


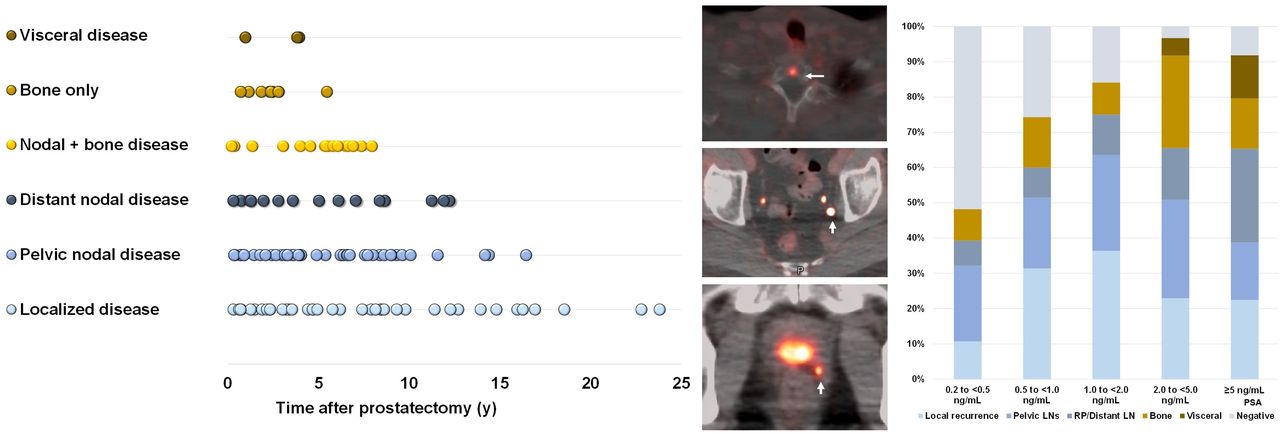
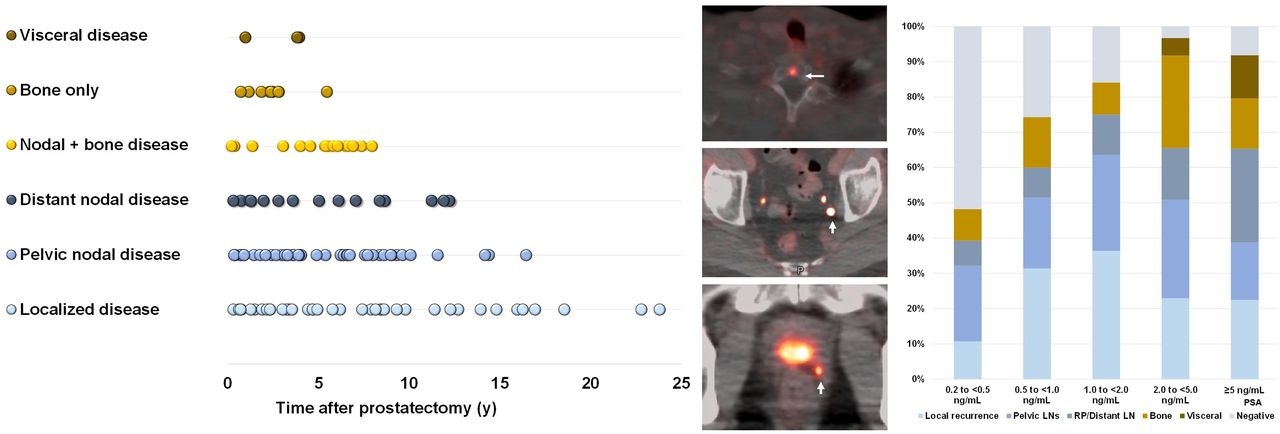
Visual Abstract
Abstract
Our objective was to investigate the factors predicting scan positivity and disease location in patients with biochemical recurrence (BCR) of prostate cancer (PCa) after primary local therapy using prostate-specific membrane antigen–targeted 18F-DCFPyL PET/CT. Methods: This was a 2-institution study including 245 BCR PCa patients after primary local therapy and negative results on conventional imaging. The patients underwent 18F-DCFPyL PET/CT. We tested for correlations of lesion detection rate and disease location with tumor characteristics, time from initial therapy, prostate-specific antigen (PSA) level, and PSA doubling time (PSAdt). Multivariate logistic regression analyses were used to determine predictors of a positive scan. Regression-based coefficients were used to develop nomograms predicting scan positivity and extrapelvic disease. Results: Overall, 79.2% (194/245) of patients had a positive 18F-DCFPyL PET/CT result, with detection rates of 48.2% (27/56), 74.3% (26/35), 84% (37/44), 96.7% (59/61), and 91.8% (45/49) for PSAs of <0.5, 0.5 to <1.0, 1.0 to <2.0, 2.0 to <5.0, and ≥5.0 ng/mL, respectively. Patients with lesions confined to the pelvis had lower PSAs than those with distant sites (1.6 ± 3.5 vs. 3.0 ± 6.3 ng/mL, P < 0.001). In patients treated with prostatectomy (n = 195), 24.1% (47/195) had a negative scan result, 46.1% (90/195) showed intrapelvic disease, and 29.7% (58/195) showed extrapelvic disease. In the postradiation subgroup (n = 50), 18F-DCFPyL PET/CT was always negative at a PSA lower than 1.0 ng/mL and extrapelvic disease was seen only when PSA was greater than 2.0 ng/mL. At multivariate analysis, PSA and PSAdt were independent predictive factors of scan positivity and the presence of extrapelvic disease in postsurgical patients, with area under the curve of 78% and 76%, respectively. PSA and PSAdt were independent predictors of the presence of extrapelvic disease in the postradiation cohort, with area under the curve of 85%. Time from treatment to scan was significantly longer for prostatectomy-bed–only recurrences than for those with bone or visceral disease (6.2 ± 6.4 vs. 2.4 ± 1.3 y, P < 0.001). Conclusion: 18F-DCFPyL PET/CT offers high detection rates in BCR PCa patients. PSA and PSAdt are able to predict scan positivity and disease location. Furthermore, the presence of bone or visceral lesions is associated with shorter intervals from treatment than are prostate-bed–only recurrences. These tools might guide clinicians to select the most suitable candidates for 18F-DCFPyL PET/CT imaging.
Patients with localized prostate cancer (PCa) are usually treated with either radical prostatectomy, some variation of external-beam radiation, brachytherapy, or active surveillance (1,2). Despite definitive therapy with either surgery or radiation, approximately 20%–40% of cases will recur within 10 y of the initial treatment (3). Biochemical recurrence (BCR) occurs when prostate-specific antigen (PSA) increases during posttreatment monitoring, often without positive findings on conventional imaging, and can be seen months or years after the initial local therapy (4).
In the setting of BCR, understanding the specific sites of relapse and the patterns of recurrence improves understanding of the disease process. Local recurrence alone is usually associated with a better prognosis and slower disease kinetics, whereas nodal, bone, or visceral metastases imply a more aggressive phenotype that carries a worse prognosis. Defining the extent of disease spread with imaging can be crucial for therapeutic decision making and mapping potential treatment fields in PCa patients. The lack of sensitivity of conventional imaging (5) has limited the understanding of disease spread in BCR. With the advent of positron-emitting (PET) probes targeting prostate-specific membrane antigen (PSMA), molecular imaging has yielded new insights into PCa recurrence (6), with improved sensitivity and specificity that far exceed conventional imaging and earlier types of PET agents (7). 18F-DCFPyL is a recent U.S. Food and Drug Administration–approved PSMA PET agent with high affinity for PCa (8,9).
Men with recurrent disease are a highly heterogeneous population, carrying different profiles of disease aggressiveness; therefore, selecting the most suitable candidates for imaging with 18F-DCFPyL PET/CT might be critical to optimize its use and to spare lower-risk patients from potentially unnecessary staging procedures. We report the results of 18F-DCFPyL PET/CT in a cohort of 245 BCR PCa patients from 2 institutions. We hypothesized that patients’ clinical features, including time from initial treatment, PSA level, and PSA doubling time (PSAdt), might predict the location and extent of disease. We also sought to develop clinical nomograms to assess the likelihood of each patient to have a positive scan and extrapelvic disease, using Gleason score, PSA, and PSAdt as predictive variables, in different settings based on primary initial therapy.
MATERIALS AND METHODS
Patient Population and Study Design
This study included 2 institutional trials compliant with the Health Insurance Portability and Accountability Act. Institutional review boards approved the studies, and all subjects gave written informed consent. We included 245 patients who met the eligibility criteria for protocols NCT03181867 and NCT02825875 (ClinicalTrials.gov): 147 from the National Cancer Institute and 98 from Johns Hopkins Hospital. A cohort of 90 of these patients was previously published (10). Patients had BCR, defined as a PSA of more than 0.2 ng/mL for those who underwent radical prostatectomy or at least 2 ng/mL greater than nadir after radiation (American Society for Radiation Oncology–Phoenix criteria) or considered clinical failure (11). Patients had negative conventional-imaging results (CT and bone scans). Exclusion criteria included current androgen deprivation therapy at enrollment; inability to tolerate PET/CT, and a creatinine level at least 2 times the normal upper limit. Patients were classified by prior initial treatment (prostatectomy vs. radiation). Time from treatment to scan, Gleason score, PSA level, and PSAdt were recorded.
18F-DCFPyL PET/CT Protocol
18F-DCFPyL PET/CT was performed at 2 h after injection using a GE Healthcare Discovery MI DR time-of-flight camera (National Cancer Institute) and at 1 h using a GE Healthcare Discovery RX or a Siemens Biograph mCT time-of-flight camera (Johns Hopkins Hospital). Scanners used low-dose CT (120 kV, 60 mAs). Images were reconstructed with manufacturer-supplied maximum-likelihood or ordered-subsets expectation maximization algorithms.
18F-DCFPyL was synthesized under good-manufacturing-practice conditions, as previously described (8). Patients received an intravenous injection of 18F-DCFPyL (mean injected activity, 296 ± 33.3 MBq [8.0 ± 0.9 mCi]; range, 207.2–325.6 MBq [5.6–8.8 mCi]), followed by whole-body PET/CT at 1–2 h after injection (3 min/bed). Furosemide was not given. Patients were monitored for adverse events during injection, after scanning, and the next day via telephone query.
Imaging Interpretation
Two board-certified nuclear medicine physicians in each institution independently reviewed the images, resolving disagreements by consensus. 18F-DCFPyL PET/CT images were reviewed using MIM (version 6.9.2, MIM Software Inc.) or SyngoVia-20 (Siemens Healthineers). Maximum-intensity-projection, axial, coronal, and sagittal PET/CT images were reviewed. Only clear foci of abnormal uptake above the surrounding background (12), not associated with physiologic uptake or known pitfalls (13), were considered positive. Foci with subtle or very mild uptake not definitive for disease were called indeterminate and considered negative to avoid confusing results. PET-positive lesions in the prostatectomy region/prostate, pelvic/extrapelvic nodes, or organ/bone were classified as recurrence.
Statistical Methods
18F-DCFPyL PET lesion detection rates were analyzed as a function of PSA. Scan positivity was evaluated by stratifying PSA at ranges of <0.5, 0.5 to <1.0, 1.0 to <2.0, 2.0 to <5.0, and ≥5.0 ng/mL. Sites of recurrence by 18F-DCFPyL PET were tested for correlation with PSA, PSAdt, and time from local treatment, using Wilcoxon rank tests. Subgroup analysis was conducted by treatment type (prostatectomy vs. radiation). Patients were categorized as having a Gleason of less than 7 versus 7 or more and as having oligometastases (1–5 lesions) versus multiple metastases (>5 lesions). Descriptive values were expressed as mean ± SD.
The proportional-odds model was used to associate clinical factors with scan results, classifying scans as negative, positive with intrapelvic disease, or positive with extrapelvic disease. Clinical factors included Gleason score, PSA, PSAdt, years since treatment, and treatment type (surgery vs. radiation). Analyses were exploratory; thus, adjustment for multiple comparisons were not implemented. A variable-selection procedure based on the Akaike information criterion was used to determine the best fitted model. Model fit was examined by a calibration plot of the predicted versus observed probability of a positive scan and the presence of extrapelvic disease, calculating observations in each decile of predicted probability. The diagnostic accuracy of the predicted model was measured by area under the curve. Nomograms were generated using the R-package rms (14). All tests were 2-sided, and P values of less than 0.01 were considered significant. Statistical analyses were performed using R, version 3.5.0.
RESULTS
Patient Population
In total, 245 patients (mean age, 66 y; range, 48–85 y) underwent 18F-DCFPyL PET/CT. Median PSA was 1.6 ng/mL (range, 0.2–35.5 ng/mL). Prior primary local therapy consisted of radical prostatectomy (n = 195) or radiation with or without androgen deprivation therapy (n = 50). Patients were not actively receiving androgen deprivation therapy at imaging. The mean time from prostatectomy to scan was 6.1 ± 5.1 y (range, 1.5 mo–23.8 y), and the mean time from radiation was 4.9 ± 3.6 y (range, 9 mo–14.9 y). No adverse events were seen after 18F-DCFPyL injection. Table 1 shows the patient characteristics.
Patient Characteristics
18F-DCFPyL PET/CT Versus PSA
Overall, the patient-based lesion detection rate for 18F-DCFPyL PET/CT was 79.2% (194/245), which increased as PSA increased: 48.2% (27/56), 74.3% (26/35), 84% (37/44), 96.7% (59/61), and 91.8% (45/49) at PSA < 0.5, 0.5 to <1.0, 1.0 to <2.0, 2.0 to <5.0, and ≥5.0 ng/mL, respectively (Fig. 1). Detailed analysis by cohort and institution is reported at Supplemental Tables 1–3 (supplemental materials are available at http://jnm.snmjournals.org). No differences were seen in lesion detection between institutions. Of 51 cases with negative scan results, 13 showed indeterminate findings, with 17 indeterminate foci.

18F-DCFPyL PET overall, intrapelvic, and extrapelvic detection rates by PSA.
Patients with positive pelvic findings had a significantly lower PSA than those with positive extrapelvic lesions (i.e., retroperitoneal, distant nodes, or bone or visceral sites) (2.8 ± 3.5 vs. 5.0 ± 6.3 ng/mL, P < 0.001), suggesting that pelvic nodes may precede extrapelvic adenopathy. At a PSA of less than 2.0 ng/mL, 18F-DCFPyL PET/CT detected a higher proportion of patients with localized pelvic disease, whereas the proportion of patients with extrapelvic lesions was higher than that with intrapelvic lesions for a PSA of more than 5 ng/mL (Fig. 2).

18F-DCFPyL–positive sites by location and PSA. RP = radical prostatectomy.
Impact of Time from Local Treatment
The time from prior therapy (prostatectomy vs. radiation) and disease location were evaluated. In the prostatectomy cohort (n = 195), time from treatment to scan was longer for men with findings at the prostatectomy bed only than for those with only bone or visceral lesions or for those with nodal lesions (7.4 ± 6.3 vs. 2.3 ± 1.3 vs. 3.1 ± 4.1 y, P < 0.001). When findings were confined to the prostatectomy bed, 53.8% of patients were treated less than 8 y before the scan, and 46.1% had prostatectomies performed more than 8 y before the scan. For patients with extraprostatic extension, 75.5% were treated less than 8 y before the scan, and 24.5% were treated more than 8 y before the scan. Thus, 18F-DCFPyL PET/CT–positive nodal findings, bone-plus-nodal disease, bone-only disease, or visceral lesions were seen mostly when initial treatment was less than 8 y beforehand in 79.7%, 88.9%, 100.0%, and 100.0% of cases, respectively (Fig. 3A). The same patterns of disease distribution versus time from initial therapy were seen in a separate analysis by institution. Figure 4 and Supplemental Figure 1 show disease patterns versus time from prostatectomy by PSA and PSAdt. There were no differences in the distribution of times from prostatectomy between patients with oligometastases and those with multiple disease (4.8 ± 3.8 vs. 5.3 ± 5.7 y, P = 0.054).

Disease location vs. time from prostatectomy (A) and radiation (B).

Patterns of recurrence vs. time from therapy and PSAdt in postprostatectomy (A and B) and postradiation patients (C and D).
In the postradiation cohort (n = 50), men with prostate involvement showed significantly longer times from radiation than subjects with bone or visceral lesions (6.7 ± 4.1 vs. 2.6 ± 2.8 y) (Fig. 3B). Significantly longer times from radiation were seen in men with pelvic findings only than in men with extrapelvic lesions, with median times of 6.4 ± 3.7 versus 2.9 ± 2.8 y. When recurrence was exclusively within the prostate, 38.9% of patients were initially treated more than 8 y before the scan, and 61.1% had radiation less than 8 y before the scan. For positive extraprostatic extension, most patients (93.3%) were treated less than 8 y beforehand. No differences were seen in times from radiation between patients with oligometastases and patients with multiple lesions (3.6 ± 3.1 vs. 2.9 ± 2.6 y, P = 0.66).
Impact of Clinical Features on Scan Positivity
In the cohort treated with radical prostatectomy (n = 195), 75.9% (148/195) showed at least 1 positive lesion (Fig. 5). Lesions confined to the pelvis were seen in 46.2% (90/195) of patients, especially driven by local recurrence at the prostatectomy bed in 44.5% and pelvic nodes in 55.5%, whereas extrapelvic lesions were seen in 29.7% (58/195) of cases, often at a PSA of more than 5.0 ng/mL. PSAdt was significantly longer for patients with disease confined to the pelvis than for those with distant extrapelvic lesions (7.1 ± 8.6 vs. 5.7 ± 2.7 mo, P < 0.001).

A 70-y-old patient with BCR PCa after radiation and 2 y of androgen deprivation therapy (primary tumor, T4N1; Gleason 4 + 5; time from treatment, 2.5 y; prescan PSA, 2.41 ng/mL; PSAdt, 4.7 mo). 18F-DCFPyL PET/CT images including a maximal-intensity projection and axial fused PET/CT images show subcentimeter pelvic nodes (arrow in left iliac nodes) as well as foci at T9 (arrow) and anterior iliac bone (arrow). Follow-up biopsy confirmed bone metastasis at iliac bone.
In patients who received radiation (n = 50), only 8% (4/50) had a negative scan result, 48% showed intrapelvic disease (75% within the prostate and 25% in pelvic nodes), and 44% had extrapelvic findings (Fig. 6), and only when PSA was more than 2.0 ng/mL. Similarly, PSAdt was greater for patients with pelvic recurrences than for patients with extrapelvic lesions (17.2 ± 17.1 vs. 6.2 ± 5.7 mo, P < 0.001).

A 63-y-old patient with BCR PCa (primary tumor T3bN1, Gleason 4+5) who reached undetectable PSA after prostatectomy and 2 y of androgen deprivation therapy. PSA started to rise 5 y after initial treatment (PSA, 0.3 ng/mL; PSAdt, 3 mo). 18F-DCFPyL PET/CT images including a maximal-intensity projection and axial views of PET, CT, and fused PET/CT demonstrate focal uptake in a 0.5 cm left common iliac node (arrows). This lesion was not biopsied.
The multivariable regression analysis revealed that PSA, PSAdt, and Gleason score (≥7) were independent predictive factors of scan positivity and the presence of extrapelvic disease in postsurgical patients. In the postradiation cohort, PSA and PSAdt were independent predictors for the presence of extrapelvic disease. Multivariable derived coefficients were used to develop nomograms to predict the probability of having a positive scan result and extrapelvic disease. The nomogram based on prior therapy were built using Gleason score, PSA, and PSAdt as predictors (Fig. 7). In postsurgical patients, the area under the curve was 78% (95% CI, 68%–89%) for predicting scan positivity and 76% (95% CI, 67%–85%) for predicting extrapelvic disease. In the postradiation cohort, the area under the curve was 85% (95% CI, 71%–98%) for predicting extrapelvic disease. The number of patients having a negative scan was only 4; therefore, the prediction model for scan positivity was not considered for this cohort.

Nomogram predicting likelihood of 18F-DCFPyL PET/CT positivity for different settings of BCR patients after prostatectomy (A) or radiation (B). Instructions were to locate patient’s PSA value and draw straight line to points axis to determinate number of points toward probability of positive scan, to repeat this process for each variable and sum points for each predictor, and to locate final sum of points on total-point axis and draw line straight down to find probability (P) of having positive scan or having scan with extrapelvic lesions.
DISCUSSION
This study demonstrated that 18F-DCFPyL PET/CT detects lesions in most BCR patients. Prostatectomy-bed–only recurrence is associated with the longest duration (mean, 7.4 y) from treatment, indicating the least aggressive disease trajectory. Pelvic nodal involvement is associated with a shorter duration (3.1 y) from treatment, implying a more aggressive trajectory, whereas bone and visceral involvement manifests even earlier (2.3 y) after prostatectomy. The postradiation cohort showed a similar pattern, where bone or visceral involvement was seen after a decreased duration from therapy, compared with prostate recurrences (2.6 vs. 6.7 y). We observed no differences in time from treatment between patients with oligometastases and patients with multiple lesions in different clinical settings, suggesting that oligometastatic disease may be an early form of an aggressive phenotype.
The likelihood of having a scan with extrapelvic lesions was determined in surgical and postradiation patients using nomograms. The most relevant predictors for scan positivity were PSA and PSAdt, in line with other studies. For instance, Rauscher et al. (15) proposed a nomogram to predict positive 68Ga-PSMA-11 PET/CT results in BCR patients after prostatectomy with a PSA of no more than 1 ng/mL. In their analysis, PSA and concurrent androgen deprivation therapy were associated with scan positivity. Ceci et al. reported a nomogram with 82% accuracy, based on International Society of Urological Pathology grade, PSA, and PSAdt as predictors of scan positivity (16). Ma et al. explored predictors of overall upstaging (nodal and metastatic) by PSMA PET/CT, constructing a nomogram using PSA, percentage positive core biopsy, Gleason stage, and cT stage; the predictive model missed only 10% of patients who would have benefited from PSMA PET/CT (17).
PSA in the posttreatment setting is a reliable indicator of disease volume, and PSMA PET/CT demonstrates a relationship between PSA and extent of disease, with ascending percentages of positive scans with higher PSAs. PSAs of less than 1.0 ng/mL are associated with local recurrences and pelvic adenopathy, whereas the proportion of patients with extrapelvic nodal involvement rises with a PSA above 1.0 ng/mL. Bone and visceral metastases become a larger proportion of cases above 2.0 ng/mL. There is, however, considerable overlap in individual cases, as the rate of PSA production within tumors varies greatly. Thus, these data fit a general model of recurrent PCa that suggests several trajectories for disease. Slowly evolving recurrences tend to be confined to the prostate bed, whereas more aggressive tumors propagate to first the pelvic nodes and then the retroperitoneal nodes. More aggressive disease tends to rapidly involve bone and visceral organs. Although there is little doubt that tumors evolve over time, the rate at which this happens depends on the nature of the original tumor. This insight is uniquely provided by PSMA PET, as previously, disease could not be detected at this stage with conventional imaging.
The overall 18F-DCFPyL PET/CT positivity rate was 79.2%, with a detection rate of 48.2% at a PSA of less than 0.5 ng/mL, in line with previous reports (10). The results are equivalent to those of Wondergem et al. (18) using 18F-DCFPyL in 248 patients, identifying lesions in 59% of patients at a PSA of less than 0.5 ng/mL and in 96% at a PSA of more than 2.0 ng/mL. 18F-PSMA-1007 PET/CT exhibited a higher detection rate of 62% in patients with low PSAs (0.2–0.5 ng/mL) but similar results to our series for a PSA of more than 0.5 ng/mL (19). One persistent finding across multiple studies using PSMA PET is that approximately one quarter of scans are negative, suggesting that these patients either do not express sufficient PSMA to be detected or lesions are simply too small to be identified; these cases are associated with low PSAs and likely represent the threshold for PET detection. Using PET/MRI may help to overcome this potential limited sensitivity for detection within the prostate fossa (20). On the other hand, high PSAs (>5.0 ng/mL) are also associated with negative scans; such tumors may represent less differentiated PCa variants or may express other surface markers that might be amenable to different targeted imaging agents. Moreover, disease within the prostate bed may be obscured by radiotracer excretion into the bladder. Other 18F-PSMA ligands with low urinary excretion, 18F-PSMA-1007 (21) and 18F-rhPSMA (22), have shown higher local detection rates at low PSAs because the interpretation of lesions near the urinary bladder may be somewhat easier. Several groups proved that the use of diuretics increases detectability of local recurrence, with improved diagnostic certainty for lesions near the bladder and ureters (23,24), although forcing diuresis could be an issue for patients with urinary urgency and might require a longer waiting time for patients or additional scans.
18F-DCFPyL–positive pelvic lesions were present in 48% of subjects, whereas extrapelvic disease was found in 30%, almost exclusively when PSA was more than 1.0 ng/mL. This finding is consistent with the clinical experience that control rates with pelvic radiation therapy start to decline when PSA is more than 1 ng/m (25). This agrees with previous data (26,27) assessing the impact of PSMA PET on treatment decisions; patients with a low PSA and disease confined to the pelvis on PSMA PET might benefit from modifications to the plan for radiation treatment, whereas patients with extrapelvic lesions may require systemic therapy. In our cohort, at a PSA of more than 2.0 ng/mL, PSMA PET was almost always positive for recurrence, with distant disease seen in about 30% of prostatectomy patients and 45% of patients after radiation therapy. Furthermore, the presence of distant extrapelvic disease was significantly higher for patients with a rapid PSAdt in both postsurgical and postradiation cohorts, consistent with other prognostic indicators associated with PSAdt (28).
Interesting differences were seen between postsurgical and postradiation recurrences. Negative scan results in patients with a PSA of less than 0.5 ng/mL after surgery were seen in 24% of patients, whereas only 8% of postradiation scans were negative. Postradiation patients tended to show more local recurrences than did postsurgical patients. At a PSA of more than 2.0 ng/mL, recurrences after radiation tended to be extrapelvic, whereas this trend was less evident in postsurgical patients. The distribution of recurrences was somewhat different for postsurgical and postradiation patients. PSA thresholds for positive PSMA PET results were substantially higher in the postradiation cohort. When subjects were treated primarily with radiation, 36% showed positive prostate findings, whereas recurrences outside the prostate were seen in 56% of patients, similar to prior reports using 68Ga-PSMA PET/CT (29).
There were limitations to this study. Perhaps most notably, despite use of 18F-DCFPyL PET/CT at both institutions, the PET acquisition parameters (e.g., time from injection to imaging) varied between institutions. Although detection rates by PSA were overall similar between institutions scanning at 1 versus 2 h after injection, differences in detection rates regarding scan time cannot be addressed since individual patients were scanned at only 1 time point. Further, data harmonization relied on daily quality control procedures using the standard operating procedure provided by the manufacture for each scanner. Such heterogeneity may have affected the results, although reflecting a real-world scenario that make the findings more broadly applicable, as 18F-DCFPyL is recently Food and Drug Administration–approved. Further, findings were determined at each institution individually, followed by a combined analysis, which might lead to heterogeneity in the results but would recapitulate the use of the PSMA agent across centers. Another limitation is that no interreader variability (κ) is available for this study. Also, analyses were exploratory, and adjustments for multiple comparisons were not implemented. Lastly, at 1 institution, patients were accrued into a broader study of the utility of PSMA PET instead of a dedicated BCR study. As such, this study was not prospectively designed to meet a specific endpoint. Furthermore, the detection rate may differ from the true detection rate since histologic validation was not available for all positive sites. Unfortunately, this is a common problem in studies involving BCR patients, for whom findings are often subcentimeter, deep within the pelvis, often in unsafe locations, or otherwise not feasible to biopsy.
CONCLUSION
18F-DCFPyL PET/CT successfully identifies sites of recurrence proportional to PSA levels when conventional imaging results are negative. 18F-DCFPyL PET/CT demonstrates a high tumor detection rate even at a low PSA (<0.5 ng/mL). Disease recurrence tends to be confined to the pelvis in patients with lower PSAs, but at higher values there is visualization of disease outside the pelvis, particularly when PSA is more than 2.0 ng/mL and PSAdt is less than 6 mo. The presence of bone and visceral lesions was associated with a shorter time after initial treatment and higher PSAs than is the case with prostate-bed–only recurrences. Clinical nomograms proved that PSA and PSAdt were able to predict scan positivity and disease location in BCR patients. These tools might guide clinicians to select the most suitable candidates for PSMA PET.
As with other studies, PSMA PET is not positive in all BCR patients, and approximately 15%–20% have negative scans at low or high PSAs, likely for different reasons. Low-PSA false-negatives are likely due to subthreshold volumes of disease for detection, or overlapping with the urinary bladder within the pelvis, whereas high-PSA false-negatives are likely due to dedifferentiated tumors with low PSMA expression. 18F-DCFPyL PET/CT detection efficacy is comparable to previously published results with 68Ga-PSMA compounds and has logistic advantages because of its longer half-life. The general class of PSMA ligands is destined to significantly change management of BCR patients.
DISCLOSURE
Martin Pomper is a coinventor on a U.S. patent covering 18F-DCFPyL and is entitled to a portion of licensing fees and royalties generated by this technology; this arrangement was approved by Johns Hopkins University in accordance with conflict-of-interest policies. Michael Gorin and Steven Rowe are consultants to Progenics, a licensee of 18F-DCFPyL. Michael Gorin, Kenneth Pienta, Martin Pomper, and Steven Rowe receive research support from Progenics. This project has been funded in whole or part with federal funds from National Cancer Institute, NIH, contract HHSN261200800001E. This publication does not necessarily reflect views or policies of the Department of Health and Human Services, nor does mention of trade names, commercial products, or organizations imply endorsement by the U.S. Government. Aloyse Fourquet is a recipient of an ARC Foundation research grant. We acknowledge funding from Prostate Cancer Foundation Young Investigator Award, Progenics, and the National Cancer Institute (CA134675, CA183031, CA184228, and EB024495). No other potential conflict of interest relevant to this article was reported.
KEY POINTS
QUESTION: Are there factors predicting PSMA PET disease location in BCR PCa patients?
PERTINENT FINDINGS: PSA and PSAdt are able to predict PSMA PET scan positivity and disease location. The presence of bone/visceral lesions is associated with shorter intervals from initial treatment than are prostate-bed–only recurrences.
IMPLICATIONS FOR PATIENT CARE: These tools might guide clinicians to select suitable candidates for 18F-DCFPyL PET/CT.
Footnotes
Published online Dec. 16, 2021.
- © 2022 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication March 26, 2021.
- Accepted for publication December 2, 2021.
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.