


Abstract
This study was undertaken to assess the feasibility of lymphoscintigraphy of the gastric cardia and to identify the incidence of paraesophageal lymphatic drainage, precluding total gastrectomy with esophagojejunostomy as a potentially curative therapy for gastric cardia cancer. Methods: Ten patients scheduled for esophagectomy with high-grade dysplasia or with esophageal cancer at least 3 cm above the esophagogastric junction were enrolled in this study. Preoperatively, 111 MBq of99mTc-labeled nanocolloid (n = 5) or sulfur colloid (n = 5) were injected into the submucosa of the tumor-free cardia. Subsequently, lymphoscintigraphy in combination with CT was obtained. Locoregional lymph node stations were measured for radioactivity by a γ-probe intraoperatively and ex vivo in the resection specimen. Results: In each patient, at least 1 radioactive lymph node station was detected. In total, 42 radioactive lymph node stations were detected by γ-probe. Of those 42 areas, 38 (90%) were visible at preoperative lymphoscintigraphy. In the group of 5 patients in whom nanocolloid was used, a median of 2 (range, 1–4) node stations per patient was identified, whereas when sulfur colloid was administered a median of 6 (range, 4–8) active lymph node stations per patient could be detected (P < 0.002). Paraesophageal drainage was identified in 1 patient. Conclusion: Lymphoscintigraphy of the gastric cardia is feasible and can accurately determine the location of radioactive lymph nodes. Early paraesophageal lymphatic drainage is rare.
Although some authors consider adenocarcinoma of the distal esophagus and gastric cardia a single clinical entity, we and others have suggested that both intestinal metaplasia (i.e., the precursor lesion of adenocarcinoma) and carcinomas in the cardia or distal esophagus should be regarded as separate entities (1,2). Regional metastases of carcinomas of the distal esophagus are primarily found in the mediastinal nodes, whereas lymphatic spread from the gastric cardia is reported to be mainly to the abdomen (3,4). In many centers, gastric cardia carcinoma not substantially infiltrating the distal esophagus is treated by total gastrectomy, without dissection of the paraesophageal or mediastinal lymph nodes. However, in a prospective study of 22 patients who underwent total gastrectomy and distal esophagectomy, Wang et al. found paraesophageal metastases in 4 patients (18%) and diaphragmatic lymph node metastases in 4 patients (18%) (5). Some surgeons therefore advocate a more extensive resection in these patients by a subtotal esophagectomy plus proximal gastrectomy and gastric tube reconstruction or even a subtotal esophagectomy plus total gastrectomy and colonic interposition (6–8). In contrast, Stein et al. reported no survival benefit of esophagectomy over extended gastrectomy in patients with true carcinoma of the gastric cardia (9).
To determine the optimal surgical procedure for gastric cardia cancer, it is necessary to obtain better insight into the early lymphatic drainage of the normal gastric cardia area. The aim of this study was to assess the feasibility of lymphoscintigraphy of the normal gastric cardia area and to identify the incidence of early paraesophageal lymphatic drainage into the chest.
MATERIALS AND METHODS
Inclusion Criteria
Patients scheduled for subtotal esophagectomy with gastric cardia resection because of high-grade dysplasia or esophageal carcinoma were asked to participate in the study. The tumor had to be located at least 3 cm above the esophagogastric junction to minimize the disturbance of the normal physiologic lymphatic drainage of the cardia. Patients had to be between 18 and 80 y old. Approval of the study protocol was obtained from the institution’s ethical committee, and all patients gave witnessed written informed consent.
Endoscopy and Administration of Radiolabeled Colloids
On the last preoperative day, 111 MBq of 99mTc-labeled nanocolloid (particle size < 80 nm; Amersham Health) in 5 patients and 111 MBq of 99mTc-labeled sulfur colloid (particle size < 50 nm; Amersham Health) in another 5 patients was injected endoscopically (volume, 1.0 mL) into the submucosa of the gastric cardia. After the first 5 patients, nanocolloid was exchanged for sulfur colloid to investigate whether the use of a smaller particle size would show more intense adjacent lymph nodes and more distant lymph nodes on the lymphoscintigraphy. The endoscopic procedures were performed with a standard upper gastrointestinal endoscope (GIF-100 or GIF-140; Olympus Optical Co.). During this preoperative procedure, the endoscope was introduced with the patient in the left lateral position and was advanced into the esophagus. The injection site was chosen at the posterior wall of the lesser curvature, about 3 cm distal from the tubular esophagus. The radioactive tracer was injected into the submucosa using a standard 21-gauge needle (Boston Scientific Microvasive). This needle had a dead volume of 1.0 mL, for which the total volume and activity to be injected was corrected. After injection, the injection site was marked with an endoscopically placed hemoclip (Olympus Optical Co.) for future reference.
Lymphoscintigraphy
Lymphoscintigraphy of the lower chest and upper abdomen was performed early (15–30 min) and late (4 and 20 h) after injection of the radioactive tracers with a dual-head γ-camera (Millennium; GE Medical Systems). Planar anterior and posterior acquisitions (600 s; 128 × 128 matrix) were obtained at all time points. SPECT (128 × 128 matrix) was performed at 4 and 20 h after injection. In the last 5 patients, tracer accumulation was localized by CT (Hawkeye; GE Medical Systems) (Fig. 1).

Radioactivity in paraesophageal lymph nodes (PE) as identified preoperatively by lymphoscintigraphy in combination with CT. Shown are CT scan (left), scintigram (middle), and a combination of CT scan and scintigram (right). This sagittal projection also shows the injection site (IS) at the gastric cardia and celiac trunk nodes (CTN). See also patient 9 in Table 1.
Before surgery, paraesophageal lymph node drainage was predicted scintigraphically by consensus reading (nuclear medicine physician and surgeon). The specific lymph node stations were retrospectively evaluated using the visualization on the various scintigraphic acquisitions in combination with the knowledge of the peri- and postoperative probe measurements (reference standard; vide infra).
Patent Blue Administration, Surgical Resection, and Probe Measurement
Surgery was started shortly after the last scintigraphic acquisition. Immediately after induction of anesthesia, a second endoscopic procedure was performed. The endoscopically placed hemoclip was identified in the cardia, and at the same site, patent blue (sterile patent V 2.5% in aquadest and mannitol 5%; raw material from Brunschwig Chemie) was injected into the submucosa using a similar standard 21-gauge needle (Fig. 2). Subsequently, all patients underwent subtotal esophagectomy plus gastric cardia resection with limited lymph node dissection under direct vision by a transhiatal approach via a widened hiatus. After completion of the resection, nondissected regional lymph node stations were systematically measured in vivo for radioactivity using a γ-probe (Europrobe; PI Medical). Background measurements were performed on the jejunum and liver. Thereafter, the resection specimen itself was measured ex vivo for radioactivity, by γ-probe, in the Nuclear Medicine Department. For verification, a scintigram of the resection specimen was obtained (Fig. 3). Lymph node drainage areas were considered positive for radioactivity when the probe measurement exceeded twice the background level, with a minimum of 30 counts per second (cps). Subsequently, the Pathology Department determined whether the specimen had blue nodes.

Perioperative endoscopic injection of patent blue at the site (clip) where radioactive technetium was injected the previous day.
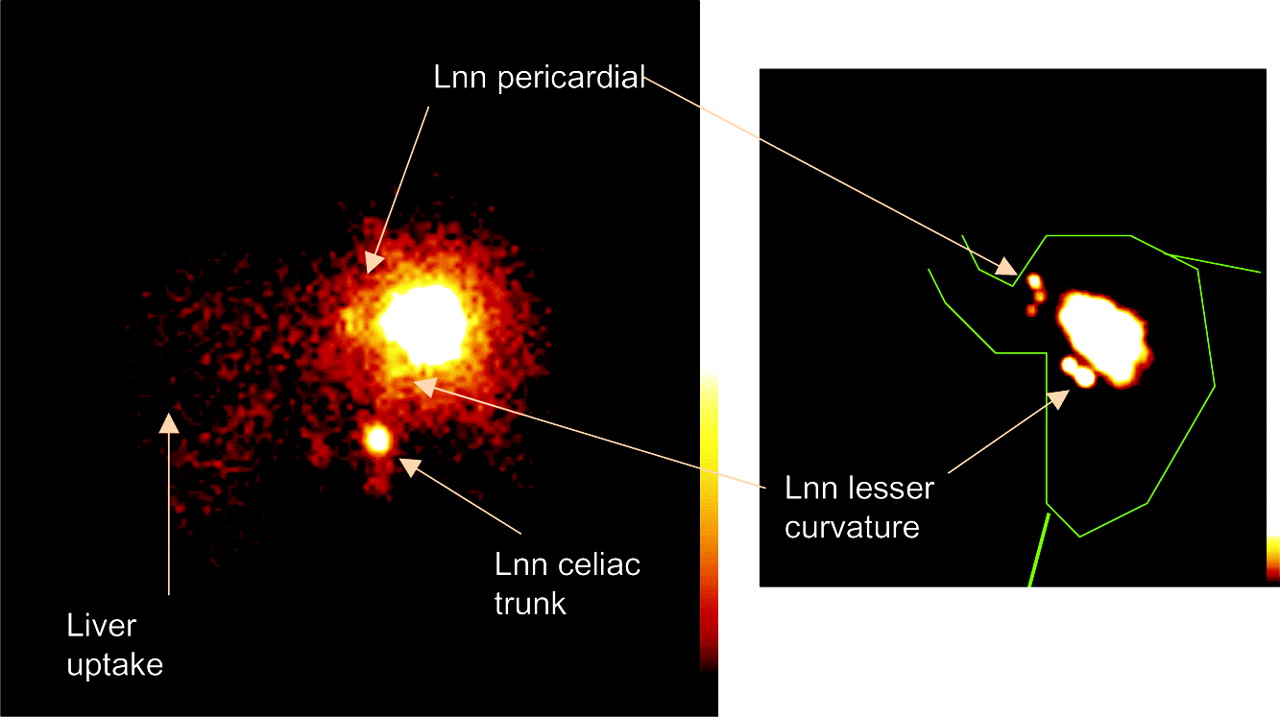
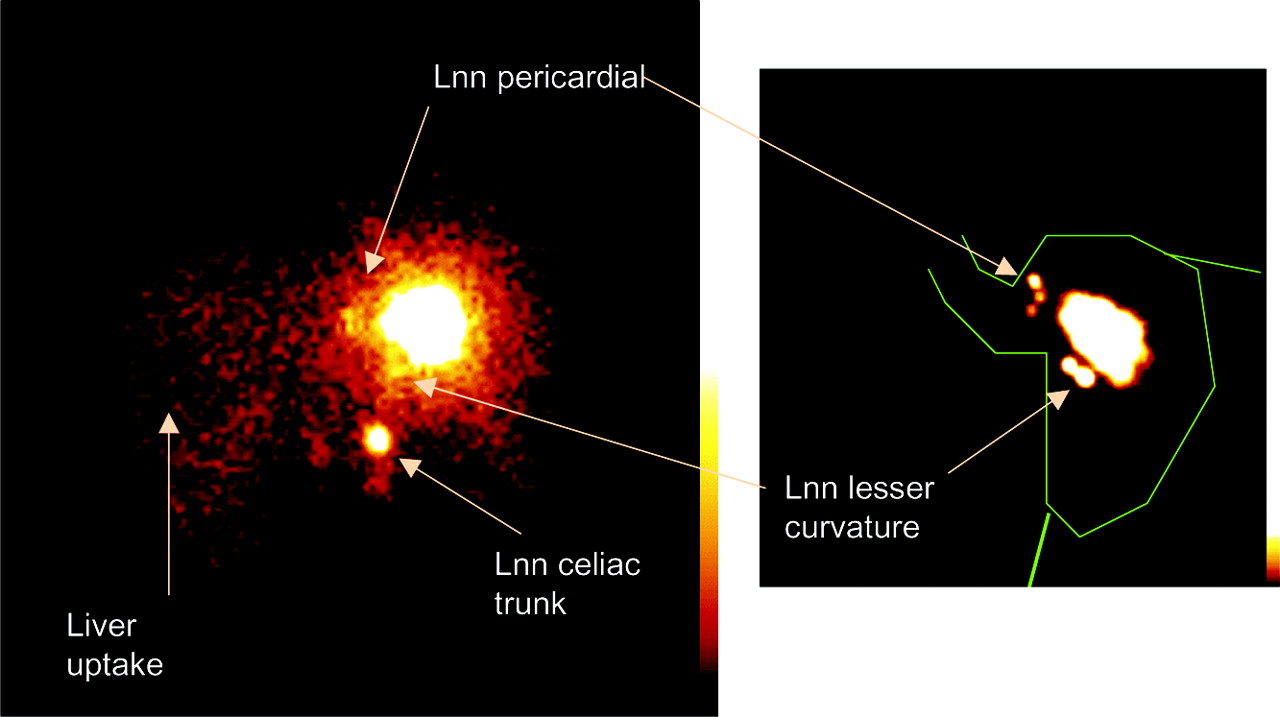
In vivo and ex vivo lymphoscintigraphy of the same patient (patient 4). On the left is a lymphoscintigram of the patient immediately before surgery (i.e., 20 h after injection of technetium-labeled nanocolloid). On the right is a lymphoscintigram of the resected specimen immediately after surgery. The green lines indicate the contours of the resection specimen (esophagus–cardia) and an additional imaginary contour of the stomach. Lnn = lymph node.
Statistical Analysis
The Mann–Whitney U test was used to compare the number of active lymph node stations as shown by scintigraphy in patients using nanocolloid as a technetium-labeled tracer (n = 5) and the number of active lymph node stations in patients using sulfur colloid as a technetium-labeled tracer (n = 5).
RESULTS
Patient Characteristics
Originally, 12 patients were included in the study. Two patients were excluded from further analysis because, in one, the endoscope could not pass the tumor and, in the other, the tracer was erroneously administered in the gastric lumen instead of the gastric cardia submucosa. The 10 patients who could be evaluated were all male, with a median age of 62 y (range, 47–74 y). Three patients were operated on for high-grade dysplasia, 4 patients for esophageal adenocarcinoma, and 3 patients for squamous cell carcinoma. The distance from the incisor teeth varied from 31 to 34 cm for high-grade dysplasia and from 25 to 35 cm for cancer.
Preoperative Lymphoscintigraphy
Early images could not be obtained in 3 instances: once because of noncompliance after sedation before endoscopy and twice because the camera was not available. In 7 patients, early images were acquired, and in only 1 of these 7 could transport of tracer be identified (patient 8, toward the celiac trunk).
Sites of scintigraphic drainage activity as detected 4 and 20 h after injection were similar. However, despite physical decay of the radioisotope, the 20-h-postinjection images were superior to the 4-h-postinjection images because of less hindrance from overprojection of the injection site.
In one patient (patient 9), paraesophageal drainage was clearly present on the late images (4 and 20 h after injection) (Fig. 1). In the remaining 9 patients, transport of tracer to paraesophageal nodes was not observed. A typical example is shown in Figure 3: active pericardial lymph nodes and activity at the lesser curvature and celiac trunk, but without paraesophageal drainage.
Preoperative lymphoscintigraphy correctly identified 38 of the 42 (90%) radioactive lymph node stations as detected by peri- and postoperative γ-probe measurements (Table 1).
Number of Active Lymph Node Stations Identified In Vivo During Surgery and in Resection Specimen After Surgery, in Relation to Preoperative Lymphoscintigraphy
In the 4 areas (in patients 2, 8, and 10) where lymphoscintigraphy failed to reveal radioactive lymph nodes found by probe measurements (false-negative lymphoscintigraphy findings), the amount of radioactivity as measured by γ-probe was small, ranging from 35 to 110 cps.
Peri- and Postoperative γ-Probe Measurements
In every patient, at least 1 radioactive lymph node station was detected peri- or postoperatively using a γ-probe. In total, 42 lymph node stations were detected: 8 in the celiac trunk, 2 in the splenic hilum, 6 in the splenic artery, 1 in the hepatoduodenal ligament, 2 in the mesenteric root, 3 paraaortal, 5 right paracardial, 5 left paracardial, 9 in the lesser curvature, and 1 paraesophageal.
The number of radioactive lymph node stations per patient is listed in Table 1. In the group of 5 patients in whom nanocolloid was administered, a median of 2 (range, 1–4) active lymph nodes stations per patient could be detected, whereas a median of 6 (range, 4–8) lymph node stations per patient was identified when sulfur colloid was used (P < 0.002; Mann–Whitney U test). The counting rate in the nodes with accumulation of nanocolloid ranged from 40 to 450 cps (median, 226 cps), versus 30 to 2400 cps (median, 230 cps) in the lymph nodes with accumulation of sulfur colloid.
In the 1 patient with paraesophageal lymph node drainage on preoperative scintigraphy (Fig. 1; patient 9), a blue paraesophageal lymph node was identified but no radioactive accumulation could be detected by γ-probe in the resection specimen ex vivo. In this same patient, another 6 active lymph nodes were detected by perioperative probe measurements and by postoperative probe measurements of the specimen.
Of the 19 radioactive nodes measured by γ-probe in the specimens, only 7 were blue. In the lymph node stations that remained in situ, the presence of patent blue could not be assessed accurately and therefore has not been evaluated.
DISCUSSION
This study showed that lymposcintigraphy of the gastric cardia is feasible and adds to our knowledge of the lymphatic pathways of the gastric cardia. In the future, this technique might be helpful to determine the optimal surgical procedure for patients with cancer of the gastric cardia.
The study used techniques recently developed for the visualization of lymphatic drainage in other tumor types (especially breast cancer and melanoma). In these types of cancer, the objective is to determine the sentinel nodes of the tumor in a particular lymph node area: for example, the axilla in breast cancer or the groin in melanoma of the lower limb. This study, however, did not investigate the visualization of sentinel nodes in stricto sensu. The objective was to assess the feasibility of lymphoscintigraphy of the gastric cardia and to determine the normal lymphatic drainage, including first- and second-echelon lymph nodes of the normal, nonmalignant gastric cardia. Baciewicz et al. showed the feasibility of lymphoscintigraphy of the esophagus in a canine model. After submucosal injection of radiolabeled99mTc-antimony sulfide colloid in 6 dogs, lymph nodes were identified on nuclear scans (10). The expected position of lymph nodes based on the scans correlated with the location of the radiolabeled nodes at anatomic dissection.
In the first part of this study, medium-sized nanocolloid was administered as is used in, for example, breast cancer, but the radiolabeled colloid was subsequently changed into the small-sized sulfur colloid to enhance transport of the radiotracer. Indeed, sulfur colloid appeared to be superior to nanocolloid for this purpose, because with sulfur colloid more lymph nodes could be visualized. Moreover, the enhanced transport from the injection site to these lymph nodes resulted in less hindrance from overprojection by the injection site. This study indicated that 1 late scintigram (3–4 h after injection) is sufficient to obtain optimal information on lymphatic drainage of the upper digestive tract. Endoscopic injection of the radiolabeled colloid at the gastroesophageal junction was relatively easy. Because the injection site was marked by a clip, patent blue could be injected at the same site just before surgery. The 4 radioactive lymph node stations that were identified intraoperatively by probe but were negative at preoperative scintigraphy (Table 1) contained relatively low count rates and were in the center of the abdomen and therefore prone to attenuation. In addition, lymphoscintigrams of obese patients were more difficult to read than were those of nonobese patients.
Because the study concerned feasibility, preoperative lymphoscintigrams were interpreted postoperatively with knowledge of peri- and postoperative probe measurements. Nevertheless, it appeared feasible to attribute accumulation of radioactivity to specific lymph node stations. However, discrimination may still be difficult between, for example, right paracardial lymph nodes and lymph nodes along the lesser curvature, or between celiac trunk nodes and lymph nodes adjacent to the pancreas. Moreover, the combined use of CT and lymphoscintigraphy improves precise localization of groups of radioactive nodes (Fig. 1).
In this study, patent blue was detected in only half of the radioactive lymph nodes in the resection specimen, probably because of manipulation of the specimen during operation and because of the time span between injection and the search for blue nodes (the blue dye might already have passed the lymph nodes). The blue dye was injected into the cardia by an endoscopic procedure just before surgery. The specimen was investigated for the presence of blue nodes 3–4 h later. The optimal procedure for detecting lymphatic spread using blue dye may therefore be to inject the blue dye intraoperatively, just before resection. This strategy was used in 3 studies evaluating the potential role of sentinel node biopsy in gastric cancer (11–13). Another problem with blue dye was a discrepancy with the radiotracer in a patient (patient 9) with paraesophageal drainage. The discrepancy might be explained by a slight difference in the localization of the injection site between the blue dye and the radiotracer. Therefore, the blue and radioactive dyes probably followed different lymphatic pathways. In this study, 1 injection site was used to visualize the lymphatic drainage routes of the normal gastric cardia. However, the primary lesion in gastric cardia cancer may be more widely spread. Therefore, multiple peritumoral injections of the radiolabeled technetium and the blue dye might be wise when, in future studies, lymphatic drainage routes of gastric cardia cancer are investigated.
Wang et al. found positive nodes along the left proximal side (32%) and right distal side (18%) of the greater curvature in 42 patients undergoing extended radical total gastrectomy for adenocarcinoma of the gastric cardia (5). Siewert et al. analyzed a group of 1,002 patients with adenocarcinoma of the gastroesophageal junction (14). A subanalysis of the lymphatic spread of 186 lymph node metastases in 271 patients with type 2 carcinoma (carcinoma of the cardia arising immediately at the esophagogastric junction) showed metastases along the greater curvature in 16.1% of patients. This finding indicates that a gastric tube made of the greater curvature is not the ideal reconstruction after a potentially curative gastroesophagectomy for gastric cardia cancer. In the same subanalysis, however, positive lymph nodes in the lower mediastinum (paraesophageal) were found in 15.6% of patients. In these patients, a total gastrectomy would not be curative. Total gastrectomy plus subtotal esophagectomy followed by colonic interposition would be necessary to cope with potentially positive lymph nodes both in the mediastinum and along the greater curvature. However, morbidity would be substantially increased. In our study, no radioactive lymph nodes were found along the greater curvature.
The preoperative lymphoscintigrams in this study showed clear patterns of lymphatic drainage. In 9 of 10 patients, we found radioactive lymph nodes at the lesser curvature. Although no radioactive lymph nodes were found at the greater curvature, radioactive lymph nodes on the left side of the cardia were found in 5 patients. Radioactive nodes were detected by scintigraphy along the esophagus in 1 patient and along the celiac trunk in 7 patients. The results of this study showed that in 9 of 10 patients, no lymphatic spread occurred from the gastric cardia toward the paraesophageal or mediastinal lymph nodes. The distribution of radioactive lymph nodes was comparable to the pattern of nodal disease found in a series of 48 patients with type 2 junctional adenocarcinoma (15). In only 2 of these 48 patients were posterior mediastinal metastatic lymph nodes found.
CONCLUSION
Lymphoscintigraphy of the gastric cardia is feasible. The scintigrams can accurately determine the location of radioactive lymph node stations in the mediastinum and upper abdomen. Lymphoscintigrams can detect 90% of the radioactive lymph node stations, as found by intraoperative (in vivo) and postoperative (ex vivo) probe measurements. The use of patent blue as a tracer for lymphatic spread adds no clear value. Paraesophageal drainage was present in only 1 of 10 patients. These preliminary data argue in favor of total gastrectomy without intrathoracic lymphadenectomy as a curative treatment in patients with gastric cardia cancer not invading the distal esophagus.
Footnotes
Received Sep. 15, 2003; revision accepted Oct. 20, 2003.
For correspondence or reprints contact: Huib A. Cense, MD, Department of Surgery, Suite G4-149, Academic Medical Center, Meibergdreef 9, 1105 AZ Amsterdam, The Netherlands.
E-mail: hacense{at}knmg.nl




{kind=link}
{kind=link}
{kind=link}