


Abstract
The goal of this study was to evaluate the role of radioimmunoscintigraphy (RIS) directed against prostate-specific membrane antigen in modifying postprostatectomy prostate fossa clinical target volume (CTV) definition. Methods: The records of 25 postprostatectomy patients who received external-beam radiotherapy after prostatectomy and who underwent vessel-based RIS/planning CT registration were reviewed. For each patient, the CTV that would have been treated (CTVpre) before this registration was compared with that defined after the registration (CTVpost). In addition, using a standard dose of 66 Gy in 2-Gy fractions, the corresponding bladder and rectum dose volume histograms were compared using 2 endpoints: volume receiving ≥60 Gy (V60) and area under the curve (AUC). Results: The mean CTVpre vs. CTVpost volumes were 24.4 vs. 35.0 cm3, respectively (P = 0.032). The V60 results for CTVpre and CTVpost were 32.7 vs. 41.0 cm3, respectively, for the rectum (P = 0.168) and 33.9 vs. 46.6 cm3, respectively, for the bladder (P = 0.015). The AUC results for CTVpre and CTVpost were 4,027 vs. 4,516 Gy × cm3, respectively, for the rectum (P = 0.396) and 4,782 vs. 5,561, respectively, for the bladder (P = 0.119). No Radiation Therapy Oncology Group grade 3, 4, or 5 (acute or late, gastrointestinal, or genitourinary) toxicity was observed. Two-year biochemical failure-free survival (with failure defined as 2 consecutive prostate-specific antigen rises above 0.2ng/mL) was 87% for the cohort. Conclusion: Incorporating RIS uptake resulted in significant modifications in CTV definition. The consequences of these modifications on the rectum V60 or AUC or on the bladder AUC were not significant, although the bladder V60 did increase. However, observed toxicity was low, with acceptable short-term biochemical control, suggesting that treatment to the modified CTV was tolerable.
Prostate cancer screening and management have undergone an evolution over the past few decades. Because of screening efforts that have resulted in diagnosis at earlier stages, a multitude of local therapy options exists, including radical prostatectomy, external-beam radiotherapy (RT), and brachytherapy (1,2). The most common surgery performed for prostate cancer is the radical retropubic prostatectomy (RRP), a procedure with an excellent cure rate, particularly for early-stage disease (3). Evaluation of the pathologic specimen provided at the time of RRP often results in upstaging of the cancer and can facilitate the decision on whether to administer adjuvant RT. Local recurrence is a primary pattern of failure, even in those patients with negative margins at the time of surgery. Although some recurrences are identified on digital rectal examination (DRE), are symptomatic, or are detected on radiologic workup, the majority of patients with recurrence are found to have biochemical (prostate-specific antigen [PSA]) failure preceding clinical failure.
Postoperative RT has been used with success for those patients who are believed to have high-risk disease predictive of a local recurrence or for those in whom the PSA record, clinical examination, and radiologic findings suggest a local-only recurrence. Although a consensus does not yet exist in the RT community on the definition of high-risk disease or on the precise group of patients that should receive immediate or delayed adjuvant treatment, RT has been used with some success in the postoperative setting (4–11). In addition, no consensus yet exists on the volume to be irradiated (whether to treat the prostate bed alone or whether the regional lymph nodes should be included) in those patients for whom the decision has been made to offer RT. The focus of the current investigation was on the prostate bed portion of the postprostatectomy target.
The design of the postprostatectomy clinical target volume (CTV) poses clinical challenges. One design approach is to reconstruct the location of the prostate and seminal vesicles. Guidelines on average prostate and seminal vesicle volumes were published in the pre-CT era (12). With the advent of CT, these volumes could be assessed more precisely (12,13). However, it is necessary to account for the fact that the space occupied by these volumes is replaced by bladder and rectum after surgery. In addition, special attention must be paid to include the regions at higher risk (i.e., the regions in the prostate bed believed to be the source of persistent/recurrent disease). Often these volumes at risk are tailored to the findings at prostatectomy. In some cases, however, a long interval may separate the time of prostatectomy from the time of RT consultation, so the regions of high risk on the prostatectomy specimen may not necessarily coincide with the source of the PSA rise. The yield of conventional CT, which is useful in planning RT, is often too low to identify areas of high risk. Only rarely can gross disease be seen on the planning CT. Efforts have been undertaken to integrate ultrasound to identify areas of recurrence, but it is often difficult to register ultrasound with precision to the planning CT (14). A bone scan is useful for ruling out extrapelvic (EP) disease (indeed, a positive bone scan usually excludes curative RT altogether) but generally cannot be used to assist in designing the prostate bed target volume (15). Thus, an alternate imaging study that is specifically aimed at visualizing prostate cancer may be of use in assisting in the task of CTV definition. Radioimmunoscintigraphy (RIS) targeted against the prostate-specific- membrane antigen (PSMA) (ProstaScint; Cytogen Corp.) may be one such tool (16–23).
RIS for prostate cancer has been carefully studied in the diagnostic setting, in establishing whether cancer is localized to the prostate and thus amenable to surgery or RT (16–23). RIS is particularly useful in assisting in identifying pelvic or EP lymphadenopathy before undertaking local or locoregional therapy. A multicenter study documented the incidence of prostate fossa (PF), pelvic nodes, and EP uptake among different clinical settings (20). From this investigation and others, approximate values for diagnostic parameters in the postsurgery setting (the primary scenario under current study) are sensitivity, 75% (extraprostatic) and 92% (PF); specificity, 86%; positive predictive value, 81%; and negative predictive value, 67% (16,21). These diagnostic parameters speak favorably for the use of RIS in the diagnostic setting, and the correlation of RIS findings with clinical outcomes has been documented. The impact on clinical outcome is still being investigated, with both positive (24) and negative (25) studies documented thus far. However, the manner in which the RIS information should be integrated into postprostatectomy RT treatment planning has not yet been studied systematically.
In this article, we report on the use of vessel registration to guide and modify the definition of the prostate bed portion of the postprostatectomy CTV for external-beam RT (26–28).
MATERIALS AND METHODS
The role of RIS in the current investigation was to assist in modifying the postprostatectomy CTV. An inherent implication is that the CTV has been designed without knowledge of the RIS information and that the radiotherapist is using RIS to fine-tune the target volume by integrating the RIS-identified areas of uptake. Thus, the goal was to determine how RIS augmented the already existing information of the CT scan, DRE findings, and prostatectomy pathologic findings in guiding CTV definition.
To accomplish this task, the records, image data, and treatment planning data from 1999 to 2002 of 25 postprostatectomy patients who received external-beam RT for biochemical failure (or high risk of failure) in our consortium and who underwent an RIS scan to aid RT treatment volume definition were reviewed. The database used for this investigation was approved by the Institution Review Boards of all of the hospitals from which patient data were obtained for this investigation. Because this investigation was retrospective, a formal waiver of informed consent was requested and approved before conducting the study. In addition to routine demographics (age and race), patient charts were reviewed for pre-RT information (T stage, pretreatment PSA, prostatectomy date, prostatectomy pathology [margin status, seminal vesicle invasion status, extracapsular extension, and grade], postoperative PSA nadir, and PSA/clinical course) leading to the RT consultation. This information is summarized in Table 1. Also shown in Table 1 are the RIS findings. As displayed, the majority of patients (23 of 25) had PF-only uptake, whereas 2 of 25 had uptake in the PF and pelvis outside the PF. No patient had EP uptake, because this was usually a criterion for deciding not to offer RT. Also, all patients had uptake in the PF, because PF uptake was a requirement for attempting vessel registration. No pre-RT biopsies were performed, because DRE did not reveal gross tumor amenable to biopsy in any patient. Also displayed in Table 1 are the treatment techniques, general fields, final dose used, and follow-up information.
Patient Characteristics
For each patient, a planning CT scan was obtained at the time of simulation. The planning CT scan was obtained using intravenous contrast, scanning from the top of the L2 vertebral body (top border) to below the ischial tuberosities (lower border) using 5-mm spacing. This scanning protocol was necessary to enable vessel registration. Rectal and bladder contrast agent was used to visualize these critical avoidance structures. A RIS scan was obtained in the nuclear medicine department, typically during the same week as the planning CT scan. The RIS scan had 2 components: a99mTc-labeled red blood cell (RBC) SPECT scan and a simultaneously acquired 111In-capromab pendetide monoclonal antibody (mAb) (7E11.C5) RIS scan (16–28).
Figure 1 shows how the planning CT and RIS scans were used to define the prostate bed CTV. On the planning CT scan, the blood vessels, rectum, and bladder were outlined, as well as the CTV (CTVpre) that would have been treated without the RIS information. The design of the CTVpre incorporated information from the planning CT, prostatectomy findings, and the PSA record but did not incorporate information provided by the RIS scan. The electronic archive of CTVpre was recovered in the majority of patients. In those instances where it was not possible to recover CTVpre in this manner, for this investigation CTVpre was entered by the radiotherapist, who was unaware of the RIS findings or of the target ultimately used to treat the patient. This blinding process was critically important in avoiding the introduction of observer bias. At the time of simulation, outlining of the bladder and rectum was performed on each patient in a manner that adhered to Radiation Therapy Oncology Group (RTOG) studies (29). The bladder was outlined from apex to dome, and the rectum was outlined from the level of the ischial tuberosities to the rectosigmoid junction.

Flow diagram of image data, showing how planning CT was registered with simultaneously acquired dual-isotope 99mTc-labeled RBC SPECT and 111In-mAb RIS scans, enabling the projection of CTVRIS into the planning CT scan for assistance in modifying CTVpre to define CTVpost.
Next, the RIS information was integrated into the RT planning process. This integration is a key component of the methodology of the current investigation and was accomplished by performing a vessel registration to project the regions of uptake on the RIS into the planning CT scan (27,28). Because the details of the vessel registration process are described in considerable detail in these references, only a brief description is provided here. The major arterial vessels (abdominal aorta, bifurcation into the common iliac arteries, subsequent bifurcation into the internal and external iliac arteries, and the inferior extent to which these arteries could be visualized) were outlined on the99mTc-labeled RBC SPECT scan. These same vessels were outlined on the planning CT scan (which was obtained using the scanning protocol described previously), and the 2 scans were then registered.
Next, the areas of uptake were entered by the nuclear medicine physician on the111In-mAb 7E11.C5 (RIS) scan. This volume, which in all individuals for the current investigation involved at least the prostate bed (and in a very few cases regional pelvic lymph nodes), was denoted as CTVRIS. A vessel subtraction technique was often used to prevent shadowing of the volume of interest by vessel uptake (26) and facilitate accurate delineation of CTVRIS. Then, because the RIS scan was acquired simultaneously with (and, hence, automatically registered to) the RBC SPECT scan, the CTVRIS could be projected into the planning CT scan.
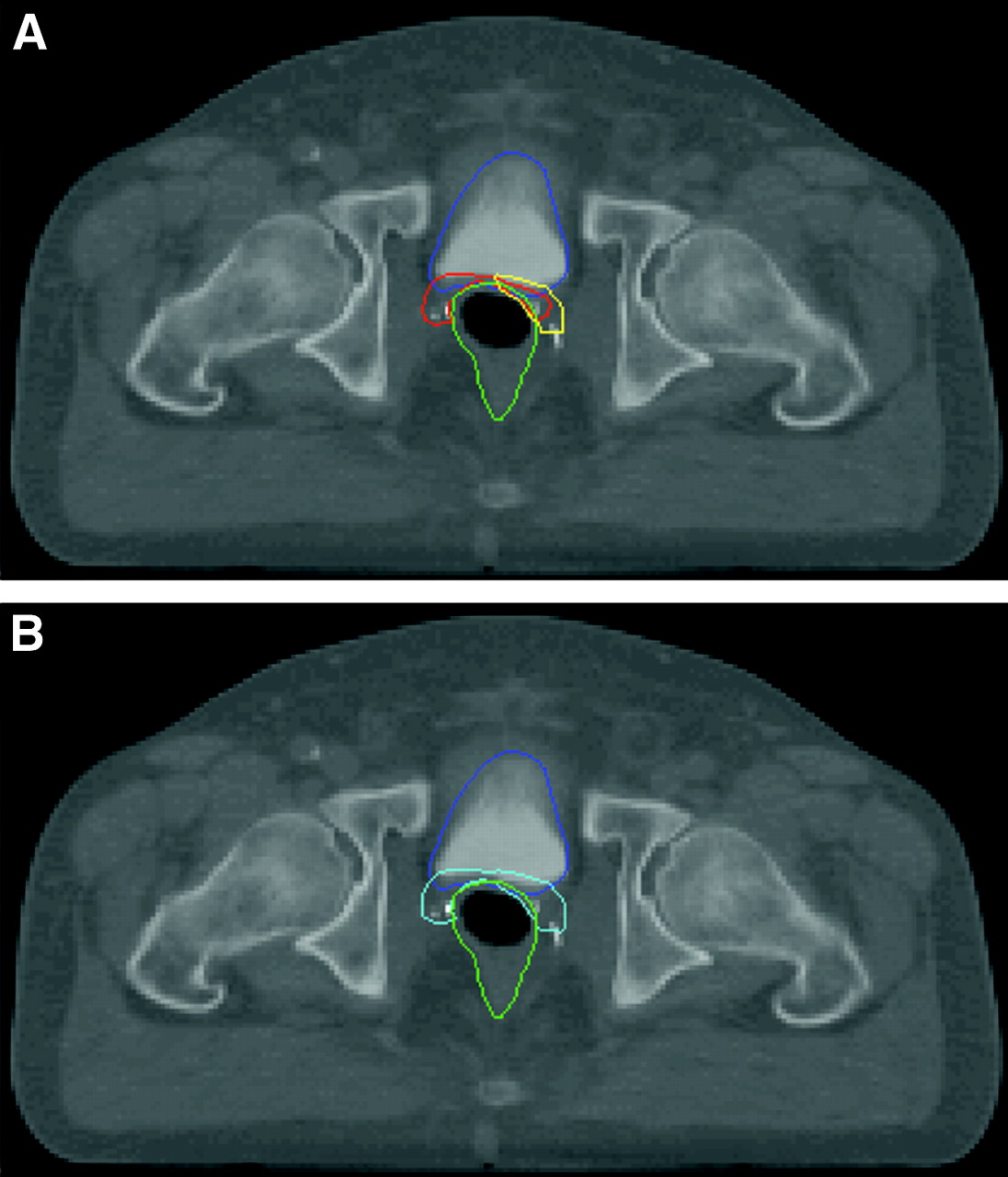
Finally, this projection of CTVRIS in the planning CT was used in conjunction with the CTVpre described previously to assist in defining the final CTV, denoted as CTVpost. CTVRIS was used in a variety of different manners for patients under study. Figure 2 is an example of an axial CT slice showing the bladder and rectal contours and CTVpre and CTVRIS (A) and CTVpost (B). In some cases, as in Figure 2, CTVpost was the union of the CTVpre and CTVRIS targets. In many other cases, however, the CTVRIS was used to subtly change the shape or location of CTVpre. CTVpost was recovered from the original electronic archives for all patients and was important because it was this volume that was actually used as a target for treatment.

Axial images of planning CT showing the use of RIS in modifying the prostate-bed CTV. Normal structures: bladder (blue), and rectum (green). (A) The CTVpre (red) was entered before the RIS/CT fusion. CTVRIS (yellow) is the projection of the delineated uptake on the RIS scan into the planning CT. (B) CTVRIS was used to modify CTVpre to define CTVpost (aqua). In this case, CTVpost is the union of CTVpre and CTVRIS in A.
For each patient, the absolute volume (in cm3) of CTVpre was compared with that of the corresponding CTVpost. Although the change in absolute volume serves as a measure of the impact of RIS on the design of the CTV, it does not take into account the shape or location of the CTV. In particular, even if the CTVpre and CTVpost were similar in absolute volume, the location of CTVpost may have been subtly different from that of CTVpre, and it was necessary to take into account the relationship of the CTV with the surrounding structures, principally the bladder and rectum. To address this issue, the RT treatment plans generated using CTVpre were compared with those generated using CTVpost to quantitate the dosimetric effects of these CTV differences on the bladder and rectum dose volume histograms (DVHs).
As mentioned previously, CTVpost was used for patient treatment. However, the ways in which CTVpost was used varied. As shown in Table 1, a more generous (i.e., whole pelvis) volume was used to treat 2 patients initially, particularly where there was a portion of CTVRIS away from the prostate bed or a high risk of pelvic nodal involvement based on PSA records or prostatectomy findings. Under these few circumstances, CTVpost was used only during the final phase of the treatment. In the vast majority of cases, however, CTVpost was used for the entire treatment. Because the portion of the CTV away from the prostate bed was not the focus of the current investigation, for purposes of understanding the dosimetric influences of the RIS information, the comparison of CTVpost versus CTVpre was made considering CTVpost to be used for the entire duration of treatment.
The planning target volumes (PTVs) were defined as 1-cm expansions around the respective CTVs. That is, to perform the dosimetric analysis, CTVpre was uniformly expanded by 1 cm to define PTVpre, and CTVpost was uniformly expanded by 1 cm to define PTVpost. Because the treatment techniques evolved in our hospital consortium over the time frame of the investigation, it was necessary to use a uniform analysis strategy. Specifically, the prostate bed RT was delivered using 4-field treatment, 6-field conformal therapy, or intensity-modulated RT (IMRT) (Table 1). In addition, a variety of treatment planning software packages (and several different versions of these packages) were used. Thus, to perform a uniform comparison of the dosimetric consequences when using PTVpost and PTVpre, for this investigation the planning was done using 6-field conformal therapy. The authors are aware of recent efforts documenting the probable advantages of IMRT in the postprostatectomy setting (30). Indeed, for this reason 10 of the 25 patients in the later years of the current study received IMRT. However, the technique used in this study was chosen because the majority of patients under study were treated using the 6-field technique. Using a 1-cm expansion from PTVpre to block edge, a 6-field conformal treatment plan using 18-MV photons was generated for all 25 patients, using the same beam angles and weightings for each patient. The same prescription dose (66 Gy) was based on the consensus conference (31). The dose was prescribed to the PTV (i.e., minimum target dose, not isocentric), and the fraction size was 2 Gy, delivered once daily. Then, with the same beam angles, weightings, energy, and prescription dose, the plan was rerun for each patient using PTVpost (again, expanded uniformly by 1 cm to block edge) to compare the differences in bladder and rectal DVHs. This methodology allowed a uniform and consistent comparison of the dosimetric consequences of the CTV modifications in a manner that held constant other variables influencing dosimetry.
To compare the bladder and rectal DVH systematically, 2 parameters were chosen: area under the curve (AUC) and volume of bladder or rectum receiving ≥60 Gy (V60). These endpoints were chosen, in part, because they measure different consequences. AUC is a measure of integral dose to the structure and has been shown by some investigators to correlate with gastrointestinal (GI) and genitourinary (GU) toxicity during prostate treatment (32). However, others have demonstrated that the rectum and bladder may be serial structures, so the volume of the organ receiving high doses may be better correlated with toxicity (33). For this reason, the V60 analysis was also included. Figure 3 illustrates the chosen endpoints. Similar to the absolute CTV volume analysis, the AUC and V60 endpoints were compared using 2-tailed t tests (34). Dose calculations for the AUC and V60 analyses were performed using standard conformal RT treatment planning tools without tissue inhomogeneity corrections. Any small residual radiation from excretion of the radionuclide (from the RIS scan, which was usually performed several days before the planning CT scan) on the bladder DVHs was clinically negligible, because patients were typically treated with fractionated external-beam RT beginning 1–2 wk after the planning CT scan, continuing for 6–8 wk thereafter.
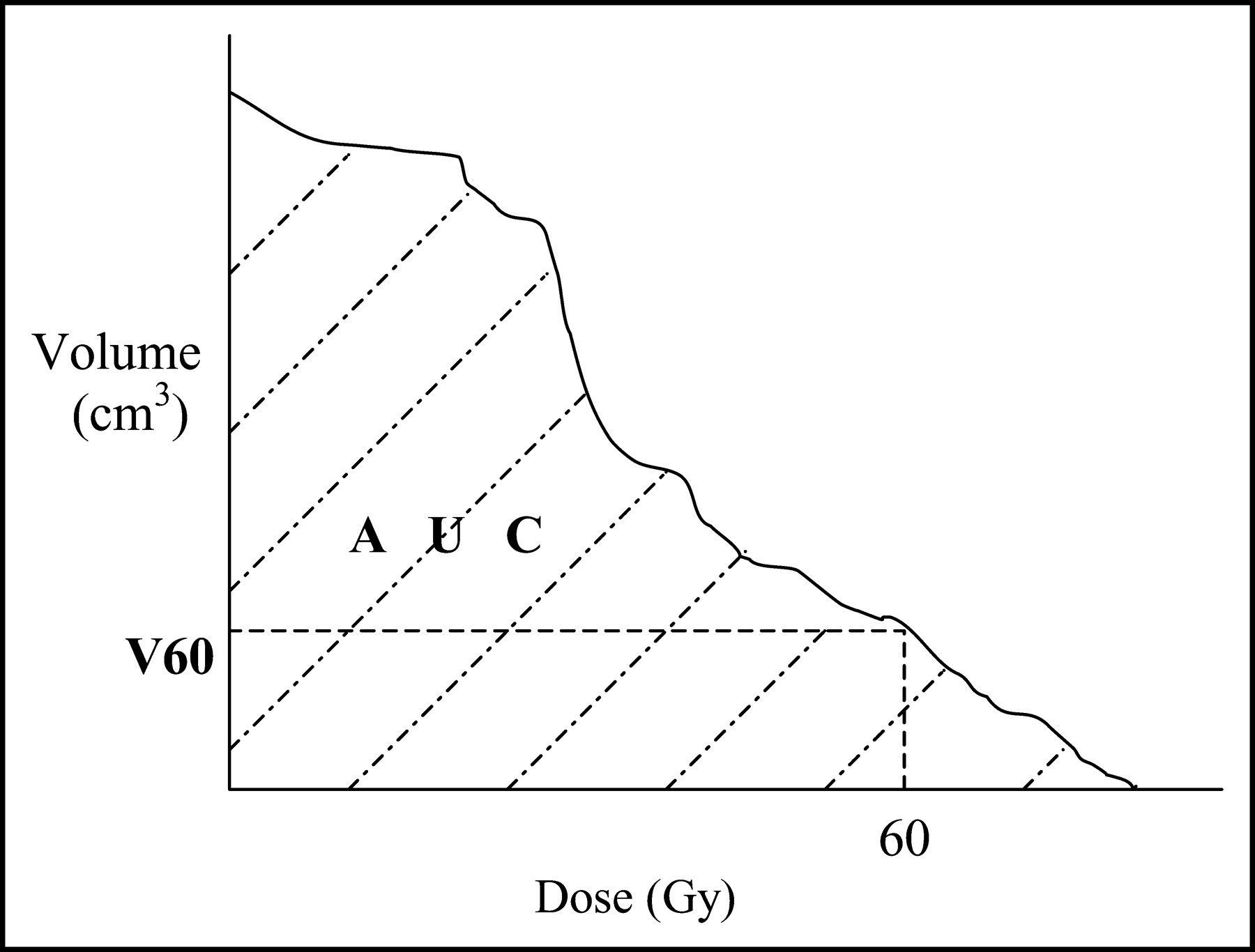
Dose volume histogram dosimetric endpoints for bladder and rectum. AUC = hatched area.
In addition to the toxicity analysis, an analysis of cancer control was undertaken. Specifically, a Kaplan–Meier curve was generated for biochemical failure-free survival, based on available follow-up PSA information after RT (35). The definition of biochemical failure was the presence of 2 consecutive PSA rises above the level of 0.2 ng/mL. This definition combines features of definitions relying on successive rises and others relying on reaching an absolute threshold value to declare failure (4–10).
RESULTS
Table 2 displays the results of the volumetric analysis comparing CTVpre (the CTV designed without knowledge of the RIS findings) with CTVpost (the prostate bed CTV designed after the RIS/planning CT fusion). As shown, the CTVpre volume was 24.4 ± 10.2 cm3 (mean ± SD) and the CTVpost volume was 35.0 ± 21.2 cm3. This volumetric difference was found to be significant (P = 0.032).
Volumetric Analysis
Table 3 displays the rectum and bladder dosimetric analyses. This table shows the absolute rectal and bladder volumes, which, as a result of differences in patient anatomy, varied considerably despite consistency in definition. The V60 and AUC statistical comparisons were performed. For the rectum, the V60 results were (using PTVpre and PTVpost) 32.7 ± 15.9 cm3 and 41.0 ± 25.1 cm3, respectively (P = 0.168). The rectum AUC results (using PTVpre and PTVpost) were 4,027 ± 1,878 Gy × cm3 and 4,516 ± 2,151 Gy × cm3, respectively (P = 0.396). These V60 and AUC analyses suggest that PTVpost was not significantly different from PTVpre in terms of overlap with the rectum. Also displayed in Table 3 are the V60 and AUC results for the bladder. The bladder V60 results (using PTVpre and PTVpost) were 33.9 ± 13.0 cm3 and 46.6 ± 21.2 cm3, respectively (P = 0.015). The AUC results (using PTVpre and PTVpost) were 4,782 ± 1,584 Gy × cm3 and 5,561 ± 1,873 Gy × cm3, respectively (P = 0.119). Thus, these results suggest that although there was not a significant influence on integral dose to the bladder, using PTVpost for treatment planning resulted in a higher volume of bladder receiving a high dose than when using PTVpre, probably as a result of PTVpost being closer to or overlapping with the bladder to a greater extent than the corresponding PTVpre. This is an expected result, given the fact that often the CTVRIS is projected at or close to the bladder neck in many cases.
Dosimetric Analyses for Rectum and Bladder
Table 4 shows the observed treatment toxicity, using RTOG acute- and late-toxicity grading criteria (36,37). It should be noted that a patient could belong to more than a single category (e.g., acute GI and late GU toxicity could develop in a patient). The reported toxicity is the highest recorded (i.e., a patient would not belong to both the grade 2 and grade 1 acute GI toxicity groups). In addition, although all 25 patients could be analyzed for acute toxicity, only 21 could be analyzed for late toxicity, because 4 patients did not have sufficiently long follow-ups after RT. It should be noted that this toxicity summary corresponds to the treatment plans and fields actually used to treat, not the standard 6-field PTVpost plans used in making comparisons with the PTVpre plans. Nevertheless, toxicity analysis serves as a reasonable means of estimating the toxicity of treating using PTVpost for the entire duration. As shown, toxicity results were generally acceptable. Although the rate of acute grade 2 GI toxicity (most commonly, diarrhea requiring medication) was somewhat high (9/25, or 36%), the medication required was nonprescription loperamide in all cases (corresponding to mild grade 2 GI toxicity). As Table 4 show, no grade 3, 4, or 5 (acute or late GI or GU) toxicity was observed.
Toxicity Analysis
Figure 4 shows the Kaplan–Meier biochemical failure-free survival curve. As displayed, the 2-y biochemical failure-free survival was 87% for the cohort. It should be noted that although the range of available follow-up data extends to several years (Table 1), the average follow-up is slightly greater than 1 y.

Kaplan–Meier curve displaying biochemical failure-free survival for the cohort.
DISCUSSION
Previous reports of the role of RIS in the setting of RT document the role of RIS as a diagnostic test (16–23). The current report extends this previous work in a different direction, to the use of RIS in guiding prostate bed CTV definition. The current analysis suggests that RIS may provide information complementary to that provided using standard methods for the task of CTV definition. Although other investigators have made progress in using RIS for designing the volume to be treated with brachytherapy or external-beam RT in the setting of the intact prostate (38), the current investigation focused on the role of RIS in aiding the target definition in the postprostatectomy setting.
Formal analysis suggests that incorporating RIS uptake results in significant modification in the volume of the postprostatectomy CTV, with the incorporation of the RIS uptake in the majority of cases causing the volume of CTVpost to be larger on average than that of the corresponding CTVpre. This suggests that projecting the RIS findings into the planning CT scan is feasible and may serve as a tool (in addition to prostatectomy pathologic findings and planning CT) to guide the radiotherapist in defining the prostate bed CTV.
Concerns may arise about whether treatment to these larger volumes will result in additional toxicity. However, the dosimetric consequences of the CTV modifications on the rectum did not reach significance. Moreover, the CTV modifications did not appear to adversely affect the integral dose to the bladder. The CTV modifications based on the RIS uptake regions did appear to have an effect on the volume of bladder receiving high doses, however. This may be a cause for concern, particularly if dose escalation is performed to the CTVpost. However, many of these concerns can be alleviated, because no grade 3, 4, or 5 (acute or late GI or GU) toxicities were seen, suggesting that treatment to the modified CTV is tolerable.
Several observations about the toxicity analysis bear mention. First, the dosimetric analysis was performed using a uniform planning technique, despite the fact that patients were treated with heterogeneous techniques (in many cases, treatment techniques such as the 4-field or 6-field technique) that would be considered outdated and more prone to toxicity than newer techniques such as IMRT. Thus, the current analysis may slightly overestimate the toxicity of treatment expected using modern treatment techniques. Second, in some patients, treatment was to the whole pelvis, although for the purposes of comparing PTVpre and PTVpost, they were considered to receive RT only to the prostate bed. Again, this would serve to increase the toxicity over that which would be expected from treating the prostate bed for the entire duration of treatment. Third, it cannot be known with certainty what the toxicities would have been if PTVpre had been used for treatment planning and delivery. In other words, patients can serve as their own controls for the type of dosimetric/volumetric analyses reported here but cannot serve as their own controls for the toxicity analysis. To analyze this problem more accurately, a matched-pair control group treated without knowledge of the RIS information requires identification and analysis, which is outside the scope of the current investigation. An even more valid approach, of course, would be a randomized single-blinded study. Such a trial ideally would be multiinstitutional and adequately statistically powered to determine the toxicity and biochemical control differences when using the RIS/CT correlation.
Several issues regarding the survival curve warrant comment. First, the follow-up of the current cohort, treated with radiation planning using a new technology (RIS/CT vessel registration), is relatively short in relation to the known long natural history of prostate cancer. However, the results can still be interpreted, because early failures are common in the postprostatectomy RT setting. With the available follow-up, the biochemical failure-free survival is similar to or slightly higher than that reported in most post-RRP RT series (9–14). As with toxicity analysis, because the patients undergoing the RIS/CT correlation for RT treatment planning cannot serve as their own controls for survival analysis, a matched-pair control group requires identification and analysis to determine the true impact of the RIS/CT correlation on biochemical control.
The authors recognize that there may be biases related to intra- and interobserver variability, particularly because no existing guidelines have been published on integrating RIS information into the design of radiation treatment plans. Although we recognize these biases, we believe that because our study spanned several institutions and several providers, the results are generally representative of those likely to be obtained with RIS in the general RT community. The biases and limitations inherent in the retrospective nature of the analyses reported here are understood by the investigators. Within these limitations, however, the current investigation does shed light on the use of RIS in the setting of guiding postprostatectomy CTV definition. It is hoped that the current communication can provide a preliminary framework on which to design a prospective investigation evaluating the role of RIS in postprostatectomy CTV definition.
CONCLUSION
Incorporating RIS uptake resulted in significant modifications in the postprostatectomy definition of the CTV for RT treatment planning, suggesting that projecting the RIS findings into the planning CT scan is feasible and may serve as a tool (in addition to prostatectomy pathologic findings and planning CT) to guide the radiotherapist in defining the prostate bed CTV. The consequences of these modifications on the rectum V60 or AUC or on the bladder AUC were not significant, although the bladder V60 did increase. However, observed toxicity was low, with acceptable short-term biochemical control, suggesting that treatment to the modified CTV was tolerable.
Acknowledgments
This work was supported in part by Cytogen Corp. The authors wish to thank Brett Smith, Julius Turian, and Karl Farrey for their help in acquiring the necessary data for analysis.
Footnotes
Received Aug. 15, 2003; revision accepted Oct. 14, 2003.
For correspondence or reprints contact: Ashesh B. Jani, MD, Department of Radiation and Cellular Oncology, University of Chicago Hospitals, 5758 S. Maryland Ave., MC 9006, Chicago, IL 60637.
E-mail: jani_1969{at}yahoo.com
REFERENCES
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Impact of 18F-Fluciclovine PET on Target Volume Definition for Postprostatectomy Salvage Radiotherapy: Initial Findings from a Randomized Trial
- The Role of Indium-111 Radioimmunoscintigraphy in Post-Radical Retropubic Prostatectomy Management of Prostate Cancer Patients
- Radioimmunoscintigraphy for Postprostatectomy Radiotherapy: Analysis of Toxicity and Biochemical Control
- Influence of Radioimmunoscintigraphy on Postprostatectomy Radiotherapy Treatment Decision Making