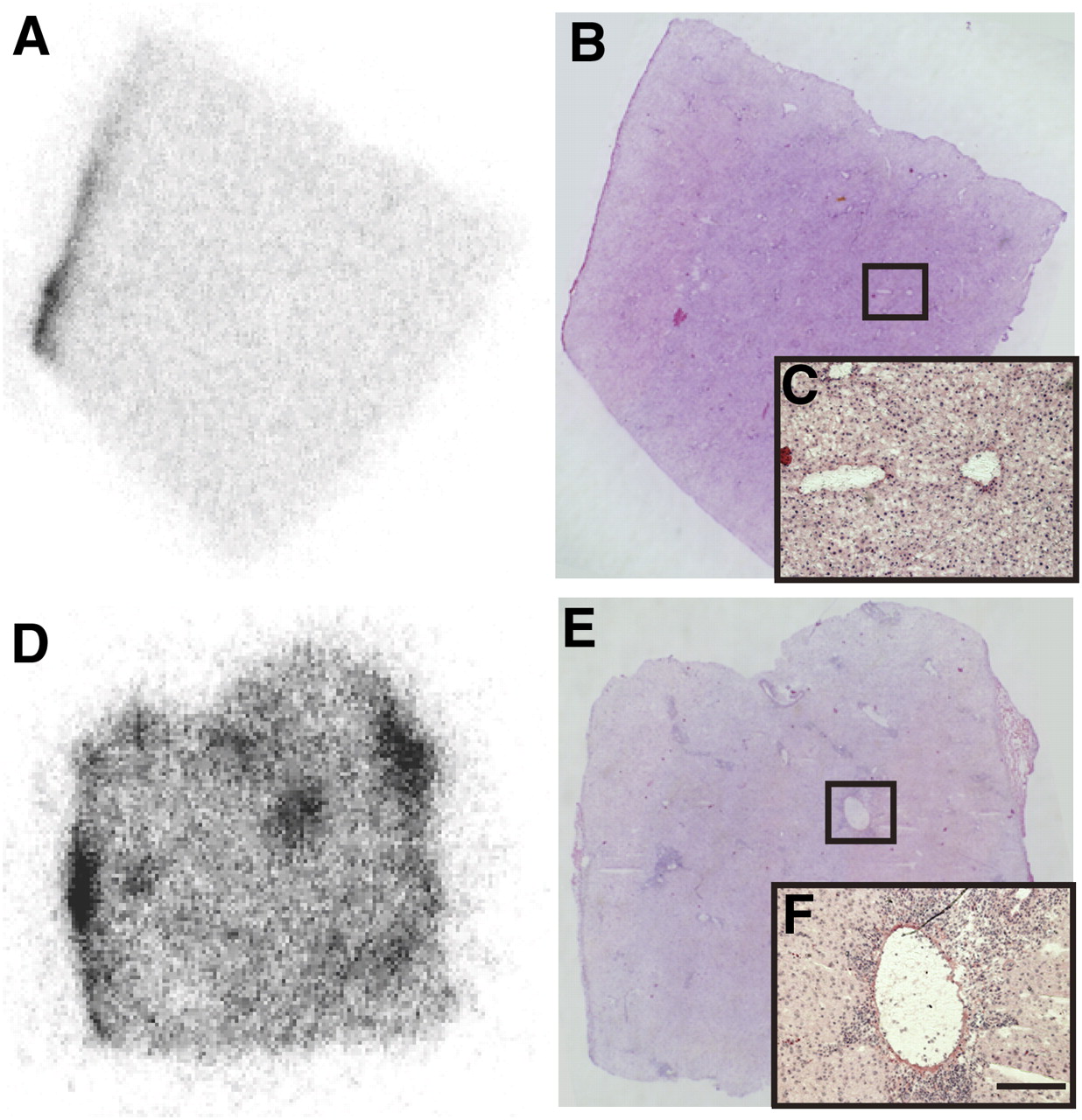
We first acquired 18F-FDG PET scans of syngeneic and allogeneic hepatic transplantation rats without immunosuppressive treatment (Fig. 1). Hepatic 18F-FDG uptake in syngeneic transplanted rats barely changed through the experiment, but that in allogeneic transplanted rats clearly increased with time (Fig. 1; Table 1). These PET results were confirmed by biodistribution experiments on a single rat at each time point (days 3, 5, 8, and 9; data not shown). On day 3, autoradiography of a syngeneic transplanted liver exhibited a faint and relatively homogeneous density distribution, whereas that of an allogeneic transplanted liver exhibited stronger and quite heterogeneous density distribution (Fig. 2). Corresponding hematoxylin and eosin staining revealed that an increased 18F-FDG signal was concentrated in the areas where inflammatory cells were abundant around the vessels (Fig. 2).

Serial 18F-FDG PET images of syngeneic and allogeneic (without treatment) liver transplantation rat models (upper, coronal; lower, transaxial).

Autoradiography (A and D) and hematoxylin and eosin staining (B, C, E, and F) of liver in syngeneic (A–C) and allogeneic (D–F) transplantation rats on day 3 after transplantation. Bar indicates 200 μm.
Mean Liver SUV in Syngeneic, Allogeneic, and Tacrolimus-Treated Allogeneic Hepatic Transplantation Rats
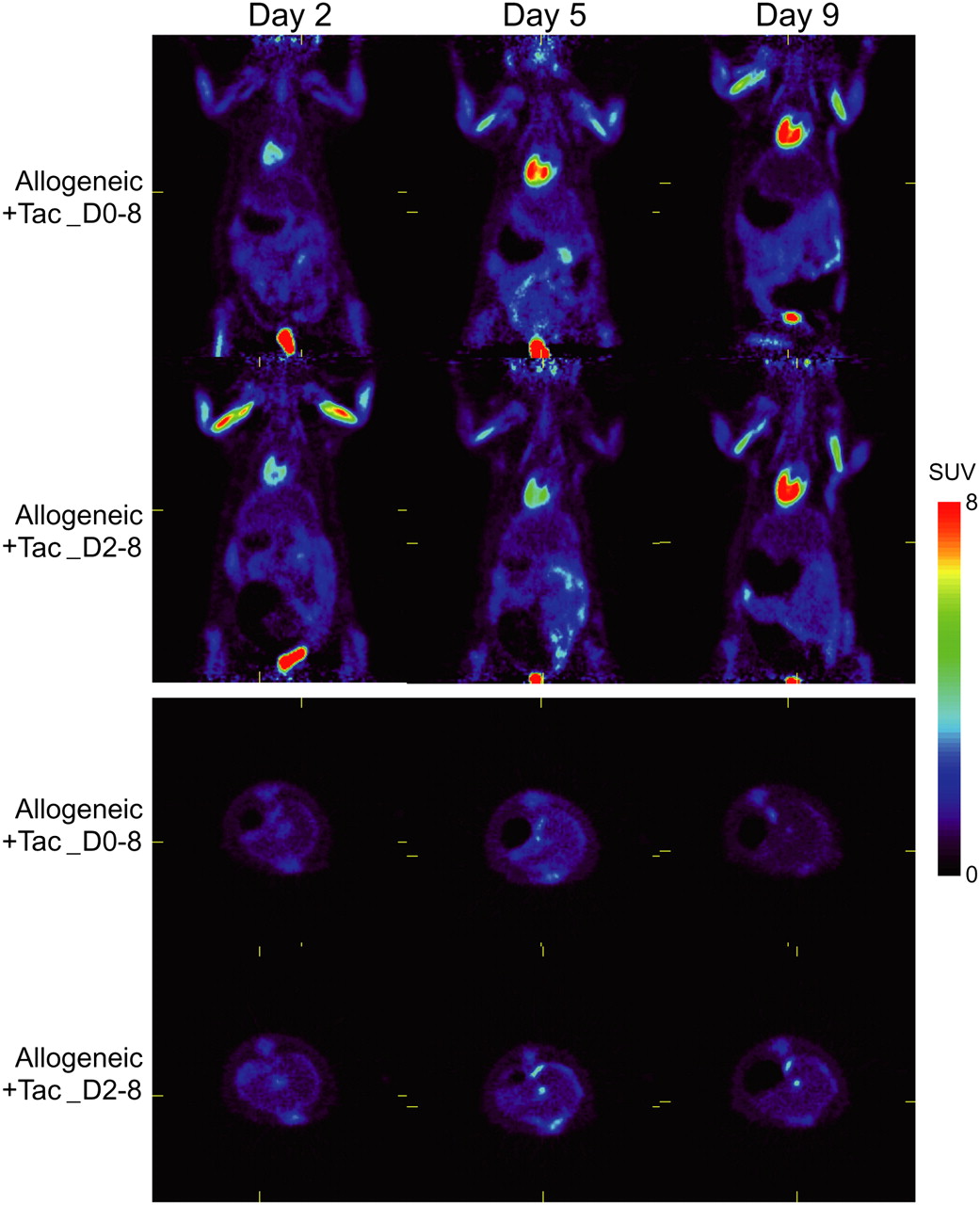
Next, we treated allogeneic transplanted rats with an immunosuppressive agent, tacrolimus, from day 0 or 2 through day 8, and we performed serial 18F-FDG PET on days 2, 5, and 9. Hepatic 18F-FDG uptake in tacrolimus-treated rats (both protocols) remained low and unchanged from days 2 to 9, similar to syngeneic transplanted rats (Fig. 3; Table 1). There were no statistically significant differences in hepatic uptake between the 2 protocols.

Serial 18F-FDG PET images of allotransplanted rats treated with tacrolimus from days 0 to 8 or from days 2 to 8 (upper, coronal; lower, transaxial).
DISCUSSION
The aim of this study was to determine whether 18F-FDG PET would prove useful in monitoring liver allograft rejection. Our results suggest that it does. First, 18F-FDG uptake in livers of syngeneic and allogeneic transplanted rats could be quantitatively evaluated by PET images. The mean SUV of liver allografts was significantly higher than that of syngeneic grafts as early as day 2 and markedly increased with time thereafter. This result is consistent with 18F-FDG uptake in a biodistribution study of skin transplant mouse models (9). Autoradiography and hematoxylin and eosin staining of allotransplanted liver indicated that the 18F-FDG signal was concentrated in inflammatory cells around the vessels. This result is consistent with 18F-FDG accumulation and localization in the liver of a mouse model of acute inflammation induced by concanavalin A (10). Our results suggest that 18F-FDG PET detects changes in glucose metabolism consistent with the presence of inflammatory infiltrates in liver allografts and provides an early and accurate diagnosis of allograft rejection in rat models. Second, hepatic 18F-FDG uptake in allogeneic transplanted rats treated with tacrolimus remained low and stable during treatments. These results suggest that 18F-FDG PET can be used to monitor the efficacy of immunosuppressive treatment as a noninvasive method, in contrast to biopsy.
There are 2 potential problems in applying 18F-FDG PET to the clinical setting: hepatic 18F-FDG uptake in humans is higher than in rats, and 18F-FDG accumulates in transplanted liver not only with acute rejection but also with inflammation due to other causes in an immunocompromised condition. Hepatic 18F-FDG uptake in humans is moderately high and could cause a high background level that would decrease the quality of the detection or diagnosis of acute rejection and monitoring of the efficacy of immunosuppressive treatment. However, our results clearly demonstrated that 18F-FDG accumulates strongly in acute allograft rejection of liver transplantation rats. Although we need to conduct a clinical study, SUV measurement may overcome this problem. The second problem inevitably impairs specificity in diagnosing acute rejection. However, high 18F-FDG accumulation in transplanted livers could indicate the need to explore the nature of the abnormality and proceed to appropriate treatment. 18F-FDG PET/CT can be used to determine the appropriate location for hepatic biopsy in patients with suspected acute rejection. Furthermore, monitoring treatment efficacy by 18F-FDG PET may yield important information for the management of patients.
CONCLUSION
The present investigation suggests that 18F-FDG PET could be useful for evaluating acute rejection of hepatic transplants and the efficacy of immunosuppressive treatment.
Acknowledgments
We acknowledge Drs. Megumu Miyamoto, Shiro Takahara, Shizuko Nagao, and Yoshikazu Kurosawa for comments and discussion. We also thank Dr. Chie Toramatsu for advice and help with PET imaging, and Ms. Yuriko Ogawa for technical assistance. This study was supported by research grants from the Ministry of Education, Culture, Sports, Science and Technology of Japan (17390355 and 20390349) and from the Ministry of Health, Labor and Welfare of Japan (HS KHC1025).
Footnotes
-
↵* Contributed equally to this work.
-
COPYRIGHT © 2009 by the Society of Nuclear Medicine, Inc.
References
- Received for publication October 10, 2008.
- Accepted for publication January 6, 2009.





{kind=link}
{kind=link}
{kind=link}