


Abstract
The goal of this study was to evaluate the clinical reliability of the 131I-6β-iodomethyl-norcholesterol (131I-NP-59) uptake semiquantitative evaluation method we propose for the characterization of adrenocortical masses in a selected population of patients with disease clinically classified as subclinical (SC) and preclinical (PC) Cushing’s syndrome (CS) according to Reincke’s definition. Methods: Forty-seven consecutive patients with incidentally discovered unilateral adrenal masses were examined by a triple-head SPECT system after intravenous injection of 131I-NP-59. Abdominal SPECT was performed at 24, 48, 72, and, in selected cases, 96 h after tracer injection. Connected with adrenals and liver, a standard elliptic region of interest (ROI) was manually drawn, taking care to avoid the gallbladder region. The adrenal ROI integral count, obtained by summing the 24-, 48-, and 72-h counting values, was normalized by the hepatic integral count. Subsequently, the adrenal percentage of relative uptake (UPT%) was computed. Results: Discriminant analysis was performed on the variables UPT%, adrenocorticotropic hormone (ACTH) serum concentration, and CT mass dimension (CTMD) to determine the variable, or combination thereof, best discriminating between the SC-CS and PC-CS groups. Compared with both ACTH and CTMD variables, univariate analysis confirmed the UPT% variable as the most significant to discriminate between these 2 clinical groups. In fact, UPT% alone correctly classified 8 of 9 patients in the SC-CS group and 20 of 22 patients in the PC-CS group with 95% positive and 80% negative predictive values and with overall accuracy, sensitivity, and specificity equal to 90%, 91%, and 89%, respectively. When all 3 variables were submitted to stepwise discriminant analysis, the derived classification matrix, after cross-validation, correctly classified 9 of 9 patients in the SC-CS group and 18 of 22 patients in the PC-CS group with 100% positive and 69% negative predictive values and with overall accuracy, sensitivity, and specificity equal to 87%, 82%, and 100%, respectively. Conclusion: According to these initial results, use of the proposed semiquantitative approach associated with both laboratory screening for cortisol production and CTMD measure seems to be able to increase the clinical diagnostic accuracy of PC-CS. This approach could be used in the follow-up of adrenal mass function every time hormonal or clinical features are suggestive of adrenocortical hyperfunction.
The increasing use of radiologic imaging diagnostic tools supplied with high anatomic resolution has increased the frequency of incidentally detected adrenal masses (incidentalomas) (1–3). Benign, nonhyperfunctioning, nonautonomous, adrenocortical adenomas represent the most frequent types of incidentaloma (approximately 2%–9% of cases in autopsy series (4)). The excellent morphologic details afforded by CT and MRI associated with both laboratory assessment and clinical signs provide us with the diagnosis in most clinical cases. But, the adrenal mass functional characterization is essential when it is not causing clinical adrenal hyperfunction (5–7), which arises whenever cortisol hyperproduction is not in a sufficient amount to produce specific signs and symptoms of hypercholesterolism in the patient (8). Indeed, even though most of the incidentally detected adrenal masses are nonfunctional adrenocortical adenomas, a nonnegligible percentage of them are hormonally active, with as many as 20% of the tumors producing glucocorticoids (8).
Functional assessment of benign adrenal masses is an important issue because several late clinical consequences may be expected in patients with borderline preclinical functional increase. The terms “subclinical Cushing’s syndrome” (SC-CS) and “preclinical Cushing’s syndrome” (PC-CS) have often been used as synonyms; actually, the PC-CS patients have the potential risk of developing an overt Cushing’s syndrome (CS). Recent reports suggest that the progression from PC-CS to CS occurs in a low percentage of patients, but long-term prospective studies evaluating the outcome of PC-CS patients are still lacking (9). Reincke proposed a definition showing subtle but important differences between SC-CS and PC-CS (8). To synthesize, SC-CS relates to biochemical abnormalities, which, most likely, will not become clinically manifest. PC-CS relates to biochemical abnormalities with a general progression to overt CS. In the PC-CS clinical subgroup, a high prevalence of obesity, arterial hypertension, and non–insulin-dependent diabetes mellitus (NIDDM) is frequently observed, whereas the classical pattern of hypercortisolism is missing. These observations suggest that the clinically silent hypercortisolism is not completely asymptomatic; its duration and extent may influence the development of clinical signs. Because surgery seems to be able to correct hypertension, obesity, and NIDDM, patients with these diseases should be screened for a possible alteration in cortisol production (10). To avoid postoperative adrenocortical insufficiency, adrenalectomy should be considered in patients with suppressed plasma adrenocorticotropic hormone (ACTH) and increased urinary free cortisol concentration before complete adrenal functional autonomy (8). It follows that the implementation of clinical methods, able to discriminate the 2 groups, is a matter of great importance. Hormonal features alone are not able to reach that aim. Indeed, neither subtle changes in glucocorticoid secretion, as well as the excretion of the main glucocorticoid metabolites, nor a blunted ACTH response to corticotropin-releasing hormone, in the presence of a normal inhibition by dexamethasone, is specific enough to make a diagnosis of PC-CS (8,10,11).
Several reports analyze the different adrenal uptake patterns of radiotracers obtained by conventional scintigraphic planar techniques (12–16). The analysis of these patterns is useful to differentiate hypersecreting adrenocortical adenomas from bilateral hyperplasia and nonfunctional adenomas. However, the interpretation of scintigraphic images by strictly qualitative criteria is liable to subjectivity, especially in the cases of moderate cholesterol uptake and superimposition of anatomic structures with physiologic accumulation.
As is well known, SPECT improves image resolution of smaller lesions and increases sensitivity without reducing specificity. It follows that the qualitative pattern analysis by SPECT, owing to its better target-to-background ratio, could prove to be an effective approach either to identify adrenal or to distinguish its uptake from that of liver, gallbladder, or colon (17,18). Furthermore, SPECT can perform quantitative analysis of adrenocortical uptake. The uptake in target tissues normalized to the ones in a reference region may be used in clinical practice as an indicator of biologic behavior in time (19). This approach proved fruitful in neurology and cardiology (20,21).
Accordingly, in this study we tested the clinical reliability of the 131I-6β-iodomethyl-norcholesterol (131I-NP-59) uptake semiquantitative evaluation method for the characterization of adrenocortical masses in a selected population of patients clinically classified as SC-CS and PC-CS according to Reincke’s definition (8).
MATERIALS AND METHODS
Patient Population
Between January 1999 and June 2002, 47 consecutive patients (25 men, 22 women; mean age ± SD, 56.8 ± 10.3 y) with incidentally discovered unilateral adrenal masses in the course of abdominal CT performed for evaluation of unrelated disease were examined by triple-head SPECT (IRIX 3000; PIKER International) after intravenous injection of 131I-6β -iodomethyl-norcholesterol (131I-NP-59 [NORCHOL-131]; CIS Bio International) (Table 1).
Summary of Patient Population Clinical Characteristics
The patients were unaware of extraadrenal malignancies and showed no severe or paroxysmal hypertension, hypokalemia, or clinical signs of overt hypercortisolism or hyperandrogenism (22). Inclusion criteria were established on the basis of both radiologic (23) and endocrinologic values. We included in the study only adrenal masses with radiologic signs suggestive for the presence of a benign mass: tumor with an oval shape, hypodense and homogeneous pattern with well-defined margins, and no enhancement or mild enhancement after contrast medium administration. All patients underwent the following endocrine staging valuations: baseline measurements of plasma cortisol at 0800 h, morning adrenocorticotropin (ACTH), 24-h urinary free cortisol (UFC), dehydroepiandrosterone sulfate (DHEA-S), 17-hydroxyprogesterone (17-OHP), supine and upright plasma renin activity and aldosterone, and 24-h urinary aldosterone. The above selected hormonal variables were determined using commercially available immunoassay kits. The normal range for serum cortisol and ACTH concentrations at 0800 h were 140–690 nmol/L and 9–52 ng/L, respectively. The normal value for 24-h UFC was <275 nmol/L. The normal ranges for serum DHEA-S and 17-OHP concentrations were 1.3–6.7 mmol/L and 0.2–9 nmol/L, respectively. Twenty-two patients with clear hypothalamus–pituitary–adrenal axis abnormalities showed at least 2 clinical signs suspected for subtle hypercortisolism, as mild hypertension (24), NIDDM (fasting glycemia, >126 mg/dL) (25), and diffuse obesity (body mass index (BMI), >25). In all patients, plasma cholesterol concentration was in the normal range (160–220 mg/dL) (26). According to Reincke’s proposal (8) and on the basis of both clinical and endocrine features at the staging, the study population was classified in 3 groups (Table 2): (a) No functioning adenoma (NF): subjects showing neither endocrine abnormalities (EA) nor typical signs or symptoms of hypercortisolism (SS) (9 M, 7 F; mean ± SD, 55.8 ± 12.8 y); (b) SC-CS: subjects showing EA but no SS (6 M, 3 F; mean ± SD, 58.5 ± 6.7 y); (c) PC-CS: subjects showing EA, no SS, but at least 2 of the following clinical signs: edema, arterial hypertension, diffuse obesity, NIDDM, or glucose intolerance (10 M, 12 F; mean ± SD, 53.8 ± 9.8 y). The final clinical diagnosis was confirmed in all patients included in the study by 1-y follow-up data. Anyone developed an overt CS during this observation period.
Characteristics of Patient Population According to Reincke Clinical Classification
Corticoadrenal Scintigraphy
All 47 selected patients underwent corticoadrenal scintigraphy after intravenous injection of 37 MBq 131I-NP-59. Abdominal SPECT was performed at 24, 48, 72, and, in selected cases, 96 h after tracer injection. To block the free 131I thyroid uptake, 10 drops of Lugol’s solution were given daily to each patient starting 3 d before tracer injection and continuing for an additional 1 wk. To avoid enterohepatic circulation of radiocholesterol resulting in intestinal background, which can obscure adrenal radioactivity, a mild laxative was given beginning 2 d before the first day of image acquisition and for the duration of examination (27). The triple-head gamma camera was equipped with 1 high-energy collimator, and a 15% window was centered at 364 keV. Using a 360° arc step-and-shoot acquisition, 120 projections (40 per head) were acquired resulting in 4.4 × 4.4 mm pixel size, 128 × 128 matrices. Images, acquired for 60 s per projection for a total imaging time of 40 min, were reconstructed from projection data by the filtered backprojection algorithm. A ninth-order Butterworth filter with a cutoff frequency of 0.30 was selected. A summation image was obtained by adding 10 consecutive slices from the first one in which the adrenal uptake was detected. In any case, the 10 slices completely comprised both adrenal glands. Connected with adrenals and liver, a standard elliptic region of interest (ROI) was drawn, taking care to avoid the gallbladder region. The adrenal ROI integral count, obtained by summing the 24-, 48-, and 72-h values, was normalized to the hepatic integral one (nUPTint). Subsequently, the adrenal percentage of relative uptake (UPT%) was computed as follows:
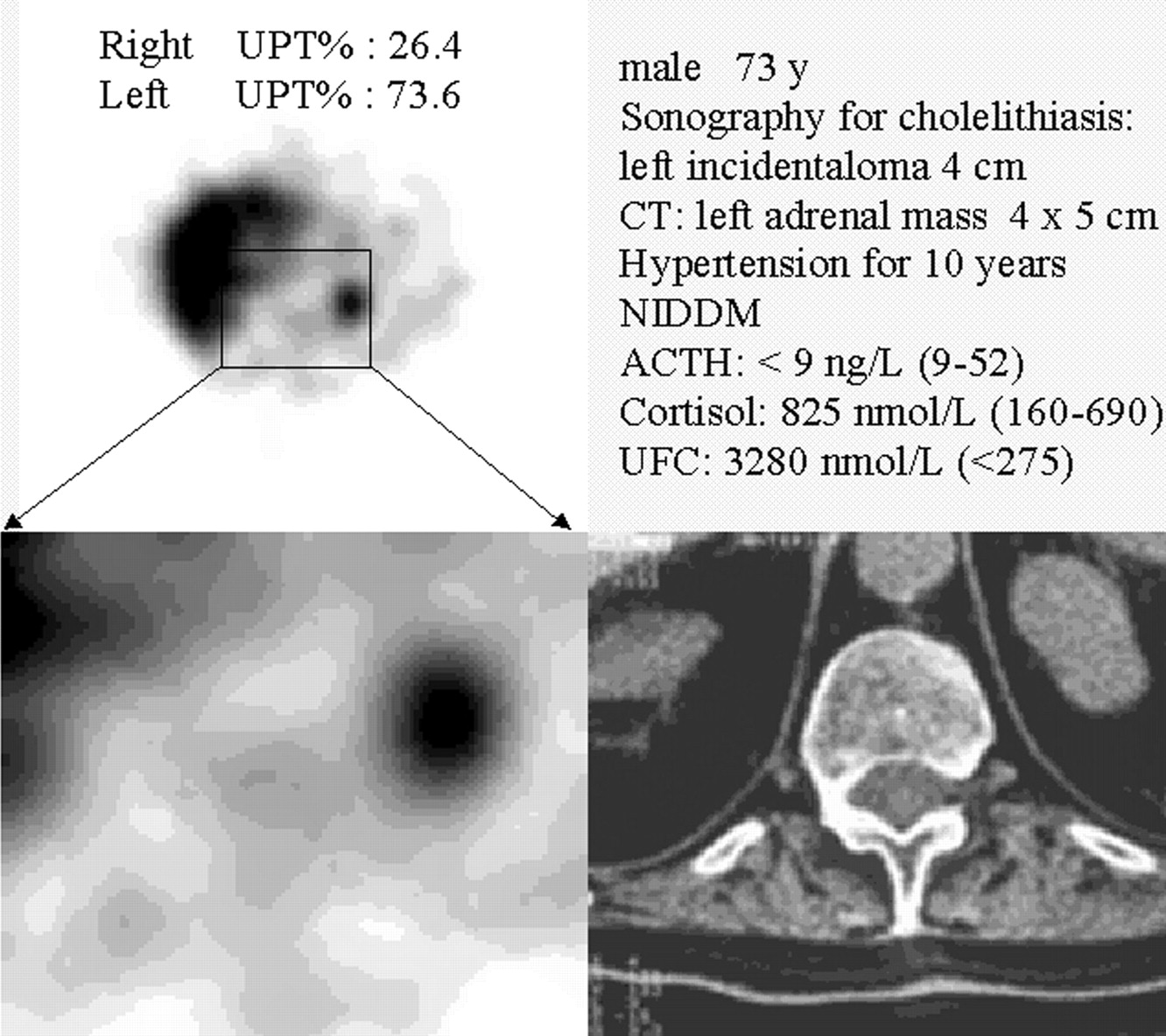
 where (nUPTint)adenoma is the normalized integral count on the adrenal gland afflicted with adenoma and (nUPTint)normofunctional is the normalized integral count on the other adrenal gland (Fig. 1).
where (nUPTint)adenoma is the normalized integral count on the adrenal gland afflicted with adenoma and (nUPTint)normofunctional is the normalized integral count on the other adrenal gland (Fig. 1).
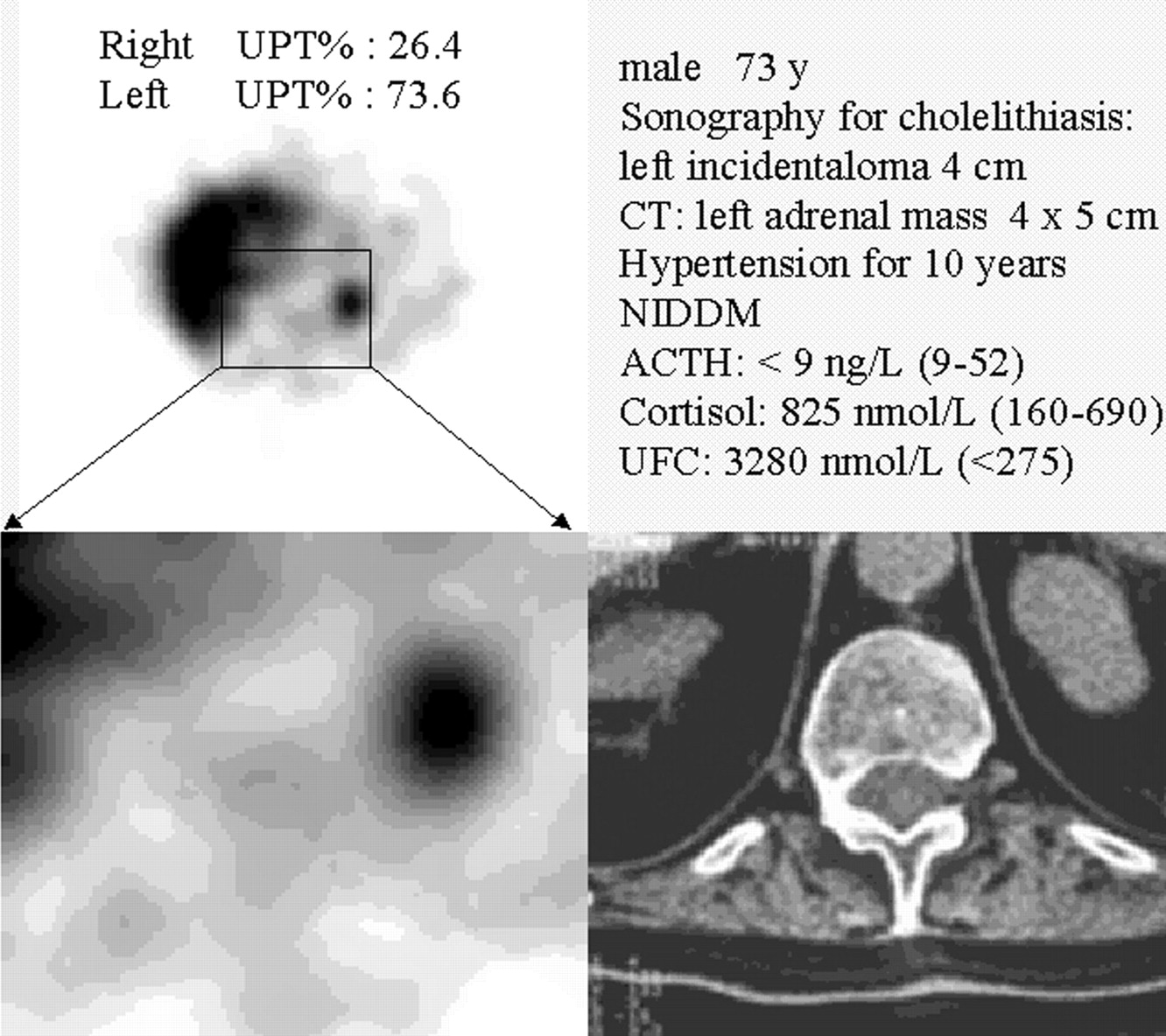
Typical adrenal incidentaloma SPECT study at 72 h after 131I-NP-59 injection in patient classified, according to Reincke (8), as PC-CS. Scintigraphic study shows typical example of concordant pattern: increased radiotracer uptake on side of lesion demonstrated on CT scan (4 × 5 cm left corticoadrenal adenoma).
Statistical Analysis
All results are expressed as mean ± SD. All correlations were examined by linear regression analysis. ANOVA by the Tukey post hoc test was used for between-group and within-group comparisons. Comparison of proportions was done by the Fisher exact test. To analyze the reproducibility of UPT% measurements, the absolute interobserver difference of UPT% values was calculated. In addiction, paired t tests were used to assess interobserver differences. Stepwise discriminant analysis was performed on the variables UPT%, ACTH, and CT mass dimension (CTMD) to determine the variable, or combination thereof, that is able to linearly discriminate the best between the NF, SC-CS, and PC-CS groups. This procedure involves the computation of a linear function yielding the optimal possible classification of the observations having as its reference a grouping factor. In this study, the reference grouping factor was the staging clinical diagnosis (NF, SC-CS, and PC-CS), confirmed after almost 1 y of patient follow-up. The achieved classification, after cross-validation, was submitted to a jack-knife validation procedure to limit bias in the number of patients correctly classified. Details about the discriminant function analysis follow.
In a 3-group case (NF, SC-CS, and PC-CS), a canonical correlation analysis that will determine the successive functions and canonical roots (eigenvalues that are associated with the respective canonical function) must be performed. The maximum number of functions will be equal to the number of groups minus 1, or the number of variables in the analysis. To discriminate NF, SC-CS, and PC-CS, the following equations were applied:


In the 2-group case (SC-CS and PC-CS), discriminant function analysis is analogous to a multiple regression function; in general, in the 2-group case, we fit a linear equation of the type:
 where a is a constant, b1 through bm are regression coefficients, and x1 to xm are equal to the quantification parameter used (UPT%, CT, and ACTH). Those variables with the largest standardized regression coefficients are the ones that contribute most to the prediction of group membership. To discriminate SC-CS from PC-CS, the following equation was applied:
where a is a constant, b1 through bm are regression coefficients, and x1 to xm are equal to the quantification parameter used (UPT%, CT, and ACTH). Those variables with the largest standardized regression coefficients are the ones that contribute most to the prediction of group membership. To discriminate SC-CS from PC-CS, the following equation was applied:

The coefficients given in these 2 equations were calculated for the data included in this study.
The STATISTICA (STATSOFT; www.statsoft.com) and the Minitab Statistical software (MINITAB; www.minitab.com) packages were used for statistical data analysis. P < 0.05 was considered statistically significant.
RESULTS
Sixteen of 47 patients, classified in the NF group, showed a normal bilateral and symmetric 131I-NP-59 uptake. Thirty-one of 47 patients, classified in the SC-CS and PC-CS groups, showed an asymmetric and prevalent 131I-NP-59 uptake on the side of the lesion, suggesting a hyperfunctioning adrenal mass. No patient showed a discordant uptake pattern (4). The range of the UPT% values in the NF, SC-CS, and PC-CS groups were 51.3–64.7, 54.2–63.9, and 55.5–73.6, respectively. The same UPT% values were significantly different between the PC-CS (65.1 ± 4.1) and SC-CS (57.9 ± 2.8) groups and also between the NF (56.9 ± 3.9) and PC-CS groups (P < 0.0001). The range of the CTMD values in the NF, SC-CS, and PC-CS groups were 1.5–3.5 (1.9 ± 0.6), 1.5–3 (2.4 ± 0.6), and 2–5.8 (3.2 ± 1), respectively. A statistically significant difference was found only between the NF and PC-CS groups (P < 0.0001). Morning ACTH levels were significantly different between the NF (24.3 ± 5.8) and SC-CS (8.7 ± 1.5) groups (P < 0.0001) as well as between the NF and PC-CS (8.5 ± 1.8) groups (P < 0.0001). Both morning serum cortisol and UFC variables showed no significant difference among the 3 groups.
The existence of any relationship between UPT%, CTMD, morning ACTH levels, morning serum cortisol, and UFC was investigated by multiple regression analysis. A low significant correlation between UPT% and morning ACTH levels (r = 0.53; P < 0.0001), morning serum cortisol (r = 0.32; P < 0.03), UFC (r = 0.38; P < 0.01), and CT dimension (r = 0.42; P < 0.005) was found. Therefore, morning ACTH levels correlate with the CT dimension (r = 0.41; P < 0.005). No significant correlation was found with morning serum cortisol (r = 0.25; P < 0.09) and UFC (r = 0.18; P = 0.22) (Fig. 2).
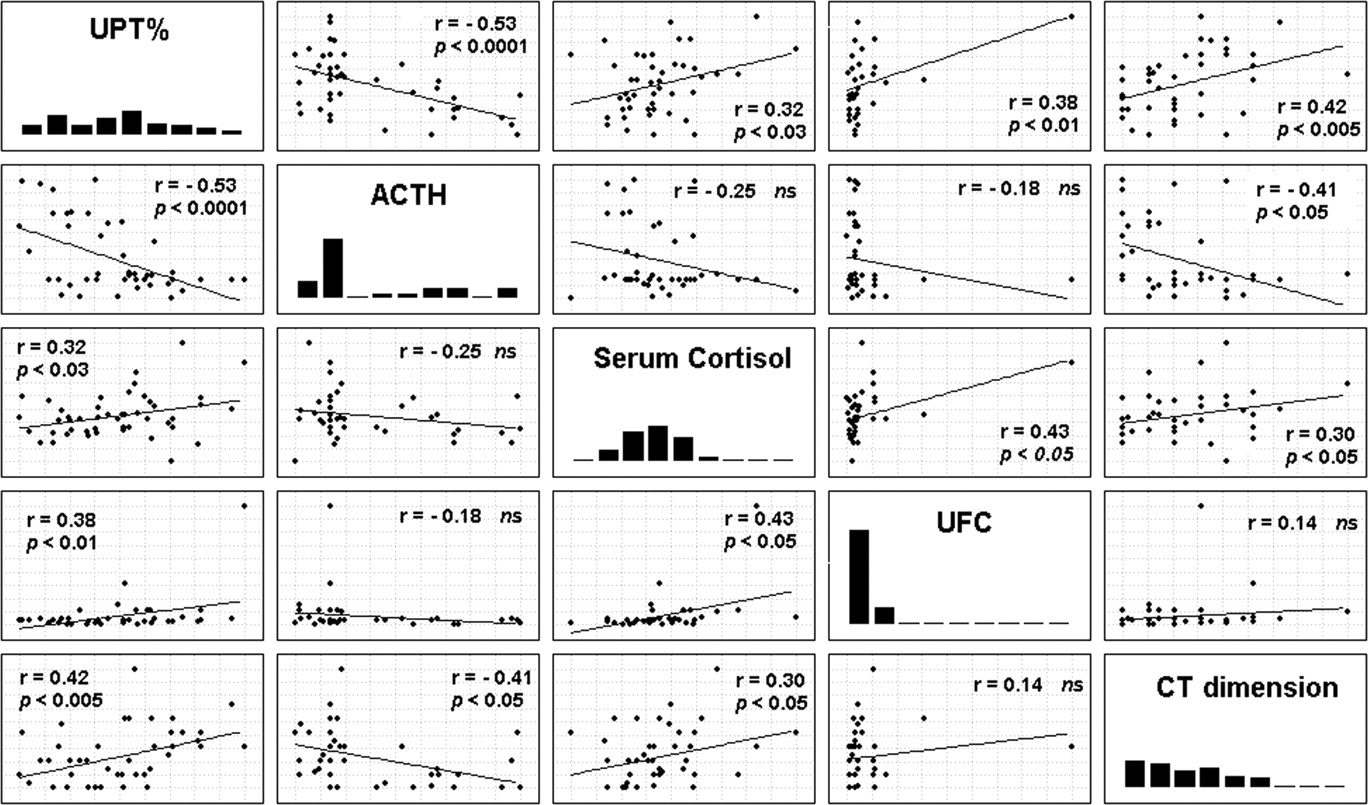
Scatter plots show correlations between UPT% and some biochemical and radiologic parameters.
To classify patients in the NF, SC-CS, or PC-CS groups, the 3 considered variables—UPT%, ACTH serum concentration, and CTMD—were submitted to univariate discriminant analysis; subsequently, different combinations were submitted to stepwise discriminant analysis. For each of them, after cross-validation, a classification matrix was derived. To differentiate among the 3 clinical groups, the cutoff values related to all considered variables were derived by an univariate discriminant analysis: UPT% of 57.4 and 61.5 best discriminate NF versus SC-CS and SC-CS versus PC-CS, respectively. ACTH values (expressed in nmol/L) of 16.5 and 8.6 best discriminate NF versus SC-CS and SC-CS versus PC-CS, respectively. CT mass dimension values (expressed in cm) of 2.2 and 2.8 best discriminate NF versus SC-CS and SC-CS versus PC-CS, respectively. Using the previous specified cutoff values, ACTH correctly identified 14 of 16 NF, 7 of 9 SC-CS, and 7 of 22 PC-CS with a global diagnostic accuracy of 59% (P < 0.0001). UPT% correctly identified 9 of 16 NF, 4 of 9 SC-CS, and 20 of 22 PC-CS with a global diagnostic accuracy of 70% (P < 0.0001). CT correctly identified 12 of 16 NF, 4 of 9 SC-CS, and 14 of 22 PC-CS with a global diagnostic accuracy of 64% (P < 0.0001). ACTH together with UPT% correctly identified 14 of 16 NF, 8 of 9 SC-CS, and 20 of 22 PC-CS with a global diagnostic accuracy of 89% (P < 0.0001). ACTH, UPT%, and CT correctly identified 13 of 16 NF, 9 of 9 SC-CS, and 17 of 22 PC-CS with a global diagnostic accuracy of 83% (P < 0.0001). Table 3 summarizes the results. Addition of the CT diameter as a new decision factor in discriminant analysis decreased sensibly the percentage of PC-CS correctly identified and did not considerably improve the overall diagnostic accuracy.
Results of Discriminant Analysis Applied on ACTH, UPT%, and CTMD Using Reincke Classification as Population Grouping Factor
Subsequently, using the variables combinations as above, discriminant analysis was applied on the SC-CS and PC-CS groups. The univariate analysis results confirmed the UPT% variable as the most efficient discriminant parameter between those 2 clinical groups, compared with both ACTH and CTMD. In fact, UPT% alone correctly classified 8 of 9 SC-CS and 20 of 22 PC-CS, with an overall accuracy of 90%, a sensitivity and specificity of 91% and 89%, respectively, and a 95% positive predictive value and an 80% negative predictive value. ACTH alone correctly classified 7 of 9 SC-CS and 7 of 22 PC-CS, with an overall accuracy of 45%, a sensitivity and specificity of 32% and 78%, respectively, and a 78% positive predictive value and a 32% negative predictive value. CT alone correctly classified 6 of 9 SC-CS and 14 of 22 PC-CS, with an overall accuracy of 64%, a sensitivity and specificity of 64% and 67%, respectively, and an 82% positive predictive value and a 43% negative predictive value. When all 3 variables were submitted to stepwise discriminant analysis, the derived classification matrix after cross-validation correctly classified 9 of 9 SC-CS and 18 of 22 PC-CS, with an overall accuracy of 87%, a sensitivity and specificity of 82% and 100%, respectively, and a 100% positive predictive value and a 69% negative predictive value. Table 4 summarizes the results.
Results of Discriminant Analysis Applied on ACTH, UPT%, and CTMD in SC-CS and PC-CS Groups
Our UPT% measurements are reproducible. The interobserver difference of UPT% measurements was not significant (P = 0.57). The mean of interobserver absolute difference of UPT% measurements was 0.56% with a range of 0%–2.3%. The interobserver variability, expressed as a coefficient of variation and 1 SD, was 1.02% and 0.55%, respectively.
DISCUSSION
In the vast majority of cases, adrenal masses discovered by CT and MRI are nonhypersecreting adrenocortical adenomas. Moreover, they can be associated with subtle endocrine abnormalities with risk of progression from asymptomatic hormonal increases to overt endocrine hyperfunction. The functional characterization of adrenocortical masses is necessary in all patients with laboratory-proven hormonal hyperproduction, asymptomatic or with clinical presentation questionable for CS. In the past, selective venous sampling from renal veins was performed to evaluate functional adenomas. The technique is very sensitive in the cases of lateralized hormonal hyperproduction. However, it is invasive and expensive and is rarely used today. Adrenocortical scintigraphy provides both functional characterization and anatomic localization of the adrenal glands by radiolabeled norcholesterol uptake.
The scintigraphic pattern is related to both the nature and the functional status of the adrenal incidentaloma. Barzon et al. (28) demonstrated the relationship between endocrine data and radiocholesterol uptake, indicating that the presence of both concomitant increased tracer uptake by lesioned adrenal and contralateral adrenal suppression is suggestive of adrenal hyperfunctioning adenoma. Nevertheless, adrenal planar scintigraphy shows low sensitivity for adrenal masses of <2 cm in diameter (29). The introduction of multiple-head gamma cameras with SPECT capability has improved image resolution of smaller lesions, permitting a correct diagnosis of a concordant or discordant uptake pattern (17, 18). Our results, obtained by 131I-NP-59 SPECT scintigraphy, demonstrate the diagnostic role in the adrenocortical investigations of UPT%, as a semiquantitative index of adrenal function, with the aim to stratify patients with hormonally proven secreting adenomas. Compared with ACTH and CTMD, the UPT% index shows a better capacity of differentiating between the PC-CS and SC-CS groups. In our experience, using a cutoff of 61.5%, UPT% correctly classified in the SC-CS and PC-CS groups with an overall accuracy of 90%. Obviously, an UPT% cutoff value is strictly dependent on the specific performance of the instrumentation used; thus, any institution interested in reproducing this method must perform a preliminary study to obtain its own reference values. The close observed relationship between the UPT% index and the presence of clinical symptomatology might be explained, considering that the clinical feature onset may be influenced by a variable extent and duration of subtle cortisol autonomous secretion (30).
Barzon et al. (9) demonstrated that the presence of isolated endocrine abnormalities at diagnosis (i.e., low circulating ACTH levels) has a predictive value for tumor enlargement and an autonomous adrenal function. In agreement with this recent report, our data demonstrated a negative correlation between ACTH values and the final clinical diagnosis. But, hormonal features, especially ACTH, are not able to discriminate between SC-CS and PC-CS patients (overall accuracy, 45%; P = 0.77). In other words, ACTH values are not related to the presence or absence of obesity, arterial hypertension, and NIDDM (aspecific signs).
It has been proven that adrenocortical adenomas of >30 mm in size should be considered a risk factor of progressing toward overt CS (9,10,30), which is worthy of close follow-up. In our experience, the CTMDs, negatively correlated with the ACTH values, are more sensitive than ACTH to stratify patients in SC-CS and PC-CS groups. Indeed, by a 2.81-cm cutoff CT diameter, patients were classified in the SC-CS and PC-CS groups, with an overall accuracy of 64% and with positive and negative predictive value of 64% and 67%, respectively (P < 0.04).
Tauchmanovà et al. (31) recently demonstrated that a chronic mild endogenous cortisol excess may have important systemic effects on the human body: Indeed, an increased cardiovascular risk profile, similar to that described in overt CS, is present in PC-CS. Although surgical treatment of cortisol excess is reserved only for those patients with overt hormone hyperproduction, there is evidence that hypertension, BMI, and hyperglycemia improved in PC-CS patients who were treated surgically (10,32).
In conclusion, hormonal evaluation (ACTH) is mandatory to determine the functional state of a CT incidentally discovered adrenal mass, but a tomographic quantitative evaluation of iodocholesterol uptake is useful to identify patients at risk of developing an overt hyperproduction of glucocoticoids.
CONCLUSION
According to the initial results of our study, the use of tomographic acquisition together with a semiquantitative analysis of acquired data appears to be a valuable approach to identify and functionally characterize incidentally discovered clinically silent adrenal masses, especially small and partially superimposed on both liver and colon hyperactivity. Use of the proposed semiquantitative approach associated with both laboratory screening for cortisol production and CTMD measurement seems able to increase the clinical diagnosis accuracy of the PC-CS. This approach could be used in the follow-up of adrenal masses function, every time hormonal or clinical features are suggestive of adrenocortical hyperfunction even if the CTMD measure is not sensibly growing. The effective clinical availability of the proposed UPT% index as a new diagnostic factor should be proven after a long-term clinical follow-up of almost 3 y. Once a significant relationship between the degree of uptake and the clinical evaluation of the adrenocortical dysfunction is proven, the UPT% index will be looked upon as an adrenal hyperfunction risk factor.
Footnotes
Received Oct. 25, 2002; revision accepted Mar. 5, 2003.
For correspondence or reprints contact: Alessio Imperiale, MD, Nuclear Medicine Unit, Department of Clinical Pathophysiology, University of Florence, Viale Morgagni 85, 50134 Florence, Italy.
E-mail: a.imperiale{at}dfc.unifi.it




{kind=link}
{kind=link}