


Abstract
Results from animal experiments have shown that human IgG2/mouse chimeric antitenascin 81C6 (ch81C6) monoclonal antibody exhibited higher tumor accumulation and enhanced stability compared with its murine parent. Our objective was to determine the effect of these differences on the maximum tolerated dose (MTD), pharmacokinetics, dosimetry, and antitumor activity of 131I-ch81C6 administered into the surgically created resection cavity (SCRC) of malignant glioma patients. Methods: In this phase I trial, eligible patients received a single injection of 131I-ch81C6 administered through a Rickham catheter into the SCRC. Patients were stratified as newly diagnosed and untreated (stratum A), newly diagnosed after external beam radiotherapy (XRT) (stratum B), and recurrent (stratum C). 131I-ch81C6 was administered either before (stratum A) or after (stratum B) conventional XRT for newly diagnosed patients. In addition, chemotherapy was prescribed for all patients after 131I-ch81C6 administration. Dose escalation was performed independently for each stratum. Patients were observed for toxicity and response until death or progressive disease. Results: We treated 47 patients with 131I-ch81C6 doses up to 4.44 GBq (120 mCi), including 35 with newly diagnosed tumors (strata A and B) and 12 with recurrent disease (stratum C). Dose-limiting hematologic toxicity defined the MTD to be 2.96 GBq (80 mCi) for all patients, regardless of treatment strata. Neurologic dose-limiting toxicity developed in 3 patients; however, none required further surgery to debulk radiation necrosis. Median survival was 88.6 wk and 65.0 wk for newly diagnosed and recurrent patients, respectively. Conclusion: The MTD of 131I-ch81C6 is 2.96 GBq (80 mCi) because of dose-limiting hematologic toxicity. Although encouraging survival was observed, 131I-ch81C6 was associated with greater hematologic toxicity, probably due to the enhanced stability of the IgG2 construct, than previously observed with 131I-murine 81C6.
Although a recent phase III study demonstrated that temozolomide combined with radiotherapy improves outcome of patients with newly diagnosed glioblastoma multiforme (GBM), the vast majority of patients still die from progressive disease (PD) within 1–2 y of diagnosis (1). Salvage therapies after progression have also proven ineffective (2). Thus, there is no established therapy for patients with PD after standard external beam radiotherapy (XRT) and temozolomide chemotherapy. In addition, current treatments contribute to a limited quality of life (3).
Most patients progress at the primary tumor site (4), indicating that better local control represents a critical first step to improve overall outcome. Prior studies using regionally administered radiolabeled monoclonal antibodies (mAbs) directed against molecular targets on malignant glioma (MG) tumors have noted an encouraging rate of overall survival (5–8).
mAb 81C6 (m81C6), a murine IgG2b, binds an isoform of tenascin C abundantly expressed in the extracellular matrix of gliomas but does not react with normal adult brain (9,10). Preclinical studies confirmed the specificity and efficacy of 131I-m81C6 therapy (11–13), whereas initial clinical studies confirmed its specificity and selectivity in human subjects (14,15).
Subsequent phase I studies defined the MTD of 131I-m81C6 to be 4.44 and 3.7 GBq (120 and 100 mCi) for newly diagnosed and recurrent patients, respectively, with the dose-limiting toxicity (DLT) being delayed neurologic and hematologic toxicities (6,7). A recent phase II study demonstrated a median survival of 79.4 wk among newly diagnosed GBM patients treated with 131I-m81C6 (8).
Human/mouse chimeric mAbs join murine antigen-binding domains to the human immunoglobulin constant domains (16). Because of difficulties producing murine 81C6 in sufficient quantity to support a multiinstitutional randomized trial, we developed a human/mouse chimeric 81C6 mAb (ch81C6) that was capable of bulk production and that incorporated a human IgG2 constant region because of its low affinity for Fc receptors. Although the specificity and binding affinity of ch81C6 is virtually identical to m81C6, ch81C6 unexpectedly also demonstrated increased tumor uptake in human glioma xenografts and enhanced in vivo stability compared with m81C6 (17). Similar results in humans would suggest that 131I-ch81C6 might be a better reagent than m81C6 for brain tumor−targeted radiotherapy. To investigate this hypothesis, the current phase I study was conducted to determine the MTD, dosimetry, and evidence of therapeutic benefit of 131I-ch81C6.
MATERIALS AND METHODS
Patient Eligibility and Treatment
Eligibility criteria for the current trial were the same as those used in our published phase I and II studies with 131I-m81C6. Briefly, eligible patients had resectable, unifocal, supratentorial, recurrent MG tumors that expressed tenascin. Additional inclusion criteria included age over 18 y, Karnofskyperformance status (KPS) over 60, and adequate bone marrow, hepatic, and renal function (5). Pregnant patients and those with an iodine allergy were ineligible.
After resection and Rickham catheter placement into the surgically created resection cavity (SCRC), patency of the Rickham catheter and intactness of the SCRC were confirmed by injecting 99mTc-labeled albumin or diethylenetriaminepentaacetic acid into the reservoir followed by analysis of γ-camera images immediately, 4 h, and 24 h after injection. Patients with leakage of 99mTc-labeled tracer from the SCRC were not eligible. All patients underwent peripheral blood leukopheresis of CD34+ stem cells (PBSC) before treatment. Circulating antibodies to ch81C6 were measured before and 30–120 d after treatment (5).
Patients were stratified as newly diagnosed with no prior therapy (stratum A), newly diagnosed after XRT (stratum B), or recurrent (stratum C). The initial dose for all strata was 2.96 GBq (80 mCi) because this dose was below the MTD previously established for 131I-m81C6 (6,7). Dose escalation, defined in consultation with the Food and Drug Administration, was empirically set in 0.74-GBq (20 mCi) increments and was performed independently for each stratum. To maintain optimal immunoreactivity, 20 mg of ch81C6 were used with doses of 3.7 GBq (100 mCi) or greater. A minimum of 3 patients was treated per dose level. Patients with a SCRC volume of <5 cm3 were eligible for treatment; however, they were not included in the dose-escalation schema because of concern for increased toxicity risk. The absorbed doses to the cavity interface and 2-cm margin were estimated using S values as a function of cavity volume. These S values were calculated by means of β- and photon Monte Carlo transport using previously described methods (18).
Suppression of thyroid radioiodine accumulation and administration of 131I-ch81C6 were performed as described (8). Patients on stratum A received XRT after 131I-ch-81C6. Patients on all strata also received chemotherapy for approximately 1 y using a “best clinical management” regimen determined individually, which included conventional dosing schedules of temozolomide, lomustine, irinotecan, and etoposide (Fig. 1).

Treatment schema for each stratum.
The Duke Investigational Review Board approved this trial and each patient provided informed consent.
Antibody Production and Labeling
Genomic cloning was used to combine the murine 81C6 variable region genes with those for the human IgG2 constant regions (19). ch81C6 was grown in a Mini-Max hollow fiber bioreactor (Biovest Inc.) with CD Hybridoma media (Invitrogen) without serum or protein additives. Purification was by affinity chromatography over a Sepharose−staphylococcal protein-A column, followed by polyethyleneimine ion-exchange chromatography. Food and Drug Administration Manufacture and Testing Guidelines were followed for each clinical batch (20). 131I-ch81C6, prepared using the IODO-GEN method (19), had an immunoreactivity of >75%, with >95% of the label eluting as IgG on size-exclusion high-performance liquid chromatography and precipitating with trichloroacetic acid. The dose of 131I-ch81C6 was prepared the day of administration and was administered to patients within 1–3 wk of surgical resection.
Pharmacokinetics and Dosimetry
Absorbed-dose calculations for the SCRC, whole body, and bone marrow were performed as previously described using a serial, 2-compartment system in which the SCRC and body (excluding the SCRC) were assumed to be the first and second compartments, respectively. Specifically, depth–dose calculations and corresponding isodose curves for the SCRC, SCRC interface, and normal brain were performed using the 3-dimensional discrete Fourier transform convolution method based on a dose kernel for 131I (21).
Toxicity and Response Determinations
Patients were monitored for toxicity (Common Toxicity Criteria database, version 2.0; National Cancer Institute; http://ctep.cancer.gov/reporting/ctc.html) until PD or death. Complete blood counts were performed weekly for the first 8 wk. Initial follow-up occurred 1 mo after 131I-ch81C6 and then regularly thereafter as described (8). 18F-FDG PET scans were obtained as needed to help determine whether progressive enhancement on follow-up MRI represented either progressive tumor or treatment-related inflammatory changes. A thyroid panel was obtained 1–2 mo after 131I-ch81C6 and every 4–6 mo thereafter.
DLT was defined as either (a) attributable grade ≥3 nonhematologic toxicity or (b) hematologic toxicity within 6 wk of 131I-ch81C6 administration consisting of >14 d of either an absolute neutrophil count of <500 cells per milliliter or a platelet count of <20,000 platelets per milliliter.
Seizures were recorded but were not considered neurologic toxicity attributable to 131I-ch81C6 because of their expected occurrence in this disease setting. The precise etiology of nonseizure neurologic toxicity after 131I-ch81C6 was difficult to define. Neither clinical features nor radiographic findings observed on either MRI or 18F-FDG PET reliably distinguished between recurrent tumor and treatment-induced radiation necrosis. Although stereotactic needle biopsy is limited with regard to volume sampling, it remains the state of the art for diagnosis of focal brain lesions. Therefore, the etiology of observed neurologic toxicity was determined based on stereotactic needle biopsy whenever possible.
Statistical Analysis
A single-center phase I study with a classical “3 + 3” design was performed to determine the MTD of 131I-ch81C6 (6). Kaplan–Meier survival distributions were estimated from initial treatment to either death or last contact (22). Logistic regression was used to examine the effect of cavity size as well as 131I-ch81C6 absorbed and cumulative (131I-ch81C6 plus XRT) radiation doses to the 2-cm-thick SCRC interface on toxicity.
RESULTS
Patient Characteristics
Forty-seven patients accrued between October 1999 and February 2002. Patient characteristics were comparable among the 3 strata (Table 1). All stratum C patients received prior radiation therapy and 9 of these patients received prior chemotherapy. The median number of episodes of prior PD for patients enrolled on stratum C was 1 (range, 1–2). The median number of prior chemotherapy agents administered to these patients was 1 (range, 0–4).
Patient Characteristics on Phase I 131I-ch81C6
Dosimetry Results
Dosimetry findings for patients on the 3 strata were comparable and displayed significant interpatient variability. The average SCRC volumes were 21 cm3 (range, 2–81 cm3), 17 cm3 (range, 2–65 cm3), and 18 cm3 (range, 2–57 cm3), whereas the average (range) 131I-ch81C6 SCRC residence times were 79 h (10–113 h), 85 (24–177 h), and 86 h (54–161 h) for patients on strata A, B, and C, respectively. The average absorbed dose to the 2-cm SCRC margin was 32 Gy (3–59 Gy), 45 Gy (9–97 Gy), and 40 Gy (18–110 Gy) among patients enrolled on strata A, B, and C, respectively. The average (range) residence time for the whole body, excluding the SCRC, for all patients was 69 h (48–106 h).
Toxicity
The MTD established for all 3 strata was 2.96 GBq (80 mCi), due primarily to hematologic toxicity (Table 2). Reversible, grade 4 hematologic toxicity developed in 17 patients (36%) within 6 wk of 131I-ch81C6 administration, including 9 patients on stratum A, 5 patients on stratum B, and 3 patients on stratum C. Criteria for hematologic DLT were met in 7 patients (15%), all of whom received an 131I-ch81C6 dose that exceeded the MTD. The median duration of grade 4 hematologic toxicity among patients who did not meet criteria for DLT was 6 d (range, 3–14 d), whereas the median duration for those who met DLT criteria was 20 d (range, 18–31 d). Six patients received PBSC reinfusion because of acute hematologic toxicity associated with 131I-ch81C6 administration.
Treatment Levels and Toxicity
Neurologic DLT occurred in 3 patients (6%) and seemed to be related to a small SCRC volume (<5 cm3) or proximetry to critical functional centers in the brain. Reversible grade 3 aphasia developed in 1 patient on stratum B the day after receiving 2.22 GBq (60 mCi) of 131I-ch81C6. This patient remains alive with a good quality of life 6.3 y from diagnosis of an anaplastic astrocytoma (AA). Irreversible neurologic toxicity developed in 2 patients (4%). Irreversible grade 3 left-sided weakness developed in 1 stratum B patient approximately 4 mo after administration of 1.85 GBq (50 mCi) of 131I-ch81C6. A stereotactic biopsy performed on this patient revealed gliosis and necrosis. Unfortunately, this patient died acutely of a presumed pulmonary embolism approximately 9 mo after 131I-ch81C6 administration. Grade 3 aphasia developed in 1 stratum C patient with recurrent AA 8 mo after receiving 3.7 GBq (100 mCi) of 131I-ch81C6, which gradually resolved over the next year. He remains alive approximately 5.4 y from original diagnosis.
Grade 2 hypothyroidism developed in 4 patients (9%) 4–33 mo after 131I-ch81C6, including 2 treated at the 3.7-GBq (100 mCi) level and 2 treated with 2.96 GBq (80 mCi). All of these patients also received prior XRT. One patient experienced an initial seizure after 131I-ch81C6 therapy; however, the overall frequency and severity of seizures experienced by study patients were within the expected range for this patient population. No significant hepatic, renal, or other organ toxicities attributable to therapy with 131I-ch81C6 were observed.
Of note, myelodysplasia (MDS) developed in 2 patients with newly diagnosed GBM. Grade 2 leukopenia, neutropenia, and thrombocytopenia developed in 1 patient treated with 3.7 GBq (100 mCi) of 131I-ch81C6 followed by XRT approximately 4 mo after 131I-ch81C6 therapy. A bone marrow examination 10 mo after 131I-ch81C6 revealed moderate hypocellularity (20%) but no dyspoiesis and <3% blasts. Flow cytometry was unremarkable, but cytogenetic examination revealed 46,XX,t(3;21)(q26;q22) and fluorescence in situ hybridization analysis showed rearrangement of the AML1 locus. A histocompatibility locus antigen (HLA)-matched, sibling, nonmyeloablative, T-cell depleted, allogeneic stem cell transplantation was performed and 99% donor engraftment with a normal karyotype was noted 2 mo after transplantation. However, biopsy-proven recurrent GBM developed and she died 4 mo after transplantation. Persistent pancytopenia developed in the second patient approximately 26 mo after administration of 2.22 GBq (60 mCi) of 131I-ch81C6, followed by conventional XRT and 10 cycles of systemic chemotherapy, including temozolomide (4 cycles), lomustine (2 cycles), and irinotecan (4 cycles). Bone marrow examination revealed clonal rearrangements, including monosomy 7 and deletion of 11q23. Fatal pneumonia developed in this patient 32 mo from original diagnosis.
Human Antimouse Antibody (HAMA)
The serum of 19 of 41 evaluable patients (46%) reacted with ch81C6. However, all 25 available patient serum samples tested against murine single-fragment-chain region were negative. No observed toxicity was related to HAMA reactivity.
Biopsies and Further Surgery
Twenty-seven patients (57%) underwent 30 surgical procedures for progressive clinical or radiographic changes, including 25 stereotactic biopsies and 5 resections. Seventeen biopsies revealed gliosis, whereas 8 confirmed recurrent tumor. Four patients had recurrent tumor on resection, whereas 1 asymptomatic patient had only gliosis at the time of resection. Five patients who had an initial biopsy demonstrating gliosis underwent a second surgical procedure. Repeated biopsy in 2 patients confirmed gliosis, whereas the remaining 3 patients had recurrent tumor.
Pattern of Recurrence
PD was local in most cases. Distant recurrence occurred in 14 patients (30%), including 9 patients with simultaneous local and distant progression and 5 patients with solely distant recurrence.
Response/Survival Data
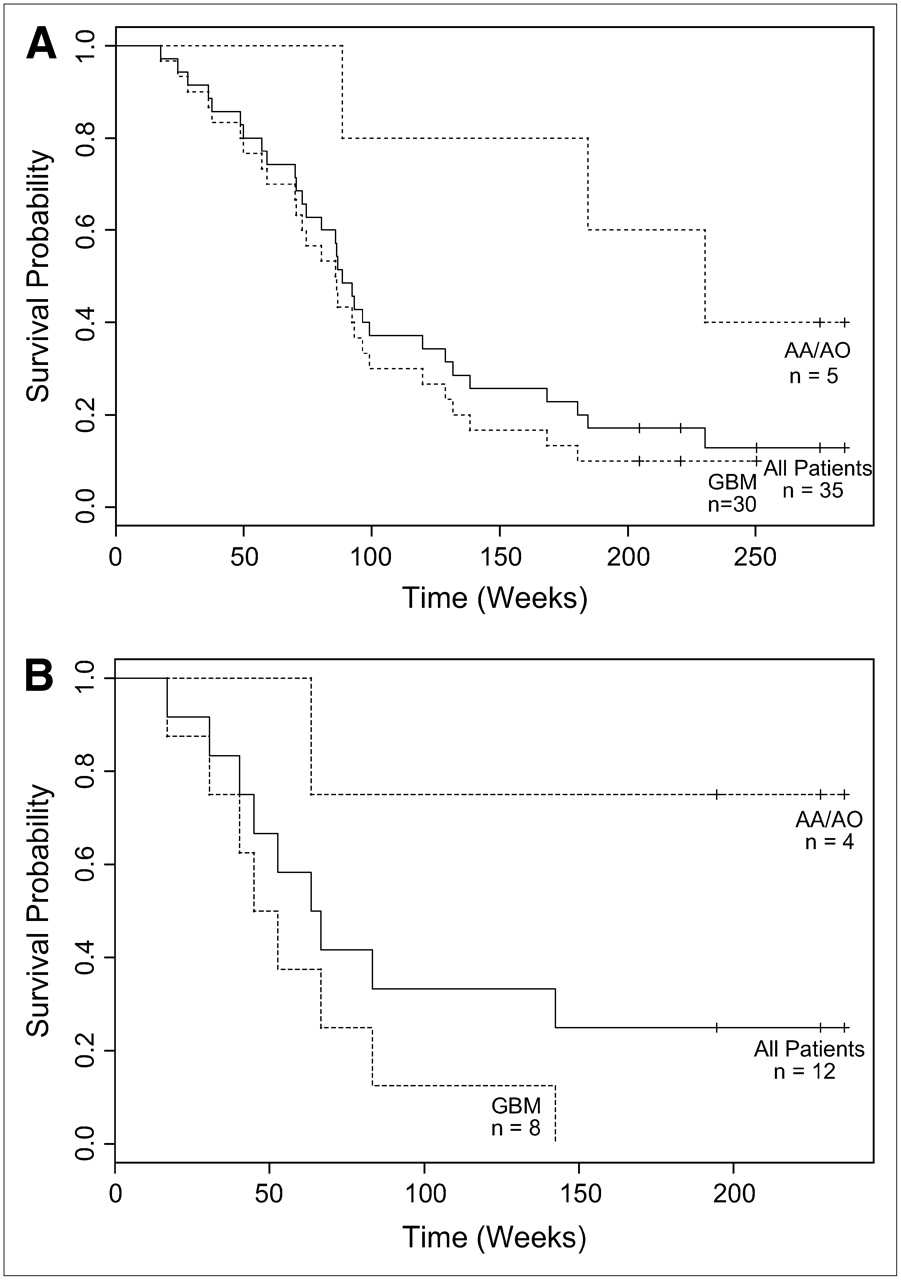
Survival was the most important criterion for efficacy because all patients underwent total or near-total resection leaving little or no residual tumor. With a median follow-up of 185 wk, the median survival for all newly diagnosed patients, those with GBM, and those with World Health Organization (WHO) grade III tumors was 88.6 wk (95% confidence interval [CI], 72.9; 128.7 wk), 86.1 wk (95% CI, 70.1; 99.1 wk), and 230.3 wk (95% CI, 88.6 to not estimable), respectively (Fig. 2A). Of note, there was no significant difference in outcome between stratum A and stratum B patients.
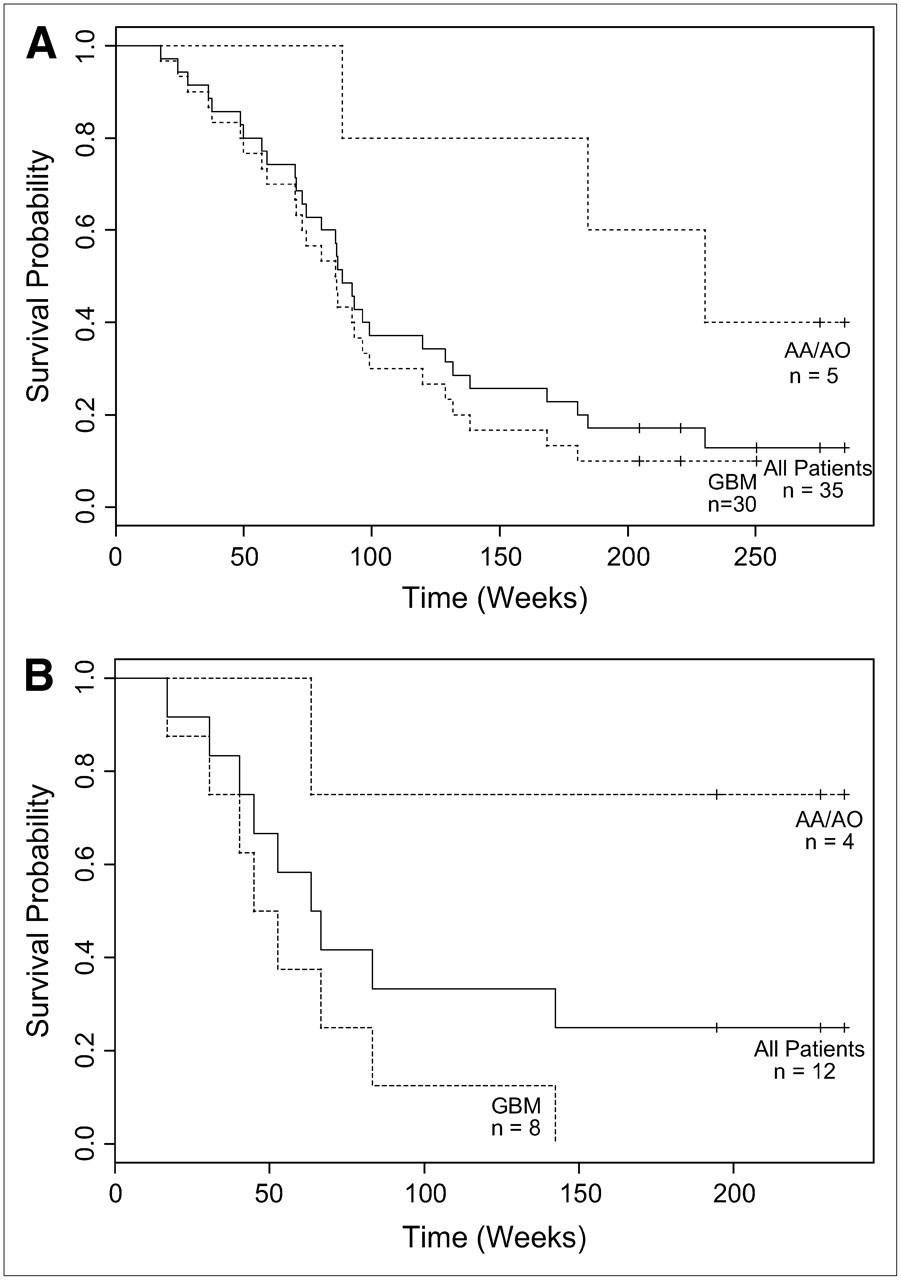
Kaplan–Meier overall survival estimates for newly diagnosed patients (A) and recurrent patients (B) after stratification by histology. AO = anaplastic oligodendroglioma.
With a median follow-up of 228 wk, the median survival for all patients with recurrent disease, those with GBM, and those with WHO grade III tumors was 65 wk (95% CI, 45.0; 142.4 wk), 48.9 wk (95% CI, 30.4; 83.3 wk), and not estimable, respectively (Fig. 2B). Figure 3 depicts representative radiographic findings after 131I-ch81C6.
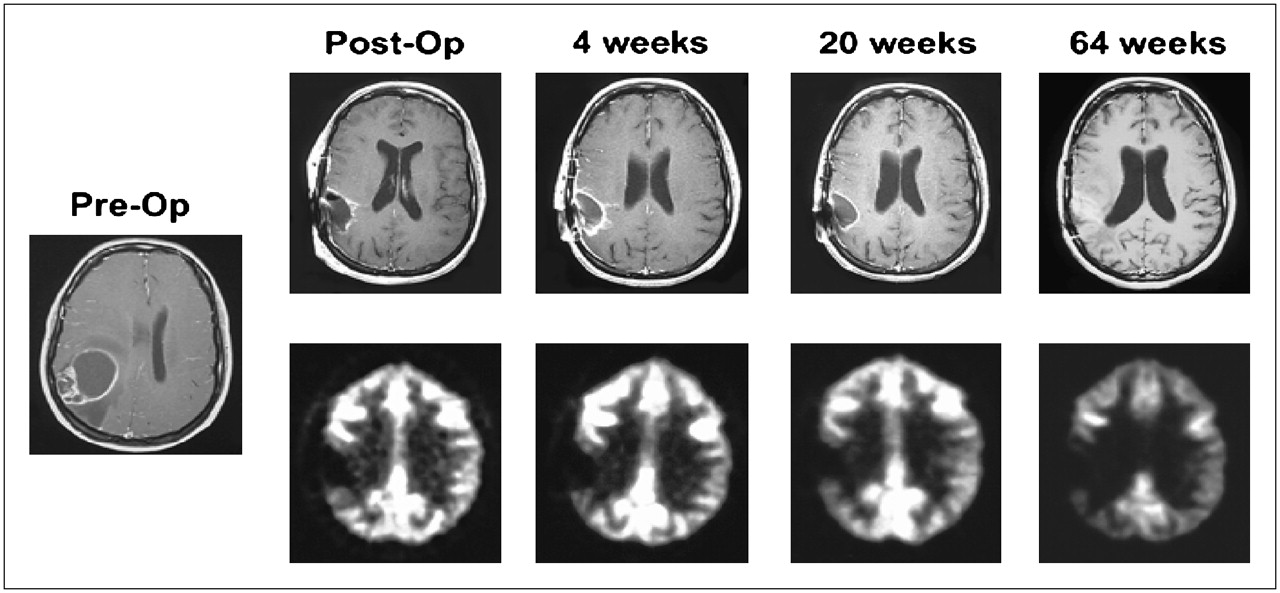
Serial MRI (top and middle) and 18F-FDG PET scan results of representative patient after 131I ch81C6 therapy. Corresponding 18F-FDG PET scan images (bottom) demonstrate a lack of increased metabolic activity in region of SCRC.
DISCUSSION
Recurrence immediately adjacent to or at the primary tumor site occurs predictably in nearly all MG patients following current standard therapies, indicating that local control remains elusive and represents the critical first step required to improve overall outcome (4,23).
Radioimmunotherapy, consisting of radiolabeled mAbs targeting tumor antigens, is associated with encouraging survival and acceptable toxicity for patients with both newly diagnosed and recurrent MG (24–29). Our group has extensively evaluated the clinical activity of radioimmunotherapy using 131I-m81C6 administered directly into the SCRC for MG patients. In previously published phase I studies, dose-limiting neurotoxicity defined the MTD of 131I-m81C6 to be 3.7 and 4.44 GBq (100 and 120 mCi) for patients with recurrent and newly diagnosed MG, respectively. Of note, only 1 of the 76 patients treated on these 2 protocols (1.3%) required further surgery to debulk radionecrosis. In addition, patients with recurrent and newly diagnosed GBM treated on our phase I studies achieved median survivals of 56 and 69 wk, respectively (6,7), whereas patients with newly diagnosed GBM treated with 4.44 GBq (120 mCi) of 131I-m81C6 in a recently completed phase II study achieved a median survival of 79.4 wk (8).
However, in the past, sufficient m81C6 for clinical use could be produced only in ascites of athymic mice because of instability of the murine 81C6 hybridoma. Although that difficulty has been overcome recently, human/mouse chimeric 81C6 mAb (ch81C6) was developed by combining the variable region genes of m81C6 with human IgG2 constant region domains, to have a stable hybridoma capable of producing 81C6 in cell culture (17). The human IgG2 constant region was selected because IgG2 exhibits the lowest Fc receptor affinity of human IgG, thereby minimizing potential reactivity with normal tissues. There are few clinical studies of human IgG2 constructs and, to our knowledge, the current study may be the first involving use of this type of construct as a carrier for therapeutic levels of radionuclide.
Although ch81C6 has the same reactivity with tenascin as m81C6 and exhibits an identical affinity constant for recombinant tenascin CD fragment, paired-label experiments demonstrated a significantly higher tumor uptake of ch81C6 in both subcutaneous and intracranial xenografts compared with m81C6. This behavior is likely attributed to enhanced in vivo stability of 131I-ch81C6 (30).
Because of its greater stability, we hypothesized that ch81C6 might remain in the SCRC longer than its murine counterpart, thereby increasing delivered radiation dose. The average residence time for 131I-ch81C6 for all patients in the current study was 83 h, which is longer than that seen previously for m81C6 (7,8). Furthermore, comparable clinical benefit was observed with 131I-ch81C6 at lower administered activity levels than those used previously with m81C6 (8).
In the current study, we determined the MTD of 131I-ch81C6 to be 2.96 GBq (80 mCi) for patients with either newly diagnosed or recurrent MG. The DLT was hematologic in most cases. The frequency and severity of hematologic toxicity associated with 131I-ch81C6 increased significantly at doses above the MTD, regardless of prior treatment status, whereas hematologic DLT was not observed among patients treated at the MTD. The lower MTD and higher hematologic toxicity for 131I-ch81C6 compared with its murine parent is consistent with the prolonged retention of the chimeric construct in the whole body. Of note, the average whole-body residence time determined for 131I-ch81C6, 69 h, was nearly twice that determined previously for 131I-m81C6 (7,8,21). Neurotoxicity developed in 3 patients, including 2 with a SCRC volume of <5 cm3, suggesting that additional modifications are required to safely administer 131I-ch81C6 to patients with small SCRC volumes. However, none of the patients on this study required further surgery for symptomatic radionecrosis.
It is possible that 131I exposure contributed to the cases of MDS observed in our study. Secondary cancers, including leukemia and MDS, have been noted after radiotherapy with 131I for thyroid disorders (31,32). In addition, cases of secondary MDS have been recently reported among lymphoma patients treated with 131I-labeled mAbs (33). The cytogenetic abnormalities observed in our patients who developed secondary MDS are associated with therapy-induced hematologic malignancies (34). Of note, we have not observed secondary leukemia or MDS among >300 patients with MG treated with intracavitary 131I-m81C6. It is likely that the hematologic toxicities observed with 131I-ch81C6 result from the long plasma half-life of the human IgG2 construct, which, in turn, yields greater radiation dose to the bone marrow than 131I-m81C6.
The median survival achieved among newly diagnosed and recurrent patients treated in the current study with 131I-ch81C6 therapy is encouraging and compares favorably with “standard of care” treatments (1,2,35,36). However, this result, as well as those of our previously published trials incorporating 131I-m81C6, must be interpreted with caution. Our current and prior studies are limited by enrollment of patients with favorable prognostic features and by a single-institutional study design. Definitive conclusions regarding the efficacy of radioimmunotherapy approaches such as ours will only be possible after the completion of randomized, multiinstitutional trials.
A question that often arises is the extent to which radioimmunotherapy provides a tangible advantage in efficacy compared with brachytherapy. An important factor is the extent to which the labeled mAb penetrates beyond the cavity margin, potentially providing a means of irradiating tumor cells infiltrating proximal normal brain. Unfortunately, this important question cannot be addressed adequately using existent animal brain tumor models and it is unethical to subject human patients to repeated, invasive procedures to address this question. Thus, current information on this subject is limited. Using multiple biopsies obtained at autopsy, Hopkins et al. demonstrated that mAb penetration is much greater than expected, with a mean Ro of 0.6 cm (37). Furthermore, in a recent dosimetry and SPECT study, we have shown that 131I-m81C6 can penetrate into areas of edema associated with the resection cavity of patients with malignant tumors of the central nervous system (38). Penetration of radiolabeled, tumor-antigen-specific, mAbs into areas of adjacent edema may provide a potential advantage of radioimmunotherapy over other approaches to boost radiation delivered to the resection cavity perimeter such as stereotactic radiosurgery, which has failed to demonstrate a survival advantage for newly diagnosed MG patients in a randomized, phase III setting (39), and interstitial brachytherapy with 125I-labeled interstitial beads (40,41).
CONCLUSION
The encouraging median survival observed on the current study compares favorably with that achieved with 131I-m81C6; however, the clinical benefit of 131I-ch81C6 was partially offset by increased hematologic toxicity. The efficacy, as well as the toxicity of 131I-ch81C6, most likely reflects the enhanced stability of the human IgG2 construct. Because we now have stabilized the m81C6 hybridoma and can produce amounts of m81C6 needed for phase III multiinstitutional trials, no further studies with 131I-ch81C6 are planned.
Acknowledgments
This research was supported by National Institutes of Health grants 1-P50-CA108786-01, NS20023, and CA11898 and by grant MO1 RR 30 through the General Clinical Research Centers Program, National Center for Research Resources, National Institutes of Health.
References
- Received for publication December 6, 2005.
- Accepted for publication February 11, 2006.





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Conventional and pretargeted radioimmunotherapy using bismuth-213 to target and treat non-Hodgkin lymphomas expressing CD20: a preclinical model toward optimal consolidation therapy to eradicate minimal residual disease
- Clinical Experience with {alpha}-Particle Emitting 211At: Treatment of Recurrent Brain Tumor Patients with 211At-Labeled Chimeric Antitenascin Monoclonal Antibody 81C6