


Abstract
Precise PET/CT localization of focal 18F-FDG uptake in the gastrointestinal tract (GIT) may exclude malignancy in sites of physiologic activity but may also induce false-negative reports for malignant or premalignant lesions. The purpose of the present study was to retrospectively evaluate the nature and significance of unexpected focal 18F-FDG uptake localized by PET/CT within the GIT. Methods: The files of 4,390 patients referred for 18F-FDG PET/CT were retrospectively reviewed. The incidence of studies showing unexpected focal uptake of 18F-FDG localized by PET/CT to the GIT was determined. The position of these foci along the GIT and their intensity were recorded. The etiology of the findings was confirmed histologically or by long-term follow-up. Results: Unexpected focal 18F-FDG uptake in the GIT was found in 58 patients (1.3%). Follow-up data were available for 34 of these patients, including 4 with sites in the stomach, 2 in the small bowel, and 28 in the colon. GIT-related disease was confirmed in 24 patients (71%). There were 11 malignant tumors, 9 premalignant lesions, and 4 benign processes including 2 benign polyps, 1 case of active gastritis, and 1 abscess of the sigmoid. Ten patients (29%) had no further evidence of GIT abnormality, and the suggestive sites were considered to be physiologic uptake. Maximal standardized uptake value was 17.3 ± 10.2 in malignant lesions, 14.0 ± 10.5 in premalignant lesions, 18.0 ± 12.1 in benign lesions, and 11.1 ± 7.4 in foci of physiologic 18F-FDG uptake in the GIT, with no statistically significant difference among the 4 subgroups. Conclusion: Incidental focal 18F-FDG uptake localized by PET/CT within the GIT is of clinical significance in most patients. These findings should be followed up with appropriate invasive procedures guided by hybrid imaging results.
PET using 18F-FDG has successfully been implemented in the evaluation of malignant tumors. Diagnosis of cancer is based on the ability of 18F-FDG PET to detect foci of tumors with increased glycolysis (1,2). Increased 18F-FDG uptake, however, besides being present in malignant lesions, is present in benign, inflammatory, or granulomatous processes and in sites of normal, physiologic tracer biodistribution (3,4). These physiologic or benign sites of 18F-FDG uptake may be falsely attributed to a cancerous etiology, and increased tracer activity in malignant lesions may be erroneously interpreted as unrelated to cancer (2–6). 18F-FDG is excreted in part through the gastrointestinal tract (GIT), with uptake in the distal esophagus, stomach, small intestine, and large intestine representing normal patterns of tracer distribution (3,4). Diffuse increased 18F-FDG uptake in the GIT can be defined as physiologic and unrelated to the malignant process with relatively high certainty. A focal, well-circumscribed intraabdominal area of increased 18F-FDG uptake may, however, be interpreted as equivocal or suggestive of malignancy with an unclear location (4,5).
Hybrid PET/CT provides anatomic landmarks for better characterization of increased 18F-FDG uptake (7). Initial literature reports have shown that the precise localization of hypermetabolic lesions by PET/CT may change the definition of focal intraabdominal 18F-FDG uptake from an indeterminate or equivocal to a benign etiology and therefore improve the diagnostic accuracy of PET (7,8). This study was initiated by a series of cases in which focal intraabdominal 18F-FDG uptake that had been localized by PET/CT to the GIT, which had no previously known morphologic lesions, was proven on follow-up to be of malignant or premalignant etiology. The purpose of the present study was to evaluate the frequency of incidental focal sites of increased 18F-FDG uptake in the GIT and to assess the clinical significance of these unexpected findings.
MATERIALS AND METHODS
Patient Population
The files of 4,390 patients with known or suspected malignancy, who underwent whole-body 18F-FDG PET/CT during the period September 2001 to March 2004, were retrospectively reviewed. All patients gave written informed consent for the PET/CT study and for evaluation of their clinical records for follow-up.
This analysis included PET studies showing a single site of focally increased abdominal 18F-FDG uptake that was more intense than liver uptake and was localized by fused PET/CT to the GIT. The patients had no previous malignant involvement and no clinical or imaging suspicion of abnormalities in the same areas. Fifty-eight patients met these inclusion criteria, and they represented the group for calculating the incidence of unexpected focal 18F-FDG uptake in the GIT on whole-body PET.
Of the 58 studies showing incidental focally increased 18F-FDG uptake in the GIT, follow-up data were available for 34 patients, who represented the study group for further assessment of the clinical significance of these findings. There were 22 men and 12 women, with a mean age of 66 y (range, 27–88 y). The primary malignant tumors were colon cancer (n = 9), lymphoma (n = 7), lung cancer (n = 6), and metastatic cancer of unknown origin (n = 2). One patient each had sarcoma; malignant histiocytoma; and esophageal, gastric, or breast cancer. Five additional patients were evaluated for further characterization of single pulmonary nodules. PET/CT was performed on 14 patients assessed for diagnosis or staging, 5 patients assessed at restaging after initial treatment, and 15 patients assessed as part of routine follow-up or because recurrence was suspected.
Imaging Protocol
Patients were instructed to fast, except for glucose-free oral hydration, for 4–6 h before the injection of 370–555 MBq (10–15 mCi) of 18F-FDG. After the tracer administration, patients remained lying comfortably and then voided immediately before PET/CT. The urinary bladder was not catheterized, and oral muscle relaxants were not administered. Whole-body PET and unenhanced CT images were acquired consecutively, 60–90 min after the injection, using a PET/CT system (Discovery LS; General Electric Medical Systems) combining a dedicated, full-ring PET scanner with bismuth germanate crystals and a third-generation multislice spiral CT scanner. The PET and CT devices were mechanically aligned back to back and shared a common table. The CT and PET images were registered using their shared positional information about the table and the patient.
Data obtained from CT were used for low-noise attenuation correction of the PET emission data and for fusion with attenuation-corrected PET images. PET images were reconstructed iteratively using ordered-subset expectation maximization software. PET, CT, and fused whole-body images displayed in axial, coronal, and sagittal planes were available for review. The PET data were also displayed in a rotating maximum-intensity projection.
Interpretation and Analysis of PET/CT Images
PET studies showing single, well-circumscribed foci of increased abdominopelvic 18F-FDG uptake localized by PET/CT images to the GIT, including the esophagus, stomach, small intestine, or colon, were reviewed. The colon was further divided into ascending colon, descending colon, sigmoid, and rectum. The intensity of the 18F-FDG uptake was measured as the maximal standardized value uptake of 18F-FDG (SUVmax), using the software provided by the workstation manufacturer.
After PET/CT, 30 of the 34 patients underwent additional procedures for evaluation of the area of focally increased 18F-FDG uptake. These included surgery in 8 patients, colonoscopy with biopsy in 11 patients, gastroscopy with biopsy in 4 patients, and ultrasound-guided fine-needle aspiration in 1 patient. Six patients underwent colonoscopy that revealed no abnormal findings, and therefore no histologic specimens were obtained. Four patients had only clinical follow-up, for periods ranging from 12 to 31 mo.
Foci of increased tracer uptake in the GIT in patients with negative endoscopic findings, and with no further evidence of disease during a follow-up period of at least 12 mo, were considered to represent sites of physiologic 18F-FDG activity.
The incidence of unexpected focally increased 18F-FDG uptake in the GIT was calculated. The locations of suggestive foci were recorded. The intensity of the uptake was measured for the whole study population and compared among subgroups defined by histologic results and clinical follow-up. Differences in SUVmax among the 4 subgroups were assessed for statistical significance using 1-way ANOVA.
RESULTS
Focally increased 18F-FDG uptake localized by PET/CT to the GIT was found in 58 of the 4,390 patients (1.3%). Of the 34 patients with confirmatory follow-up data, the focal 18F-FDG uptake was in the stomach in 4 patients, the small intestines in 2, and the colon in 28. Of the 28 suggestive colonic sites, 13 were in the ascending colon, 6 in the descending colon, 7 in the sigmoid, and 2 in the rectum (Table 1).
Incidental 18F-FDG Foci in GIT: Diagnosis, Localization, and Intensity of Uptake
Eleven (32%) of these 34 foci were found to be caused by malignant tumors. Tissue diagnosis after biopsy or surgery indicated the presence of 7 primary neoplasms in the colon (n = 4) or stomach (n = 3), with 3 of these tumors representing second primary malignancies. There were 4 metastatic lesions in the small bowel (n = 2), ascending colon (n = 1), or descending colon (n = 1), and these originated from colon (n = 2), stomach (n = 1), or lung cancer (n = 1) (Figs. 1 and Table 2). The mean interval between detection of the focal 18F-FDG uptake and the histopathologic diagnosis was 3.3 mo (range, 1–13.5 mo).
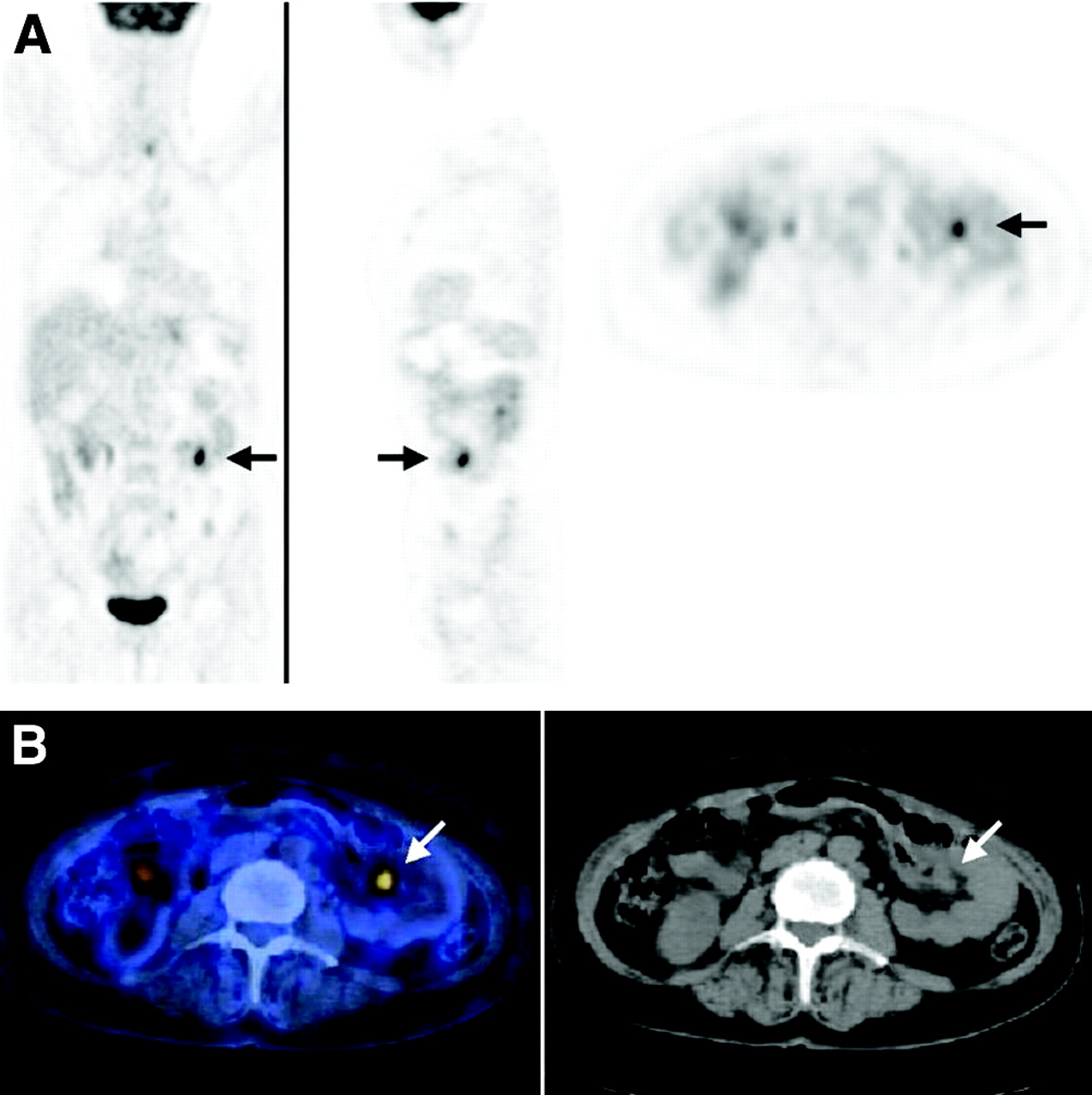
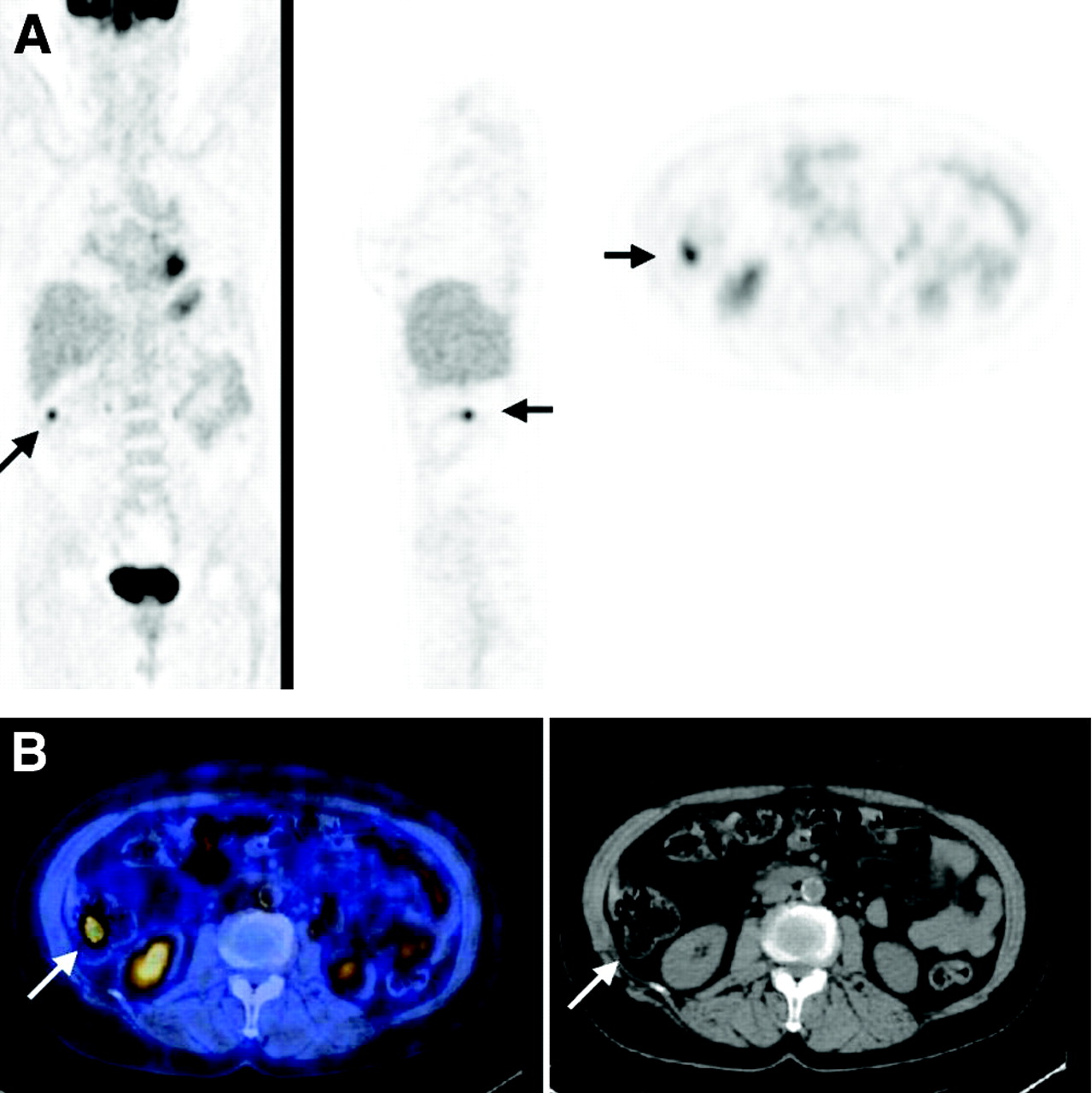
Focal 18F-FDG uptake in 57-y-old woman who had undergone total gastrectomy for stomach cancer and was being evaluated for fatigue, abdominal pain, frequent vomiting, equivocal endoscopic findings at level of anastomosis, and negative findings on whole-body CT. (A) From left to right, coronal, sagittal, and transaxial PET slices show focus of increased 18F-FDG uptake (arrows) in left lower abdomen. (B) Area of increased uptake (arrows) was localized by PET/CT (left panel) to small bowel, as seen on corresponding CT image (right panel). PET/CT-guided surgery revealed small-bowel metastasis originating from primary gastric cancer. No abnormal 18F-FDG uptake was seen in region of anastomosis, and there was no further evidence of disease in this area.
Localization and Etiology of 34 Foci of Incidental GIT Uptake of 18F-FDG
For 13 sites (38%), histologic assessment of biopsy or surgical specimens showed no evidence of malignancy, indicating instead the presence of premalignant adenomatous polyps in the colon (n = 9) (Fig. 2) or benign lesions (n = 4). The 4 benign lesions included 1 case of active gastritis, 1 serrated polyp and 1 hamartomatous adenoma in the colon, and 1 abscess of the sigmoid. The mean interval between detection of the focal 18F-FDG uptake and the final histopathologic diagnosis for these patients was 1.7 mo (range, 0.5–4 mo).
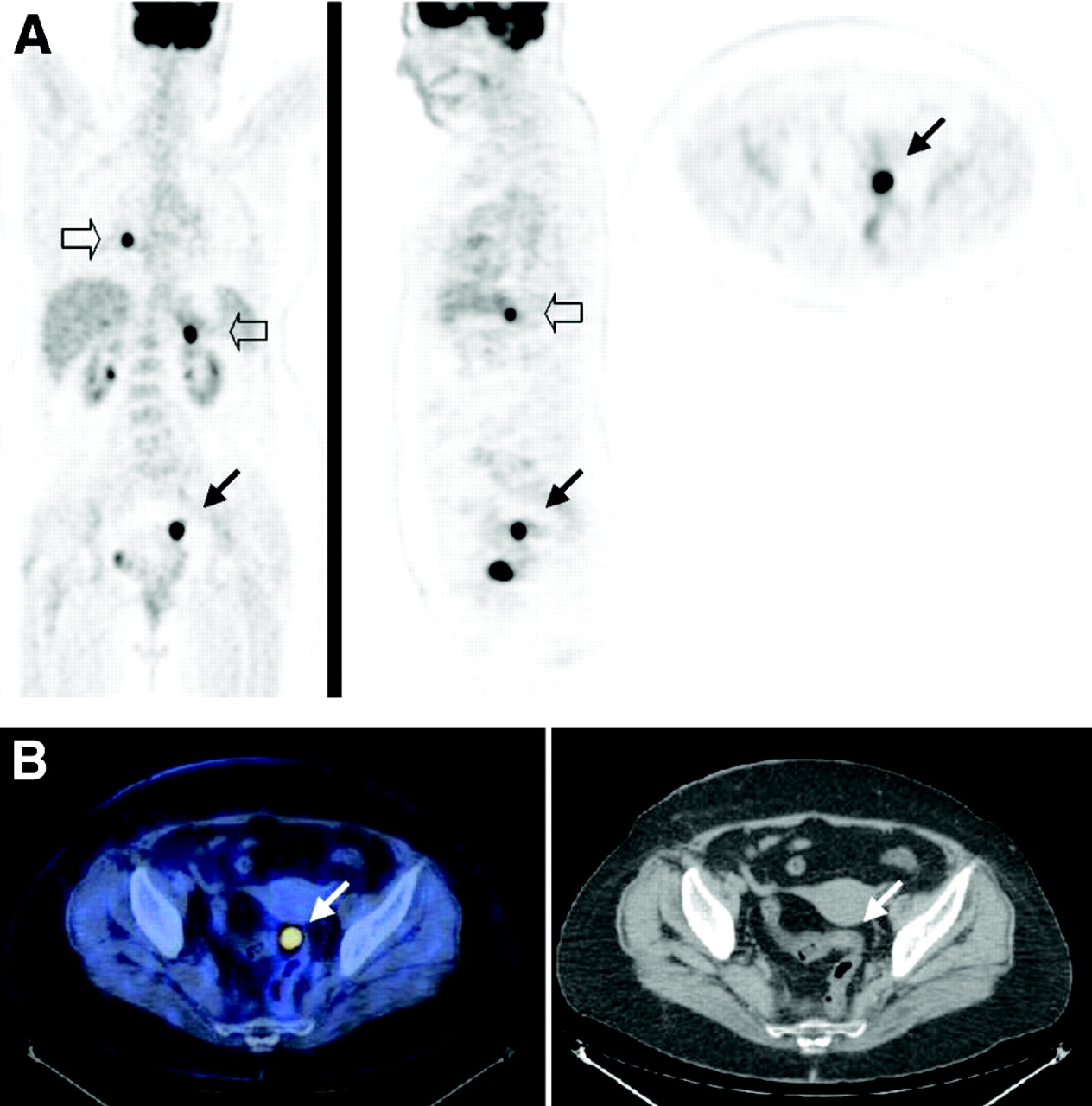
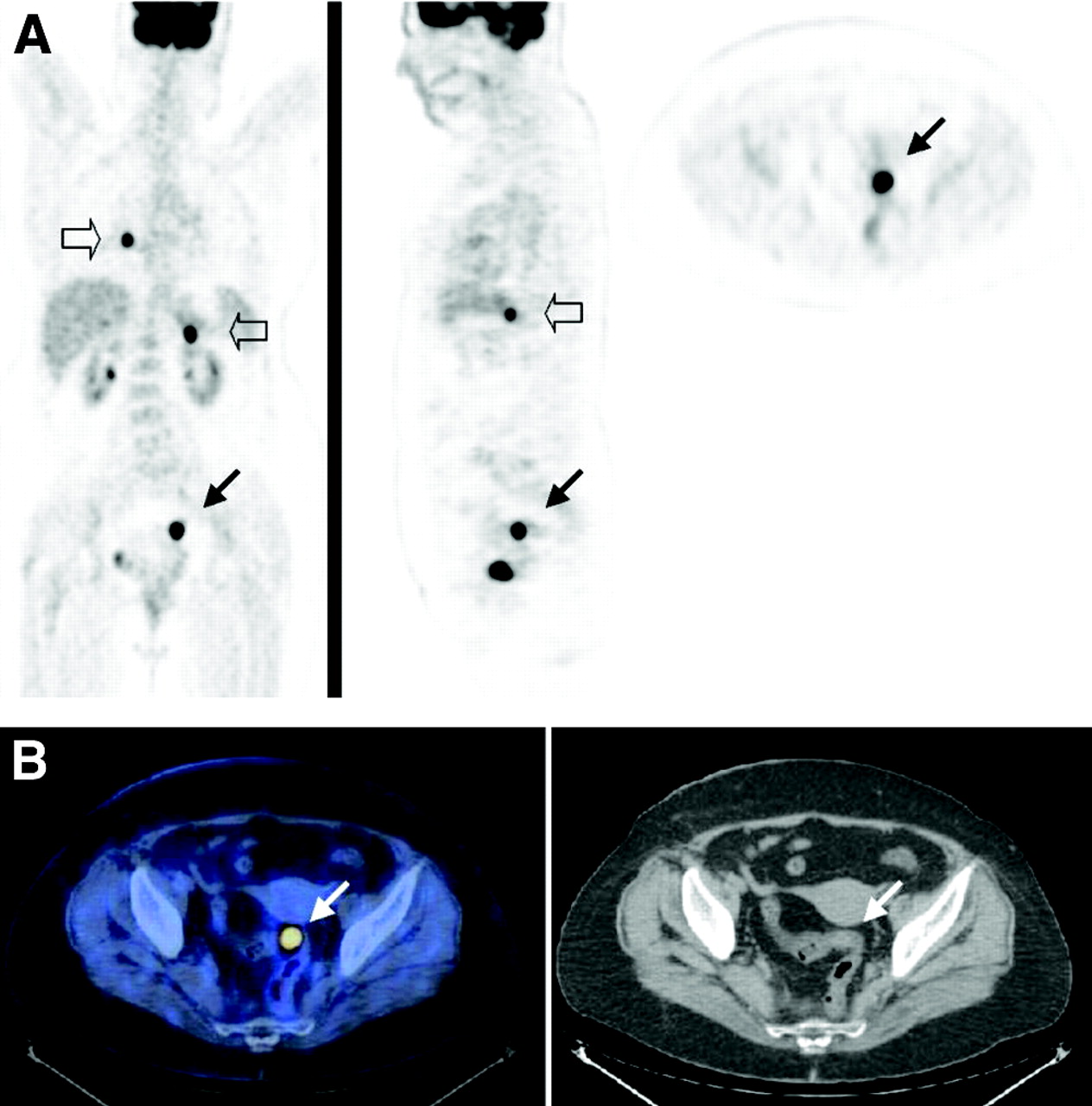
Focal 18F-FDG uptake in 64-y-old woman who was being evaluated for staging of aggressive non-Hodgkin’s lymphoma. (A) From left to right, coronal, sagittal, and transaxial PET slices show focus of increased 18F-FDG uptake (arrows) in left pelvis. Coronal and sagittal PET images show additional areas of abnormal 18F-FDG uptake in mediastinum and left upper abdomen (open arrows), consistent with sites of active lymphoma. (B) Pelvic area of increased uptake (arrows) was localized by PET/CT (left panel) to sigmoid, as seen on corresponding CT image (right panel). Villous adenoma was diagnosed from biopsy sample taken during colonoscopy.
There was no further evidence of disease in 10 areas of focal 18F-FDG uptake in the GIT (29%), localized to the ascending (n = 7) or descending colon (n = 3) (Fig. 3). Colonoscopy had negative results for 6 patients who also had no evidence of disease during a clinical follow-up period of 5–17 mo. No additional diagnostic procedures were performed on 4 patients who had an uneventful clinical follow-up period of 12–31 mo. These 10 foci were considered physiologic 18F-FDG uptake in the bowel.
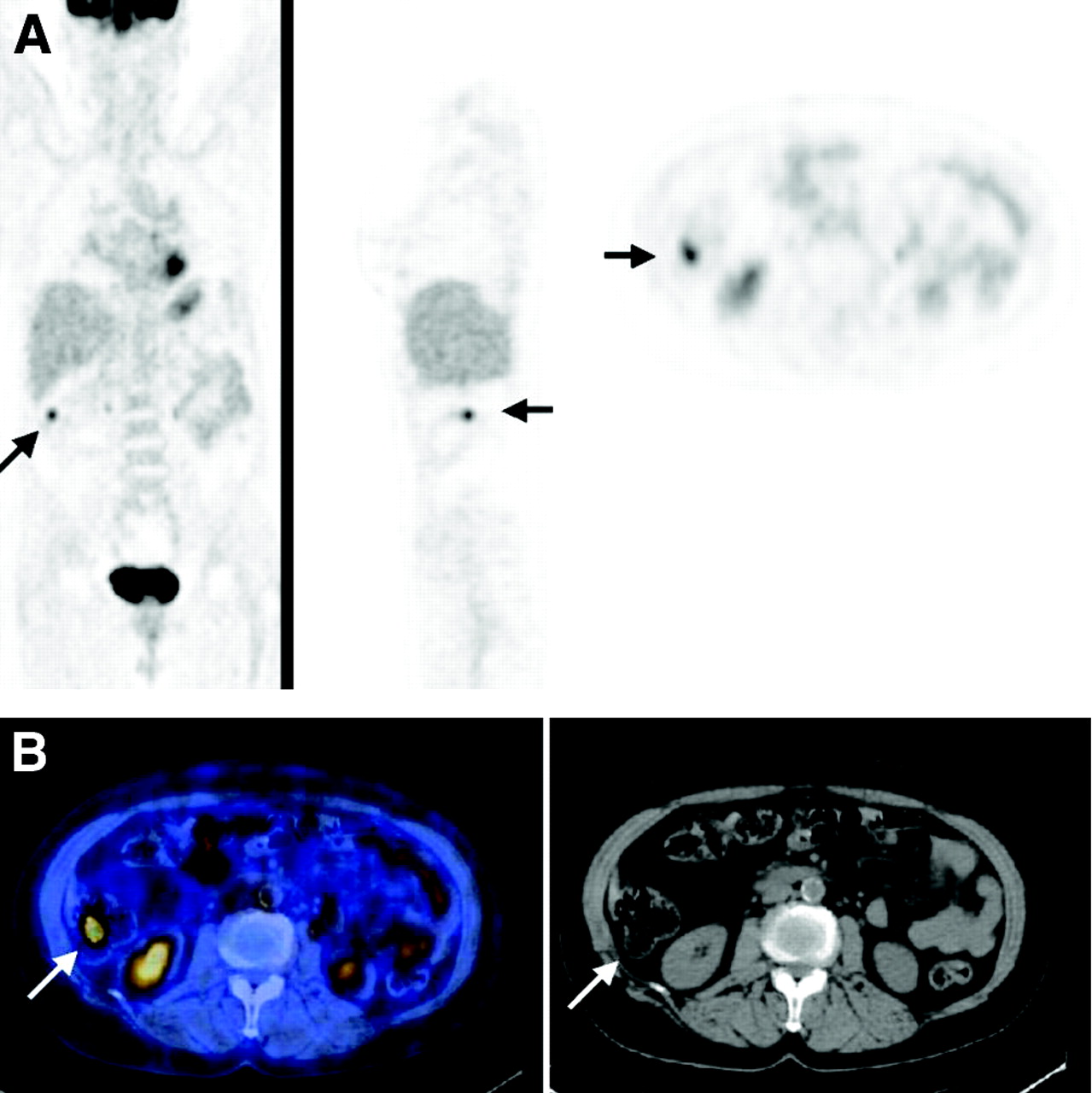
Focal 18F-FDG uptake in 70-y-old woman with low-grade non-Hodgkin’s lymphoma who was undergoing routine follow-up examination. (A) Coronal, sagittal, and transaxial PET slices show focus of increased 18F-FDG uptake (arrows) in right upper abdomen. (B) Area of increased uptake (arrows) was localized by PET/CT (left panel) to ascending colon, as seen on corresponding CT image (right panel). Colonoscopy had negative findings, and patient showed no evidence of disease after 16 mo of follow-up. Focus of increased 18F-FDG uptake was considered to represent physiologic bowel activity.
SUVmax for the 34 foci of increased 18F-FDG uptake in the GIT ranged from 4.5 to 40.3. Mean SUVmax was 17.3 (range, 8.1–40.3) for the 11 malignant lesions, 14.0 (range, 4.5–40) for the 9 premalignant lesions, 18.0 (range, 8.7–35.6) for the 4 benign lesions, and 11.1 (range, 5.7–30.8) for the 10 sites of physiologic activity. No statistically significant difference was found in the intensity of 18F-FDG uptake among the 4 subgroups (Table 1).
The final histologic diagnosis, location, and intensity of focal 18F-FDG uptake in the GIT are summarized in Tables 1 and 2.
DISCUSSION
Incidental foci of abnormal 18F-FDG uptake, precisely localized by PET/CT to the GIT, were found in 1.3% of the present study population. Of these unexpected suggestive sites, follow-up data showed that 71% were caused by GIT-related pathology, with 59% representing malignant or premalignant lesions.
Physiologic 18F-FDG uptake of variable intensity and localization patterns within the GIT has previously been described. Focal tracer uptake is frequently seen at the gastroesophageal junction; moderate uptake, in the stomach; low-intensity uptake, in the small bowel; and diffuse or focal uptake, in the colon (3). This physiologic tracer activity in the GIT has been attributed to uptake by smooth muscles (mainly in the bowel), swallowed secretions, or excretion and intraluminal concentration of 18F-FDG (9,10).
PET using 18F-FDG is more accurate than CT or other conventional imaging modalities for diagnosis of previously unknown recurrent or metastatic malignant foci (11,12). Focal colonic 18F-FDG uptake has a high, 70%–80%, probability of showing corresponding abnormal histopathologic findings (11–13). Despite possible false-positive results, colonoscopy has therefore been recommended as the next diagnostic step for further evaluation of these findings (14,15). The present study found a slightly lower incidence, 64%, of clinically significant lesions in the colon, with a total of 71% throughout the whole GIT.
Although previous studies have evaluated the etiology of incidental 18F-FDG PET findings in the colon (13,15), the clinical significance of abnormal foci in other parts of the GIT has not, to our knowledge, previously been addressed. In the present study, 6 of the 34 suggestive foci (18%) were in the stomach or small bowel, with all but 1 of these lesions proving malignant on further evaluation (Fig. 1).
Metastases have previously been considered to represent an unusual etiology for unexpected single sites of 18F-FDG uptake in the GIT (11). In the present study population, 12% of incidental foci represented metastatic lesions, in addition to the 26% that were premalignant lesions and the 21% that were primary malignancies (Figs. 1 and 2).
Semiquantitative SUV measurements have been suggested as a tool to differentiate between potential etiologies of 18F-FDG foci in the GIT (16). In the current series, a similar but wide range of 18F-FDG uptake values was found in the different subgroups.
PET/CT has been advocated as a useful novel imaging tool leading to a decrease in the number of false-positive and false-negative PET findings in cancer patients (5,7,11). Despite this increase in confidence and decrease in the number of suggestive or equivocal lesions, the precise localization of increased 18F-FDG foci using PET/CT cannot, at present, solve the diagnostic dilemma of abnormal tracer uptake in the GIT. Single sites of focally increased 18F-FDG uptake, precisely localized by hybrid images to the GIT, warrant further evaluation using more invasive diagnostic procedures. Tissue sampling appears to be the only way to define the etiology and clinical significance of focal areas of 18F-FDG uptake in the GIT in individual patients. In this clinical setting, however, PET/CT can play an important role in guiding further investigations, including biopsy or surgery, leading to a decrease in tissue-sampling errors and enhancing early, improved diagnosis and treatment.
CONCLUSION
The results of the present study indicate the need for further assessment and PET/CT-guided tissue sampling in patients with unexpected single areas of focal abnormal 18F-FDG uptake in the GIT. Most of these incidental foci represent unexpected GIT-related abnormalities, such as second primary tumors, sites of unusual metastatic spread, or premalignant lesions.
Acknowledgments
This work was supported in part by a research grant from the Israeli Cancer Association. The authors acknowledge the many useful suggestions of Dr. Anthony J. Parker and Judy Buchanan.
Footnotes
Received Nov. 2, 2004; revision accepted Dec. 15, 2004.
For correspondence or reprints contact: Ora Israel, MD, Department of Nuclear Medicine, Rambam Medical Center, Haifa 35254, Israel.
E-mail: o_israel{at}rambam.health.gov.il
REFERENCES
In this issue





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Long-term Outcomes of Early-stage Non-stomach Gastrointestinal Mucosa-associated Lymphoid Tissue Lymphoma Treated With Radiation Therapy
- Correlation of BRAFV600E Mutation and Glucose Metabolism in Thyroid Cancer Patients: An 18F-FDG PET Study
- Assessment of incidental and clinically unsuspected fluorodeoxyglucose-avid foci detected on oncological positron emission tomography/CT
- The role of the breast radiologist in evaluation of breast incidentalomas detected on 18-fludeoxyglucose positron emission tomography/CT
- Incidental findings on positron emission tomography/CT scans performed in the investigation of lung cancer
- Amoebic Abscess Diagnosed on Fluorodeoxyglucose Positron Emission Tomography Scan in Patient With Recurrent Oropharyngeal Squamous Cell Carcinoma
- Incidental Focal 18F-FDG Uptake in the Pituitary Gland: Clinical Significance and Differential Diagnostic Criteria
- Total Abdominal 18F-FDG Uptake Reflects Intestinal Adenoma Burden in Apc Mutant Mice
- Nonlaxative PET/CT Colonography: Feasibility, Acceptability, and Pilot Performance in Patients at Higher Risk of Colonic Neoplasia
- Incidental findings in imaging diagnostic tests: a systematic review
- 18F-FDG PET and PET/CT in the Evaluation of Cancer Treatment Response
- PET/CT assessment of clinically unsuspected, incidental FDG-avid lesions in oncological patients
- 18F-FDG PET/CT in Evaluating Non-CNS Pediatric Malignancies
- Detection of extrapulmonary lesions with integrated PET/CT in the staging of lung cancer
- Improvements in Cancer Staging with PET/CT: Literature-Based Evidence as of September 2006
- Screening for Cancer with PET and PET/CT: Potential and Limitations
- Lung Cancer Presenting With a Solitary Colon Metastasis Detected on Positron Emission Tomography Scan