


Abstract
Recurrences after resection of hepatocellular carcinoma are frequent. A single postoperative injection of 131I-labeled lipiodol in the hepatic artery was shown in 1999 by Lau and colleagues to be an effective adjuvant treatment, and those results were strengthened by our experience with a case-control study, reported in 2003. The goal of this paper is to update the 2003 results for a minimal follow-up of 5 y. Methods: Between January 1999 and September 2001, 38 patients were given an adjuvant postoperative intraarterial injection of 131I-lipiodol and were matched (for Okuda group and tumor size) with 38 patients who had undergone resection between January 1997 and January 1999 without postoperative treatment. The 2 groups were similar. Results: There were 28 recurrences in the control group and 22 in the 131I-lipiodol group (not statistically significant), and the mean time of recurrence was 21 and 26.5 mo, respectively, after surgery (statistically significant). The number of recurrences was lower in the first 2 y in the 131I-lipiodol group (statistically significant). Disease-free survival was better (P < 0.03) in the 131I-lipiodol group than in the control group (2-, 3-, and 5-y rates [±95% confidence interval] of 77% ± 7%, 63% ± 8%, and 42% ± 8.5%, respectively, for the 131I-lipiodol group vs. 47% ± 8%, 34% ± 8%, and 27% ± 8%, respectively, for the control group). Overall survival did not differ between the 2 groups (P = 0.09), even though there was a trend toward better survival in the 131I-lipiodol group (2-, 3-, and 5-y rates of 76% ± 7%, 68% ± 7.5%, and 51% ± 9%, respectively, vs. 68% ± 7.5%, 53% ± 8%, and 39% ± 8%, respectively, in the control group). Conclusion: With a longer follow-up, the results of this retrospective case-control study still favor a single postoperative injection of 131I-lipiodol. These retrospective findings point out the need for a large-scale, prospective, randomized study.
The recurrence rate after potentially curative treatments in patients with hepatocellular carcinoma (HCC) is about 40%–60% at 2 y and 80% at 5 y (1–5). Intrahepatic recurrence can represent either de novo tumor formation in a cirrhotic liver or intrahepatic metastasis of a clonally identical neoplasm. HCC is well suited to treatment with locoregional therapy, because the disease tends to stay within the liver until advanced. The treatment of choice in this setting is local. Among the few positive randomized, controlled trials in HCC therapy (6–8), a small study demonstrated the efficacy of a single postoperative intraarterial injection of 131I-labeled lipiodol (7). This treatment (1,850 MBq of 131I-lipiodol) decreased the recurrence rate and improved overall and recurrence-free survival. After the publication of that series, we decided in 1999 to propose this treatment for patients undergoing complete surgical resection for HCC. In 2003, we reported our results in a case-control study comparing the outcome in 2 populations treated surgically, matched for tumor size and Okuda class, and differing only by the postoperative treatment (8). Surveillance was proposed for patients treated from January 1997 to January 1999, and those treated from January 1999 to September 2001 received a single postoperative injection of 131I-lipiodol (2.4 GBq) between the eighth and 12th postoperative weeks. In that study, we found an improved recurrence-free and overall survival, but the mean follow-up was short (15 mo in the treated group). We report here our final results for a minimal follow-up of 5 y in all patients.
MATERIALS AND METHODS
The study setup was reported previously (8–11). Briefly, 38 patients with a good clinical status (World Health Organization score of 0 or 1) who had undergone a curative surgical resection (negative histologic margins and no residual lesion on intraoperative ultrasound) of histologically proven HCC between January 1999 and September 2001 and who had no contraindication (lower limb arteritis or respiratory failure) for the intraarterial hepatic injection of 131I-lipiodol received a single postoperative injection (2,400 MBq [60 mCi] of Lipiocis; CIS bio international) into the proper hepatic artery. Each patient was then isolated in a protected room for 7 d. Adjuvant therapy was given between the eighth and 12th postoperative weeks. A previous 131I-lipiodol distribution study had revealed that 131I-lipiodol concentrated mainly in the liver and the lungs, with a liver–to–liver + lung activity ratio of greater than 75% for all 3 groups of patients. 131I-Lipiodol distribution was homogeneous in normal livers and heterogeneous in cirrhotic livers. 131I-Lipiodol concentrated in the tumor with a tumor-to-nontumor activity ratio of 4.3 ± 3.6 for HCC. Consequently, 99mTc-macroaggregated albumin scanning was not required to evaluate shunting into the lungs and gastrointestinal system and to assess gastroduodenal embolization before this arterial procedure. Before discharge, CT and γ-camera imaging were performed on the seventh day after injection to, respectively, search for small tumor formations and evaluate selective or nonselective hepatic and pulmonary 131I-lipiodol retention. A standard follow-up scheme was applied (consultation every 3 mo for physical examination, α-fetoprotein assay, and abdominal ultrasound or CT). The patients and their primary care physicians were contacted during September 2006 to collect exact follow-up data; the minimum follow-up for the treated group was thus 5 y.
These 38 patients were matched 1/1 for tumor size (±2 cm) and Okuda class (12) (class by class) with 38 patients who had undergone curative surgery for HCC between January 1997 and January 1999, a period during which no adjuvant treatment was proposed. These matched controls were also free of lower-limb arteritis and respiratory failure. The general and tumor characteristics of patients are summarized in Table 1.
General and Tumor Characteristics of Patients
The classic definition of tumor recurrence was retained: either development of a hepatic tumor that was larger than 2 cm, hypervascularized, and eventually associated with clear elevation of serum α-fetoprotein levels (>250 ng/mL) or development of an extrahepatic tumor highly suggestive of metastasis. No histologic proof was required.
The 2 groups were comparable in clinical, biologic, and histologic data and had identical Cancer Liver Italian Program scores (13).
The χ2 test and Student t test were used for statistical analysis, with the Fisher exact test applied for small sample sizes. Kaplan–Meier survival curves were plotted and compared with the log-rank test. Survival was defined as starting from the date of surgery, and disease-free survival was defined as the time between surgery and diagnosis of recurrence; results are expressed along with the 95% confidence interval.
RESULTS
The patients tolerated the 131I-lipiodol injections easily. There were no early complications and, during more than 5 y of follow-up, none of the patients presented with late complications attributable to radiation. Specifically, none showed severe lung disease.
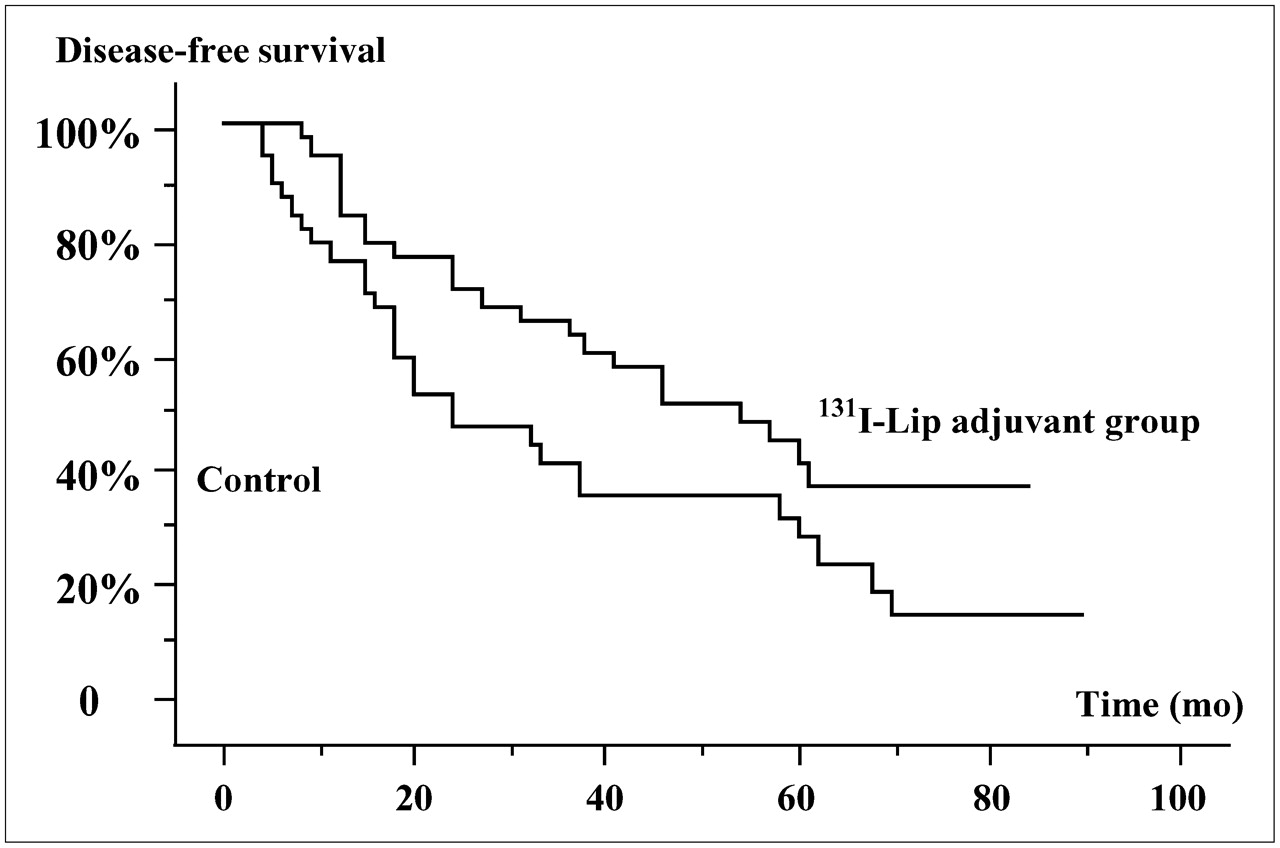
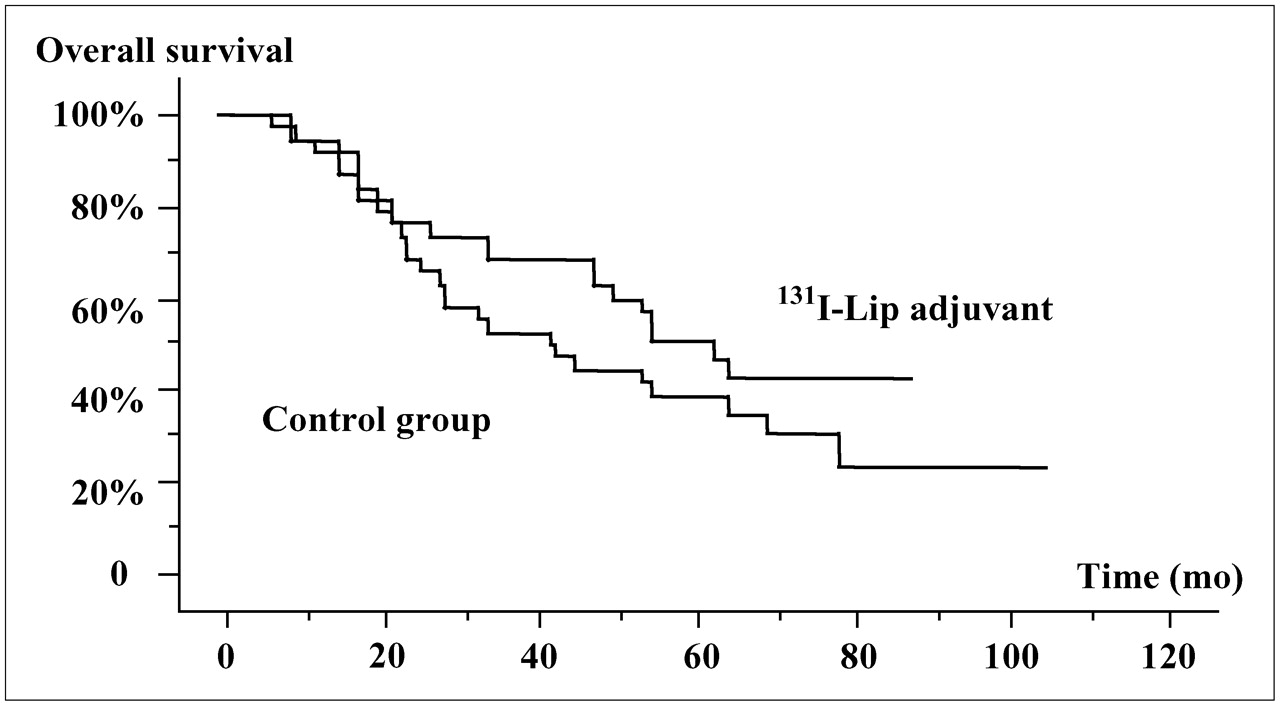
During the follow-up period, there were 28 recurrences in the control group and 22 in the 131I-lipiodol group (not statistically significant). These recurrences occurred, respectively, a mean of 21 and 26.5 mo after surgery (statistically significant). The number of recurrences was lower (statistically significant) within the first 2 y in the treated group: 15 patients in the control group versus 7 patients in the 131I-lipiodol group experienced recurrence during this period (Fig. 1). The disease-free survival curves were different between the 2 groups (P < 0.03) (Fig. 2). Two-, 3-, and 5-y disease-free survival (±95% confidence interval) was 76.9% ± 7.4%, 62.6% ± 7.9%, and 41.7% ± 8.5%, respectively, in the 131I-lipiodol adjuvant therapy group, versus 47.4% ± 8.4%, 34.4% ± 8.2%, and 27.1% ± 7.9%, respectively, in the control group without adjuvant therapy. Overall survival curves were not significantly different between the 2 groups despite a trend toward a benefit from adjuvant therapy (P = 0.09) (Fig. 3). Two-, 3-, and 5-y survival was 76.3% ± 6.9%, 68.4% ± 7.5%, and 50.9% ± 8.7%, respectively, in the 131I-lipiodol adjuvant therapy group and 68.4% ± 7.5%, 52.6% ± 8.1%, and 38.9% ± 8.2%, respectively, in the control group.
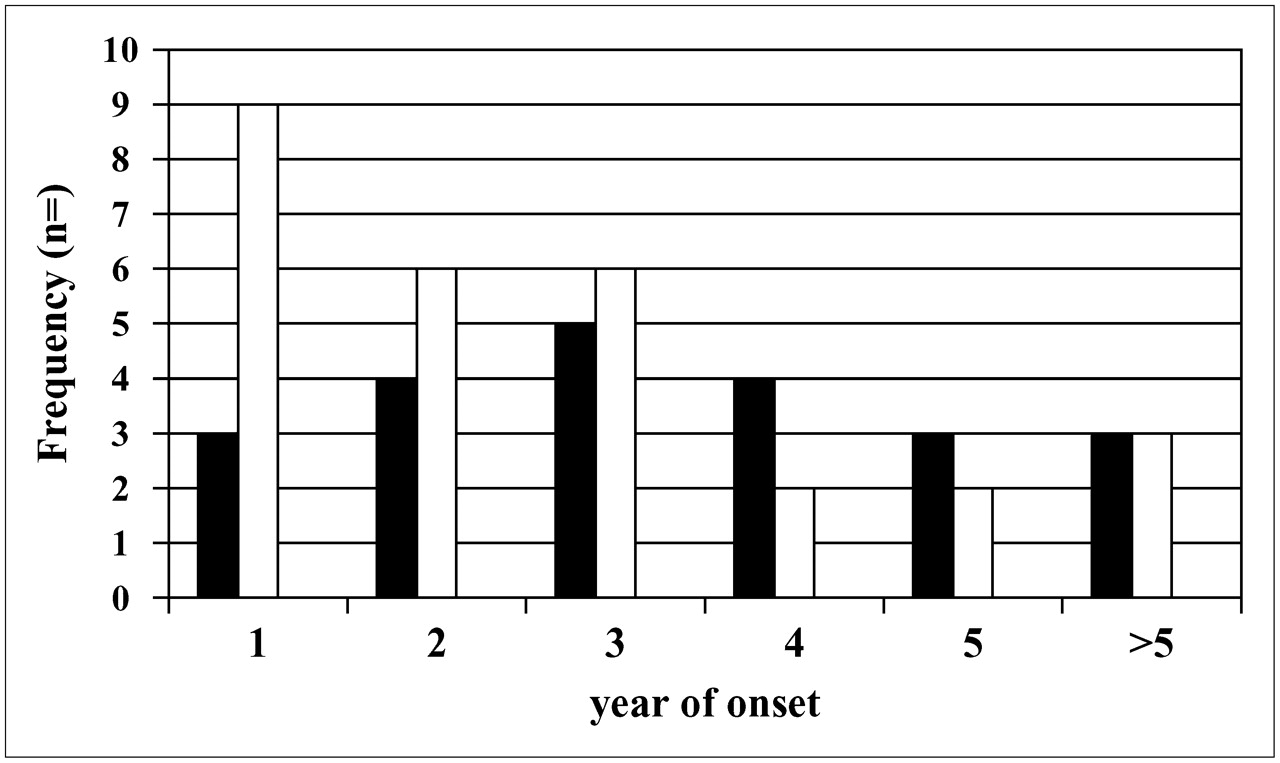
Frequency and date of onset (years) of recurrences in control group (n = 28 [white bars]) and in 131I-lipiodol group (n = 28 [black bars]).
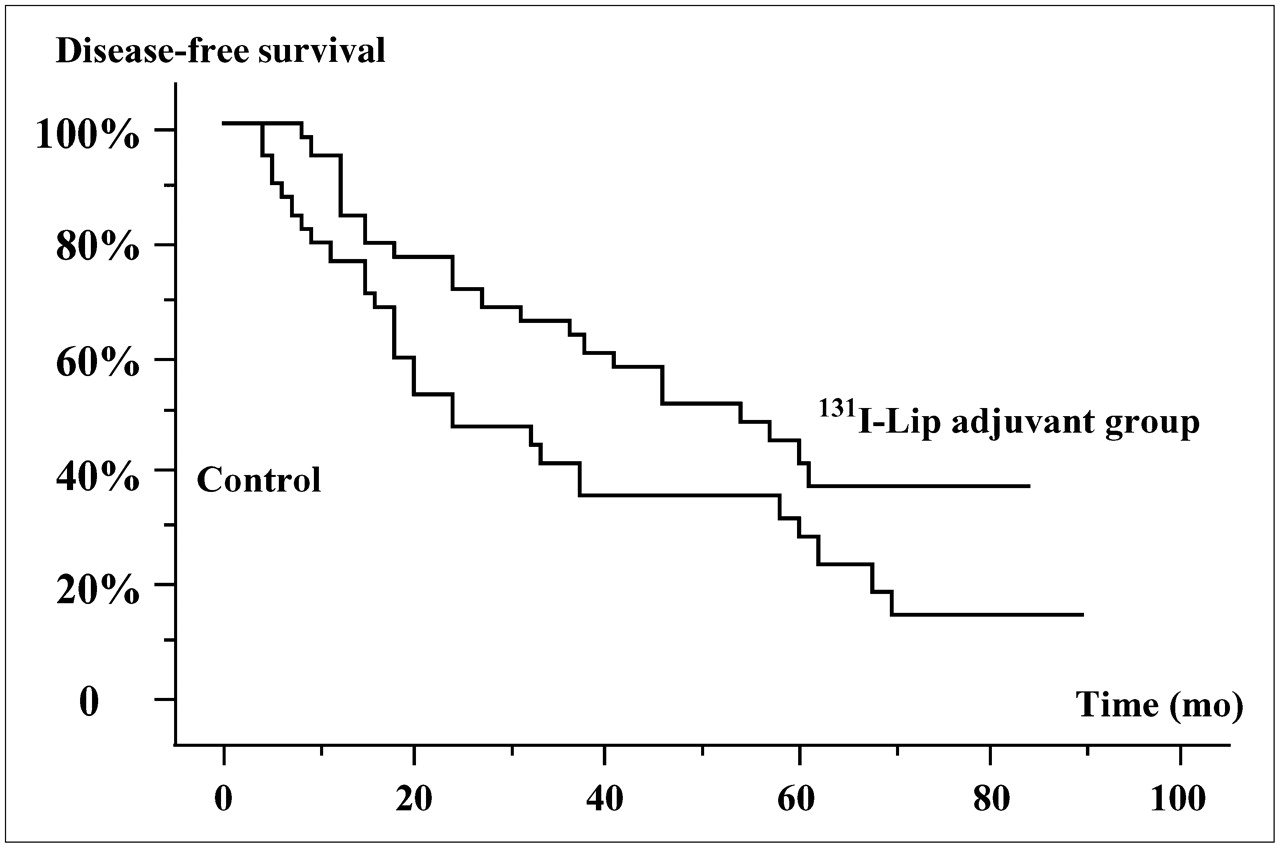
Disease-free survival by postoperative adjuvant treatment (P < 0.03). Lip = lipiodol.

Overall survival of patients receiving a single 131I-lipiodol postoperative injection or surgery alone (not statistically significant). Lip = lipiodol.
Patient outcome is summarized in Table 2. There were 20 deaths in the 131I-lipiodol group, 14 due to tumor recurrence and 6 to other causes (1 to hepatic insufficiency without tumor recurrence, 3 to cardiac failure, and 2 to other types of cancer). Half the patients were not given specific treatment for recurrence because they had multiple foci or poor liver function. In the control group, 27 patients died, 21 due to tumor recurrence and 6 to other causes (5 to liver failure or other types of cancer and 1 to suicide).
Patient Outcome
DISCUSSION
The recurrence rate after surgical resection of HCC is high, even when strict indications (very early or early Barcelona Clinic Liver Cancer stage; limiting of surgical indications to 1 small nodule in patients with good hepatic function, no hyperbilirubinemia, and normal portal pressure) are used. Currently, some preoperative procedures could increase the future remnant liver volume, and surgeons are more prone to treat large HCC tumors even in cases of cirrhosis with portal hypertension, despite a higher risk of margin invasion or of recurrence. Thus, there is clearly room for postoperative adjuvant treatment. These recurrences could be real recurrences corresponding to intrahepatic metastasis of the removed cancer, usually occurring within the first 2 y and close to the surgical margin, or second cancers caused by the natural course of the underlying cirrhosis, with an annual incidence depending on its etiology. Among cirrhotic patients free of previous HCC, the 5-y cumulative incidence of HCC is 30% in hepatitis C virus–related cirrhosis in Japan, 17% in hepatitis C virus–related cirrhosis in Europe and the United States, 15% in hepatitis B virus–related cirrhosis in Taiwan and Singapore, 10% in hepatitis B virus–related cirrhosis in Europe, and 21% in hereditary hemochromatosis (14,15). Some adjuvant treatments seem to decrease the risk of real recurrences, whereas some others decrease the risk of de novo cancer. These latter treatments include acyclic retinoids and interferon (5,6). In a recent paper, Mazzaferro et al. demonstrated the prevention of late tumor recurrences in hepatitis C virus patients receiving chemopreventive interferon (5). Treatment with retinoids gave the same results and prevented second HCC tumors after surgical resection or radiofrequency therapy (6). Systemic chemotherapy, contrary to what is observed in some other digestive cancers, did not decrease this risk (16–18). Early recurrences due to the removed cancer could be prevented by treatments delivered in the hepatic artery (19); in this setting, chemoembolization seems of interest (20).
The hepatic artery can be used to transport treatment to the HCC while sparing tumor-free hepatic tissue because the hepatic artery is the sole blood supply to the tumor. The balance in blood supply from the portal vein and hepatic artery makes the difference between a regenerative nodule and HCC. 131I-Lipiodol has been used with success to treat unresectable HCC (21). The hypothesis in adjuvant treatment is that 131I-lipiodol emits γ-radiation with a mean penetration of 4 mm, potentially delivering a sufficient dose of radiation to the remnant liver and eradicating microscopic lesions. The intraarterial injection of radiolabeled lipiodol early (within 2–3 mo) after resection is well tolerated and was shown to be efficient in a small, randomized controlled study comparing the postoperative injection of 131I-lipiodol with surveillance (7). A single postoperative injection of 1,850 MBq of 131I-lipiodol decreased the recurrence rate and improved overall and disease-free survival. After learning of these results, we proposed treating our patients with 131I-lipiodol. Our retrospective case-control study was based on these results (8). Our treatment protocol was slightly different, in that the therapeutic activity was higher (2,400 MBq) than in the Hong Kong trial (1,850 MBq) and was delivered slightly later (8–12 wk after resection instead of 6–8 wk). We used a higher dose for practical reasons, because 131I-lipiodol is available in France only as 2,400-MBq vials and because even after repeated injections in a palliative setting we never observed hepatic toxicity. This dose corresponded to a higher radiation dose to the remnant liver (5,000–5,500 cGy vs. 4,500 cGy) but was, as expected, well tolerated. We preferred delivering the treatment slightly later than did Lau et al. to avoid surgical side effects during the radioprotective period and to avoid impairing the healing process.
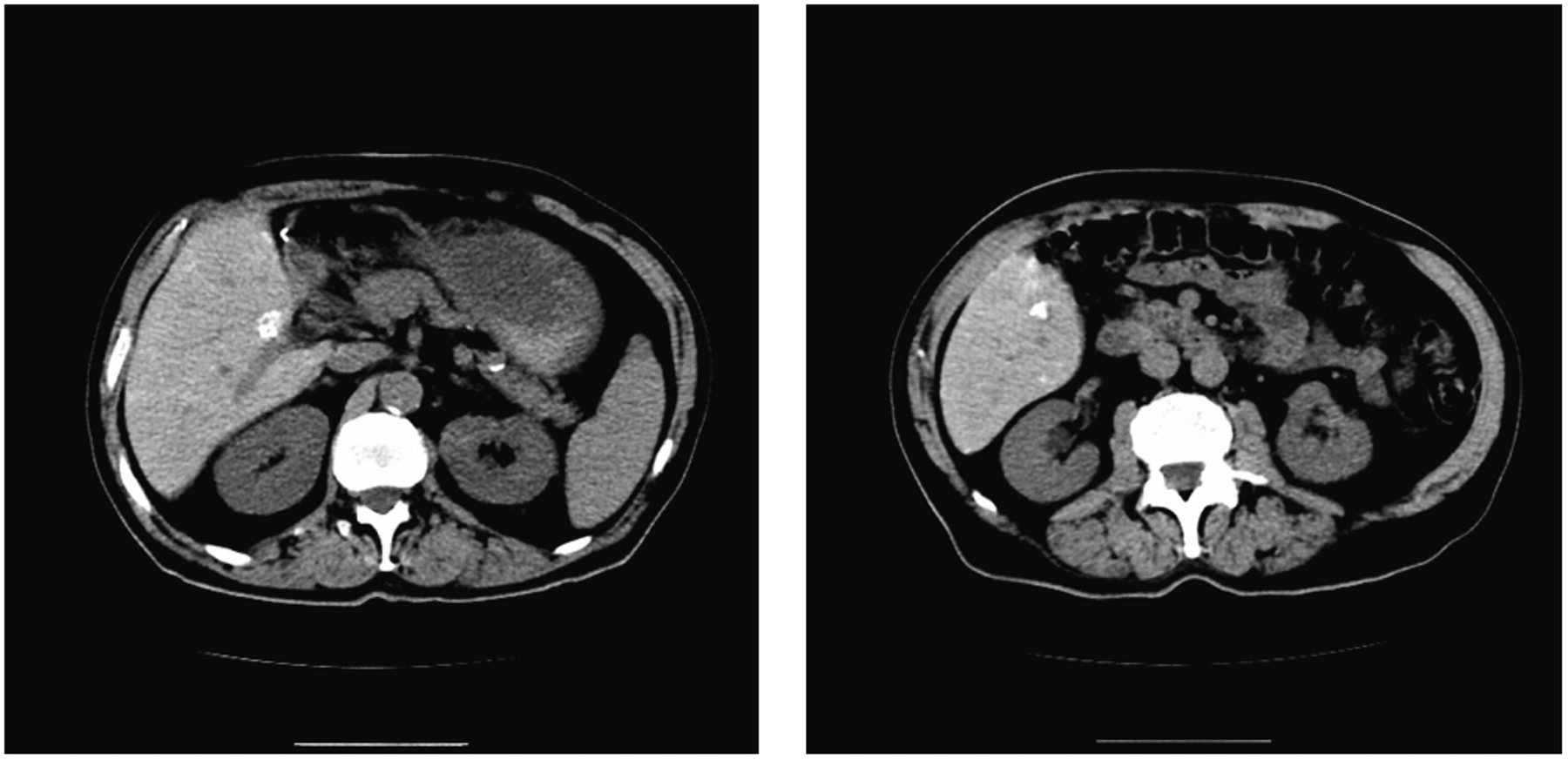
Our conclusions are still in favor of this adjuvant treatment. Disease-free survival was significantly longer in patients given adjuvant treatment, apparently because of more delayed (mean of 21 vs. 26.5 mo) and less frequent (7 vs. 15) recurrence. When considering the timing of these recurrences, one can see that the number of real recurrences was lower in patients given adjuvant treatment whereas the frequency of second cancers remained unchanged. In this retrospective analysis, 2 patients who exhibited a small zone of 131I-lipiodol retention (<15 mm) on the CT scan obtained 7 d after 131I-lipiodol injection were not considered to have recurrences (Fig. 4), and subsequent recurrence was not observed (were they cured by this injection?!). The overall survival curves were not significantly different between the 2 treatment groups despite a one-third improvement in 5-y survival (39% vs. 27%). This lack of statistical significance could be related to the small size of this series, to a potential bias in patient selection caused by lack of randomization, or to eradication of preexisting microscopic tumor foci by 131I-lipiodol—an event that might significantly improve survival but might not prevent de novo tumor formation arising from the underlying liver disease. At least, 131I-lipiodol treatment did not appear to induce any undue mortality from liver failure. The use of 188Re would probably be a better way to deliver this internal radiation therapy (21–23), because this radionuclide has a higher-energy β-emission, a wider cytotoxic range, and a shorter physical half-life, limiting radiation protection problems to a few hours. Unfortunately, despite this shorter half-life, at least 1 case of lung toxicity with 188Re-4-hexadecyl-1-2,9,9-tetramethyl-4,7-diaza-1,10-decanethiol and lipiodol has occurred, as described in a recent paper from Lambert et al. (22). In that patient, the absorbed lung doses were, respectively, 4.6 and 5.8 Gy, far from the usual toxic doses. Another option for selective internal radiation therapy could be the use of intrahepatic arterial administration of 90Y-microspheres, perhaps after simulation using 99mTc-macroalbumin aggregates. This option gives an objective response in more than 20% of patients and appears to be well tolerated (24).
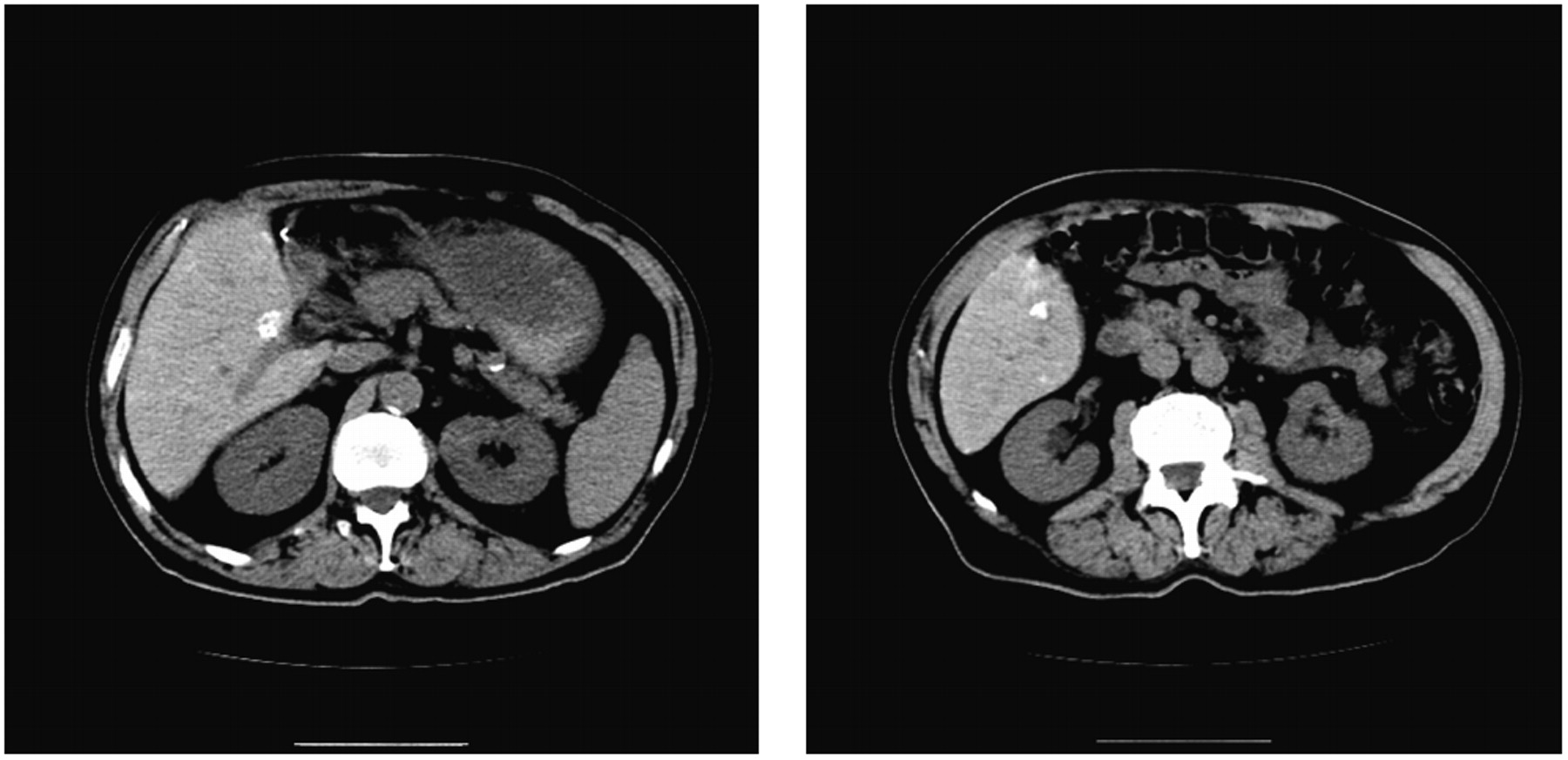
CT scans of 2 patients showing slight 131I-lipiodol retention 7 d after 131I-lipiodol injection.
CONCLUSION
This retrospective final analysis of matched patients is in line with the results of the princeps study demonstrating promise for the postoperative arterial injection of 131I-lipiodol after resection of HCC. These results point out the need for solid evidence confirming the results presented by Lau et al. (7); a randomized controlled trial to confirm the benefit of 131I-lipiodol adjuvant therapy is ongoing.
Footnotes
-
COPYRIGHT © 2008 by the Society of Nuclear Medicine, Inc.
References
- Received for publication June 28, 2007.
- Accepted for publication September 10, 2007.





{kind=link}
{kind=link}
{kind=link}
{kind=link}