


Abstract
18F-FDG PET/CT has gained wide acceptance for evaluation of recurrent colorectal carcinoma. However in clinical practice, contrast-enhanced CT (ceCT) is still the first-line restaging tool. The aim of this study was to investigate the value of contrast-enhanced PET/CT (cePET/CT) as a first-line restaging tool with a special focus on the importance of the use of intravenous contrast. Methods: Fifty-four patients (17 women, 37 men; mean age, 60.3 y), referred for restaging of colorectal carcinoma, were examined with cePET/CT. Retrospective analysis was performed by 2 experienced readers by consensus: first, ceCT alone; second, non-cePET/CT; and third, cePET/CT. The number, localization, and diagnostic certainty of lesions were evaluated. Additionally, the therapeutic impact of the findings was determined. In 29 patients, histology, clinical imaging, and clinical follow-up served as the reference standard. In 25 patients, clinical follow-up and imaging served as the reference standard. Results: Overall, non-cePET/CT delivered correct additional information to the ceCT findings in 27 of 54 patients (50%). This occurred in (a) 20 of 30 patients, where ceCT was found to be inconclusive, and in (b) 7 of 24 patients with conclusive ceCT findings, where non-cePET/CT found additional lesions, leading to a therapy modification in 5 patients. Compared with non-cePET/CT, cePET/CT revealed additional information in 39 of 54 patients (72%), with therapeutic relevance in 23 patients. This large number was primarily due to correct segmental localization of liver metastases, which is crucial for surgical therapy planning. Conclusion: On the basis of its higher accuracy and therapeutic impact compared with ceCT, our data suggest that cePET/CT might be considered as the first-line diagnostic tool for restaging in patients with colorectal cancer.
Colorectal cancer is one of the most common cancer entities worldwide (1). Even though effective therapies provide reasonable cure rates in a significant number of patients, recurrences still remain unacceptably high (2–4). Thus, when there is suspicion of relapse, it is important to find an effective restaging tool capable of accurately defining the extent of the tumor recurrence to plan the best therapy.
Several tools in follow-up of colorectal cancer are currently being used. However, there are marked differences between guidelines for follow-up and restaging (5–9). Carcinoembyonic antigen (CEA) as a tumor marker plays an important role in the American guidelines as well as in the European guidelines. The same applies to colonoscopy and ultrasound of the liver for follow-up, at least in the European guidelines. If abnormal, all modalities lead to further examinations. These usually consist of an abdominal/thoracic CT examination, which is itself also used for follow-up. Overall, contrast-enhanced CT (ceCT) is currently the most established and important tool for restaging in patients with suspicion of colorectal cancer recurrence (8,9). Depending on local availability and preferences, abdominal MRI might also serve as a primary or complementary diagnostic staging tool. However, both offer primarily only morphologic data. 18F-FDG PET/CT gives additional functional information that has also been found to be accurate in the detection of local recurrence and distant metastases (10,11). Therefore, where available, patients may also be referred for a PET/CT examination, particularly if the ceCT showed indeterminate findings.
The aim of this study was to investigate the value of contrast-enhanced PET/CT (cePET/CT) as the first-line restaging tool, with a special focus on the importance of the use of intravenous contrast, diagnostic confidence, and its impact on patient management.
MATERIALS AND METHODS
Patients
This is a retrospective study of all patients who presented with suspected recurrence of colorectal cancer between September 2004 and November 2006 and who were referred for cePET/CT. Fifty-four patients (37 men, 17 women; mean age, 60.3 y; age range, 35–78 y) fulfilled the described criteria.
The study was conducted in accordance with the local guidelines established by the ethics committee for retrospective evaluation, and written informed consent was waived for all patients.
cePET/CT
All data were acquired on a combined PET/CT in-line system (Discovery LS or Discovery ST; GE HealthCare). These dedicated systems integrate a PET scanner (Advance Nxi; GE HealthCare) with a multislice helical CT (LightSpeed Plus or LightSpeed 16; GE HealthCare) and permit the acquisition of coregistered CT and PET images in one session. Patients fasted for at least 4 h before scanning, which started 40–60 min after the injection of a standard dose of 340–370 MBq 18F-FDG. In addition, an oral CT contrast agent (150 mL, Micropaque, Guerbet; diluted with 850 mL water) was administered 75–60 min before scanning. Patients were examined in the supine position. Initially, starting at the level of the head, the non-ceCT scans were acquired with the following parameters: 80 mA, 140 kV, 0.5-s tube rotation, 4.25-mm section thickness, 867-mm scan length, and 22.5-s data acquisition time. The CT scans were acquired during breath hold with the normal expiration position, and scanning included the area from the head to the pelvic floor. Immediately after CT, a PET emission scan was acquired, with an acquisition time of 3 min for the emission scan per cradle position and a 1-slice overlap. Acquisition times ranged between 18 and 21 min. The CT data were used for attenuation correction, and images were reconstructed by using a standard 2-dimensional iterative algorithm (ordered-subset expectation maximization).
Thereafter, an intravenous, ceCT scan of the corresponding region was performed using a specified volume of contrast material (Ultravist 300; Schering) injected with a power injector (Vistron; Medrad), while the patient remained in the same position on the PET/CT table. According to the region of interest, an abdomen protocol (120 kV; dose-modulated tube current up to 440 mA; 2.5 mm; pitch, 1.375:1; 13.75 mm/rotation speed; contrast volume, 120 mL; 90-s delay with 90 mL at 2.0 mL/s and 30 mL at 1.0 mL/s) was performed. During the ceCT, the patients remained in an unchanged supine position on the PET/CT table. For image fusion, 4.25-mm slices were reconstructed. Images (non-cePET/CT and cePET/CT) were then transferred to commercially available workstations (Advanced Workstation, version 4.2-3; GE HealthCare). On those, all data (non-ceCT, non-cePET/CT, ceCT, and cePET/CT) can be evaluated as single procedures and in a fused mode.
Image Evaluation
Reading Protocol.
Image evaluation was performed in a stepwise manner on commercially available Advanced Workstations by 2 readers. Any differences were resolved by consensus. Both readers were dual-accredited, board-certified radiologists and nuclear medicine physicians. Reader 1 had 10 y of experience in CT reading and 6 y of experience in PET/CT reading; reader 2 had 8 y of experience in CT reading and 4 y of experience in PET/CT reading. Predefined criteria were used for all modalities. Reading was performed in 3 successive steps: First, ceCT alone was evaluated. In the second step, non-cePET/CT reading was performed. Finally, the cePET/CT images were evaluated. Simulating clinical daily routine, all images of one patient were read the same day and knowledge of the findings of the previous reading steps was not neglected. Results of reading steps 1 and 2 and of reading steps 2 and 3 were then compared.
Criteria for ceCT-Only Reading.
Hypodense liver lesions with irregular margins and contrast enhancement in the marginal region were regarded as malignant. Detection of soft-tissue masses outside the liver with contrast enhancement or further suggestive signs (e.g., surrounding tissue infiltration, localization) were also considered as malignant. The lymph node assessment used a size-based threshold of 1.0 cm (short axis) for malignancy. Furthermore, lymph nodes with a fatty hilum or with calcifications were regarded as benign, whereas a central necrosis was considered malignant.
Criteria for Non-cePET/CT Reading.
Soft-tissue masses in conjunction with focally increased glucose metabolism above the surrounding tissue level were regarded as malignant. A maximum standardized uptake value (SUVmax) of more than 2.5 (for extrahepatic lesions) and 3.5 (intrahepatic lesions) supported the diagnosis of a malignant lesion but was always considered in conjunction with the qualitative appearance of the lesion (e.g., a liver lesion with a SUVmax of 3.1 clearly demarcated from the background liver activity was considered malignant) (12).
Lymph nodes were assessed for metastatic spread on the basis of an increased glucose metabolism independent of their size. In cases of morphologically malignant appearance without increased glucose metabolism, the lymph nodes were evaluated on the basis of non-ceCT criteria only.
Criteria for cePET/CT Reading.
Reading criteria for cePET/CT were the sum of the described criteria.
Diagnostic Confidence Score and Potential Referral for PET/CT
Images were evaluated with regard to the number, localization, and certainty of lesions using a diagnostic confidence score with a scale ranging from −2 to 2:
−2: Lesions considered to be certainly benign (e.g., cysts, calcified lymph nodes, hemangiomas).
−1: Lesions considered probably benign (e.g., small pulmonary nodules without 18F-FDG uptake and without other morphologic signs of malignancy were considered probably benign granulomas).
0: Lesions considered indeterminate (e.g., borderline-sized lymph nodes or liver lesions not clearly definable as cysts or metastases).
1: Lesions considered probably malignant (e.g., liver lesions with blurry margins at resection sites).
2: Lesions considered certainly malignant.
If all lesions in a ceCT scan could be stated as −2 or 2 (certainly benign or certainly malignant) the examination was reported as conclusive. When multiple lesions stated as 2 (certainly malignant) were present in a constellation that made a curative therapeutic approach impossible, the ceCT was reported as conclusive (as in clinical routine) even if additional inconclusive findings were found. If one or more lesions were present that were stated as −1, 0, or 1 (probably benign, indeterminate, probably malignant), the ceCT was reported as inconclusive. In clinical routine, this generally leads to a referral for PET/CT. Therefore, those patients received a “virtual” referral for PET/CT in our study.
Comparison of Diagnostic Modalities
After the reading protocol, changes with regard to detection and certainty of lesions between the ceCT evaluation and the non-cePET/CT evaluation were reported. On the basis of the diagnostic confidence score, the ceCT was reported as conclusive or inconclusive (see criteria for certainty score) and the virtual referral for further non-cePET/CT was assessed. Thereafter, the same procedure was followed for the evaluation of the non-cePET/CT versus the evaluation of the cePET/CT.
Changes in therapeutic management according to additional findings from the evaluation of ceCT versus non-cePET/CT and from the evaluation of non-cePET/CT versus cePET/CT were also determined. The term “additional findings” consisted of more precise specification or characterization of known lesions, of identification of new lesions, or of correct identification of liver segments. The assessment was based on the Clinical Practice Guidelines in Oncology of the National Comprehensive Cancer Network and by consensus with the referring physician (8,9). If patients underwent liver surgery, intravenous contrast agent was necessary for correct segmental assignment of liver lesions. Thus, a change of management between non-cePET/CT and cePET/CT was reported in those cases.
Reference Standard
Patient follow-up was performed to determine the accuracy of the imaging findings. This included histopathologic evaluation of lesions found by imaging (available in 29 patients) or clinical follow-up with all available clinical data (e.g., physical examination, laboratory reports) and additional imaging, such as CT, PET/CT, MRI, or ultrasound (available in the remaining 25 patients). The mean clinical follow-up was 21 mo (range, 10–35 mo) and included tumor markers (CEA), ultrasound, ceCT, PET/CT, MRI, and physical examinations.
Statistical Methods
Calculations of confidence limits for proportions were done according to Wilson (13). To test for differences between groups on a categoric variable, the Pearson χ2 test was applied.
RESULTS
Disease Characteristics
The majority of our patients initially had advanced disease with T3/T4 (42 patients), N1/N2 (37 patients), and M1 (19 patients) tumor stages. All had undergone first-line treatment, including resection of the primary colorectal tumor. Five patients had surgery only, 39 patients had surgery and neoadjuvant or adjuvant chemotherapy, and 6 patients had surgery and neoadjuvant or adjuvant radiochemotherapy. In 4 patients, only parts of the primary treatment pathway were available (e.g., surgical therapy but no information about further chemo- or radiotherapy despite advanced tumor stage). Thirty-seven patients had abnormal findings in previous routine follow-up imaging (CT or ultrasound). Eight patients had rising CEA levels, and 9 patients were referred for routine follow-up. On the date of imaging, according to the reference standard, our patient population had the following extents of disease: Six patients were free of disease, 24 patients had disease limited to the liver, 13 patients had extrahepatic disease only, and 11 patients had intrahepatic as well as extrahepatic disease.
ceCT Versus Non-cePET/CT
Inconclusive ceCT.
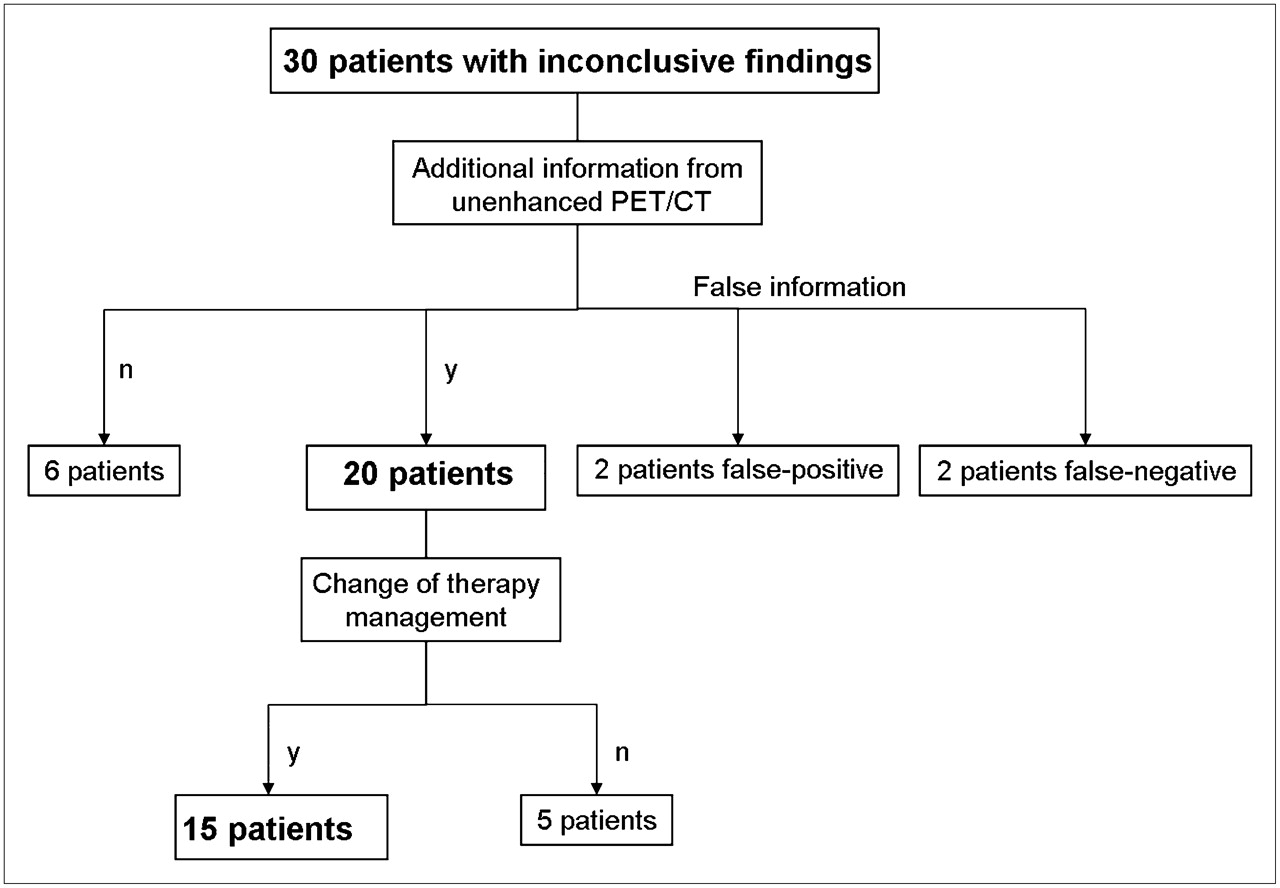
In 30 of 54 patients (56%; confidence limits, 42% and 68%), inconclusive findings were reported due to the uncertain status of lesions based on the defined evaluation criteria (lesions stated as −1, 0, or 1). Fourteen patients had unclear findings in the liver (e.g., structural alterations of the parenchyma after resection), 7 patients had pathologically enlarged lymph nodes, and 2 patients had lung lesions requiring further investigation. One patient had a new soft-tissue mass at the resection site, 1 patient had unclear lesions in the spleen, 1 patient had suggestion of an abdominal wall metastasis, and 4 patients had unclear findings in more than one location. In clinical routine, those patients would have been referred for a non-cePET/CT and, therefore, received from the readers a virtual referral (Fig. 1).

Comparison of ceCT and non-cePET/CT: patients with inconclusive findings in ceCT. n = no; y = yes.
In 20 of 30 patients, non-cePET/CT delivered correct additional information in terms of transforming indeterminate lesions (stated as −1, 0, or 1) into lesions stated as 2 or −2 or showing new lesions stated as 2 or −2. In 15 of 20 patients (28% of 54 patients; confidence limits, 18% and 41%) with correct additional information delivered by non-cePET/CT, the additional information had an effect on follow-up therapy according to the current guidelines (8,9). (Fig. 2). In 7 of 15 patients non-cePET/CT avoided surgical therapy, whereas in 6 of 15 patients surgery was now considered appropriate. Two of 15 patients already had an indication for an operation on ceCT, but non-cePET/CT altered the surgical strategy. One patient had known lung metastases, and non-cePET/CT found an additional liver metastasis. The other patient had a known liver metastasis and non-cePET/CT confirmed an additional local recurrence. In the remaining 5 of 20 patients (9% of 54 patients), no effect on therapy was found.

A 64-y-old male with carcinoma of sigmoid: stage T3 N1 M0; surgery and chemotherapy 3 y earlier; referral because of increasing CEA level. (A) ceCT revealed unclear lesions in spleen (arrow) and, therefore, virtual referral for non-cePET/CT. (B and C) Non-cePET/CT excluded splenic metastases and revealed a hepatic metastasis (arrow) in liver, which was confirmed histologically later.
In 2 of 30 patients, non-cePET/CT was false-negative. Both patients had visible but 18F-FDG–negative liver lesions on CT (stated as −2 by the readers). Consecutive histopathologic verification revealed necrotic metastases (due to previous chemotherapy). In 2 of 30 patients, non-cePET/CT was false-positive: 1 patient had a 18F-FDG–positive lesion at the resection site in the liver (stated as 2, certainly malignant); however, histopathology revealed granulomatous inflammation only. The other patient had a 18F-FDG–positive osteolysis in the sacrum (confidence score, 2), which had completely resolved on the follow-up PET/CT despite the patient's progressive disease. In 6 of 30 patients, non-cePET/CT provided no additional information.
Thus, findings based on the non-cePET/CT, led to appropriate management decisions in 26 of the 30 patients (87%; confidence limits, 70% and 95%) on an equivocal ceCT.
Conclusive ceCT.
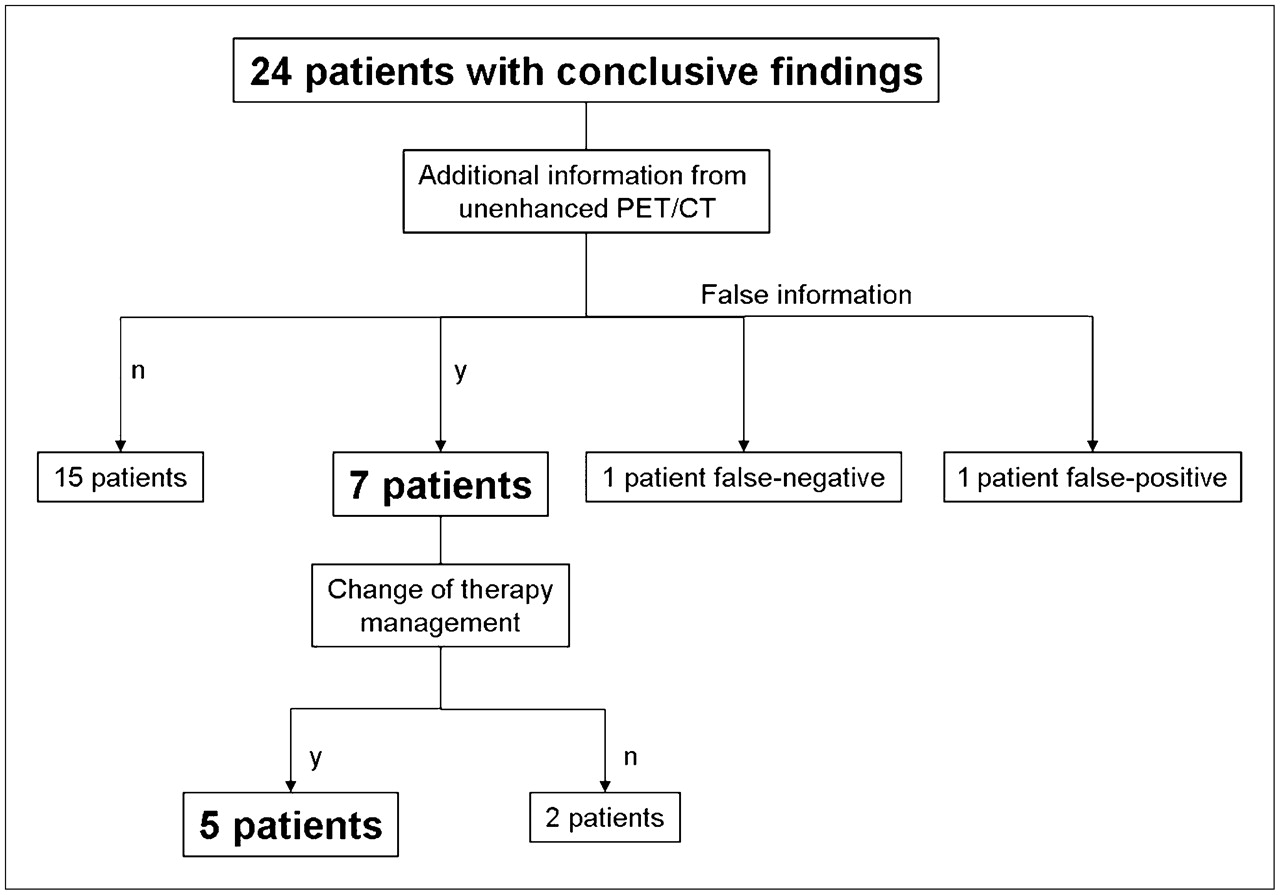
In the remaining 24 of 56 patients (44%; confidence limits, 32% and 58%), the ceCT was reported as conclusive, meaning that in the clinical routine, those patients (even though possibly considerable for referral to PET/CT according to the guidelines) would normally not have been referred for further evaluation by non-cePET/CT. Hence, those patients did not receive a virtual referral by our readers (Fig. 3).
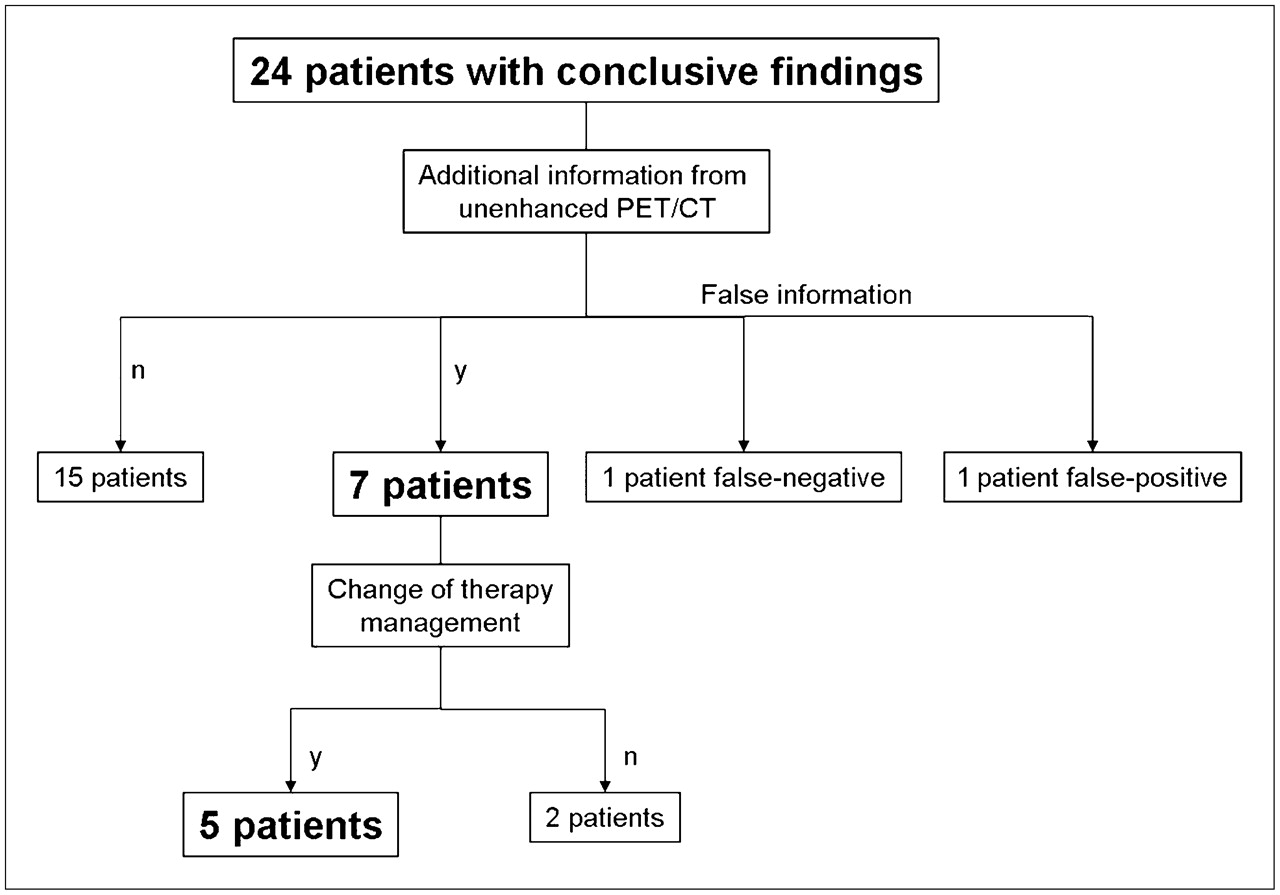
Comparison of ceCT and non-cePET/CT: patients with conclusive findings in ceCT. n = no; y = yes.
Seven of those 24 patients had correct additional findings on the non-cePET/CT. Furthermore, in 5 of 7 patients (9% of 54 patients; confidence limits, 4% and 20%), these findings led to a change of therapy management according to the current guidelines (8,9). (Fig. 4). In 2 of 5 patients, surgical therapy could be avoided by non-cePET/CT and, alternatively, 3 of 5 patients were now deemed to be operable. In the remaining 2 of 7 patients, the additional findings had no effect on therapy.

A 66-y-old man with carcinoma of sigmoid: stage T3 N1 M0; surgery and chemotherapy 1 y earlier; referral because of unclear liver lesion on ultrasound. (A) ceCT revealed no pathologic findings in liver and, therefore, no virtual referral for non-cePET/CT. (B and C) Non-cePET/CT revealed suspicious lesion in right liver lobe (arrow), which was confirmed histologically later.
On the other hand, 1 patient had a false-negative finding on the non-cePET/CT: 1 liver lesion was considered benign (stated as −2 by our readers) because of negative 18F-FDG uptake and sharp lesion margins. On follow-up with cePET/CT, this lesion increased in size on CT and the patient underwent a hemihepatectomy, which revealed a metastasis. Another patient had a false-positive finding: A liver lesion with 18F-FDG–avid uptake was stated as metastasis. However, liver surgery detected only a granulomatous inflammation. In 15 of 24 patients, non-cePET/CT found no additional information compared with ceCT.
Overall, findings based on the non-cePET/CT led to an appropriate management decision in 22 of the 24 patients (92%; confidence limits, 74% and 98%) with a conclusive ceCT.
Overall Comparison.
Most important, non-cePET/CT increased reading confidence, allowing the readers to state more lesions 2 or −2 and, furthermore, to increase the number of detected lesions. In ceCT, a total of 175 lesions was found, of which 97 (56%) were stated as certainly benign/malignant (confidence score, −2 or 2). Twenty-three lesions (13%) were stated as probably malignant/benign (confidence score, −1 or 1), and 55 lesions (31%) were stated as indeterminate (confidence score, 0). Non-cePET/CT detected overall 199 lesions (24 lesions additional), of which 175 lesions (88%) were stated as certain (confidence score, −2 or 2). Five lesions (3%) were stated as probably malignant/benign (confidence score, −1 or 1), and 19 lesions (9%) were stated as indeterminate (confidence score, 0) (Table 1). Testing with the Pearson χ2 test showed a highly significant superiority of non-cePET/CT in this comparison (P < 0.0001). The remaining unclear findings in non-cePET/CT were primarily lesions that were smaller than the spatial resolution of PET or lesions that were obscured due to breathing artifacts (e.g., small lung lesions).
Diagnostic Certainty Score
Compared with ceCT, non-cePET/CT provided correct additional information in 27 patients (50%; confidence limits, 37% and 63%), which had an effect on therapy in 20 of 54 patients (37%; confidence limits, 25% and 50%). However, not all findings would have led to correct management. The overall appropriateness of the additional PET/CT findings was found to be 89% (48/54 patients; confidence limits, 78% and 95%).
Non-cePET/CT Versus cePET/CT
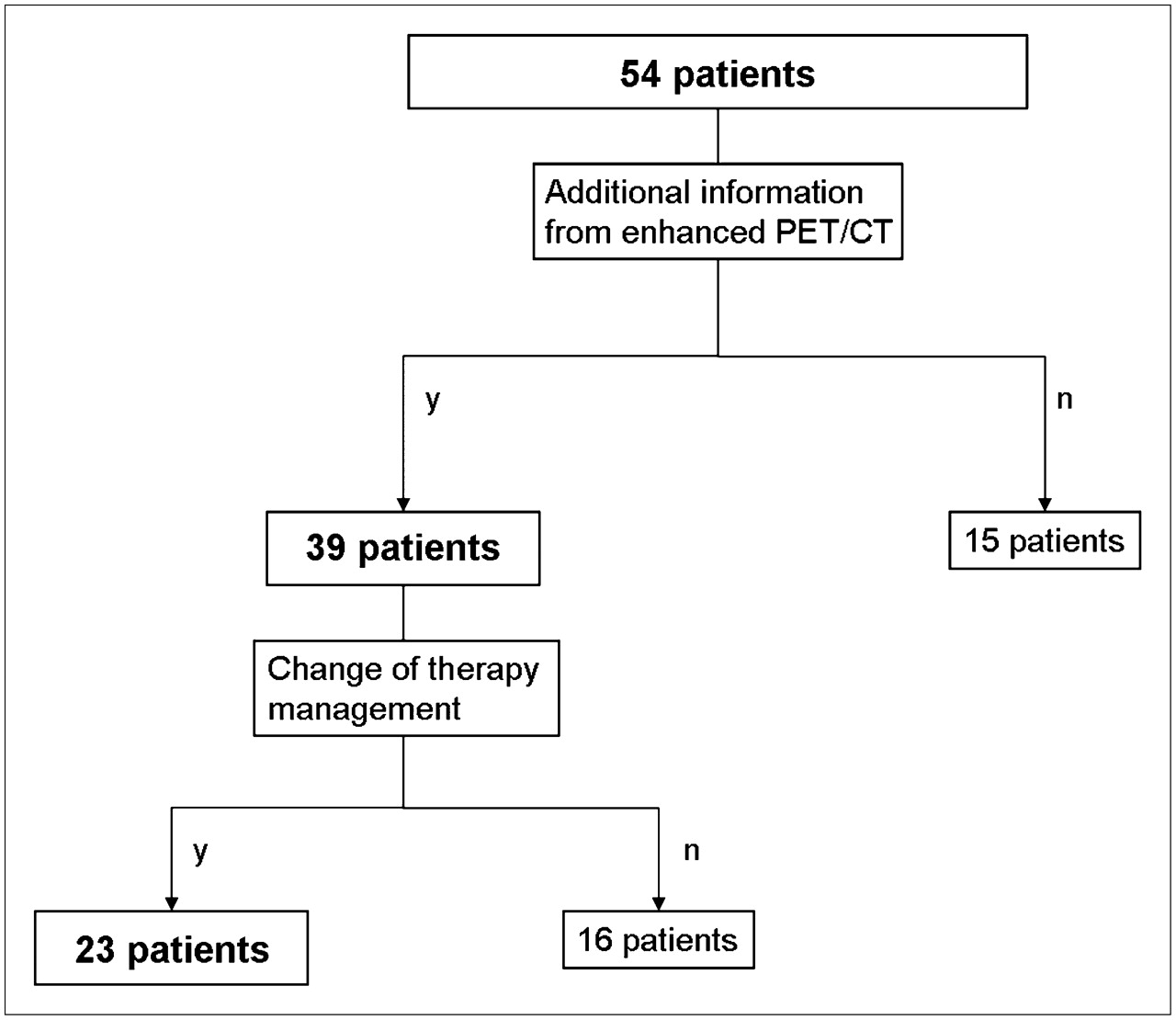
Integrated reading of cePET/CT compared with non-cePET/CT brought additional information in 39 of 54 patients (72%; confidence limits, 59% and 82%) (Fig. 5). In 37 patients, this additional information consisted of visualization of hepatic vessels and, thus, correct segmental localization of present hepatic metastases, which is generally achievable only with administration of intravenous contrast agents. In 1 patient, intravenous contrast delivered additional information with regard to the bowel wall of a local recurrence. In another patient, intravenous contrast was useful for evaluation of the extent of disease in a lymph node.
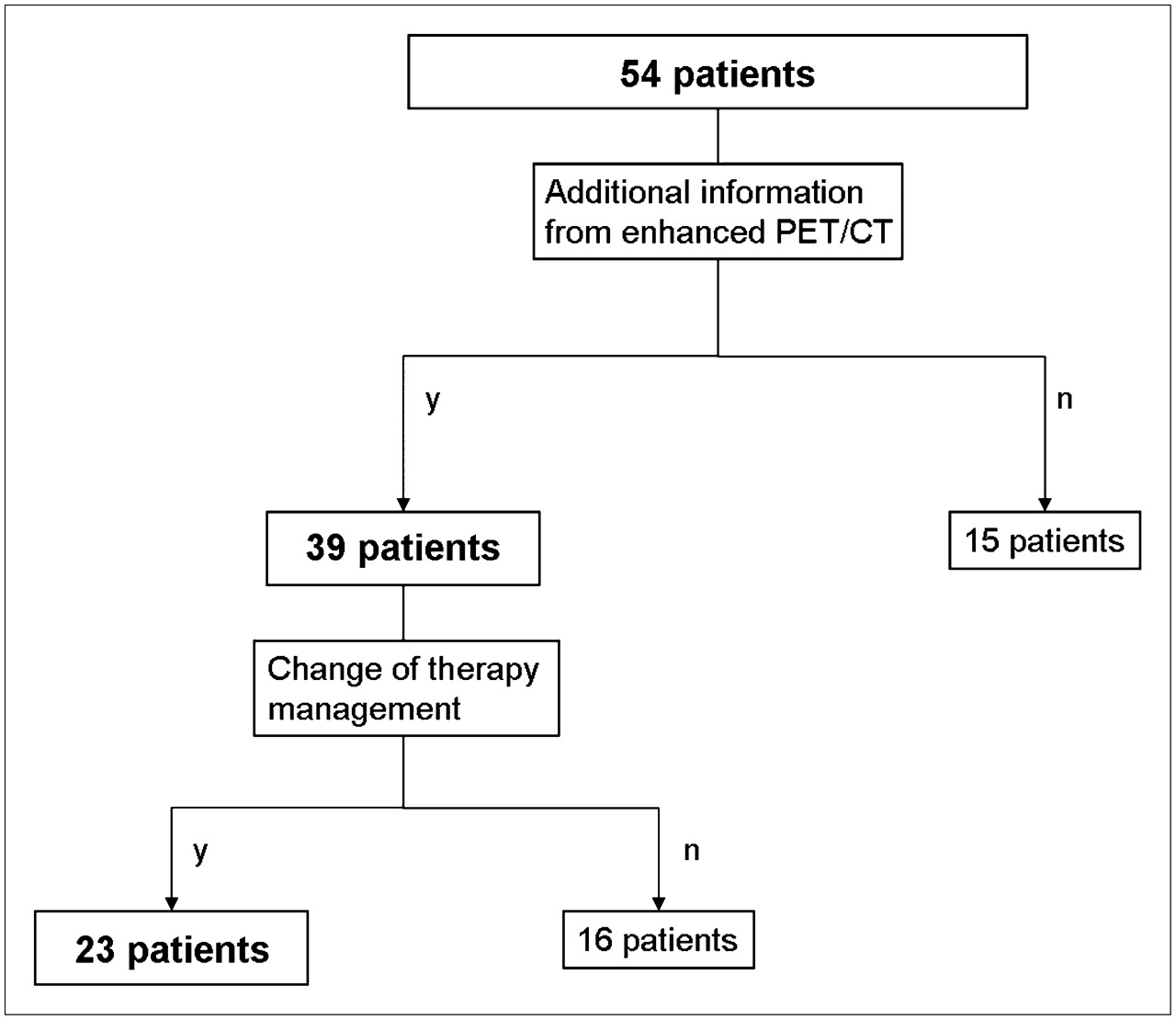
Comparison of non-cePET/CT and cePET/CT. y = yes; n = no.
Twenty-three of all patients (43%; confidence limits, 30% and 56%) with liver metastases underwent a liver resection. Therefore, in those patients, the correct localization of the liver lesions was considered therapeutically relevant (Fig. 6).

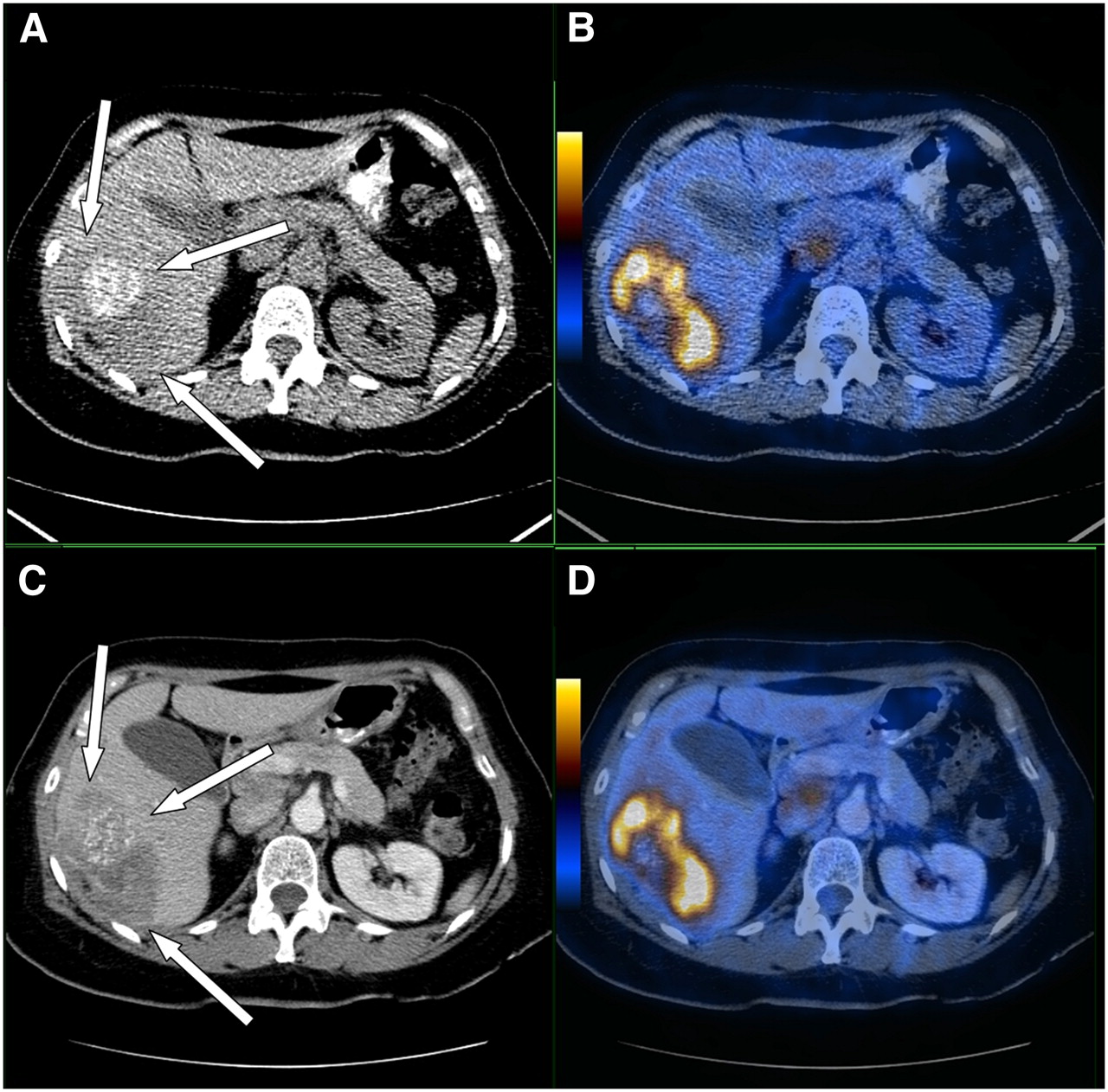
A 58-y-old woman with carcinoma of sigmoid: stage T3 N2 M0; surgery and chemotherapy 5 y earlier; referral because of increasing CEA level. (A and B) Non-cePET/CT revealed a large, hypodense 18F-FDG–avid lesion in right liver lobe with partial calcification. Tumor margins cannot be clearly depicted (arrows). (C and D) cePET/CT revealed clear identification of liver vessels and their relationship to the lesions and clear identification of the lesion margins (arrows). In the course, patient received liver surgery and lesions were confirmed histologically.
No changes with regard to the diagnostic confidence score were observed when comparing non-cePET/CT and cePET/CT, as in both of the 2 described patients the lesions had already been stated as 2 in our confidence score (certainly malignant) on non-cePET/CT (Table 1). Thus, no significant differences with regard to the number of lesions or diagnostic confidence was observed.
DISCUSSION
An effective imaging modality for restaging of patients with suspicion of recurrent disease is crucial, as several studies have shown that surgery with curative intention may be possible even in patients with distant colorectal metastases (14,15). This study has shown that cePET/CT as a single-step examination has equal diagnostic confidence and impact compared with a sequential approach with ceCT first and non-cePET/CT afterward.
Our results confirm the finding that, although the lesion detection rate on ceCT images is high, evaluation by ceCT alone can be challenging because of several inconclusive results that require further diagnostic evaluation (56% of our patient population) (8,9,11,16). The reason for this is predominantly related to specificity issues with the structural abnormalities found by this modality. Because combined 18F-FDG PET/CT has already shown its superiority over PET or CT alone in staging and restaging of patients with colorectal cancer, patients with inconclusive ceCT findings now are being frequently referred for further evaluation with 18F-FDG PET/CT (11,17).
More important, this study has shown that in 21% (5 patients) of the patients with apparently conclusive findings on ceCT, the addition of non-cePET/CT information led to appropriate changes in therapy. In clinical routine, cases in which ceCT has been evaluated as conclusive, the patient would not routinely be referred for a further evaluation with 18F-FDG PET/CT.
When looking at the therapy management decisions, it might be not surprising that in cases with initially conclusive ceCT, the general impact of non-cePET/CT is a lot smaller than that in the inconclusive ceCT group. On one hand, it could be argued that, therefore, the power of non-cePET/CT in the conclusive group is smaller. Alternatively, the examination with a more powerful tool (such as non-cePET/CT) adds diagnostic confidence even when no changes in therapy management occur. However, those patients had to be considered, also, when looking at the appropriateness of management decisions. This explains our high appropriateness of 87% in the inconclusive group and 92% in the conclusive group.
By performing cePET/CT as the initial imaging modality, 65% (30 patients with inconclusive ceCT and 5 patients with conclusive ceCT and therapeutically relevant information in non-cePET/CT) of the patients would have had a clear benefit, including changes in management as well as in diagnostic confidence. Therefore, must cePET/CT now be performed as the first-line diagnostic tool in restaging of colorectal cancer? One could argue that in 35% of the patients, a futile radiation exposure, as well as attributed costs would have been generated. However, this theory holds true only if ceCT and non-cePET/CT were performed within 2–4 wk. In general, surgeons insist on contrast-enhanced CT studies not older than 4 wk before taking a patient into the operating room. Thus, another additional scan with contrast enhancement (ceCT or cePET/CT) would be needed in the majority of patients. Additionally, it has to be considered that, in the inconclusive patients, depending on the protocol used for the cePET/CT, radiation exposure might be reduced compared with the 2-step approach with ceCT and non-cePET/CT.
It also raises the question of whether one can take the responsibility to underdiagnose 21% of all apparently conclusive ceCT cases, as these patients would not have been referred for a non-cePET/CT.
It has already been shown for several other oncologic diseases that contrast media in PET/CT can enhance the diagnostic accuracy and certainty (18,19). Our data do not contradict these studies, even though diagnostic certainty was equal between non-cePET/CT and cePET/CT. This finding was attributed primarily to our study setup, which was intentionally designed to simulate the diagnostic work-up of patients in daily clinical practice, including the reader's knowledge of previous imaging studies in most of the cases. It can be assumed that evaluation of non-cePET/CT without access to concomitant ceCT might have an impaired diagnostic accuracy and certainty. Therefore, our study setup probably overestimates the impact of non-cePET/CT and underestimates the power of cePET/CT. This explains why, in most of our cases, additional information provided by the intravenous contrast agent was related only to the localization of hepatic vessels, which was not relevant to the lesion certainty.
Even though diagnostic confidence is strongly improved with cePET/CT, several lesions cannot be definitively stated. In our study, 12% of the lesions remained uncertain. For example, in pulmonary lesions, which are too small to be characterized by PET, follow-up examinations (mostly CT) must be performed. In some cases, MRI can bring further information (e.g., in bone or small liver lesions) (20). Additionally, PET and PET/CT evaluation can be challenging in cases with chronic inflammatory changes. In our study, 2 of the false-positive findings on PET/CT were related to granulomatous inflammation, which is a known and common cause of overstaging in PET and PET/CT (21). Even with the application of contrast media, which also accumulates in inflammatory lesions, further differentiation of malignancy or inflammation can be difficult.
The use of quantitative structural parameters to generate a diagnostic confidence score is another controversial issue. A size-related cutoff of 1.0-cm short-axis diameter has been used to define malignant lymph nodes on ceCT only. Recent publications have shown that in different areas malignant lymph node sizes can vary between medical conditions and tumor entities (17,22). However, a general 1.0-cm threshold for lymph node assessment is still widely accepted, and further research must be done with regard to lymph node sizes in different body compartments under different medical conditions.
The advantage of a more sophisticated examination such as cePET/CT over the routine ceCT is clearly evident and has been discussed. However, even when non-cePET/CT showed therapeutic relevant information in 20 patients, to date there is no evidence that our single-step examination pathway is more cost-effective compared with the routine multistep pathway. So far, cost-effectiveness has been proven for PET alone only and for only a few tumor entities on PET/CT (23–25). Cost-effectiveness might also depend on different national reimbursement and hospital charges. Furthermore, the time advantage gained from faster diagnosis provided by our “1-step-approach” is also challenging to determine. Thus, considerations about cost-effectiveness have not been part of this study but will be necessary, as they will play an increasing role in the near future.
Another limitation is the retrospective character of our study. All of our patients received their treatment according to the results of the cePET/CT. Therefore, our “changes in therapy management” must be seen as potential changes, following the treatment guidelines and by consensus with the referring physician. Individual prospective changes could not be evaluated, as the initial therapy plan was not individually defined before the cePETCT.
CONCLUSION
Overall, on the basis of a higher confidence score and significant therapeutic impact, our data suggest that cePET/CT might be considered as the first-line staging tool for restaging in patients with suspected recurrence of colorectal cancer.
Acknowledgments
We thank Victor Kalff (Department of Nuclear Medicine, The Albert Hospital, Melbourne, Australia) for sharing his profound knowledge and for his structural inputs to our project.
Footnotes
-
COPYRIGHT © 2008 by the Society of Nuclear Medicine, Inc.
References
- Received for publication October 16, 2007.
- Accepted for publication November 20, 2007.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}