


Visual Abstract
Abstract
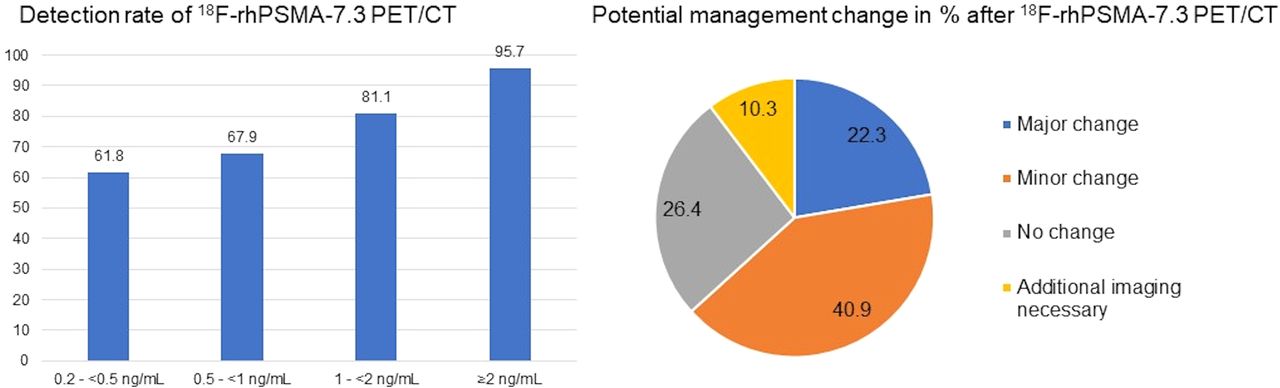
Radiohybrid prostate-specific membrane antigen (rhPSMA) ligands are a new class of 18F-labeled PSMA-targeting agents. 18F-rhPSMA-7.3 is a lead compound that is currently under investigation in 2 multicenter phase III trials for PET imaging. Here, we report the first retrospective data on its detection efficacy and potential impact on clinical management in a homogeneous cohort of patients with biochemical recurrence after radical prostatectomy and before any salvage therapy. Methods: In total, 242 patients (median prostate-specific antigen [PSA], 0.60 ng/mL; range, 0.2–60.8 ng/mL) who underwent 18F-rhPSMA-7.3 PET/CT were retrospectively selected from the institution’s database. Images were reread by an experienced nuclear medicine physician. Lesion detection rates were stratified by PSA. Further, potential management before and after PET was assessed by an interdisciplinary simulated tumor board and categorized (major vs. minor vs. no therapeutic change). The distribution of management change identified in each PSA subgroup was determined. Results: In total, 176 of 242 (72.7%) patients showed PSMA-ligand–positive findings. 18F-rhPSMA-7.3 detection rates were 61.8% (63/102), 67.9% (38/56), 81.1% (30/37), and 95.7% (45/47) for PSA levels of 0.2 to less than 0.5 ng/mL, 0.5 to less than 1 ng/mL, 1 to less than 2 ng/mL, and at least 2 ng/mL, respectively. 18F-rhPSMA-7.3 PET/CT revealed local recurrence, pelvic lymph node metastases, retroperitoneal lymph nodes metastases, supradiaphragmatic lymph nodes, bone metastases, and visceral metastases in 48.8% (n = 118), 28.9% (n = 70), 6.6% (n = 16), 1.2% (n = 3), 13.2% (n = 32), and 1.2% (n = 3) of patients, respectively. Notably, bone lesions were identified in 8.8% of patients (9/102) with a PSA of less than 0.5 ng/mL. Results from the tumor board indicated a change in therapeutic management in 153 of 242 patients (63.2%), with 54 (22.3%) considered major and 99 (40.9%) minor. 18F-rhPSMA-7.3 PET/CT did not prompt any therapeutic changes in 64 patients (26.4%). Conclusion: 18F-rhPSMA-7.3 PET offered high detection efficacy in patients with biochemical recurrence after radical prostatectomy and before potential salvage therapy and resulted in a potential change in treatment plan in nearly two thirds of patients.
Prostate cancer relapse after curative-intent primary therapy remains a considerable clinical challenge, with up to one third of patients experiencing biochemically recurrent disease (1,2). The utility of conventional imaging—as well as PET imaging using, for example, 11C-choline or 18F-FDG for the localization of recurrence—is limited, especially in patients with low prostate-specific antigen (PSA) levels (3). Several studies have already proven the high impact of prostate-specific membrane antigen (PSMA)–targeted radiopharmaceuticals on the clinical management of prostate cancer patients (4–6). 68Ga-PSMA-11 PET has been extensively assessed in multiple retrospective and prospective studies and is already recommended in various guidelines as the preferred imaging tool to localize recurrent disease (7–11). Along with improved detection efficacy in comparison to conventional imaging and PET using, for example, 11C-choline, the impact of 68Ga-PSMA-11 PET on the management of prostate cancer patients has been assessed in several studies (12–15). A recent metaanalysis investigating the impact of PSMA-ligand PET on the management of primary or recurrent disease reported management changes in approximately half of patients but found considerable heterogeneity among trials, depending on PSA level, PET positivity, and type of change definition (16). Further, a recent prospective trial in recurrent prostate cancer patients reported management changes in more than half of patients (17).
Recently, promising 18F-labeled PSMA ligands (e.g., 18F‐DCFPyL, 18F-PSMA‐1007, and 18F‐rhPSMA-7) have been developed using the superior nuclear properties of 18F, resulting in potential logistic and economic advantages (18–20). Radiohybrid PSMA (rhPSMA) ligands form a novel class of radiopharmaceuticals that can be labeled either with 18F or with radiometals (e.g., 68Ga, 177Lu, or 225Ac), offering unique options for both imaging and theranostic applications (21). 18F-rhPSMA-7 has already been assessed in staging and restaging of prostate cancer patients and has demonstrated high detection rates (22,23). 18F-rhPSMA-7 consists of 4 stereoisomers (18F-rhPSMA-7.1 to -7.4), and preclinical data comparing all 4 isomers in tumor-bearing mice identified rhPSMA-7.3 as the preferred isomer given its pharmacokinetics, high tumor accumulation, and low uptake in kidneys (24). Thus, single-isomer rhPSMA-7.3 has been evaluated in a phase I study (NCT03995888) of biodistribution and internal dosimetry in both healthy individuals and patients with prostate cancer. Further, its diagnostic performance in newly diagnosed intermediate- to high-risk prostate cancer and suspected disease recurrence is being investigated in 2 currently enrolling multicenter phase III studies (NCT04186819 and NCT04186845).
Therefore, the aim of this retrospective analysis was to assess the detection efficacy of 18F-rhPSMA-7.3 PET/CT and its impact on patient management in a highly selected homogeneous series of patients with biochemical recurrence after radical prostatectomy but before potential salvage treatment.
MATERIALS AND METHODS
Patients
In total, 242 patients with biochemical recurrence of prostate cancer who underwent clinically indicated 18F-rhPSMA‐7.3 PET/CT between September 2018 and October 2019 at our institution were reviewed retrospectively. Only patients who had undergone primary radical prostatectomy with curative intent were included. Patients with any documented salvage therapy (e.g., radiation therapy or salvage surgery) or the use of androgen deprivation therapy (ADT) after radical prostatectomy were excluded from the analysis. Patients had a median age of 72 y and a median prescan PSA level of 0.6 ng/mL (Table 1).
Patient Characteristics (n = 242)
All patients gave written informed consent to undergo the procedure. All reported investigations were conducted in accordance with the Helsinki Declaration and with national regulations. The retrospective analysis was approved by the local Ethics Committee (permit 99/19). The administration of 18F‐rhPSMA‐7.3 complied with the German Medicinal Products Act, AMG §13 2b, and the responsible regulatory body (Government of Oberbayern).
Synthesis of 18F‐rhPSMA‐7.3 and Imaging Protocol
18F‐rhPSMA‐7.3 was synthesized as described previously (24). A median activity of 332 MBq of 18F‐rhPSMA‐7.3 (mean, 336 ± 43 MBq; range, 206–454 MBq) was administered by intravenous bolus at a median of 73 min (mean, 75 ± 11 min; range, 58–117 min) before scanning.
All patients underwent 18F‐rhPSMA‐7.3 PET/CT on a Biograph mCT flow scanner (Siemens Medical Solutions). A diagnostic CT scan was performed in the portal venous phase 80 s after intravenous injection of contrast agent (iomeprol [Imeron 300; Bracco]) followed by the PET scan. All patients received diluted oral contrast medium (300 mg of ioxitalamic acid [Telebrix; Guerbet]) and 40 mg of furosemide. All PET scans were acquired in 3-dimensional mode with an acquisition time of 1.1 mm/s. Emission data were corrected for randoms, dead time, scatter, and attenuation and were reconstructed iteratively by an ordered‐subsets expectation maximization algorithm (4 iterations and 8 subsets) followed by a postreconstruction smoothing gaussian filter (5 mm in full width at half maximum).
Image Analysis
PET images were reviewed by a board‐certified nuclear medicine physician with 8 y of experience in reading oncologic images. All lesions suggestive of recurrent prostate cancer were noted. Any focal tracer uptake higher than blood-pool activity and not associated with physiologic uptake was considered suggestive of malignancy. Typical pitfalls in PSMA‐ligand PET imaging such as low‐to‐moderate PSMA expression associated with osteoblastic changes or in ganglia were considered (25). For lesion assessment, the Prostate Cancer Molecular Imaging Standardized Evaluation (PROMISE) criteria were used (26). All lesions suggestive of recurrent prostate cancer were noted and categorized as prostate bed, pelvic nodes, extrapelvic nodes, bone metastases, or visceral metastases using the miTNM framework.
Assessment of Potential Impact of 18F‐rhPSMA‐7.3 PET/CT on Patient Management
A simulated interdisciplinary tumor board was formed to assess potential management before and after 18F‐rhPSMA‐7.3 PET/CT. Therapeutic decisions by the tumor board were based mainly on national and international guidelines (e.g., German S3 Guideline on Prostate Cancer and the Guideline on Prostate Cancer of the European Association of Urology) (27,28). Since the category of oligometastatic prostate cancer is still insufficiently represented in the guidelines, some therapeutic decisions were also individual decisions considering, for example, recently published results on salvage lymph node dissection or PSMA radioguided surgery (29–33). The tumor board consisted of a urooncologist, a radiation oncologist, and a nuclear medicine physician experienced in oncologic imaging. First, all available clinical information (T- and N-stage, initial PSA at time of diagnosis, PSA nadir, time from radical prostatectomy to biochemical recurrence, and PSA level), but not results from 18F‐rhPSMA‐7.3 PET/CT, were presented. On this basis, tumor board members were asked for a consensus on their currently intended potential management. There was also the possibility that no potential baseline management plan could be defined by tumor board members on the basis of the clinical information.
In the second step, the presence and localization of recurrent disease on 18F‐rhPSMA‐7.3 PET/CT images was demonstrated by a nuclear medicine physician. Then, the tumor board members were asked to indicate post-PET management. Therapeutic management was grouped into 5 major modality groups: radiation therapy (local radiation therapy of the prostatic bed, radiation therapy to pelvic lymphatic drainage, stereotactic body radiotherapy), surgery (salvage lymphadenectomy, systemic therapy [e.g., ADT], hormone chemotherapy), multimodal therapy (a combination of radiation therapy/surgery and systemic treatment), and no therapy (e.g., active surveillance and follow-up). Finally, therapeutic change was categorized as major change, minor change, or no change. An intramodality change was considered a minor change, whereas intermodality changes were considered major changes, with the exception of ADT added to or removed from local therapy, which was considered a minor change. Furthermore, the presence of at least 2 minor changes was considered a major change, as well as a switch of systemic treatment (i.e., modality abiraterone/enzalutamide to chemotherapy), the addition of radiation to M1 lesions, and the addition of second-generation androgen receptor inhibitors, such as apalutamide, to systemic treatment. A detailed description of category changes can be found in Table 2.
Post-PET Management Pathway Category Details (n = 242)
Statistical Analysis
The detection rate of presumed recurrence sites was plotted against the baseline PSA value for both patient‐level recurrence (number of patients with at least 1 positive finding) and regional levels according to the miTNM classification. The Mann–Whitney U test was used to evaluate differences in PSA values between groups with and without pathologic uptake. Proportions of management change (major vs. minor change, no change) were determined. Further, the potential change in management is illustrated using a Sankey diagram that shows the selected therapies in relation to previous treatments with and without PET information. All tests were 2‐sided and used a significance level of α = 5%. Statistical analyses were conducted with MedCalc software (version 13.2.0, 2014).
RESULTS
18F‐rhPSMA‐7.3 Detection Efficacy
Detection Rate
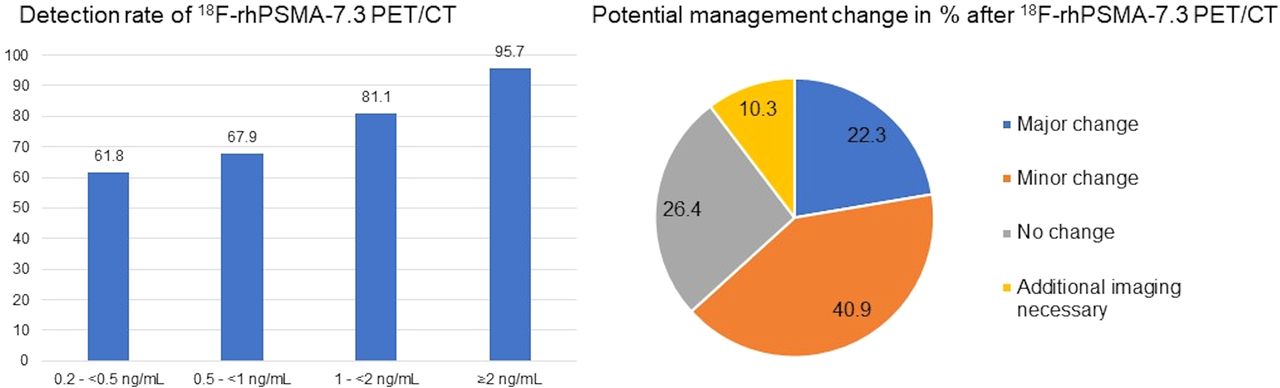
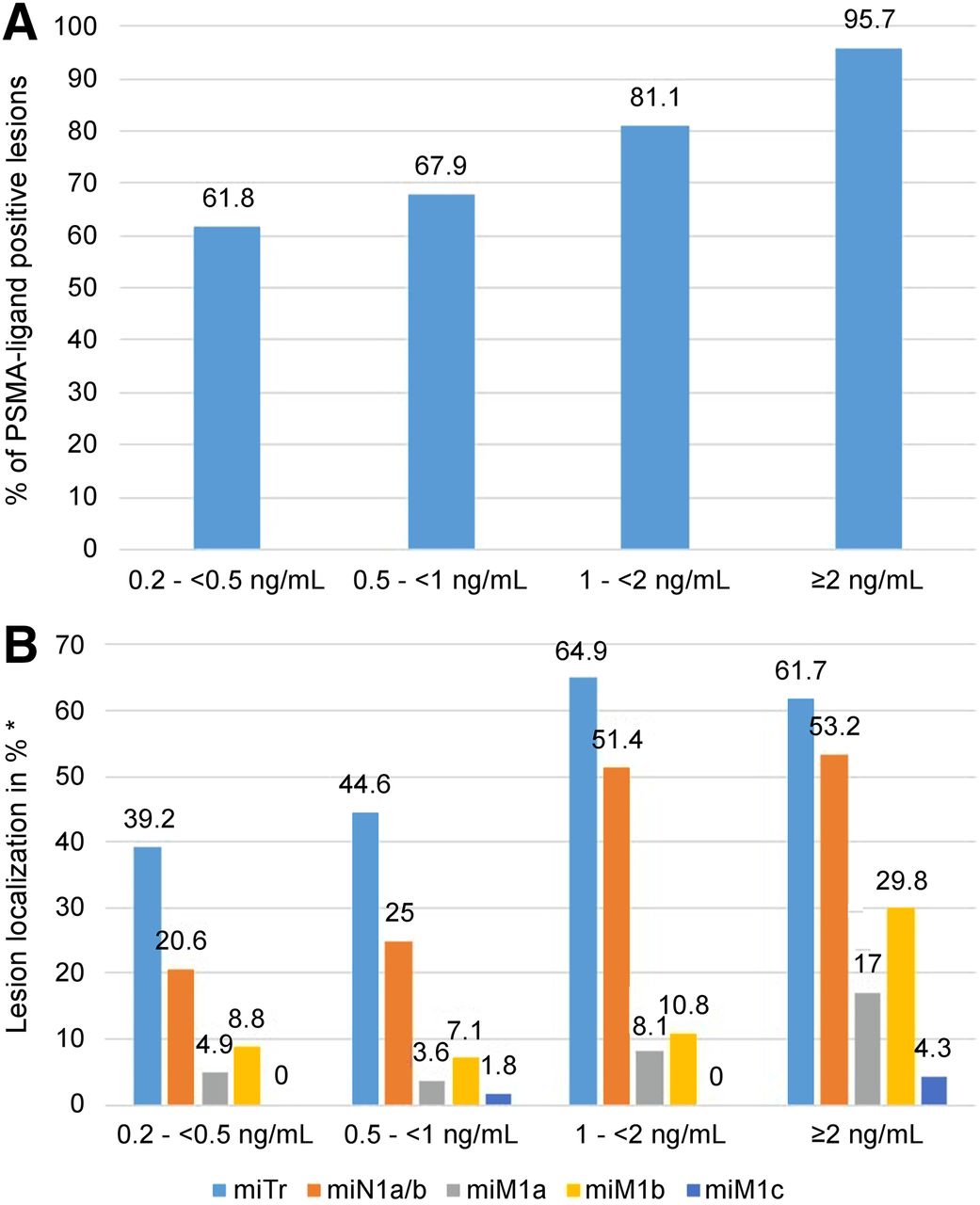
Of the 242 patients, 176 (72.7%) showed one or more localized areas suggestive of recurrent prostate cancer on 18F‐rhPSMA‐7.3 PET. The detection efficacy of 18F‐rhPSMA‐7.3 PET/CT positively correlated with PSA levels. It was 61.8% (63/102; 95% CI, 0.52–0.71), 67.9% (38/56; 95% CI, 0.55– 0.79), 81.1% (30/37; 95% CI, 0.66–0.91), and 95.7% (45/47; 95% CI, 0.86–0.99) for PSA levels of 0.2 to less than 0.5 ng/mL, 0.5 to less than 1 ng/mL, 1 to less than 2 ng/mL, and at least 2 ng/mL, respectively (Fig. 1A). The mean PSA level was significantly (P < 0.0001) lower among patients with negative findings on 18F‐rhPSMA‐7.3 PET/CT (0.61 ± 0.68 ng/mL) than among 18F‐rhPSMA‐7.3–positive patients (2.77 ± 6.88 ng/mL).

Overall detection rate of 18F‐rhPSMA‐7.3 PET stratified by PSA value (A) and lesion localization using miTNM classification stratified by PSA value (B). miTr = presence of local recurrence after radical prostatectomy; miN1a/b = single or multiple positive regional lymph nodes; miM1a = extrapelvic lymph nodes; miM1b = bone metastases; miM1c = other distant metastases. *Multiple metastatic regions within 1 patient possible.
Lesion Location
Lesion localization on 18F-rhPSMA-7.3 PET/CT based on the miTNM classification system is shown in Figure 1B. Local recurrence in the prostate bed was 39.2% at a PSA of 0.2 to less than 0.5 ng/mL and 61.7% at a PSA of at least 2 ng/mL, whereas pelvic lymph node metastases were present in 20.6% at a PSA of 0.2 to less than 0.5 ng/mL and increased to 53.2% at a PSA of at least 2 ng/mL. Although extrapelvic lymph node metastases were rare (<5%) at a PSA of 0.2 to less than 0.5 ng/mL, 17% of patients with a PSA of at least 2 ng/mL presented with positive retroperitoneal or supradiaphragmatic lymph nodes. 18F‐rhPSMA‐7.3–avid bone metastases were even present in 8.8% of patients who had early biochemically recurrent disease with a PSA of 0.2 to less than 0.5 ng/mL, increasing to 29.8% in patients with a PSA of at least 2 ng/mL. Visceral metastases were absent or low at all PSA levels, as only 4.3% of patients with a PSA of at least 2 ng/mL showed visceral metastases. Further, the number of regions involved broadly increased with increasing PSA level, with more than 1 region being involved in nearly half of the patients (44.4%) with a PSA of at least 2 ng/mL, compared with only 16% of patients with a PSA of 0.2 to less than 0.5 ng/mL.
Impact on Patient Management
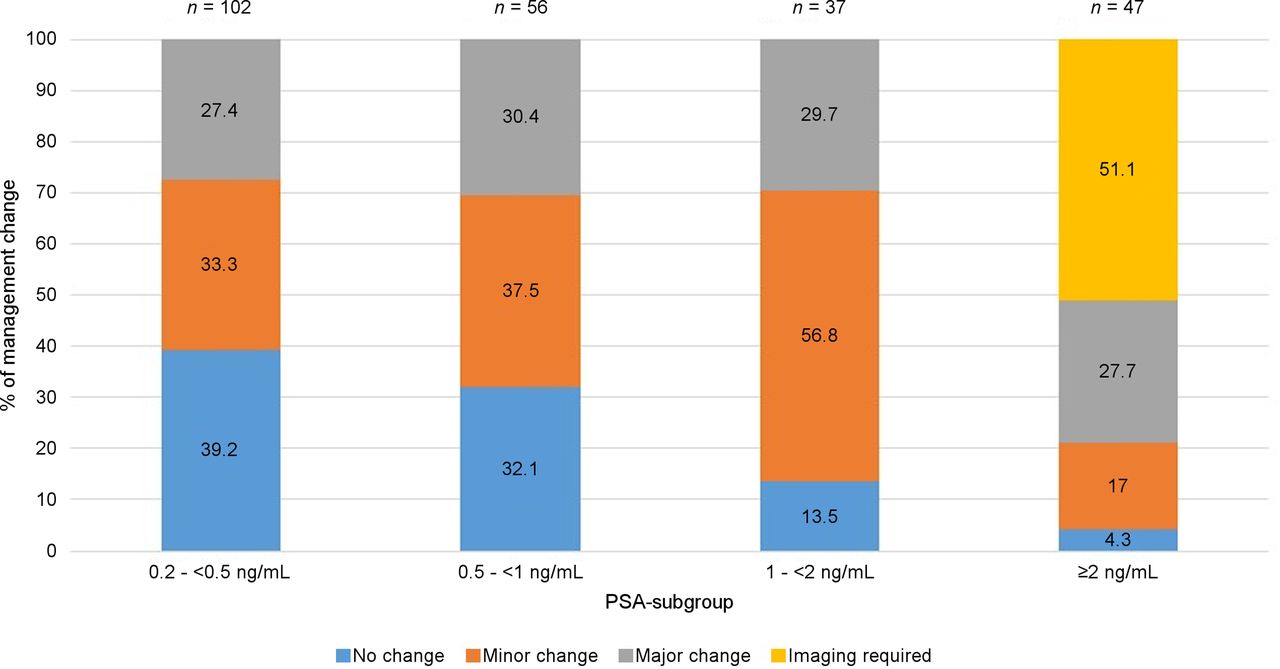
Compared with the initial plan, therapeutic management was changed by the tumor board for 153 of 242 patients (63.2%) after results from 18F-rhPSMA-7.3 PET/CT were presented. In detail, the potential management change was considered major in 22.3% (n = 54) and minor in 40.9% (n = 99). No change in therapeutic management was stated in 26.4% (n = 64) after 18F-rhPSMA-7.3 PET/CT. In 10.3% (n = 25) of patients, no baseline management plan could be assessed. All 25 of these patients presented with a PSA of at least 3 ng/mL at the time of 18F‐rhPSMA‐7.3 PET/CT, and tumor board members decided that no potential management could be defined because additional imaging is recommended before treatment planning. Figure 2 visualizes the potential management before and after 18F-rhPSMA-7.3 PET/CT. Potential management changes after 18F-rhPSMA-7.3 PET/CT stratified by PSA value can be seen in Figure 3. Here, the number of patients with a potential management change after 18F-rhPSMA-7.3 PET/CT was already high (60.7%) in the patient subgroup with a PSA of 0.2 to less than 0.5 ng/mL and consistently increased to 67.9% and 86.5% in patients with a PSA of 0.5 to less than 1 ng/mL and a PSA of at least 2 ng/mL, respectively.
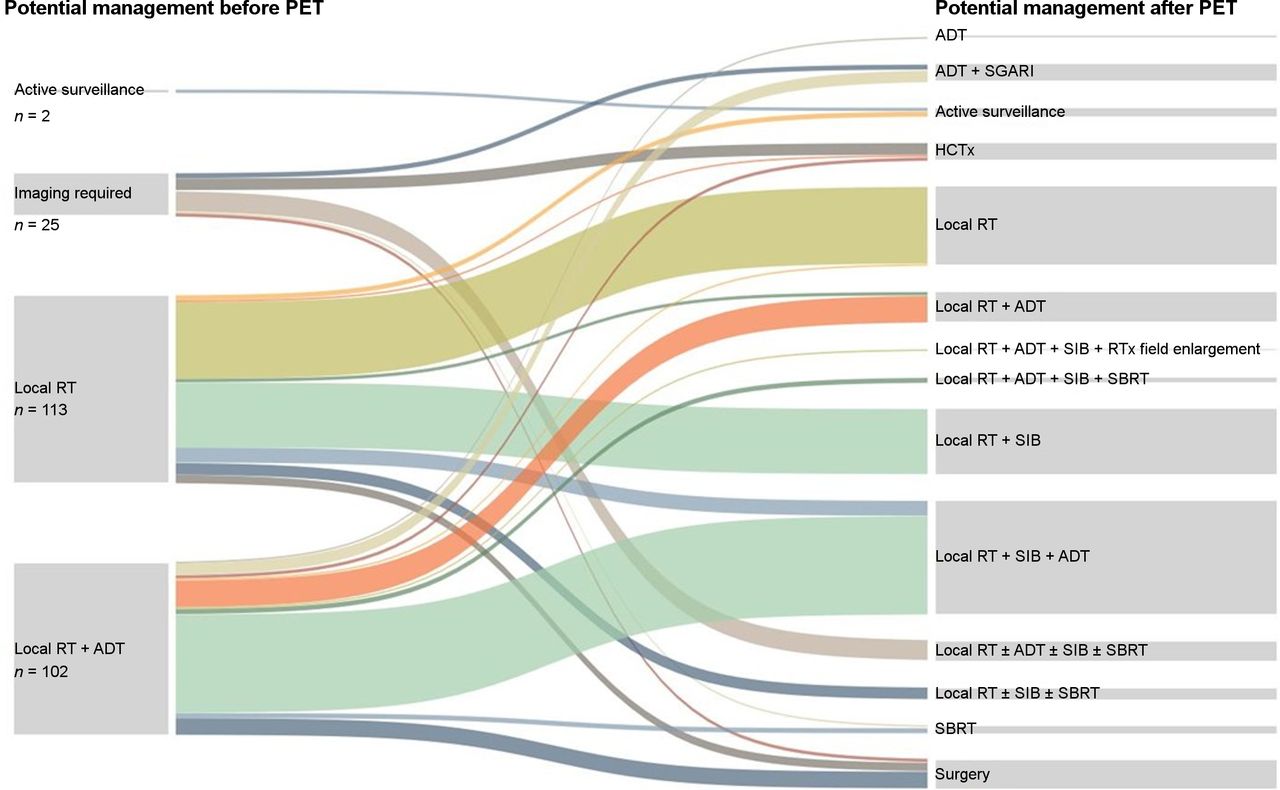
Sankey diagram for pre- to post-PET change in potential management (n = 242). HCTx = hormone chemotherapy; RT = radiation therapy; SBRT = stereotactic body radiotherapy; SGARI = second-generation androgen receptor inhibitor; SIB = simultaneous integrated boost.
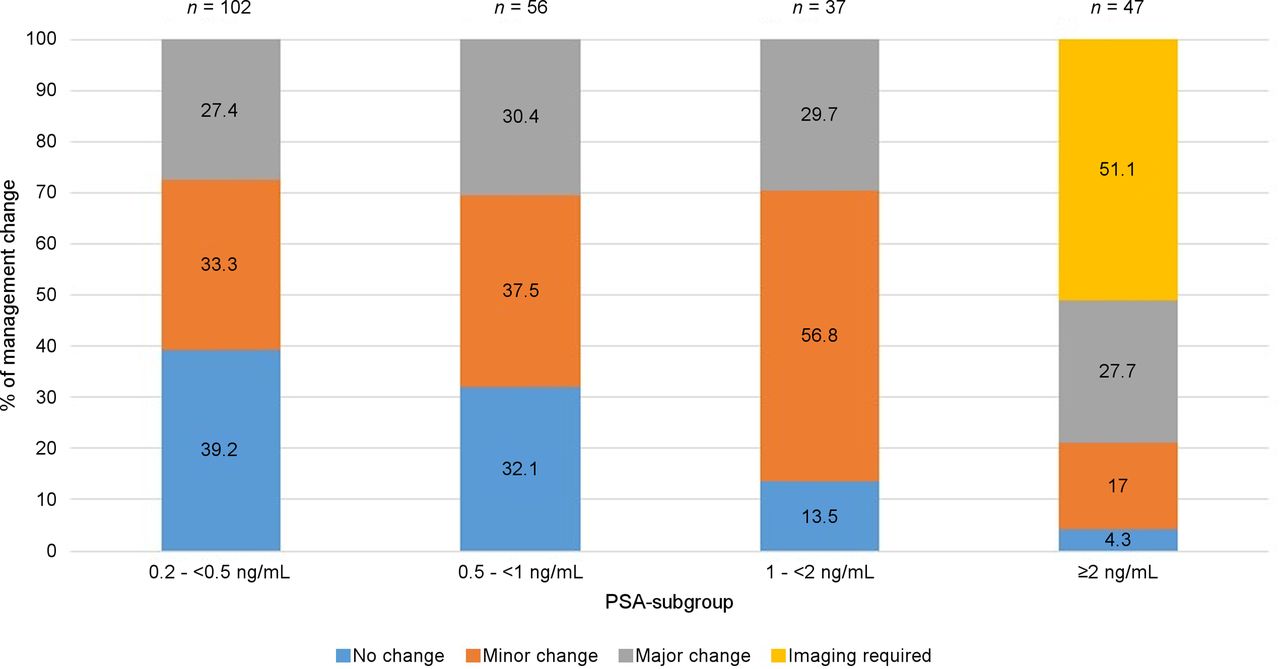
Potential management change after PSMA PET stratified by PSA value. In patients with no assessment feasible, tumor board members suggested additional imaging before management decision.
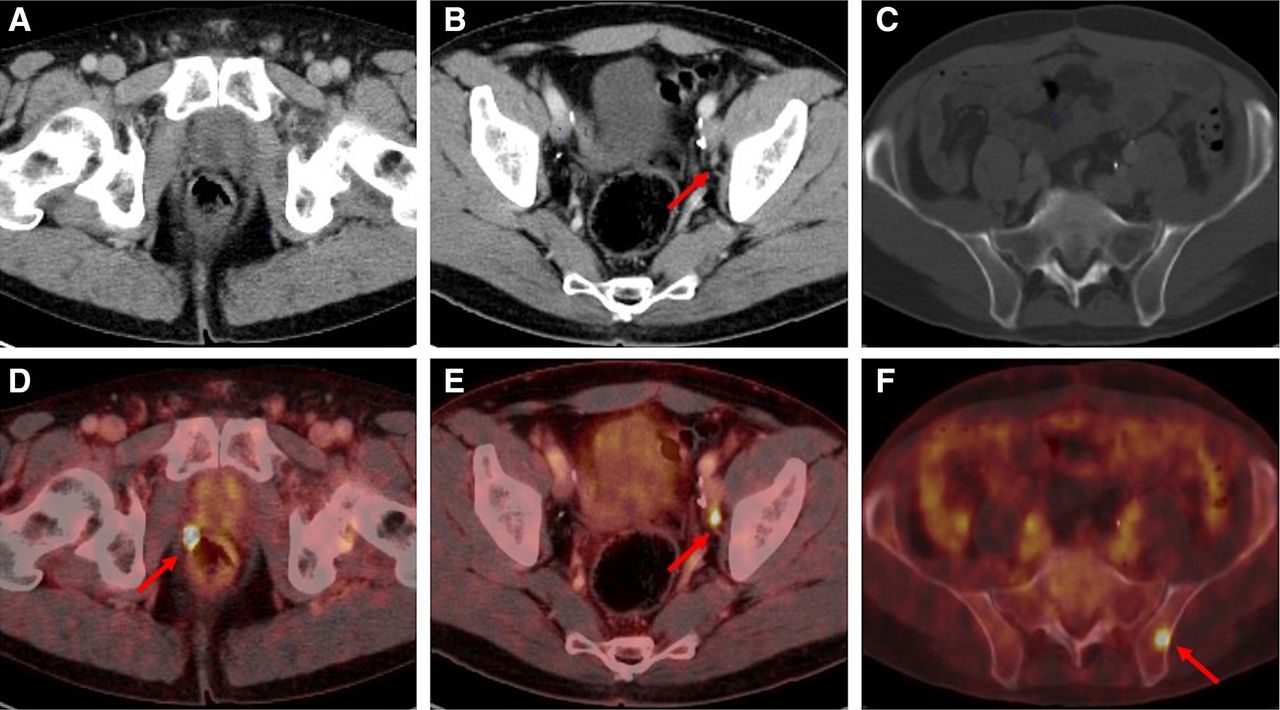
Management changes according to lesion localization are presented in Table 3. The presence of a local recurrence resulted in only a minor change in management in a majority of patients (67.8%; 80/118), whereas the presence of pelvic lymph node metastases and either extrapelvic lymph node, bone, or visceral metastases induced a major change in treatment in 67.1% (47/70) and 66.7% (36/54) of patients, respectively. Figure 4 presents patient examples with minor and major therapeutic changes in management.
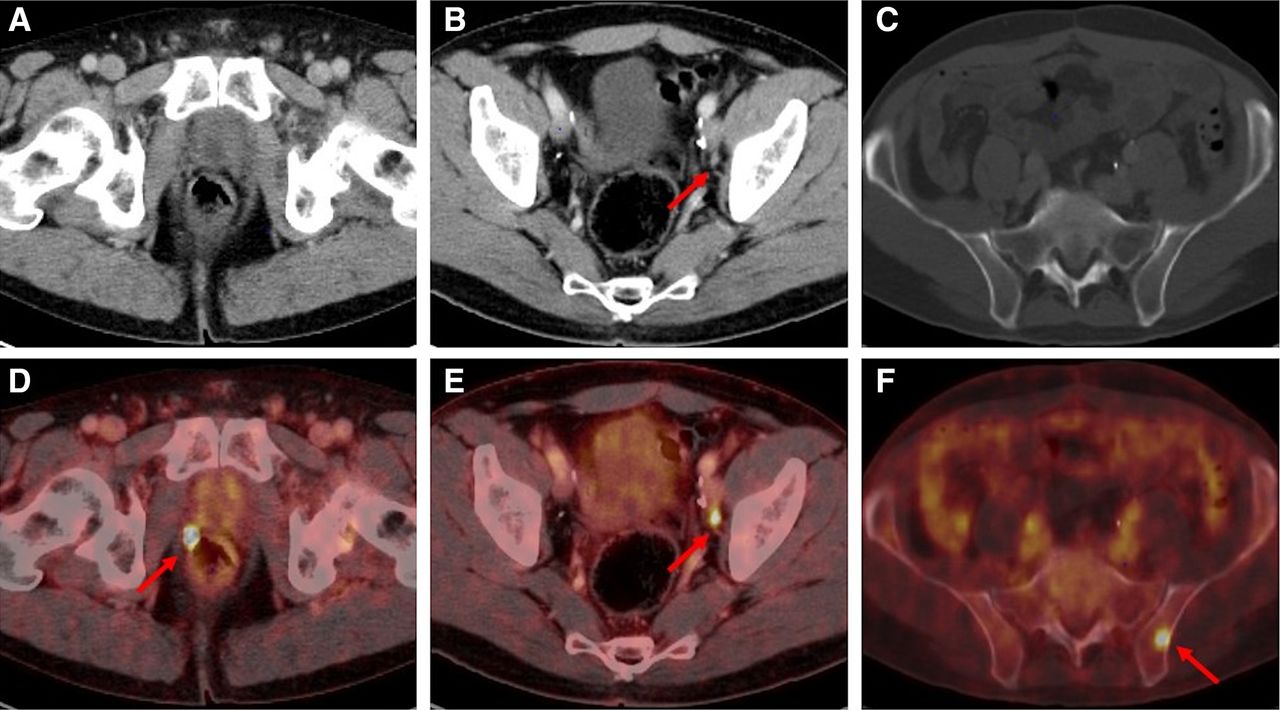
Examples of individual minor and major therapeutic change in patients with biochemical recurrence after radical prostatectomy undergoing 18F‐rhPSMA‐7.3 PET/CT. (A and D) A 70-y-old patient (PSA level at time of PET, 0.49 ng/mL) with 18F‐rhPSMA‐7.3-ligand uptake in right prostatic bed (D, red arrow) without clear morphologic correlate on corresponding CT. Therapeutic management was changed from radiation therapy of prostatic bed to radiation therapy of prostatic bed with simultaneous integrated boost and was considered minor change. (B and E) A 57-y-old patient presenting with biochemical recurrence (PSA level, 1.0 ng/mL) 7 y after radical prostatectomy (T2c; N0; grade group, 8; initial PSA, 4.5 ng/mL). 18F‐rhPSMA‐7.3 PET/CT shows focal PSMA-ligand uptake in unsuggestive lymph node (axial diameter, 5 mm) adjacent to left external iliac artery suspected of being single lymph node metastasis. Therapeutic management was changed from radiation therapy of prostatic bed and additional short-term ADT to salvage lymphadenectomy (major change) as individual treatment concept. (C and F) A 62-y-old patient presenting with biochemical recurrence (PSA level, 0.3 ng/mL) 1.5 y after radical prostatectomy (T3a; N0; grade group, 9; initial PSA, 7.0 ng/mL). 18F‐rhPSMA‐7.3-PET/CT shows focal PSMA-ligand uptake in left iliac bone without unequivocal morphologic correlate. Therapeutic management was considered major change (change from ADT to stereotactic body radiation therapy of single bone metastasis).
Potential Management Change According to Lesion Localization
DISCUSSION
In this retrospective analysis investigating a large cohort of patients with biochemical recurrence of prostate cancer after prostatectomy and before potential salvage therapy, 18F‐rhPSMA‐7.3 PET/CT detected and localized prostate cancer highly effectively in 72.3% of patients. Consistent with other PET tracers, the detection rate of 18F‐rhPSMA‐7.3 increased with PSA level (61.8% in patients with a PSA of 0.2 to less than 0.5 ng/mL, rising to 95.7% in patients with a PSA of at least 2 ng/mL) (22,23,25). Of note, the detection rate in this study was lower than in our previously published data on the diastereomeric mixture of 18F‐rhPSMA‐7 in biochemically recurrent prostate cancer after radical prostatectomy (62%, 68%, 81%, and 96% for 18F‐rhPSMA‐7.3 vs. 71%, 86%, 86%, and 95% for 18F‐rhPSMA‐7 at PSA levels of 0.2–<0.5 ng/mL, 0.5–<1 ng/mL, 1–<2 ng/mL, and ≥2 ng/mL, respectively) (22). This difference is most likely explained by inclusion, in this study, of only patients without prior salvage therapy or ADT, compared with—in the previous study using 18F-rhPSMA-7—26% and 40% of patients, respectively, who have been on ADT in the 6 mo preceding the PET or had external radiation after radical prostatectomy. The latter cohort can be regarded as slightly more advanced in the course of biochemical recurrence, potentially leading to higher detection rates. Therefore, direct comparison between these datasets is not feasible. Nevertheless, on the basis of data from both retrospective analyses, the high detection rates of 18F‐rhPSMA‐7 and -7.3 are very likely similar.
Recent data suggest that 18F‐labeled PSMA ligands with low urinary excretion (e.g., 18F-PSMA-1007 and 18F-rhPSMA-7.3) can achieve higher detection rates than reported for 68Ga‐labeled PSMA ligands. Our data provide further evidence for this hypothesis, in particular given the results for patients with PSA levels of less than 0.5 ng/mL. In our study, the detection rate for local recurrence was 39% for 18F‐rhPSMA‐7.3, in comparison to only 20% reported in a recently published study of 272 patients undergoing 68Ga‐PSMA‐11 imaging (34).
Accurate localization of disease is crucial in the management of patients with biochemical recurrence of prostate cancer, as focal salvage therapies need accurate target delineation. On the other hand, the presence of distant metastases may trigger additional or alternative systemic therapy (10). Therefore, the updated European Association of Urology guidelines recommend PSMA PET, if available, in patients experiencing biochemical recurrence after radical prostatectomy when the results might influence subsequent treatment decisions (10). The results of our study demonstrate that after 18F-rhPSMA-7.3 PET/CT, potential therapeutic management was changed in 153 of 242 patients (63.2%) compared with an initial treatment strategy based on clinical characteristics. This result is in line with a recently published prospective study by Fendler et al., with a change in intended management in more than two thirds of patients undergoing 68Ga-PSMA-11 PET for localization of biochemically recurrent prostate cancer (17). Several other studies have demonstrated the potential of 68Ga‐PSMA‐11 to influence the future management of these patients, with the detection of lymph nodes and distant metastases having the highest impact on patient management (16,35,36). Similarly, in our study, the presence of either pelvic or extrapelvic lymph node metastases, bone metastases, or visceral metastases on 18F-rhPSMA-7.3 PET resulted in a major treatment change in about two thirds of the patients. In contrast, minor management changes were observed predominantly in patients with local recurrence and in a few patients with pelvic lymph node metastases. The high number of potential management changes derived from our tumor board provides further data—in this case, based on the application of 18F-rhPSMA-7.3 PET/CT—outlining the high value of PSMA-ligand PET imaging in early biochemical recurrence of prostate cancer.
After evaluation of tumor extent and localization with 18F‐rhPSMA‐7.3 PET/CT, modern local therapies with either local salvage surgery or local stereotactic body radiotherapy according to our tumor board was possible in 17 (7%) and 15 (6%) patients, respectively, whereas in 3 patients active surveillance was possible instead of local radiation therapy. This result is in line with a metaanalysis of Han et al. including 15 studies with 1,163 patients showing that imaging with PSMA-ligand PET has shifted the percentage of patients receiving systemic treatment in favor of local treatment (16).
There are several limitations to our study. First, intended management before and after 18F-rhPSMA-7.3 PET/CT was assessed hypothetically, as part of a tumor board, and no information on actual implemented management changes was available because of the retrospective character of this analysis, which included patients from different external and internal referrers for whom treatment approaches might differ. Thus, more prospective evaluations are still needed to prove the overall benefit of these management changes in patients.
Second, a rigorous validation of PSMA-ligand–positive lesions by histopathology or immunohistopathology was not performed, although the very high positive predictive value for PSMA-ligand PET, considering known limitations or pitfalls, has been shown in several studies (37–39). Only a subset of 17 patients underwent salvage PSMA-radioguided surgery, and in the region of all 18F-rhPSMA-7.3 PET–positive lesions, lymph node metastases or local recurrences were confirmed histopathologically. Further, concise follow-up imaging was not available for lesion validation in most patients. However, in the case of PSMA-ligand uptake in the bone with no clear correlate on either CT or, more importantly, MRI, it has to be assumed that the uptake is not related to prostate cancer, because MRI is currently regarded as the gold standard for the detection of bone metastases. However, lesion characterization also depends on the number of lesions and the clinical context, as a single PSMA-ligand–positive bone lesion (especially in the ribs) without any morphologic correlate in a patient presenting with a very early biochemical recurrence would most likely be considered unspecific benign PSMA-ligand uptake, whereas the presence of multiple PSMA-ligand–positive bone lesions in the context of a clearly increased PSA level would rather be interpreted as malignant, resulting in a potential major change in management.
Third, the results of conventional imaging modalities (e.g., CT or bone scanning) were not incorporated into the intended management before 18F-rhPSMA-7.3 PET because availability was limited and inhomogeneous. Nevertheless, it is appropriate to perform a tumor board review acknowledging the clinical characteristics of the patient because conventional (non–PSMA PET) imaging lacks the potential to effectively detect early biochemical recurrence (3).
Further, clinical information on PSA nadir and number of resected lymph nodes at primary lymphadenectomy was available for only a minority of patients. Thus, it remains unknown whether all patients achieved an undetectable PSA nadir after radical prostatectomy, potentially influencing intended management before 18F-rhPSMA-7.3 PET. Further, an extended pelvic lymph node dissection during primary surgery was not performed on all patients, potentially influencing intended management before 18F-rhPSMA-7.3 PET (e.g., toward a more extended radiation therapy of the lymphatic drainage).
CONCLUSION
In this large population of patients with recurrent prostate cancer after radical prostatectomy and before any potential salvage therapy, 18F‐rhPSMA‐7.3 PET/CT offered high detection rates at least equal to those reported for 68Ga‐PSMA‐11. Incorporation of the 18F‐rhPSMA‐7.3 PET/CT results into simulated clinical decision making led to a change in management in nearly two thirds of the patients, potentially paving the way to personalized medicine.
DISCLOSURE
Matthias Eiber holds patent rights on rhPSMA. Matthias Eiber and Wolfgang Weber are consultants for Blue Earth Diagnostics (licensee for rhPSMA). No other potential conflict of interest relevant to this article was reported.
KEY POINTS
QUESTION: What is the detection efficacy and the potential impact on therapeutic management of novel 18F-rhPSMA-7.3 isomer PET in patients with biochemically recurrent prostate cancer after radical prostatectomy prior salvage therapy?
PERTINENT FINDINGS: 18F-rhPSMA-7.3 PET/CT offers high detection efficacy in biochemically recurrent prostate cancer, at least equal to data published for 68Ga-PSMA11, and resulted in potential therapeutic management change in a substantial number of patients.
IMPLICATIONS FOR PATIENT CARE: 18F-rhPSMA-7.3 is a novel and effective PET agent for imaging of recurrent prostate cancer, resulting in a potential management change in approximately two thirds of the patients.
Footnotes
Published online March 12, 2021.
- © 2021 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication November 18, 2020.
- Revision received March 2, 2021.
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Diuresis During 18F-Flotufolastat (rhPSMA-7.3) PET/CT Improves Recurrence Detection After Prostatectomy: A Prospective Phase II Trial
- An Intrapatient Dosimetry Comparison of 177Lu-rhPSMA-10.1 and 177Lu-PSMA-I&T in Patients with Metastatic Castration-Resistant Prostate Cancer
- Validation of 18F-rhPSMA-7 and 18F-rhPSMA-7.3 PET Imaging Results with Histopathology from Salvage Surgery in Patients with Biochemical Recurrence of Prostate Cancer
- Utility of 18F-rhPSMA-7.3 PET for Imaging of Primary Prostate Cancer and Preoperative Efficacy in N-Staging of Unfavorable Intermediate- to Very High-Risk Patients Validated by Histopathology
- Predictors of 18F-DCFPyL PET/CT Positivity in Patients with Biochemical Recurrence of Prostate Cancer After Local Therapy