


Abstract
The aim of this study was to evaluate the role of radionuclide imaging in the characterization of nonhypersecreting adrenal masses. Methods: A total of 54 patients (19 men, 35 women; mean age, 50 ± 16 y) with nonhypersecreting unilateral adrenal tumors that had been originally detected on CT or MRI underwent adrenal scintigraphy using different radiotracers. None of the patients showed specific symptoms of adrenal hypersecretion. Screening tests for excess cortical and medullary products showed normal adrenal hormone levels. Radionuclide studies (n = 73) included 131I-norcholesterol (n = 24), 131I-metaiodobenzylguanidine (MIBG) (n = 23), and 18F-FDG PET (n = 26) scans. Results: Histology after surgery (n = 31) or adrenal biopsy (n = 23) was obtained. Adrenal lesions were represented by 19 adenomas, 4 cysts, 1 myelolipoma, 1 neurinoma, 2 ganglioneuromas, 5 pheochromocytomas, 4 pseudotumors, 6 carcinomas, 2 sarcomas, and 10 metastases (size range, 1.5- to 5-cm diameter; mean, 4.9 ± 3.1 cm). For norcholesterol imaging, diagnostic sensitivity, specificity, and accuracy were 100%, 71%, and 92%, respectively; the positive predictive value (PPV) of the norcholesterol scan to characterize an adrenal mass as an adenoma was 89%, whereas the corresponding negative predictive value (NPV) to rule out this type of tumor was 100%. For MIBG imaging, diagnostic sensitivity, specificity, and accuracy were 100%, 94%, and 96%, respectively; the PPV of the MIBG scan to characterize an adrenal mass as a medullary chromaffin tissue tumor was 83%, whereas the corresponding NPV to rule out this type of tumor was 100%. For FDG PET, diagnostic sensitivity, specificity, and accuracy were 100%, 100%, and 100%, respectively; the PPV of FDG PET to characterize an adrenal mass as a malignant tumor was 100%, whereas the corresponding NPV to rule it out was 100%. Furthermore, in 7 patients with malignant adrenal tumors, FDG whole-body scanning revealed extra-adrenal tumor sites (n = 29), allowing an accurate diagnosis of the disease’s stage using a single-imaging technique. Conclusion: In patients with nonhypersecreting adrenal masses, radionuclide adrenal imaging, using specific radiopharmaceuticals such as norcholesterol, MIBG, and FDG, may provide significant functional information for tissue characterization. Norcholesterol and MIBG scans are able to detect benign tumors such as adenoma and pheochromocytoma, respectively. Conversely, FDG PET allows for recognition of malignant adrenal lesions. Therefore, adrenal scintigraphy is recommended for tumor diagnosis and, hence, for appropriate treatment planning, particularly when CT or MRI findings are inconclusive for lesion characterization.
The high resolution of anatomic imaging techniques such as CT and MRI, used in patients with suspected abdominal disease, frequently results in detection of unexpected adrenal masses (1–3). In this setting, the main clinical concern consists of noninvasive characterization of benign and malignant adrenal lesions to determine the appropriate treatment (1–3). As an initial diagnostic approach, clinical and laboratory assessment of cortical and medullary adrenal function can identify hypersecreting adrenal lesions and, hence, the characterization of such tumors (4). However, a tumor mass may not cause adrenal hyperfunction because it may be nonhypersecreting or secretes inactive products (1–3). In such conditions, lesion identification remains uncertain. CT and MRI accurately provide anatomic details of adrenal tumors and may suggest the nature of such lesions (5,6). Radionuclide adrenal imaging performed with specifically labeled radiopharmaceuticals that target elements of adrenal function may provide specific metabolic information for lesion characterization, thus complementing morphological imaging modalities (7).
Several radiotracers that display unique biological behavior may be used in nuclear medicine for adrenal tumor evaluation. These tracers include labeled norcholesterol for cortical adenomas (5), metaiodobenzylguanidine (MIBG) (5) and hydroxyephedrine (8) for medullary chromaffin tissue lesions, including pheochromocytomas and ganglioneuromas, and 18F-FDG (9) and 67Ga (10) for malignant tumors. Recently, molecular engineering has led to the synthesis of peptides of variable forms and sizes for tumor imaging (11). In particular, radiolabeled somatostatin analogs have been proposed in the diagnostic evaluation of several tumors (12). Among these, malignant adrenal masses showed significant uptake of somatostatin analog, suggesting the presence of somatostatin receptors (13).
In this study, we report our experience with the role of radionuclide imaging using various radiotracers in the diagnostic evaluation of patients with unilateral nonhypersecreting adrenal masses to obtain lesion characterization.
MATERIALS AND METHODS
Patient Population
From January 1992 to March 1999, 54 consecutive patients (19 men, 35 women; mean age, 50 ± 16 y) with nonhypersecreting unilateral adrenal masses detected on CT or MRI studies underwent adrenal scintigraphy using different radiopharmaceuticals. A total of 73 adrenal radionuclide studies were analyzed, including 131I-norcholesterol scintigraphy (n = 24), 131I-MIBG imaging (n = 23), and FDG PET (n = 26).
In the patients included in this study, nonhypersecreting adrenal tumors had been discovered during CT or MRI scanning performed for the diagnostic evaluation of unrelated conditions. These patients underwent CT or MRI for the diagnostic evaluation of abdominal pain (n = 23), abdominal trauma (n = 1), arterial hypertension (n = 6), biliary tract stone disease (n = 1), renal cysts (n = 6), anemia (n = 2), and anuria (n = 1), or during the staging (n = 4), or follow-up (n = 10) for malignant tumors. In particular, in the 6 patients with arterial hypertension, the presence of this abnormality was not considered as an exclusion criterion because hypertension may frequently also occur in different endocrine or coexisting nonendocrine diseases. None of the patients showed other symptoms of adrenal hypersecretion. Informed consent was obtained from all patients, filling a requirement of the protocol approved by the Institutional Clinical Research Subpanel on Human Studies at Istituto Nazionale dei Tumori.
Laboratory Analysis
Evaluation of adrenal function consisted of screening tests for excess mineralocorticoid, glucocorticoid, androgen, and catecholamine secretion. In particular, plasma aldosterone levels and renin activity were measured for patients in clinostatic and orthostatic posture. Plasma cortisol and corticotropin levels were measured at 8:00 am and 11:00 pm and a 24-h urine assay for free cortisol was performed. Measurements of serum dehydroepiandrosterone sulfate, 17α-hydroxyprogesterone, androstenedione, testosterone, and electrolyte levels were included. An overnight low-dose dexamethasone suppression test was also performed (1 mg orally at 11:00 pm; measurement of serum cortisol level at 8:00 am the following morning). Plasma catecholamine levels were measured in 24-h urinary excretion of catecholamines and their metabolites, vanillylmandelic acid and metanephrine, to evaluate medullary adrenal function.
Hormonal values were determined by radioimmunoassay or immunoradiometric assay methods using commercially available kits (CIS Bio International, Clichy Cedex, France/Mallinckrodt Medical B.V., Petten, The Netherlands/Roche Diagnostic, Italy). Urinary catecholamine, vanillylmandelic acid, and metanephrine levels were measured using high-performance liquid chromatography. Sodium and potassium levels were assessed using flame photometry with lithium as an internal standard.
Norcholesterol Imaging
Before norcholesterol injection, thyroid iodine uptake was blocked with a saturated solution of potassium iodide (200 mg/d orally, starting the day before tracer administration and continuing for 8 d). Intravenous injection of 37 MBq 131I-norcholesterol (CIS Bio International, Cedex, France) was administered. Early and delayed adrenal scintigraphy were performed 5 and 7 d, respectively, after tracer injection using a large-field-of-view gamma camera (Orbiter; Siemens, Erlangen, Germany) with a high-energy collimator and a 20% window centered at 364 keV. Early and delayed posterior abdominal views were acquired. A mild laxative (bisacodyl) was given (10 mg) 2 times daily beginning 2 d before the first day of imaging to reduce interfering colonic 131I activity. When required, norcholesterol adrenal scintigraphy was also performed with a concomitant dexamethasone suppression test. For this, 1 mg dexamethasone was administered 4 times daily for 7 d before norcholesterol injection and for 5 d after tracer injection.
MIBG Imaging
Before MIBG injection, thyroid iodine uptake was blocked with a saturated solution of potassium iodide (200 mg/d orally, starting before tracer administration and continuing for 8 d). 131I-MIBG (37 MBq; Amersham Sorin, Saluggia, Italy) was administered intravenously. Anterior and posterior whole-body as well as abdominal spot views were obtained at 24, 48, and 72 h after tracer injection using a large-field-of-view gamma camera (Siemens) with a high-energy collimator and a 20% window centered at 364 keV.
FDG PET
18F was produced by an MC-1704 cyclotron (Scanditronix, Uppsala, Sweden). 18F was transferred to an automated chemical processing unit for synthesis of 18F-FDG. For quality assurance, FDG production was tested for sterility, pyrogenicity, and radiochemical purity. PET imaging was performed using a whole-body PET EXACT 47 scanner (Siemens). Patients were studied in fasting conditions 4–6 h before FDG injection. Diabetic patients were not included in the study because high levels of glucose serum competitively inhibit FDG transport into malignant cells, potentially decreasing the ability to detect and characterize adrenal lesions. Patients were positioned in the PET gantry using a rectilinear scan computerized program that localized the superior abdomen. Before injection of FDG, abdominal transmission scanning using a rod source of 67Ge for the attenuation correction of the corresponding emission scans was performed for 20 min. Subsequently, patients were intravenously injected with 370 MBq FDG. Abdominal emission counts were acquired 30–45 min after FDG administration. Finally, whole-body images using 7 bed positions with an acquisition time of 5 min each were obtained within 1 h after tracer injection. No brain FDG activity was included in the whole-body PET scans. Images were reconstructed using filtered backprojection smoothed with a Hann filter with a cutoff frequency of 0.4 cycle/pixel on a Sun Workstation; 3-dimensional PET scans were generated as axial, coronal, and sagittal views.
Data Analysis
Adrenal function, either cortical or medullary, was considered to be healthy when corresponding hormone values were in the normal range. Conversely, cortical or medullary adrenal hypersecretion was determined in cases of clearly increased levels of the corresponding hormones.
The anatomic characteristics of adrenal tumors were assessed on CT and MR images. In particular, tumor size was measured as maximal diameter in centimeters. Lesion size was compared between adenomas, nonadenoma benign tumors, and malignant adrenal masses using the Student t test for unpaired data. Data were expressed as mean ± SD. P < 0.05 were considered significant.
The presence of abnormally increased uptake of norcholesterol, MIBG, or FDG was analyzed in adrenal regions where tumor lesions had been detected by CT or MRI. The intensity of tumor uptake was qualitatively evaluated on a high-resolution display by 2 independent and experienced nuclear medicine physicians. In case of disagreement, final interpretation was determined by consensus reading. Radionuclide studies were assessed independently without knowledge of clinical and pathologic findings. Adrenal activity was considered abnormal when tracer uptake was greater than initial blood-pool and surrounding background activity and when no similar uptake was observed on the contralateral side. The criteria proposed by Gross et al. (14) were used to interpret the norcholesterol study; the following uptake patterns were defined: increased tumor activity with no visualization of the contralateral gland (exclusive concordant uptake); prevalent tumor activity with visualization of the contralateral gland (prevalent concordant uptake); reduced tumor activity compared with the contralateral gland (reduced discordant uptake); and absent tumor activity (discordant no uptake).
Scintigraphic images were categorized as positive or negative. The results were classified as true-positive, true-negative, false-positive, and false-negative compared with final pathological findings. On the basis of the data reported in the literature (5,9), the criteria to establish true-positive radionuclide scans include the following: the norcholesterol study was considered true-positive in the presence of adenoma; MIBG scans were considered true-positive in the presence of medullary chromaffin tissue tumors such as pheochromocytoma or ganglioneuroma; and the FDG findings were true-positive in cases of malignant adrenal lesions. Diagnostic sensitivity, specificity, and accuracy, positive predictive values (PPVs), and negative predictive values (NPVs) were calculated for each radionuclide study (norcholesterol, MIBG, and FDG). The results of histology after surgery (n = 31) or adrenal biopsy (n = 23) were considered the standards of reference.
Whole-body scintigraphic images of MIBG and FDG were also qualitatively analyzed. Abnormal tracer uptake in extra-adrenal locations was assessed following the same criteria as those used to evaluate abdominal scans. When abnormal extra-adrenal foci of activity were identified, CT or MRI was performed to confirm or rule out the presence of tumor lesions. Because not all lesions could be evaluated by operative or histological proof in patients with extra-adrenal disease spread, the results of CT and MRI were considered the standards of reference.
RESULTS
Adrenal lesions were represented by 19 adenomas, 4 cysts, 1 myelolipoma, 1 neurinoma, 2 ganglioneuromas, 5 pheochromocytomas, 4 pseudotumors, 6 carcinomas, 2 sarcomas, and 10 metastases. Adrenal pseudotumors consisted of nodular liver hyperplasia, a fat tissue mass, a renal cyst, and a cystic lesion of the gastric wall.
The characteristics of individual adrenal lesions and the corresponding radionuclide imaging findings are reported in Tables 1 and 2 for benign and malignant tumors, respectively. In particular, the results of abdominal CT and MRI studies showed 34 and 20 well-capsulated tumor lesions of left and right adrenal glands, respectively. In all cases, the margins of adrenal masses were regular (size range, 1.5–15 cm; mean, 4.9 ± 3.1 cm), including adenomas (size range, 1.5–6 cm; mean, 2.6 ± 1.0 cm), benign nonadenoma lesions (size range, 2.5–13 cm; mean, 6.0 ± 2.6 cm), and malignant tumors (size range, 2–15 cm; mean, of 6.4 ± 3.7 cm). Whereas the size of adenomas was significantly (P < 0.001) smaller than that of other benign lesions as well as malignant tumors, no statistical difference in tumor size was observed between nonadenoma benign lesions and malignant adrenal masses. The results of radionuclide studies in terms of diagnostic sensitivity, specificity, and accuracy, as well as PPVs and NPVs, are illustrated in Table 3.
Characteristics and Radionuclide Imaging Results of Patients with Benign Adrenal Masses
Characteristics and Radionuclide Imaging Results of Patients with Malignant Adrenal Masses
Radionuclide Imaging Results
Norcholesterol Imaging
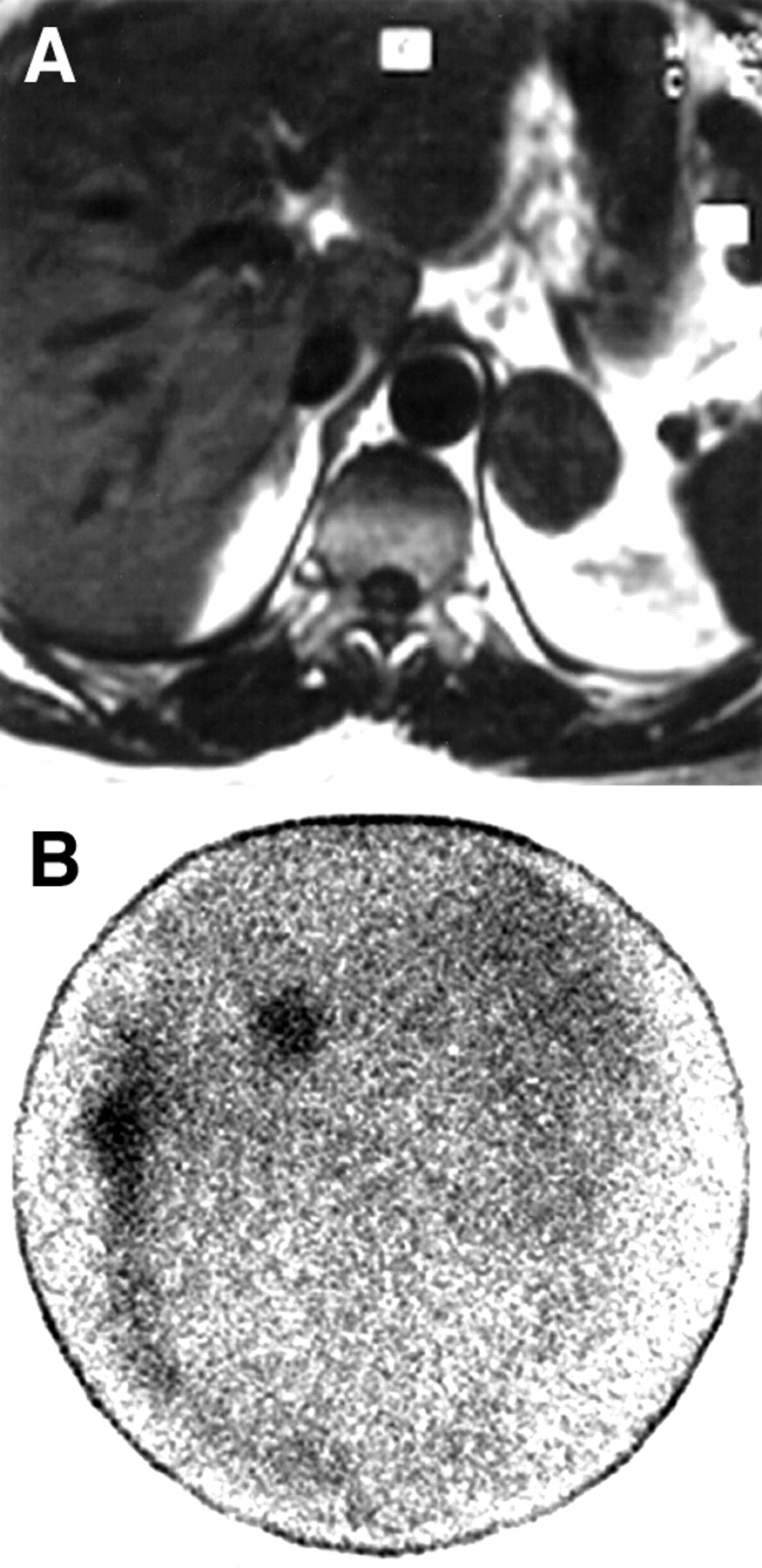
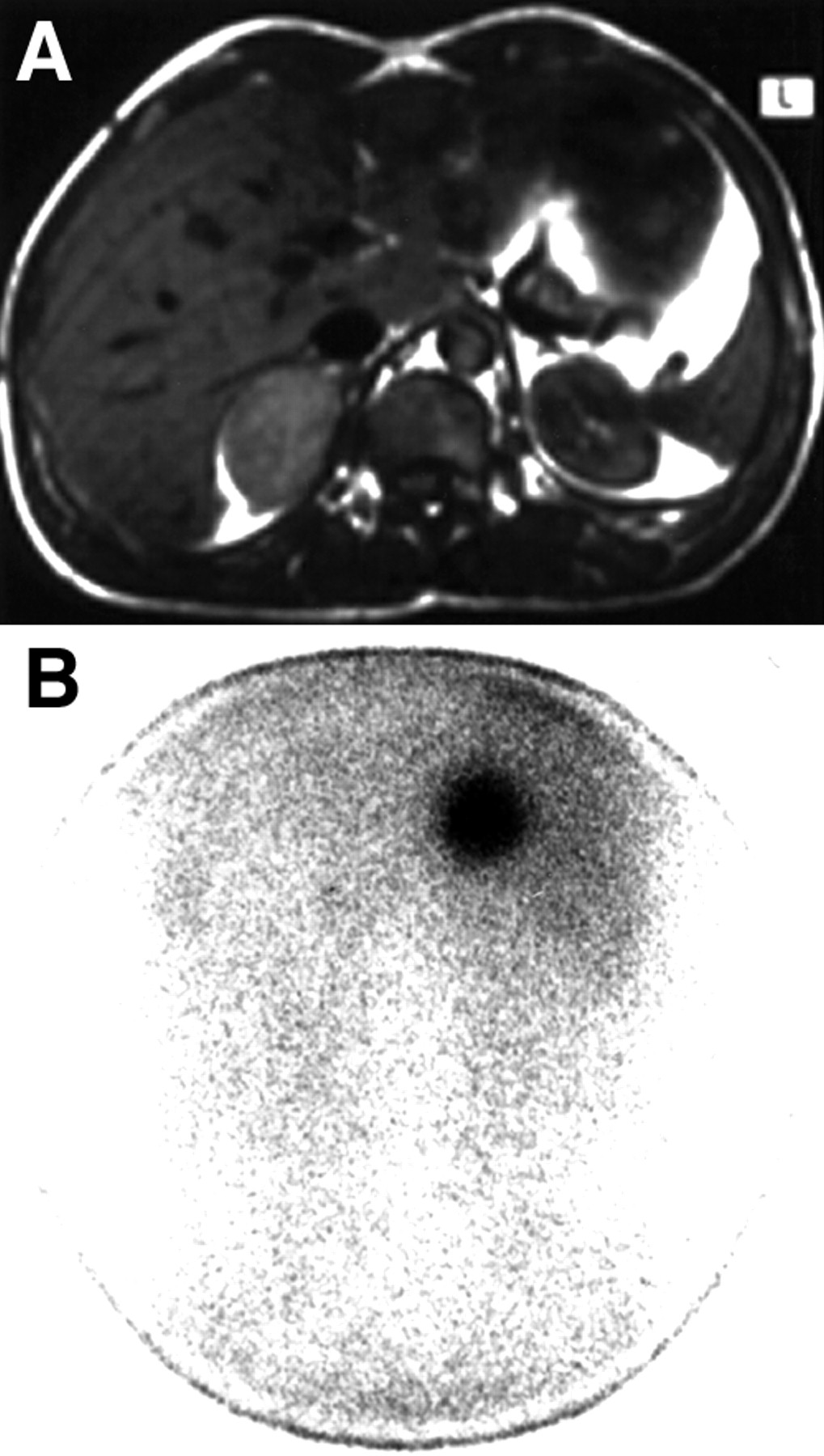
Of the 24 patients on whom these studies were performed, 17 had adenomas, 4 had nonadenoma benign lesions (1 pheochromocytoma, 2 cysts, and 1 myelolipoma), and 3 had malignant tumors (1 carcinoma and 2 metastases). Exclusive 131I-norcholesterol uptake (pattern 1) by adrenal lesions was observed in all patients with adenomas (true-positive results) (Fig. 1). However, as is not normally observed, diffuse tracer uptake was also found in 2 different adrenal lesions represented by a myelolipoma and a pheochromocytoma (2 false-positive results); these lesions showed prevalent (pattern 2) and reduced (pattern 3) uptake, respectively. The remaining 5 cases consisted of true-negative results with no activity in tumor masses (pattern 4). No false-negative findings were found. In particular, the PPV of norcholesterol imaging to characterize an adrenal mass as an adenoma was 89%; in contrast, the corresponding NPV to rule out this type of tumor was 100% (Table 3).
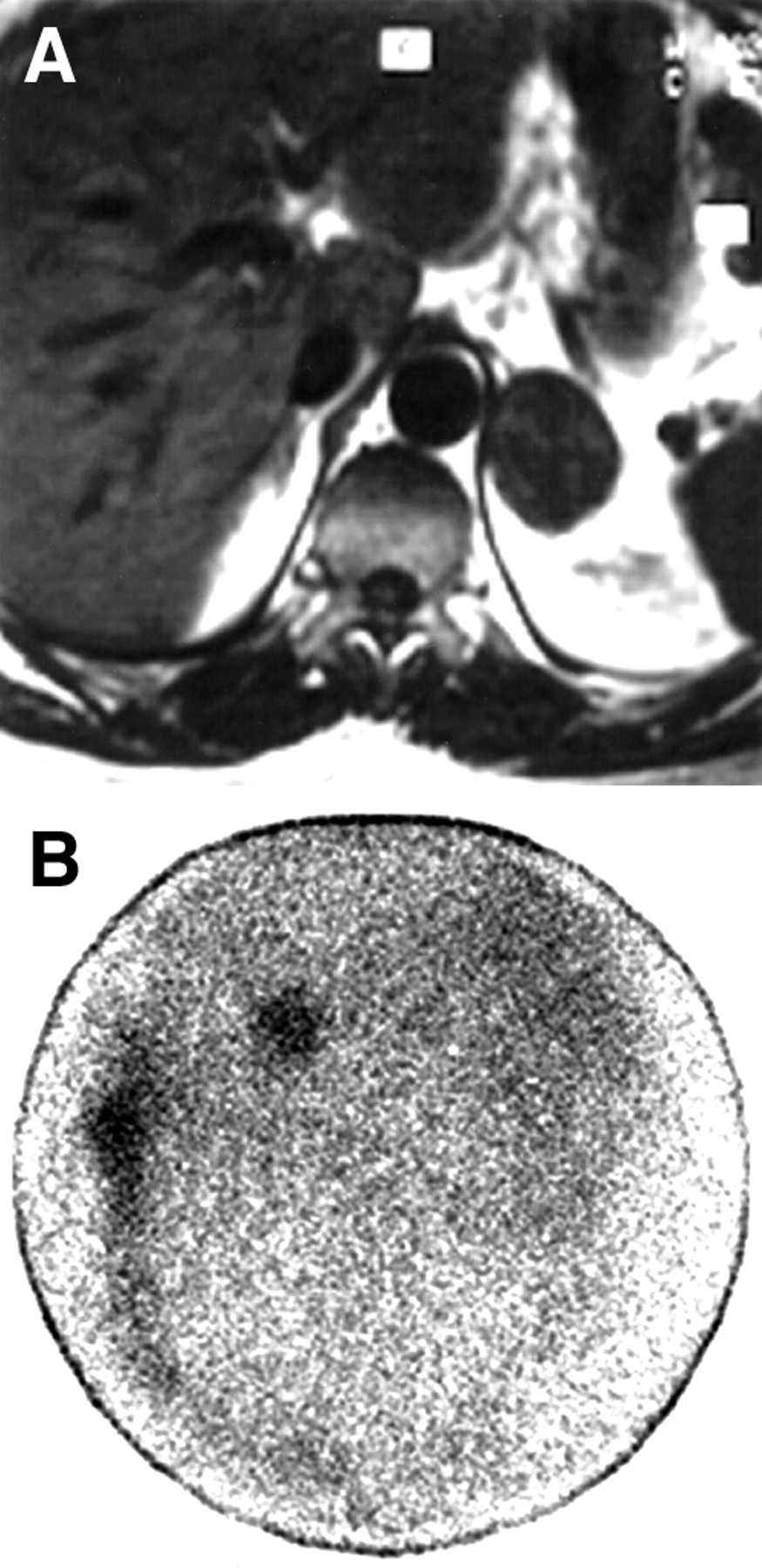
Patient with nonhypersecreting left adrenal adenoma. (A) T1-weighted (repetition time/echo time = 600/15) abdominal MR axial scan shows round left adrenal mass. (B) Abdominal posterior view of norcholesterol image shows round area of tracer uptake in left adrenal bed; diffuse physiologic activity is present in liver and through left bowel.
MIBG Imaging
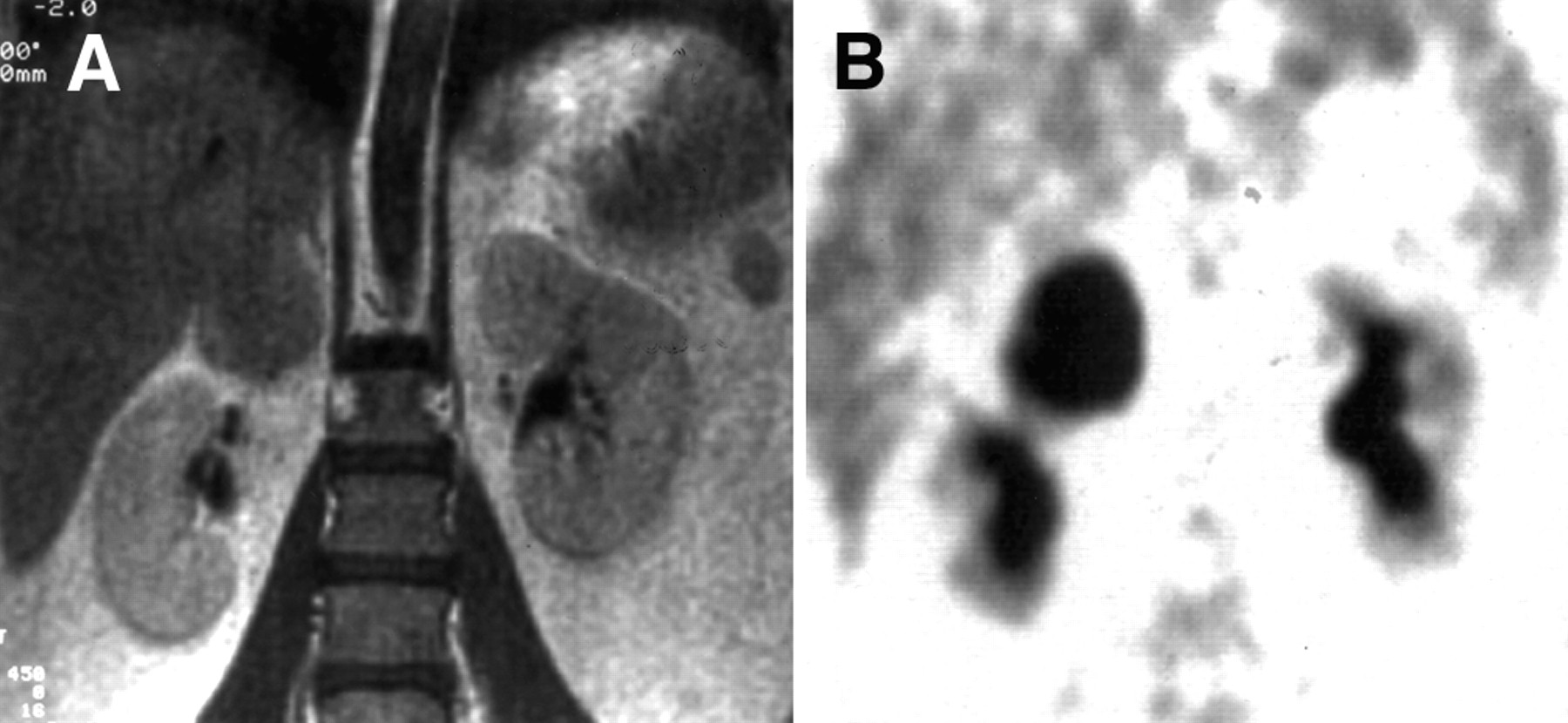
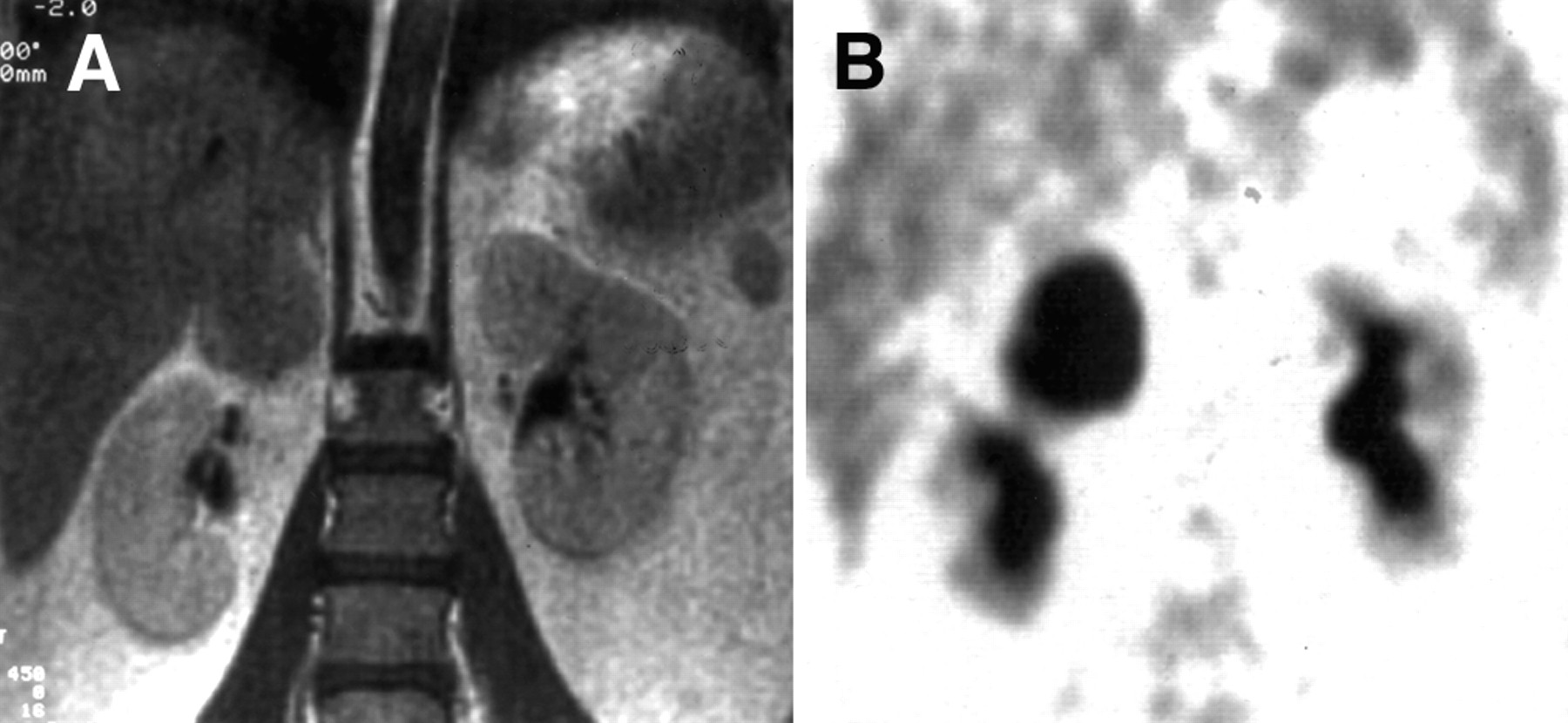
Of the 23 patients on whom these studies were performed, 10 had adenomas, 8 had nonadenoma benign lesions (4 pheochromocytomas, 1 ganglioneuroma, 2 cysts, and 1 pseudotumor), and 5 had malignant tumors (2 carcinomas, 1 sarcoma, and 2 metastases). Significantly increased 131I-MIBG uptake by adrenal lesions occurred in patients with a pheochromocytoma or a ganglioneuroma (true-positive results) (Fig. 2). Heterogeneous tracer activity was unexpectedly found in one instance of a large and necrotic cortical carcinoma (false-positive result). The PPV of MIBG imaging to characterize an adrenal mass as a medullary chromaffin tissue tumor was 83%; conversely, the corresponding NPV to rule out this type of tumor was 100% (Table 3). Whole-body MIBG images were normal in all cases.

Patient with nonhypersecreting right adrenal pheochromocytoma. (A) T1-weighted (repetition time/echo time = 600/15) abdominal MR axial scan shows round right adrenal mass. (B) Abdominal posterior view of MIBG image shows round area of intense tracer uptake in right adrenal bed.
FDG PET
Of the 26 patients on whom these studies were performed, 6 had adenomas, 7 had nonadenoma benign lesions (1 neurinoma, 1 ganglioneuroma, 1 cyst, 1 myelolipoma, and 3 pseudotumors), and 13 had malignant tumors (6 carcinomas, 1 sarcoma, and 6 metastases). No significant FDG uptake was observed in benign adrenal lesions (n = 13). Conversely, increased FDG uptake was observed in all patients with malignant adrenal tumors (Fig. 3). The PPV of FDG PET imaging to characterize an adrenal mass as a malignant tumor was 100%; the corresponding NPV to rule out this type of tumor was 100% (Table 3).
Patient with nonhypersecreting right adrenal carcinoma. (A) T1-weighted (repetition time/echo time = 600/15) abdominal MR coronal scan shows right adrenal mass. (B) Uncorrected abdominal coronal FDG PET scan shows intense tracer uptake by right adrenal lesion; significant physiologic activity is detectable in both renal pelves.
In 7 patients with malignant adrenal masses, 3 with carcinomas, and 4 with metastases, whole-body FDG PET showed a total of 29 foci of abnormal tracer uptake in extra-adrenal locations represented by chest (n = 6) and abdominal (n = 7) lymph nodes, as well as lung (n = 7), liver (n = 6), and pancreatic (n = 1) and skeletal (n = 2) tumor lesions, as documented by CT or MRI studies (Fig. 4).
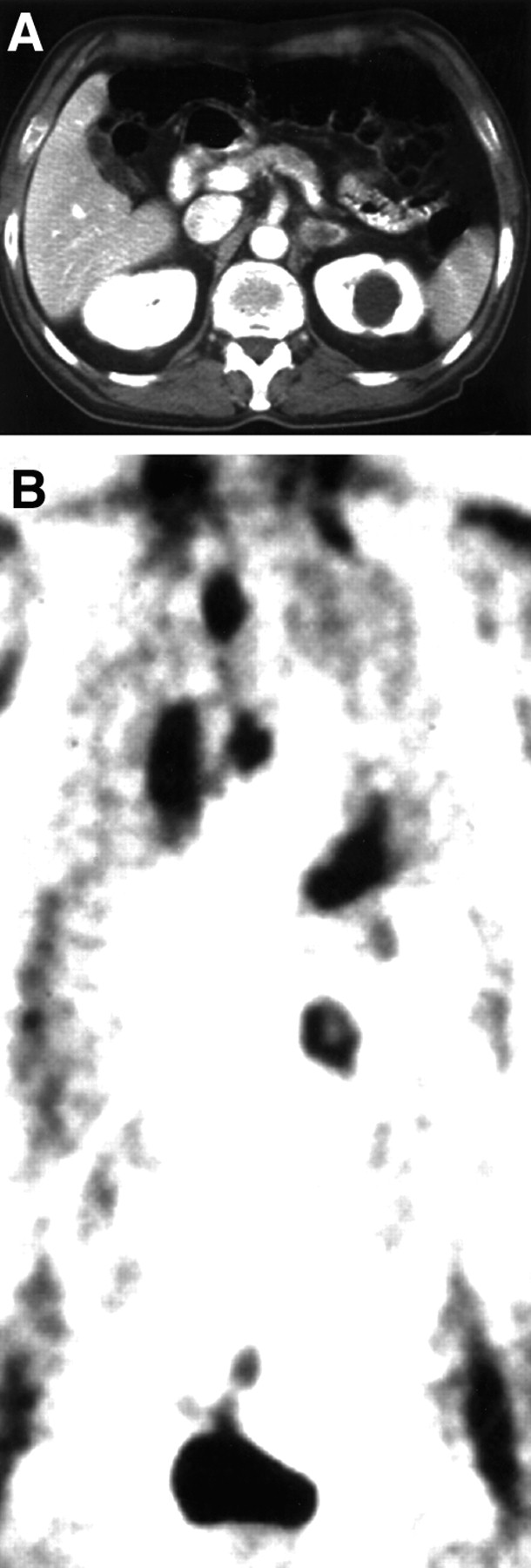
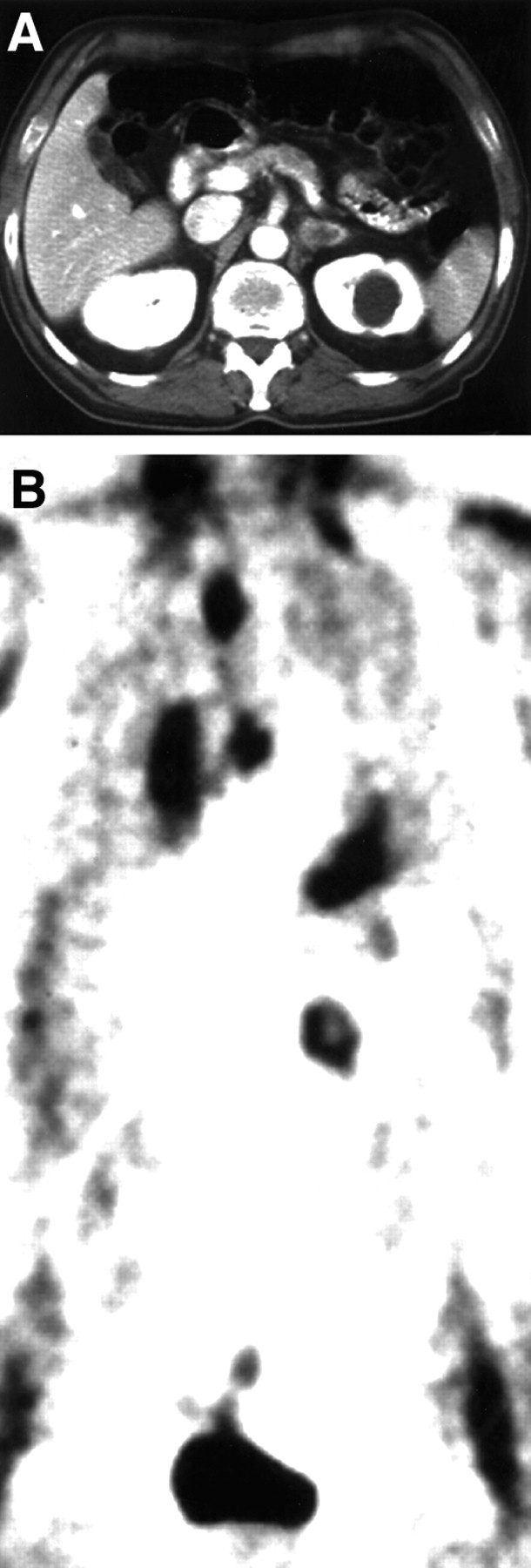
Patient with left adrenal metastasis from lung. (A) Postcontrast abdominal CT scan shows inhomogeneous left adrenal lesion. Round cystic lesion of left kidney is detectable. (B) Uncorrected whole-body FDG PET image shows abnormal increased tracer uptake by adrenal mass, primary lung tumor, and lymph nodal metastases of mediastinum; physiologic activity is present in heart as well as in neck and pelvic muscular tissues.
DISCUSSION
Image-based evidence of asymptomatic and nonhypersecreting adrenal masses has recently increased because of the widespread use of highly sensitive diagnostic techniques such as CT and MRI for the evaluation of abdominal complaints. For these patients, the most critical step is to identify the type of tumor to determine the appropriate treatment. Although anatomic criteria indicative of high risk of malignancy may be obtained using CT and MRI, radionuclide imaging using specific agents may provide in vivo tissue characterization of adrenal lesions to more clearly differentiate between benign and malignant abnormalities. Barzon et al. (15) recently proposed a morphofunctional examination by scintiscans using radioactive norcholesterol or MIBG for patients with incidentally discovered adrenal tumors.
In this study, we report our experience regarding the usefulness of adrenal scintigraphy to characterize nonhypersecreting adrenal tumors originally detected on CT or MRI; for this purpose, we reviewed nuclear adrenal scans obtained in our department with different radiopharmaceuticals such as radiolabeled norcholesterol, MIBG, and FDG. Because these agents have no relation to each other and are taken up by individual parts of adrenals on the basis of entirely separate mechanisms, they can be used to identify different types of adrenal tumors.
The precursor molecule from which all adrenocortical steroid hormones are synthesized is cholesterol (16). This ubiquitous substance may be accumulated by the adrenal cortex from the circulation through a receptor-mediated pathway for low-density lipoproteins, substances carried by cholesterol that are synthesized in the liver. Once incorporated by the adrenal cortex, cholesterol is stored in esterified form and acts as the substrate for enzymatic conversion to various adrenal steroid hormones. These characteristics form the biological basis on which labeled norcholesterol was selected for adrenal cortical scintigraphy. In this regard, this radiotracer has been used to evaluate both hypersecreting and nonhypersecreting adrenal abnormalities (14,17); in particular, norcholesterol can provide information regarding lesion diagnosis and characterization for nonhypersecreting adrenal abnormalities. In our studies, all adenomas showed clearly increased norcholesterol uptake, which allowed for identification of this benign type of tumor. Therefore, these lesions were nonhypersecreting because there was no excessive hormone secretion, but they were functional in the sense of their ability to concentrate norcholesterol.
However, 2 false-positive cases of norcholesterol imaging were observed: a myelolipoma and a pheochromocytoma, both of which showed diffuse tracer uptake. The only explanation for the evidence of norcholesterol tumor activity in these cases could be the presence of residual functional cortical tissue in the adrenal lesions. Of course, the occurrence of these 2 false-positive cases slightly reduced the PPV to 89% of norcholesterol imaging to characterize an adrenal mass as an adenoma; Gross et al. (14) reported a PPV of 100% for this characterization. Tsukamoto et al. (18) recently observed unusual norcholesterol accumulation in adrenal metastases by adrenal cell carcinoma; this last finding could also be explained by the presence of residual functional cortical tissue in malignant lesions.
MIBG has been shown to undergo specific uptake and storage by adrenal medulla, the sympathetic autonomic nervous system, and tumors derived from these tissues (19). A significant portion of tracer uptake into these tissues occurs by means of the specific and high-affinity sodium uptake mechanism as well as the energy-dependent type I amine uptake mechanism. In particular, within the adrenal medullary and pheochromocytoma cells there may be storage granules (20). Previous studies have clearly shown the usefulness of radioactive MIBG imaging in the diagnostic evaluation of patients with pheochromocytoma and with extra-adrenal paragangliomas (21). However, in these studies MIBG scintigraphy was used to localize and detect tumor sites in patients with hypersecreting lesions; no data regarding nonhypersecreting pheochromocytoma have been reported. In our study, we investigated the role of MIBG imaging to identify nonhypersecreting pheochromocytoma in a subgroup of patients with indeterminate adrenal masses. Usually, pheochromocytomas are characterized by an increased level of catecholamines, as well as their metabolites, and by corresponding symptoms so that diagnosis is clear (22). However, lesions may occur without symptoms (15,23–26). In our experience, including the 7 y of our study, we observed this finding in a significant number of patients with pheochromocytomas; in fact, we found 5 (31%) nonhypersecreting lesions and 11 (69%) classic hypersecreting medullary tumors. Furthermore, this finding represented 5 (9%) of our patient population (n = 54) with nonhypersecreting adrenal masses. Therefore, this condition merits specific attention.
In such patients, clinical diagnosis of pheochromocytoma using laboratory tests is impossible. Therefore, the integrated imaging results of MIBG and CT or MRI seem to be clinically relevant for this purpose. In fact, the presence of MIBG uptake in a nonhypersecreting adrenal mass can characterize the lesion as a pheochromocytoma. Whereas this tumor type specifically concentrates MIBG into its catecholamine storage granules, other adrenal space-occupying abnormalities do not accumulate this agent. In particular, this finding was found in our series in 4 cases of nonhypersecreting tumors histologically proven to be pheochromocytoma. A similar result was also obtained in a case of nonhypersecreting ganglioneuroma detected in the upper abdomen. A comparable finding was described by Smit et al. (27) in a patient with a paraganglioma of the neck with no clinical or biochemical evidence of catecholamine secretion, but with significant MIBG uptake. Thus, as previously reported by our group (28), we believe that MIBG scintigraphy is diagnostically useful to identify or rule out nonfunctional tumors of medullary chromaffin tissue. This observation adds an indicative criterion for the characterization of asymptomatic pheochromocytoma with nondiagnostic biochemical tests. MIBG uptake by this adrenal lesion in the absence of catecholamine hypersecretion suggests that tracer tumor activity reflects storage rather than hormone secretion. This finding is consistent with previous data showing no significant relationship between MIBG lesion uptake and catecholamine secretion (29,30).
The presurgical characterization of pheochromocytoma is critical for appropriate patient preparation before tumor resection. In the case of a hypersecreting tumor, this diagnostic information can be obtained using clinical data and laboratory measurement of adrenal medullary hormones. Conversely, this approach cannot be used for nonhypersecreting pheochromocytomas. Although a high T2-weighted MR signal intensity has been reported as a characteristic of pheochromocytomas, other adrenal lesions such as adenomas, carcinomas, and metastases may give similar images (5,6). Therefore, the presence of MIBG uptake in nonhypersecreting pheochromocytomas may represent a new noninvasive imaging criterion to perform tumor characterization and appropriate dibenzyline administration before surgery. Thus, careful observation is warranted for asymptomatic patients with normal catecholamine levels. Anesthesiologists and other physicians must be alerted to manage a hypertensive crisis during the induction of anesthesia, during surgery, and in other stressful circumstances for such patients. MIBG imaging might be proposed to screen nonhypersecreting adrenal masses to confirm or rule out the presence of silent pheochromocytoma. This approach has also been suggested by others in a different patient population (31).
In our study, no MIBG uptake occurred in adrenal masses other than pheochromocytomas or ganglioneuromas, such as adenomas, cysts, pseudotumors, or malignant lesions. However, a false-positive MIBG result was observed in a case of a large adrenal carcinoma. Although this finding was the only occurrence of a false-positive result, the PPV of MIBG imaging to characterize an adrenal mass as a chromaffin tissue tumor was not very high (83%); this finding was related to the small number of true-positive cases. The reasons for MIBG uptake in an adrenal carcinoma are unclear. The possible neuroendocrine origin of such lesions might result in MIBG concentration. Miettinen (32) showed neuroendocrine differentiation in a significant number of adrenal carcinomas, as manifested by the presence of immunoreactivity for neurofilament proteins, neuron-specific enolase, and S-100 protein. However, these laboratory findings were not observed in our case in which immunostaining was positive only for vimentin, a mesenchymal marker often present in cortical adrenal carcinomas. Therefore, MIBG uptake by this type of adrenal tumor, as reported in our case, remains to be clarified. To our knowledge, no cases of adrenal carcinoma with increased MIBG activity have been described in the literature. Hoefnagel (33) studied a patient with this type of tumor, but no MIBG uptake was found. Because no comparative data are available, additional research is needed in this field.
We performed MIBG scintigraphy using 131I because this radiolabel is used in our department. However, nuclear imaging with 131I is not optimal. MIBG labeling with 123I has several advantages (34). In fact, its shorter half-life allows a larger radionuclide dose to be given, which permits SPECT and more sensitive and accurate detection of adrenal medullary tumors. In this regard, SPECT imaging has also been proposed for norcholesterol imaging (35).
Adrenal glands are frequently associated with malignant tumors, particularly cortical carcinomas, lymphomas, and metastases. The characterization of benign and malignant lesions may be difficult in asymptomatic patients, although several hormonal and histological criteria have been proposed. In the absence of specific endocrine hypersecretion, however, no individual finding can absolutely resolve this issue. Although CT and MRI patterns can suggest the diagnosis of malignancy by such criteria as large tumor size, high contrast, or gadolinium enhancement, as well as by increased signal intensity on T2-weighted MR images or no signal change on chemical-shift MR sequence, these criteria are suggestive but not necessarily diagnostic of malignancy (5,6). In this setting, the results of previous clinical studies performed by others and our group (9,36,37) suggested the diagnostic usefulness of FDG PET to differentiate between benign and malignant adrenal masses. FDG uptake has been reported to reflect high tumor metabolism because, as a d-glucose analog, its use for in vivo imaging depends on the enhanced glycolysis in cancer cells. This phenomenon has been related to an increase in both the content of glucose membrane transporters and the functional activity of the principal enzymes controlling the glycolytic pathways. Furthermore, FDG concentration in malignancies has been associated with proliferative tissue activity and the amount of viable cells, thus, being an accurate indicator of tissue viability of adrenal lesions (38). In this study, we evaluated the role of FDG PET in characterizing nonhypersecreting malignant tumors in a subgroup of patients with indeterminate adrenal masses. Although no increased uptake of FDG was observed in patients with benign lesions, FDG activity clearly increased in malignant adrenal tumors, reflecting high glucose metabolism. Therefore, indicative specific metabolic criteria may be included in radionuclide adrenal imaging to evaluate patients with radiographically indeterminate nonhypersecreting adrenal masses in which there is a high risk of malignancy. In this regard, the possibility of characterizing benign and malignant adrenal masses using FDG PET shows a relevant clinical impact. This diagnostic information allows one to plan appropriate treatment in such patients, avoiding surgical intervention in cases of benign tumors or metastatic malignant lesions. Conversely, accurate characterization of an adrenal mass as a malignant tumor with localized increased FDG activity would suggest the need for surgical resection. In this regard, in 1 patient in our study with a small and well-encapsulated adrenal carcinoma that significantly concentrated FDG, the results of PET imaging were essential for clinical decision making; although standard adrenal imaging had resulted in misdiagnosis of the carcinoma as an adenoma, the patient underwent timely surgical treatment.
Moreover, in patients with proven malignant adrenal tumors, the evaluation of regional and distant disease spread represents critical staging for a complete work-up before any treatment strategy. In 7 patients with adrenal malignancies in our study, whole-body FDG PET detected extra-adrenal lesions, which allowed accurate tumor staging using a single imaging modality. In fact, a large number of extra-adrenal tumor sites that showed increased FDG activity in the chest and abdomen were detected by PET. Abnormal FDG uptake in these lesions was subsequently confirmed by anatomic cross-sectional imaging modalities such as CT or MRI. These findings were clinically relevant for treatment planning; chemotherapy was pursued instead of adrenal surgery. Furthermore, as an alternative to several conventional imaging techniques, this diagnostic approach might be particularly valid in terms of its cost-effectiveness and accurate management of patients.
Although fine-needle biopsy has been proposed as part of the algorithm for diagnosing and treating patients with nonhypersecreting adrenal masses, this method is invasive and can have complications (15,39). The results of this study and those of others (15) suggest that radionuclide imaging may play a significant role in noninvasively characterizing silent adrenal tumors. Therefore radionuclide imaging should be inserted in the diagnostic protocol of such patients to supplement CT or MRI findings, particularly when these images are inconclusive for lesion characterization. This approach could eliminate the need for fine-needle biopsy, which is invasive and uncomfortable for the patient. In this regard, the selection of the appropriate radiotracer for adrenal scintigraphy depends on clinical patient history and availability of radiocompounds and equipment. Because benign adenomas are the most common cause of nonhypersecreting adrenal tumors, labeled norcholesterol should be the first choice for patients with no history of cancer. In the case of a norcholesterol scan with normal results, MIBG should be used to confirm or rule out the presence of nonhypersecreting pheochromocytoma. If MIBG imaging results are also normal, FDG PET may be considered when clinical suspicion of malignancy is high. Conversely, when neoplastic patients are evaluated, FDG PET should be initially performed; if FDG PET results are normal, it should be followed by norcholesterol and, in sequence, MIBG studies. However, FDG adrenal imaging is currently limited by the availability of PET centers. The development of new PET laboratories or wider clinical application of dual-head coincidence FDG SPECT (40) might increase the use of FDG imaging in this setting. Finally, clinical applications for labeled somatostatin analogs are uncertain because experience with nonfunctional adrenal lesions has been limited (13); however, these radiocompounds may be used to identify somatostatin receptors on adrenal tumors for possible somatostatin therapy when conventional treatments are ineffective.
CONCLUSION
Adrenal scintigraphy has the potential to play a clinically significant role in the diagnostic evaluation of patients with nonhypersecreting adrenal masses. The main contribution of radionuclide imaging consists of functional information for tumor characterization. Specific radiotracers such as MIBG, norcholesterol, and FDG may be selected to identify pheochromocytomas, adenomas, and malignant lesions, respectively, both primary and metastatic. Thus, in patients with radiographically indeterminate adrenal masses, nuclear imaging is recommended for tumor diagnosis and for the selection of appropriate therapy, particularly when the CT or MRI findings are inconclusive for lesion characterization.
Acknowledgments
The authors thank Dr. Massimo Imbriaco, Dr. Francesco Izzo, and Dr. Steven Curley for manuscript revision before submission; Dr. Corradina Caracò, Dr. Luisa Castelli, and Dr. Luca Del Viscovo for performing some of the MRI studies; Carmela Imparato for assistance in organizing this work; Maria Rosaria Panico, Raffaella Roma, Gianfranco Calicchio, and Antonello Green for their collaborative work on 18F production; and Aldo Bartiromo and Anna Prisco for technical assistance in performing PET studies. This work was supported in part by grants from Consiglio Nazionale delle Ricerche, Associazione Italiana per la Ricerca sul Cancro, and Istituto Nazionale dei Tumori di Napoli. This research was presented in part at the Congress of the European Association of Nuclear Medicine in Paris, France, on September 2–6, 2000.
Footnotes
Received Aug. 16, 2000; revision accepted Nov. 17, 2000.
For correspondence or reprints contact: Simone Maurea, MD, PhD, Medicina Nucleare, Istituto Nazionale dei Tumori, via Raffaele De Cesare no. 7, 80132, Napoli, Italy.
REFERENCES
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Computed tomography criteria for discrimination of adrenal adenomas and adrenocortical carcinomas: analysis of the German ACC registry
- Guidelines on the radical management of patients with lung cancer
- Adrenocortical cancer: pathophysiology and clinical management
- Upper pole of a duplex kidney mimicking adrenal incidentaloma in 18F-fluoro-2-deoxy-D-glucose positron emission tomography: a pitfall in diagnosis
- Characterization of the Normal Adrenal Gland with 18F-FDG PET/CT
- SPECT Semiquantitative Analysis of Adrenocortical 131I-6{beta}-Iodomethyl-Norcholesterol Uptake to Discriminate Subclinical and Preclinical Functioning Adrenal Incidentaloma
- Role of Molecular Imaging in Management of Nonhypersecreting Adrenal Masses