


Abstract
The purpose of this study was to determine, with a rodent tumor model, if microelectrode measurements of unmodulated tumor oxygenation predict for the avidity of hypoxic markers to tumor tissue. Methods: The rapidly growing, anaplastic variant of the Dunning rat prostate carcinoma cell line (R3327-AT) was implanted subcutaneously on the upper backs of Fischer X Copenhagen rats. Approximately 100 measurements of Po2 were obtained from tumors of 5–10 g in animals that were restrained and then subjected to different anesthetic procedures. Values of median Po2 (in mm Hg) and percentage of measurements <5 mm Hg obtained from individual tumors were used to define tumor oxygenation status. The radiodiagnostic hypoxic markers β-d-iodinated azomycin galactopyranoside (IAZGP) and [99mTc]HL-91 were simultaneously administered to 26 animals whose tumor oxygen levels had been measured. Six hours after marker administration, the animals were killed; tumor, blood, and muscle tissues were sampled; and percentage injected dose per gram (%ID/g*), tumor/blood ratio (T/B), and tumor/muscle ratio (T/M) parameters were determined. Parameters of marker avidity to individual tumors were linearly correlated with microelectrode measurements of tumor oxygenation to determine the significance of inverse associations. Results: The median Po2 of 41 tumors varied from 2.0 to 20.9 mm Hg, with an average value of 7.5 ± 1.4 mm Hg. Six tumors had unusually high values; that is, >10 mm Hg, and when these were excluded from the analysis, the average median Po2 of the remaining 35 was 4.3 ± 0.7 mm Hg. When electrode measurements of tumor oxygenation were obtained under conditions of halothane anesthesia with the animals breathing O2, carbogen, or air, median Po2 values increased significantly (P = 0.001). When animals were deeply anesthetized by intraperitoneal injection of ketamine-xylazine, median Po2 values were not significantly different (P = 0.13) from those obtained while the animals were restrained and breathing air. There was no inverse correlation of significance between the electrode measurements of median Po2 and the avidity of β-d-IAZGP nor [99mTc]HL-91 in this tumor model. The range of median Po2 values in these tumors was at least 3 mm Hg, and the range of hypoxic marker avidity was less than twofold. Conclusion: These data demonstrate that microelectrode measurements of rat tumor oxygenation did not correlate with the avidity of the two hypoxic markers, at least in this tumor model. The larger dynamic range of tumor oxygen measurements obtained with microelectrodes might be biased to low values by their necrotic fractions, the zones within solid tumors that contain dead cells and debris that will not be labeled by bioreducible hypoxic markers. Hypoxic marker avidity to individual tumors will have to be validated by other assays that can predict for their radiosensitivity.
The oxygenation status of human tumors is an important factor for predicting tumor response and cure, especially after treatment by fractionated radiotherapy, but it cannot be routinely measured by current techniques (1). The presence of hypoxic zones within solid tumors has been shown to be extremely heterogeneous, both within and between different tumors (2,3). Over the past 10 y, several techniques for estimating tumor hypoxic fractions (HFs) and radioresistance have been developed and tested (4–9). The Eppendorf microelectrode technique has produced significant correlations between low values of tumor oxygenation and treatment failure after radiation and combination therapies (10–13). Our laboratory proposed a noninvasive technique for measuring tumor hypoxia with bioreducible markers whose avidity to tumors could be measured by SPECT or PET imaging (14). Several radiodiagnostic methods for marking hypoxic microenvironments have been developed, and their selective avidity to tumor cells in vitro and to solid tumors in both rodents and humans was recently reviewed (15).
In the search for improved radiodiagnostic techniques for tumor hypoxia, our laboratory has now synthesized over 60 novel compounds that can be radiolabeled with 123I, iodine-124, 125I, 131I, Cu-64, Cu-67, or 99mTc for detection by nuclear medicine procedures. Preclinical research to correlate tumor marker avidity with tumor hypoxia has used two rodent tumor models with known radiobiologic HFs: EMT-6 tumors growing in scid mice and Dunning R3327-AT tumors growing in Fischer X Copenhagen rats (16,17). We proposed to validate hypoxic binding of specific radiodiagnostic markers by microelectrode measurements of tumor oxygen within the same tumors. Previous microelectrode measurements of oxygen in R3327-AT and R3327-H tumors were obtained from rats that had been deeply anesthetized with ketamine-xylazine (18). Since anesthesia significantly modulates both central and peripheral blood flow in animals (19), the logistics for obtaining hypoxic marker avidity and electrode measurements of oxygen from the same tumors were further investigated.
In this study we obtained microelectrode measurements of oxygenation from the same tumor type in animals under restrained and various anesthetized conditions. As well, correlations were made between microelectrode measurements of Po2 distribution in tumors and hypoxic marker avidity, using two different radiodiagnostic markers. The data demonstrated that the dynamic range of median Po2 values obtained with electrodes and marker avidity as determined by %ID/g* or T/B and T/M are different. These assays measured different aspects of tumor physiology and oxygenation that were found not to correlate, at least for this rodent tumor model. This study demonstrated an inherent risk associated with using microelectrode and possibly other measurements of tumor oxygenation for validating hypoxic marker uptake into animal and human tumors and for predicting the radioresistance of these tumors.
Materials and Methods
Animal Tumor Model
The Dunning rat prostate carcinoma cell line R3327-AT was selected for this study since its radiosensitivity to high-dose fractions (17) and several parameters of its perfusion and oxygenation (20,21) had been measured. Fragments (8–10 mm3) were dissected from a donor tumor in sterile physiological saline and implanted under the skin on the upper backs of Fischer X Copenhagen rats. Under mild anesthesia with metophane, a small area on the upper back of each animal was shaved, sterilized, and incised to produce a slit of ∼1 cm in length. Sterile forceps were used to create a subdermal pocket in which one tumor fragment was inserted. The incision site was closed with a metal clip. Tumor tissue implanted by this procedure was palpable within 2 wk, and solid tumors reached volumes of 5–12 g in 3–4 wk. The median Po2 of R3327-AT tumors of a smaller average volume (∼2.5 mm3) was reported in a previous study to be 2.2 ± 0.3 mm Hg (18). Tumor volumes were estimated from caliper measurements of tumor diameter (17), and larger tumors of 5–12 g were selected for this study, since multiple microelectrode measurements of oxygenation were planned. All animal procedures were reviewed and approved by the Institutional Animal Care and Use Committee of the Fox Chase Cancer Center.
Eppendorf Po2 Microelectrode Measurements
The oxygenation status of individual tumors was estimated from 99–125 electrode measurements obtained along three different electrode tracts. The microelectrodes were calibrated before and after each determination of tumor oxygenation. The temperature of each tumor was obtained by an interstitial thermocouple probe and input to the histograph-associated computer to calculate absolute Po2 values. The median Po2 and percentage of measurements that were <5 mm Hg were used to define tumor oxygenation status.
Animal Restraint and Anesthesia
Animals were briefly anesthetized with metophane, the skin over the tumor area was shaved, and each animal was placed under a restraint of premolded thermal plastic (S&S Parscientific), a material commonly used in the radiation oncology clinic. This restraining mesh was screwed down to a wooden board on which the animal was positioned, and a small slit was made in the skin over the tumor after applying local anesthesia. The animals required about 10 min to wake up, resume normal respiration rates, and grow accustomed to the restraints. After this time, the first determination of tumor oxygenation was made by acquiring multiple electrode measurements. Each animal was then lightly anesthetized using a Fluorotech vaporizer made by Veterinary Anesthesia Systems Co. (VASCO) that mixed halothane vapor with a specified gas. Oxygen, carbogen, and air were sequentially transported to the animal’s anesthetic mask. After 5 min for respiratory equilibrium with each gas, another measurement of tumor oxygenation was obtained with microelectrodes guided along tumor tracts separated by at least 0.5 cm from previous tracts. When animals were anesthetized with halothane combined with oxygen or carbogen, they maintained a normal respiratory rate whereas when animals breathed halothane mixed with air, they exhibited moderate hyperventilation. After these three different measurements of tumor oxygenation were obtained under mild anesthesia, the animals were allowed to recover before an intraperitoneal injection of 0.8 mg of ketamine-xylazine per kg. Twenty minutes later, when deep anesthesia was achieved, another measurement of tumor oxygenation was obtained. Three of the 15 animals treated on this protocol did not survive the final ketamine-xylazine anesthesia, and, consequently, the analyses of oxygen levels for this condition are based on only 12 datasets. For reasons discussed below, this study indicated that Eppendorf microelectrode measurements of tumor oxygenation obtained from restrained animals were most appropriate for correlation with measurements of tumor hypoxia by radiodiagnostic methods.
Radiolabeled Hypoxic Markers
β-d-Iodinated azomycin galactopyranoside (β-d-IAZGP) was locally synthesized and radiolabeled with 125I by procedures that were previously described (22). Radiochemical purity was measured by a thin-layer chromatography (TLC)/autoradiography procedure (22). Two different preparations of 1.16 and 8.42 GBq of specific activity per millimolar concentration were used on different days. This marker contains the bioreducible moiety 2-nitroimidazole and exhibits improved hypoxia-marking properties in vivo relative to β-d-IAZA. This was attributed to its higher water solubility and faster clearance from normal tissues, mainly by renal mechanisms (15,23). It was prepared in sterile physiological saline, and ∼100 kBq were injected intraperitoneally immediately after the microelectrode procedure had been performed on restrained animals.
The ligand HL-91 (PROGNOX) was generously provided in commercial kits by Nycomed Amersham and radiolabeled with 99mTc by their recommended procedures (Amersham, Buckinghamshire, England). This hypoxia marker does not contain a 2-nitroimidazole moiety. Most of the 99mTc (96%–99%) became linked to HL-91 in the three different marker preparations used on the three different days of these experiments. The chelation of 99mTc with the ligand was quantified by two chromatographic procedures developed by Nycomed Amersham (HL-91 kit procedures [Amersham, Buckinghamshire, England]). [99mTc]HL-91 was injected intravenously immediately before β-d-IAZGP was administered intraperitoneally to each animal.
About 6 h after marker injection, the animals were killed. Their tumors, muscle, and blood were sampled and counted in the dual-channel mode of our γ-spectrometer (Packard Cobra II). From these quantitative measurements of tissue radioactivity, the %ID/g* of each marker was obtained, and T/B and T/M were computed. All specific activities were normalized to a standard rat weight of 350 g(*).
Statistical Analyses
The measurements of oxygenation status of individual tumors in animals that were subjected to restraint and various anesthetics were analyzed using the paired Student t test, as were the differences in the means of these similarly treated groups. Correlations between the median Po2 of individual tumors and parameters of hypoxic marker avidity used the Pearson Product Moment correlation. P values of 0.05 and less were considered to indicate significant differences.
Results
Our research strategy for validating novel nuclear medicine markers of tumor oxygenation included correlations with Eppendorf microelectrode measurements. Since electrode measurements of tumor Po2 can be acquired most readily from anesthetized animals and since some anesthesia procedures had been reported to interfere with microelectrode operation and tumor radiosensitivity (24–27), we performed a preliminary study with Dunning R3327-AT tumors to determine the effect of various anesthetics on tumor Po2 measurement. Table 1 shows values of median Po2 and percentage of measurements <5 mm Hg acquired from the same tumor in restrained animals and in animals while under both mild and deep anesthesia. Each animal was restrained with commercial thermomesh material used in radiotherapy practice, which had been premolded to fit various animal sizes, and five independent determinations of tumor oxygenation were acquired. The tumor weights in the first six animals were estimated from external caliper measurements, while the tumor weights for the remainder of the animals were measured after excision. The average value of median Po2 (±SE) obtained from air-breathing, restrained animals was 7.5 ± 1.4 mm Hg (n = 15). The mean value of the percentage of measurements <5 mm Hg (±SE) was 44.6 ± 8.6. The mean values of median Po2 obtained from the same tumors in animals under mild anesthesia with halothane significantly increased for animals breathing oxygen, carbogen, or air (P = 0.001–0.005). As well, the mean values of the percentage of measurements <5 mm Hg decreased significantly in each case (P = 0.0001–0.001). These data clearly demonstrated that mild anesthesia with halothane-gas mixtures resulted in significantly higher values of tumor oxygenation parameters compared to those obtained from air-breathing animals. When animals were deeply anesthetized with ketamine-xylazine, the mean value of their median Po2 was 5.1 ± 0.05, and the mean percent <5 mm Hg was 38.9 ± 7.7. Under conditions of deep anesthesia, tumor oxygenation parameters were not significantly different from those obtained from unanesthetized, restrained animals (median Po2, P = 0.13; percentage <5 mm Hg, P = 0.62).
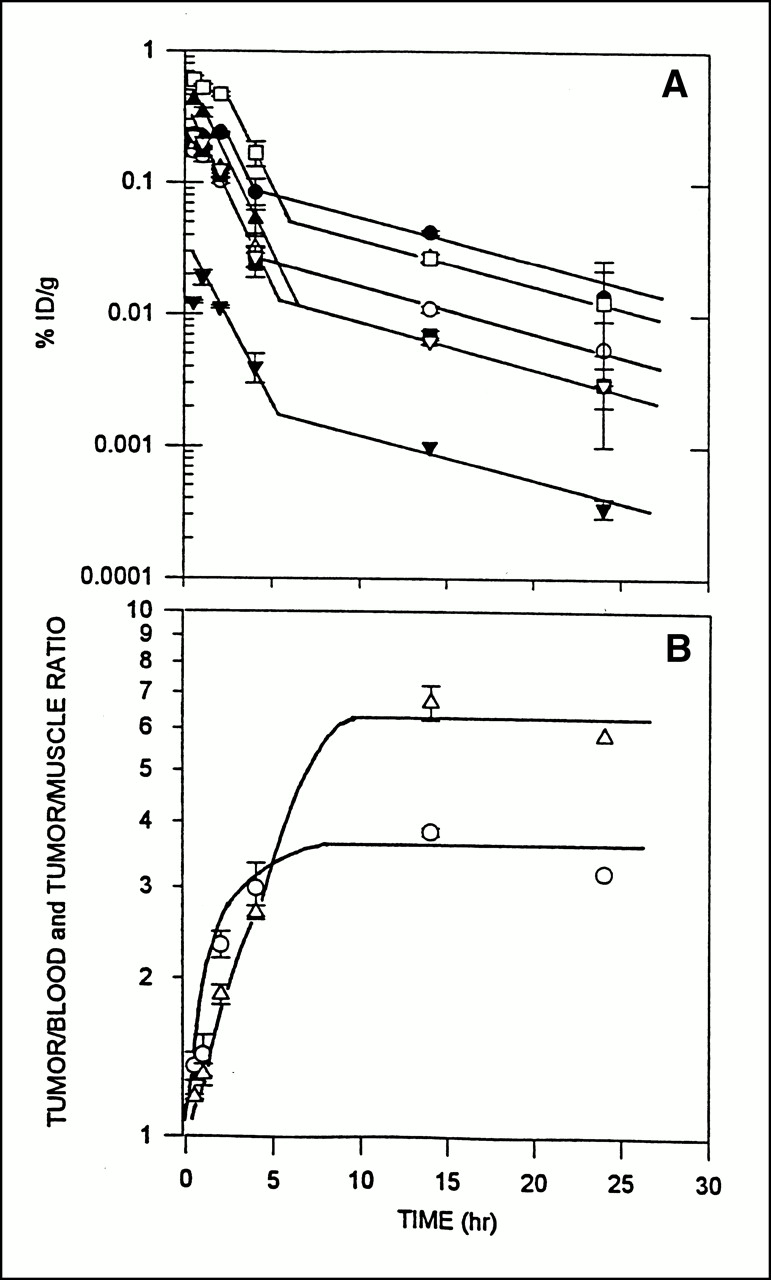
Effect of Various Anesthetic Procedures on Eppendorf Microelectrode Measurements Obtained from Individual Dunning R3327-AT Tumors*
Previous microelectrode measurements of oxygen in smaller R3327-AT tumors in deeply anesthetized rats had yielded lower average values of median Po2 (18). For this reason, tumors that exhibit median Po2 values of 10 mm Hg or more in air-breathing, restrained animals might be anomalous. When the means of median Po2 and percentage <5 mm Hg were computed for the 10 animals whose tumors had median Po2 values of <10 mm Hg (Table 1), similar conclusions were obtained. The tumor oxygen parameters from deeply anesthetized animals were similar to those obtained from air-breathing, restrained animals but significantly lower than those obtained from animals anesthetized with halothane and various gases. Since the detection of tumor HFs by nuclear medicine markers is a “pharmacologic” procedure requiring rapid biodistribution and excretion (15), it was deemed important to obtain “tumor oxygenation” measurements by both microelectrode and radiodiagnostic procedures from minimally perturbed animals at about the same time. For this reason, Eppendorf electrode measurements were acquired from air-breathing, restrained animals immediately before the administration of the two nuclear medicine markers of hypoxia. The bioreduction and binding of β-d-IAZGP to viable hypoxic tumor cells exhibit first-order kinetics with marker concentrations (23). Figures 1A and B show the biodistribution, clearance kinetics, and T/B and T/M for β-d-IAZGP in R3327-AT tumor-bearing rats. These data indicate that microelectrode measurements obtained from tumors in air-breathing, restrained animals immediately before the administration of bioreducible hypoxic markers would sample tumor microenvironments close in time (within 2–3 h) to those when the markers are at maximal concentration in the tumor tissue. The assessment of marker radioactivity retained in tumor and normal tissue samples at 6 h and longer after administration allows for the excretion of unbound β-d-IAZGP and the development of nearly maximal T/Bs and T/Ms (Fig. 1B). Complete pharmacokinetic studies of [99mTc]HL-91 biodistribution and clearance from R3327-AT tumor-bearing rats were not performed. Significant differences in the pharmacokinetics of these two markers had been observed with EMT-6 tumor-bearing scid mice (unpublished data). [99mTc]HL-91, when administered intravenously, was rapidly distributed (within 20 min) to tumor and normal tissues at unique specific activities and was cleared from all tissues with a half-life of 10–12 h, similar to the pharmacokinetics of other 99mTc-labeled markers (28). Consequently, we assumed that the retention of this marker in R3327-AT tumors 6 h after administration should yield maximal T/Bs and T/Ms.

(A) %ID/g* of 131I delivered intravenously via β-d-IAZGP in various tissues at various times after administration (n = 3). Symbols represent R3327-AT tumor (•), liver (▴), kidney (□), blood (○), spleen (▪), lungs (>), muscle (▵), and brain (t). At least 90% of the marker is renally excreted over first 5–6 h followed by much slower hepatobiliary excretion. (B) T/B (○) and T/M (▵) ratios of tissue-specific activities from data in A. Maximum sensitivity of this marker technique is expressed after 6 h.
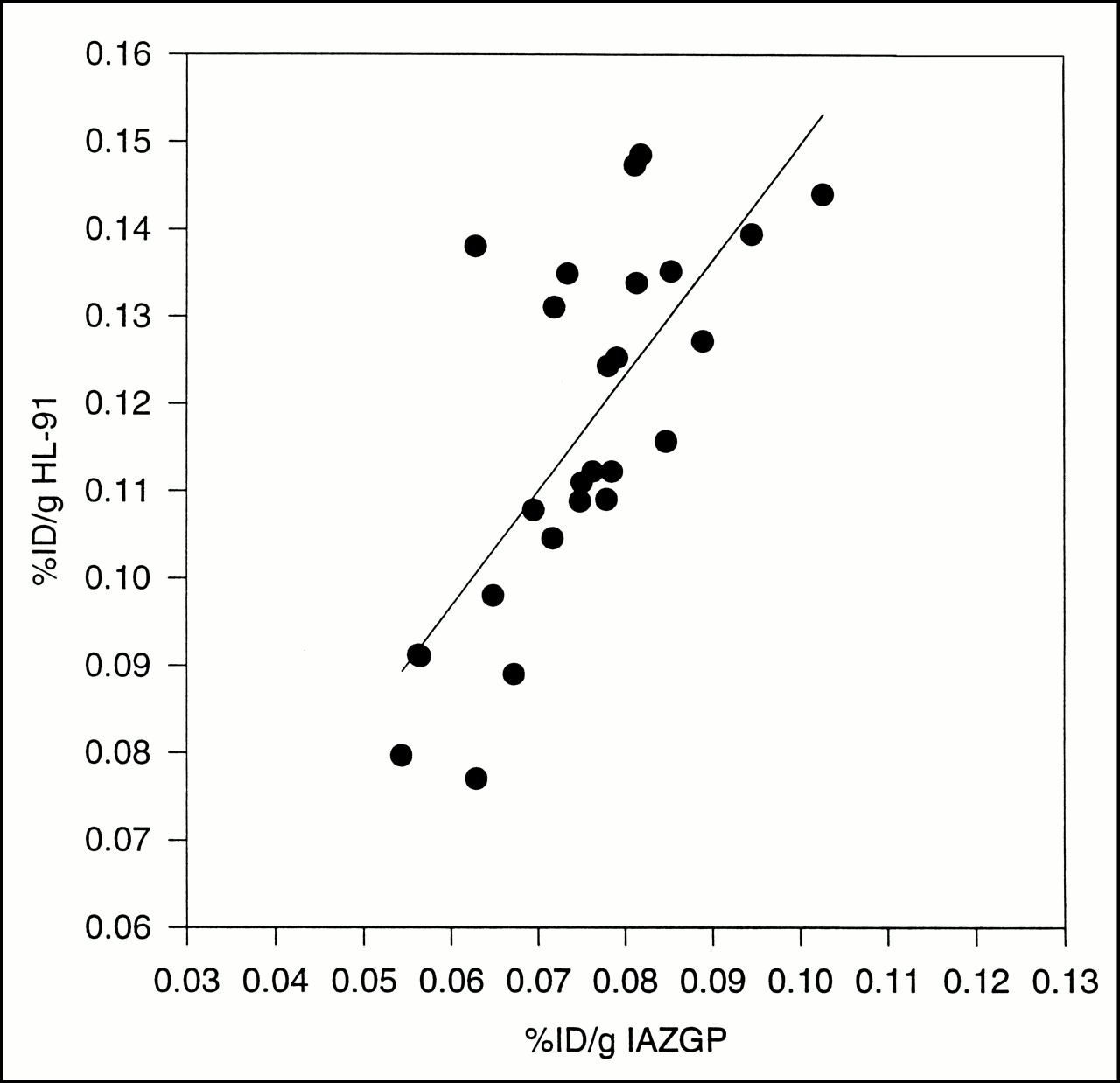
Table 2 shows the median Po2 values obtained from tumors in 26 different animals to which the hypoxic markers β-d-IAZGP and [99mTc]HL-91 were administered. The mean weight of tumors in this study was 7.8 ± 0.45 g, and the mean value of their median Po2 was 5.1 ± 0.51. This range of tumor oxygenation was similar to that reported in the study described in Table 2, with the exception that only one tumor had a median Po2 of >10 mm Hg. The microelectrode procedure detected at least a threefold range in median Po2, and Figure 2 shows the distribution of this parameter obtained from tumors in air-breathing, restrained animals shown in Tables 1 and 2. Five of the six tumors that had median Po2 values of >10 mm Hg were in the anesthetic study, and, consequently, correlations with lower–hypoxic-marker avidity were not possible. It is interesting to note that the tumor with the highest median Po2 in Table 2 did in fact have the lowest %ID/g* of β-d-IAZGP, but that was not the case for [99mTc]HL-91. Figure 3 shows a plot of median Po2 versus hypoxic marker specific activity in R3327-AT tumors for β-d-IAZGP and [99mTc]HL-91. It is apparent that no significant inverse correlation between these parameters was found. Also, when tumor median Po2 values were plotted against T/B and T/M values for both hypoxic markers, no significant inverse correlations between these parameters were observed. And yet, when the avidity of β-d-IAZGP and [99mTc]HL-91 to individual tumors was investigated, a good linear correlation (coefficient = 0.78) was observed (Fig. 4). This result suggests that the mechanisms for delivery and uptake of the bioreducible marker β-d-IAZGP in these tumors may be similar to that of HL-91. The percentage of injected HL-91 that became associated with R3327-AT tumors 6 h after administration was, on average, about 60% higher than that of β-d-IAZGP.
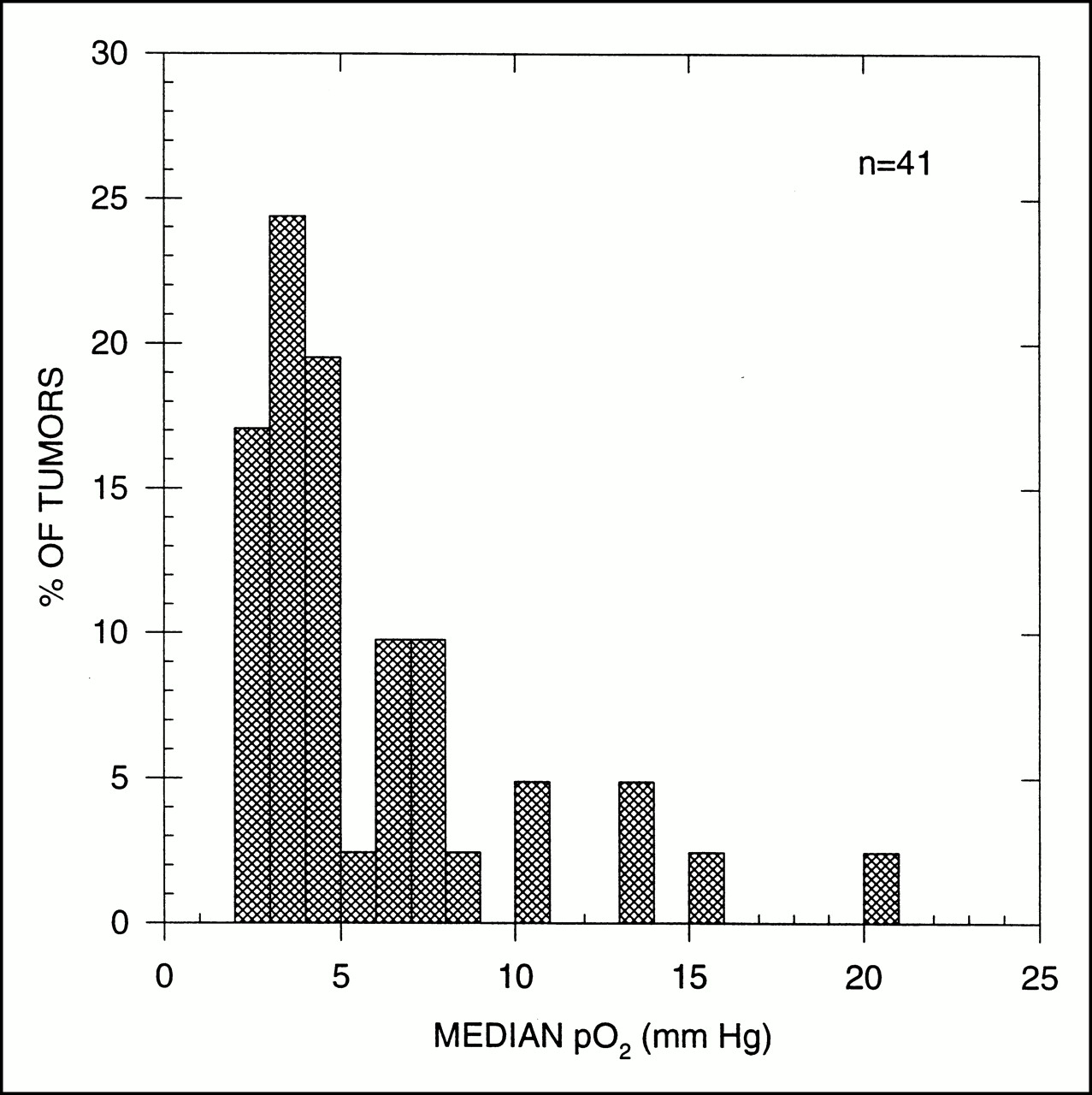
Frequency distribution of median Po2 values obtained from 41 R3327-AT tumors.

Median Po2 of individual R3327-AT tumors versus specific activity of tumor β-d-IAZGP (○) and [99mTc]HL-91 (•) measured 6 h after administration (n = 26).
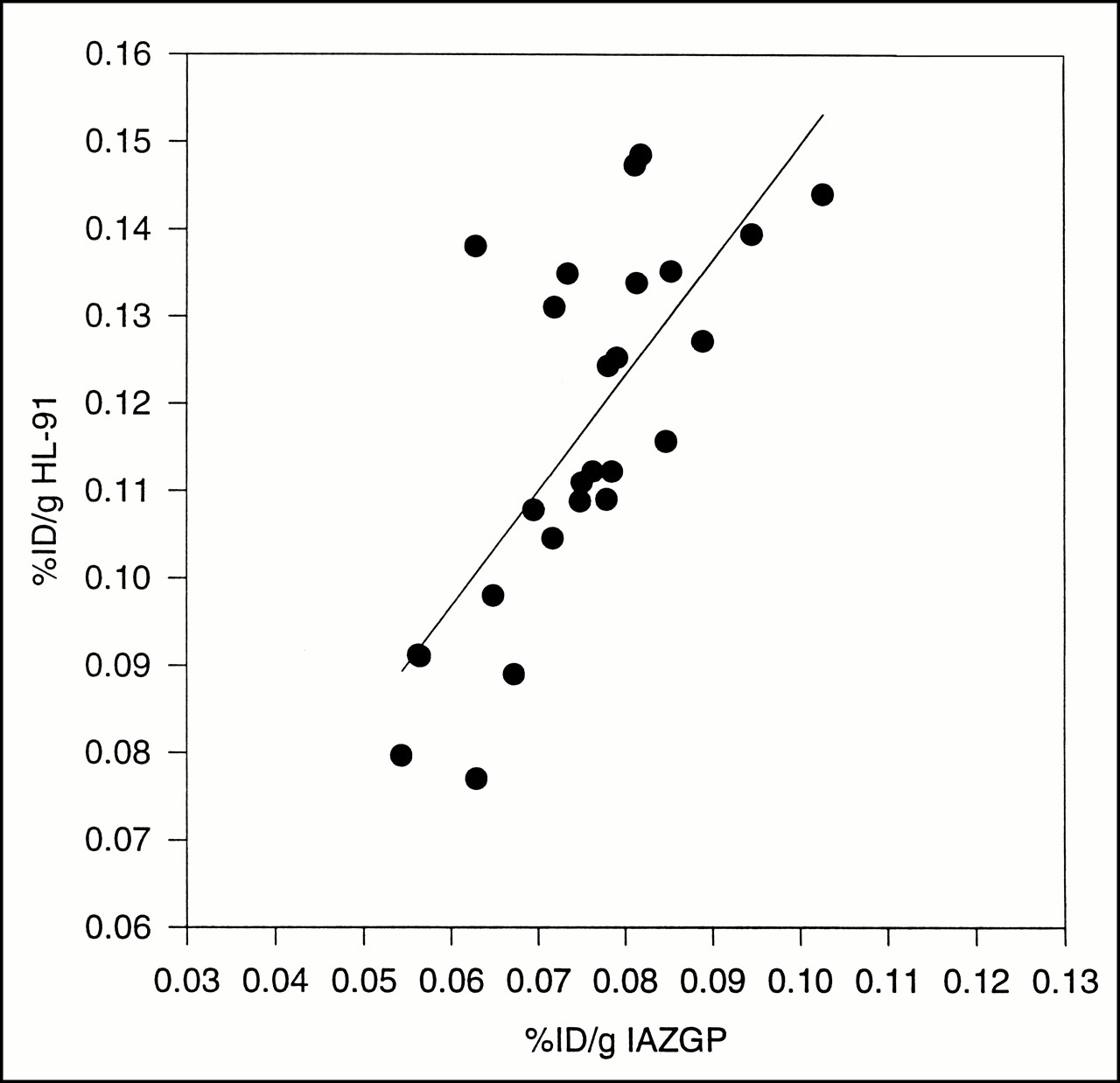
%ID/g* [99mTc]HL-91 versus %ID/g* β-d-IAZGP in individual tumors 6 h after administration.
Measurements of Median Po2 by Eppendorf Microelectrodes and Retention of Hypoxic Markers, Gb-d-IAZGP and [99mTc]HL-91, in Same Dunning R3327-AT Tumors 6 Hours After Administration to Tumor-Bearing Animals
Discussion
Previous studies have reported that the polarography associated with microelectrode measurements of Po2 is adversely affected by the presence of halothane (24,25). The data in Table 1 confirm that this was the case for the oxygenation status of R3327-AT tumors growing in Fischer X Copenhagen rats. This result indicated that assays of the correlations between radiodiagnostic hypoxia marker avidity and direct microelectrode measurements of tumor oxygenation should not use mild anesthesia with halothane-gas mixtures since anomalous (higher) electrode measurements are to be expected. Our previously reported microelectrode measurements of tumor oxygenation in R3327-AT tumors were obtained from animals that had been deeply anesthetized with ketamine-xylazine (18). While microelectrode measurements are most easily acquired from animals that have been immobilized by anesthesia, ketamine-xylazine has been known to significantly reduce the peripheral blood flow required to distribute radiolabeled markers to tumor and animal tissues, and, more importantly, it alters the clearance rate of unbound marker by renal and hepatobiliary excretion mechanisms. Another complication associated with correlations between different tumor oxygenation measurements is that the radiobiologic HF consists of both chronically hypoxic and acutely hypoxic cells (29). Studies with β-d-IAZGP labeled with two different iodine radioisotopes have shown that the estimates of HFs by this technique can vary significantly over a period of 3 h in some tumors (30). It was then concluded that the best procedure for obtaining both microelectrode and hypoxic marker measurements of tumor oxygenation from the same tumor at approximately the same time would be the acquisition of Po2 measurements from tumors in animals that were restrained and air-breathing, followed immediately by the administration of hypoxic markers. In this manner, the majority of metabolic linkages of hypoxic markers to tumor tissue would occur within 2 h of the electrode measurement, the time when marker concentrations are at their maximum in tissues. The marker kinetic data in Figure 1 show that this was true for β-d-IAZGP. Those data also show that at 6 h and longer after administration, the radioactivity of labeled β-d-IAZGP was highest in tumor tissue and that T/B and T/M reached maximum plateaus. Consequently, our protocol acquired microelectrode measurements of tumor oxygenation immediately before the administration of [99mTc]HL-91 and β-d-IAZGP.
The mean value of electrode measurements of median Po2 obtained from the R3327-AT tumors in this study was significantly higher than that obtained 4 y earlier from tumors of smaller volume (18). The median Po2 values shown in Figure 2 can be described in three groups, one group of 25 tumors with a mean value of median Po2 of ∼3.5 mm Hg, a group of 10 tumors whose mean value of median Po2 was 7 mm Hg, and 6 tumors whose median Po2 values were >10 mm Hg. The basis for the wider variation in median Po2 values for the larger tumors used in this study is not known, although there was no indication that faulty electrode operation had occurred. Although five of the six tumors with these higher values of median Po2 were from the anesthesia study, the measurements were acquired before exposure of the animals to halothane-gas mixtures that resulted in anomalously higher values of tumor oxygenation. It is interesting that, when the five animals whose tumors showed median Po2 values of >10 mm Hg were anesthetized with ketamine-xylazine (Table 1), tumor oxygen levels fell to near the restrained values, in every case. The differentiation status of tumors in this study was not individually evaluated. It could be that the tumors with the higher median Po2 values were moderately to well differentiated, a phenotype that we previously showed to exhibit higher oxygen levels (18). The six tumors with the higher oxygen levels had grown to their respective volumes in times similar to the other tumors, a characteristic that is not consistent with the slower growth rate of moderately to well-differentiated Dunning prostate carcinomas (17).
It seemed apparent that there is no significant inverse correlation between median Po2 values obtained from individual tumors and the avidity of β-d-IAZGP nor [99mTc]HL-91. Eppendorf microelectrode measurements of the low oxygen levels in these Dunning R3327-AT tumors did not correlate with the avidity of β-d-IAZGP nor HL-91. While the values of median Po2 in Table 2 cover at least a threefold greater range, the range of parameters that defined hypoxic marker avidity in the same tumors was only 1.5–1.8. These data suggest that the variation in HFs in R3327-AT tumors of this volume was too small to demonstrate significant inverse correlations between microelectrode and hypoxic marker parameters. Furthermore, the two techniques measure and emphasize quite different tumor compartments. The microelectrode samples Po2 values along tracts within both viable and necrotic tumor zones and, for R3327-AT tumors of this volume, Po2 distributions may be skewed to the very low values obtained from necrotic and dead cells. On the other hand, the hypoxic markers require viable cells at low oxygen tension for their bioreduction and linkage to cell molecules (14). Consequently, hypoxic markers sample mainly chronic and acutely hypoxic tumor cells that are viable and from which tumor regrowth may occur after reoxygenation. It is the avidities of these hypoxic markers that suggest a narrow range of HFs in these tumors. But when the avidity of β-d-IAZGP was compared to that of [99mTc]HL-91 in the same tumors, a reasonable correlation was found. This result suggests that both radiodiagnostic markers may be marking similar microenvironments within these tumors. In other studies, where tumor oxygen levels were modulated by nicotinamide and carbogen, both β-d-IAZGP (31) and [99mTc]HL-91 (31) were shown to measure reduced tumor HFs.
The results of this study are instructive for both the preclinical evaluation of radiodiagnostic markers of tumor hypoxia and for their clinical validation. Our research will now use some radiosensitivity assay of cells released from individual tumors to validate hypoxic marker avidity to tumors. Again, the sequencing of these two assays will be critical. Initially, a hypoxic marker will be administered to animals and allowed to label hypoxic cells in their tumors for 2–6 h before tumor irradiation with an acute dose of 20 Gy. Tumors will be immediately resected, chopped, and mixed, and independent assays of hypoxic marker avidity and in vitro clonogenicity will be performed. Previous studies using this protocol with EMT-6 tumors growing in scid mice showed a significant correlation between β-d-IAZGP avidity and the intrinsic tumor cell radiosensitivity of tumors (23). Whether the avidity of these hypoxic markers to these rat tumors in air-breathing animals can predict for their radioresponse remains to be demonstrated.
For validation studies of clinical hypoxic markers in cancer patients, microelectrode measurements could still be an important tool. The dynamic range of median Po2 values obtained from cervical, head and neck, and prostate carcinomas is much larger (32,33) than the range of microelectrode measurements of median Po2 obtained from tumors in air-breathing rodents (34–36). For prostate cancers of Gleason scores 6 and 7, median Po2 values ranged from ∼1 up to 20–25 mm Hg (33). While correlations between hypoxic marker avidity and an independent measure of tumor oxygenation would be useful, the ultimate radiodiagnostic analyses of tumor HFs will require clinical studies for correlation with tumor radioresistance. A nuclear medicine marker that could accurately predict for tumor hypoxia and, in particular, treatment resistance would find an important role in tumor diagnosis and for defining a subpopulation of patients that would benefit from hypoxia-targeted therapies.
Conclusion
These data show that the uptake and retention of β-d-IAZGP and [99mTc]HL-91 in individual anaplastic Dunning rat prostate carcinomas correlate significantly. This result has mechanistic consequences since β-d-IAZGP contains the “well-behaved,” bioreducible moiety 2-nitroimidazole, while [99mTc]HL-91 does not. Tumor Po2 measurements obtained with microelectrodes did not correlate significantly with the degree of tumor hypoxia measured by either radiolabeled marker. This study confirmed that anesthesia with halothane significantly alters tumor oxygen measurements obtained with microelectrodes. We conclude that the validation of hypoxia marker uptake into individual tumors will require other assays of tumor oxygenation, such as quantitative measures of tumor radioresistance.
Acknowledgments
The authors thank Barbara Edwards, George Brauers, and William Simonich of Nycomed Amersham PLC for their support and encouragement during this study. The assistance of Pat Bateman in preparing the manuscript is appreciated. Nycomed Amersham PLC generously supplied the kits of HL-91 (PROGNOX) for this study along with radiolabeling procedures. Financial support for this research was provided by National Institutes of Health grants CA06927 and CA55893 and an appropriation from the Commonwealth of Pennsylvania.
Footnotes
Received Feb. 22, 2000; revision accepted Sep. 14, 2000.
For correspondence or reprints contact: J. Donald Chapman, PhD, Department of Radiation Oncology, Fox Chase Cancer Research Center, 7701 Burholme Ave., Philadelphia, PA 19111.
REFERENCES
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Prognostic Impact of Hypoxia Imaging with 18F-Misonidazole PET in Non-Small Cell Lung Cancer and Head and Neck Cancer Before Radiotherapy
- Hypoxia-Specific Tumor Imaging with 18F-Fluoroazomycin Arabinoside
- The Synthesis and Radiolabeling of 2-Nitroimidazole Derivatives of Cyclam and Their Preclinical Evaluation as Positive Markers of Tumor Hypoxia
- On Measuring Hypoxia in Individual Tumors with Radiolabeled Agents