


Abstract
L-[3-18F]-α-methyl tyrosine (18F-FMT) is an amino-acid tracer for PET imaging. We evaluated the prognostic significance of 18F-FMT PET in patients with non–small cell lung cancer. Methods: Ninety-eight patients (80 men and 18 women; age range, 42–82 y; median age, 69 y) with stage I–IV non–small cell lung cancer were enrolled in this study. They included 57 with adenocarcinoma, 31 with squamous cell carcinoma, 5 with large cell carcinoma, and 5 with other conditions. The median follow-up duration was 17.0 mo. A pair of PET studies with 18F-FMT and 18F-FDG was performed, and tracer uptake by the primary tumor was evaluated using the maximal standardized uptake value (SUVmax). Overall survival and disease-free survival were calculated by the Kaplan–Meier method. The prognostic significance was assessed by univariate and multivariate analyses. Results: The best discriminative SUVmax cutoffs for 18F-FMT and 18F-FDG in the primary tumors were 1.6 and 11, respectively. In the univariate analysis, a high SUVmax was significant in predicting poor overall survival for 18F-FMT (P = 0.0129) and 18F-FDG PET (P = 0.0481). According to histologic types, 18F-FMT and 18F-FDG uptake were a stronger prognostic predictor in adenocarcinoma than in nonadenocarcinomatous disease. Patients with a high SUVmax for 18F-FMT showed significantly worse disease-free survival rates than those with a low SUVmax, and multivariate analysis confirmed that a high SUVmax for 18F-FMT was an independent and significant factor in predicting a poor prognosis in patients with adenocarcinoma (P = 0.0191). Conclusion: Uptake of 18F-FMT in primary tumors was an independent prognostic factor in patients with pulmonary adenocarcinoma.
Lung cancer is the leading cause of cancer death in many countries, and 80% of lung cancers are non–small cell lung cancer (NSCLC) (1). NSCLC has a poor prognosis, and clinical markers that may predict the prognosis should be investigated. Disease stage and performance status have consistently been shown to be the most powerful prognostic tools for survival rates of NSCLC patients (2). However, there has been no established clinical marker that correlates with the response to treatment and the prognosis in NSCLC patients (3).
Recent advances in PET with 18F-FDG have enabled not only the diagnosis and staging of lung cancer but also the prediction of its malignancy grade (4–7). Moreover, it has been reported that 18F-FDG uptake on PET can be a prognostic factor in NSCLC patients (8,9). However, several researchers found that 18F-FDG uptake in the primary tumors of NSCLC did not have a significant relationship with survival (10,11). There is insufficient evidence that 18F-FDG uptake on PET provides prognostic information in NSCLC patients.
We have developed L-[3-18F]-α-methyl tyrosine (18F-FMT) as an amino-acid tracer for PET and confirmed its potential usefulness in the detection of neoplasms using experimental tumor models (12–17). 18F-FMT, an amino acid analog, accumulates in tumor cells solely via an amino-acid transport system (17). Recent clinical trials have demonstrated that 18F-FMT PET is useful for differentiating between benign lesions and malignant tumors (13–17). However, 18F-FMT uptake in the primary tumors was significantly lower than 18F-FDG uptake (15–17). Although 18F-FMT uptake on PET has been found to be specific for tumor cells (17), the prognostic significance of 18F-FMT uptake in human neoplasms remains undetermined. On the basis of this background information, we conducted this study to compare the prognostic significance of 18F-FMT with that of 18F-FDG PET in NSCLC patients.
MATERIALS AND METHODS
Patients
This study was conducted on 106 consecutive NSCLC patients who underwent 18F-FDG PET and 18F-FMT PET from November 2005 to December 2007 at the Gunma University Hospital, Japan, a teaching and tertiary care hospital and a major referral site for patients with cancer. 18F-FMT PET was performed as part of the staging work-up. The patients also underwent 18F-FDG PET, CT of the thorax, whole-body bone scanning for the detection of possible distant metastases, and bronchoscopy with biopsy for diagnostic confirmation. The 18F-FDG PET and 18F-FMT PET were performed in random order, and the mean interval between the PET studies was 6 d. Patients in whom findings on CT, 18F-FDG PET, or both were consistent with stage N3 disease also underwent diagnostic mediastinoscopy. Depending on the results of staging, patients then underwent either chemotherapy or surgical management. Staging was conducted in accordance with internationally accepted guidelines. Seven patients were excluded from further studies because PET using 18F-FDG or 18F-FMT showed no visible tracer uptake in the primary tumor. The 7 patients were pathologically diagnosed with noninvasive bronchioloalveolar carcinoma (stage I). All patients were required to have had at least 3 mo of follow-up. Thus, 98 patients (80 men and 18 women) with a median age of 69 y (range, 42–82 y) were analyzed in the study.
Histologic analysis revealed adenocarcinoma in 57 patients, squamous cell carcinoma in 31, large cell carcinoma in 5, and other conditions in 5. The median follow-up duration was 17.0 mo. All patients agreed to participate in this study and provided written informed consent. The study protocol was approved by the institutional review board.
Clinical and pathologic TNM stages were established using the International System for Staging Lung Cancer adopted by the American Joint Committee on Cancer and the Union Internationale Centre le Cancer (18). Surgery was performed on 65 patients and consisted of lung resection and mediastinal lymphadenectomy in 60 patients and exploratory thoracotomy in 5. Of the 5 patients who underwent only exploratory thoracotomy, 4 had pleural dissemination and 1 had infiltration of the aorta. In the remaining 33 patients, diagnostic staging and histologic confirmation of malignancy was performed by means of mediastinoscopy, bronchoscopy, or both. The disease was classified as stage I in 30 patients, stage II in 12 patients, stage III in 42 patients, and stage IV in 14 patients. Of the 42 patients with stage III, 24 were stage IIIA and 18 were stage IIIB.
Treatment
After a definite diagnosis and PET studies, 28 patients were treated with chemotherapy, 10 patients were treated with chemoradiotherapy, and 60 patients were treated with surgical excision of the primary tumor and mediastinal lymphadenectomy. Of the patients who had surgical treatment, 1 received neoadjuvant chemotherapy and 24 received postoperative adjuvant therapy. Thirty-five patients received only surgery. Of the 24 patients who had been treated with postoperative adjuvant therapy, 7 received orally administered tegafur and 18 received platinum-based chemotherapy.
PET Studies
18F-FMT was synthesized in our cyclotron facility according to the method developed by Tomiyoshi et al. (12). The radiochemical yield of 18F-FMT was approximately 20%, and radiochemical purity was approximately 99%. 18F-FDG was also produced in our facility as described previously (19). The patients fasted for at least 6 h before the PET studies, which were performed using a whole-body scanner with Bi4Ge3O12 crystals (SET 2400W; Shimadzu) and a 59.5-cm transverse field of view, producing 63 image planes with a 3.123-mm interval between images. The transverse resolution at the center of the field of view was 4.2 mm in full width at half maximum.
A 2-dimensional data acquisition was initiated 50 min after the injection of 4–5 MBq of 18F-FMT per kilogram or 5–6 MBq of 18F-FDG per kilogram as described previously (13). The image protocol was set to use a simultaneous emission–transmission method with a rotating external source (370 MBq of 68Ge–68Ga at the time of installation) and to acquire 4–10 bed positions (an 8-min acquisition per bed position) according to the range of imaging. In cases of bone and skin lesions, a maximum of 10 bed positions was acquired to cover the whole body. Attenuation-corrected transverse images obtained with 18F-FMT and 18F-FDG were reconstructed with the ordered-subsets expectation maximization algorithm into 128 × 128 matrices with pixel dimensions of 4.0 mm in-plane and 3.125 mm axially. Coronal images with a 9.8-mm section thickness were also reconstructed from attenuation-corrected transverse images for visual interpretation.
Data Analysis
All 18F-FDG and 18F-FMT PET images were interpreted by 2 experienced nuclear physicians. The interpreting physicians were unaware of the patient's clinical history and data. We measured tracer uptake in the primary tumor. Uptake that was either moderate or intense was defined as a positive finding on visual interpretation, and either the absence of uptake or uptake that was faint (less than that in normal mediastinum) was defined as a negative finding. Discrepant results were resolved by consensus. For the semiquantitative analysis, functional images of the standardized uptake value (SUV) were produced using attenuation-corrected transaxial images, the injected doses of 18F-FMT and 18F-FDG, the patient's body weight, and the cross-calibration factor between PET and dose calibrator (20). SUV was defined as radioactive concentration in the region of interest (ROI) (MBq/g) divided by injected dose (MBq) divided by patient's body weight (g).
An ROI was manually drawn on the SUV images over the primary tumor. When the tumor was larger than 1 cm in diameter, irregularly shaped, or multifocal, an ROI of approximately 1 cm in diameter was drawn over the area corresponding to the maximal tracer uptake. The SUV of the background was defined by drawing an ROI on a nonlymphadenopathic site in the mediastinum. When the lesion showed no significant tracer uptake, the ROI was placed retrospectively on the PET image with reference to the CT image. ROI analysis was conducted by a nuclear physician with the aid of corresponding CT scans. The maximal SUV in the ROI was used as a representative value for the assessment of 18F-FMT and 18F-FDG uptake in the lesion.
Statistical Analysis
Survival was recorded from histologic diagnosis to death or last follow-up, and the survival curves were calculated according to the Kaplan–Meier method. SUVs are expressed as mean ± SD. Probability values of less than 0.05 indicated a statistically significant difference. The Fisher exact test was used to examine the association of 2 categoric variables. The correlation of SUVs between 18F-FMT and 18F-FDG uptake was analyzed using the Pearson rank test. Survival difference was analyzed by the log-rank test. Overall survival (OS) was defined as the time between diagnosis and death from any cause. Disease-free survival (DFS) was defined as the time between diagnosis and the first recurrence of the disease (local–regional or distant recurrence). Multivariate analyses were performed using the stepwise Cox proportional hazards model to identify independent prognostic factors among various demographic, clinical, pathologic, and PET findings. Statistical analysis was performed using JMP 8 (SAS Institute Inc.) for Windows (Microsoft).
RESULTS
Patient characteristics according to the maximal SUV (SUVmax) cutoff are listed in Table 1. A high SUVmax on 18F-FMT PET (>1.6) was significantly associated with the male sex, an advanced stage, and nonadenocarcinomatous disease, and a high SUVmax on 18F-FDG PET (>11.0) was significantly associated only with advanced stage. 18F-FDG PET and 18F-FMT PET images are shown in Figure 1.
Patient Characteristics

PET images of 62-y-old man with adenocarcinoma of left lung (p-T2N0M0). Both 18F-FDG (A) and 18F-FMT (B) showed increased uptake in primary tumor.
SUV for Primary Tumor
In the 98 patients, the SUVmax of 18F-FMT ranged from 0.6 to 5.8, with a median of 1.6 (mean ± SD, 1.8 ± 1.0), and that of 18F-FDG ranged from 0.9 to 29.6, with a median of 6.8 (mean, 8.1 ± 5.3). This difference was significant (P < 0.001). The SUVmax of 18F-FMT in adenocarcinoma patients ranged from 0.6 to 4.3, with a median of 1.5 (mean, 1.6 ± 0.8), and that in nonadenocarcinoma patients ranged from 0.7 to 5.8, with a median of 1.9 (mean, 2.1 ± 1.1). This difference was also significant (P = 0.0031). However, the SUVmax of 18F-FDG in adenocarcinoma patients ranged from 0.9 to 21.5, with a median of 6.2 (mean, 7.2 ± 4.4), and that in nonadenocarcinoma patients ranged from 0.9 to 29.6, with a median of 7.4 (mean, 9.3 ± 6.2), and this difference was not significant (P = 0.0574).
The SUVmax of 18F-FMT in the primary tumors correlated significantly with that of 18F-FDG (Pearson rank correlation = 0.6449, P < 0.0001). Moreover, the maximal SUVs in the hilar and mediastinal nodes were a median of 1.6 (mean, 2.0 ± 1.1) for 18F-FMT PET and 4.7 (mean, 5.9 ± 3.7) for 18F-FDG PET. There was a significant difference between primary tumors and lymph nodes for 18F-FDG PET (P = 0.032) but not for 18F-FMT PET (P = 0.346).
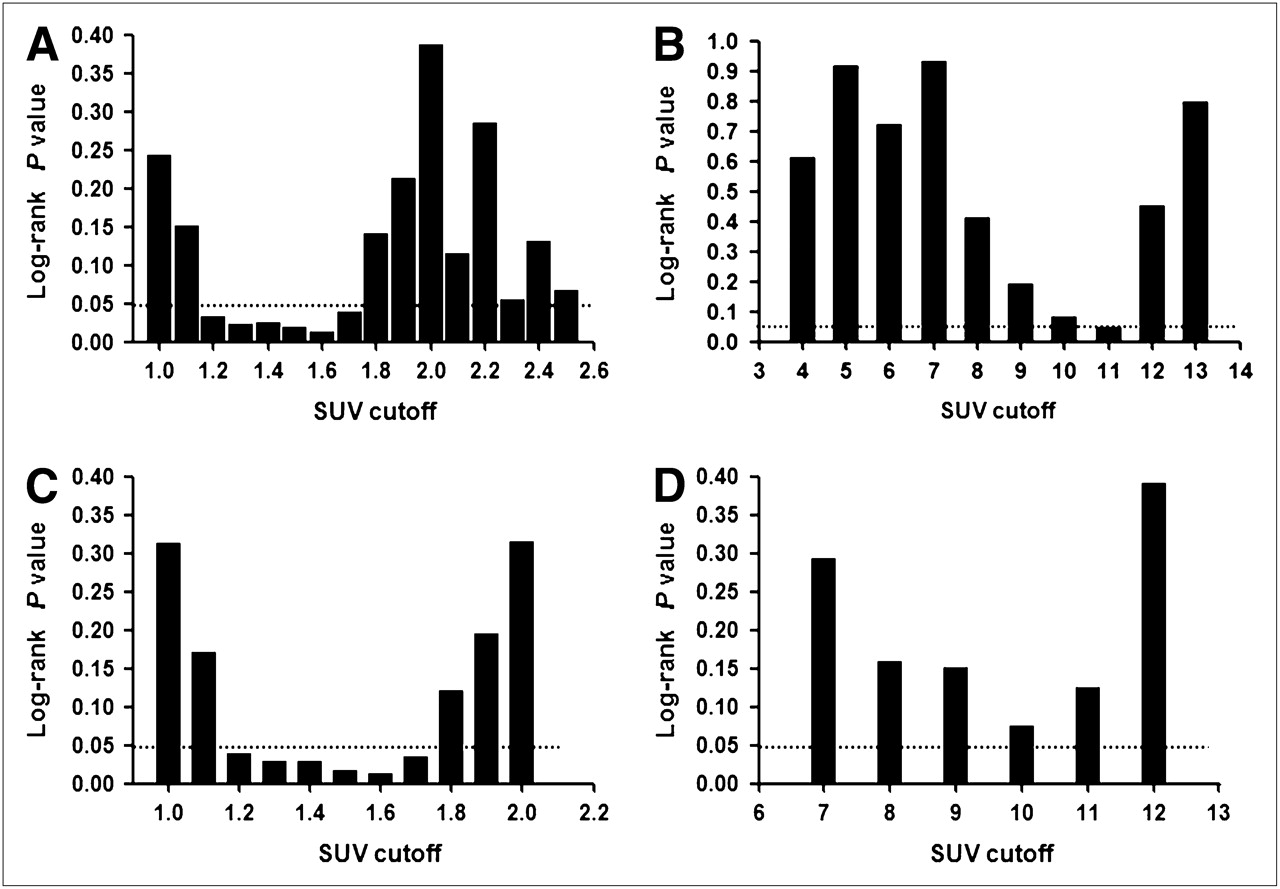
The discriminative value of various SUV cutoffs for 18F-FMT and 18F-FDG uptake by the primary tumor were explored in the context of OS and DFS. In 18F-FMT PET, the most discriminative cutoff for prognosis was an SUV of 1.6 in the OS and DFS analysis. Although a broad SUVmax range, from 1.2 to 1.7, gave significantly discriminative log-rank P values, 1.6 was used as the cutoff SUV in the following analyses (Fig. 2). In 18F-FDG PET, a cutoff of 11 showed significance in the OS analysis, but there was no discriminative cutoff SUV for DFS. Therefore, a cutoff of 11 was selected in the analysis of OS and DFS (Fig. 2).
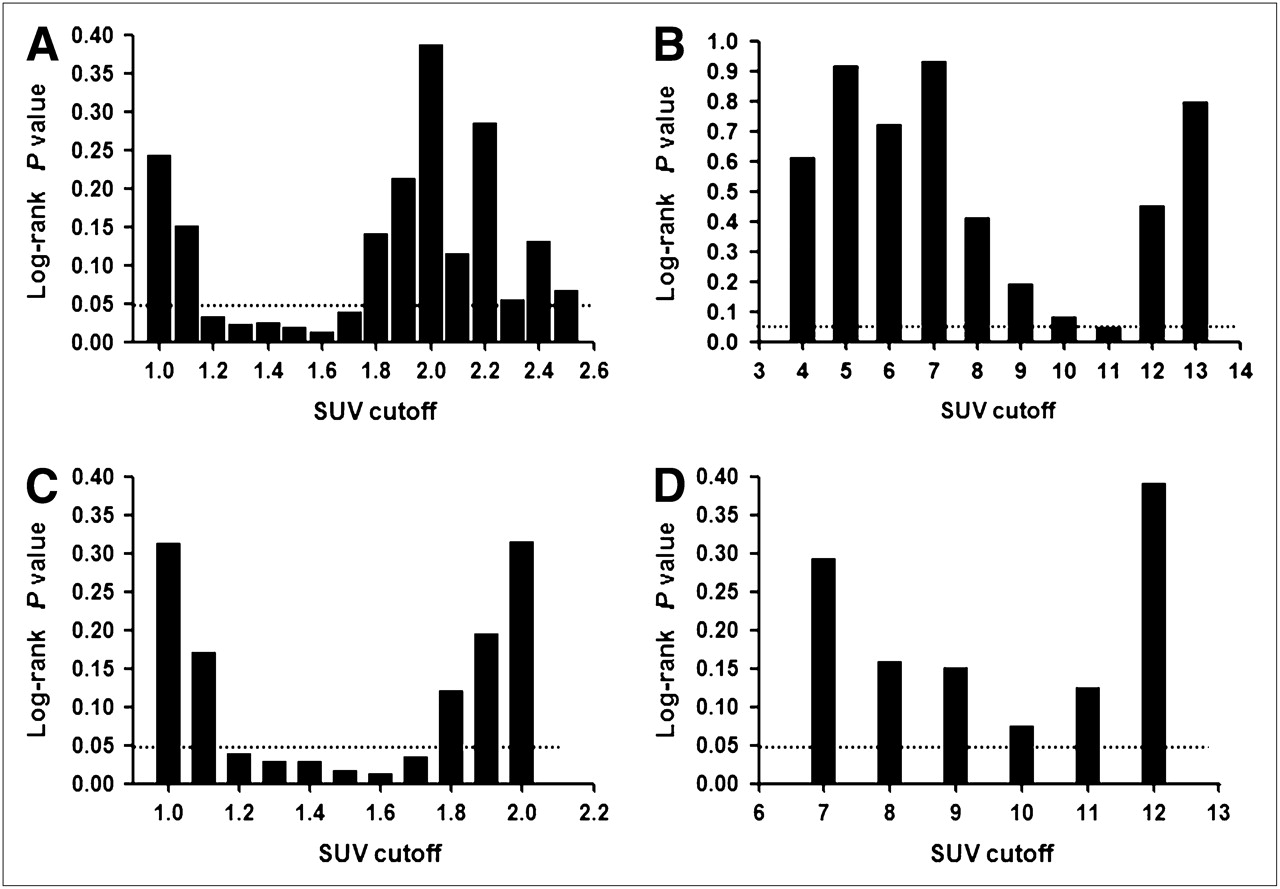
Discriminative value by Log-rank test according to various SUV cutoffs for OS in 18F-FMT PET (A) and 18F-FDG PET (B) and for DFS in 18F-FMT PET (C) and 18F-FDG PET (D).
PET and Survival
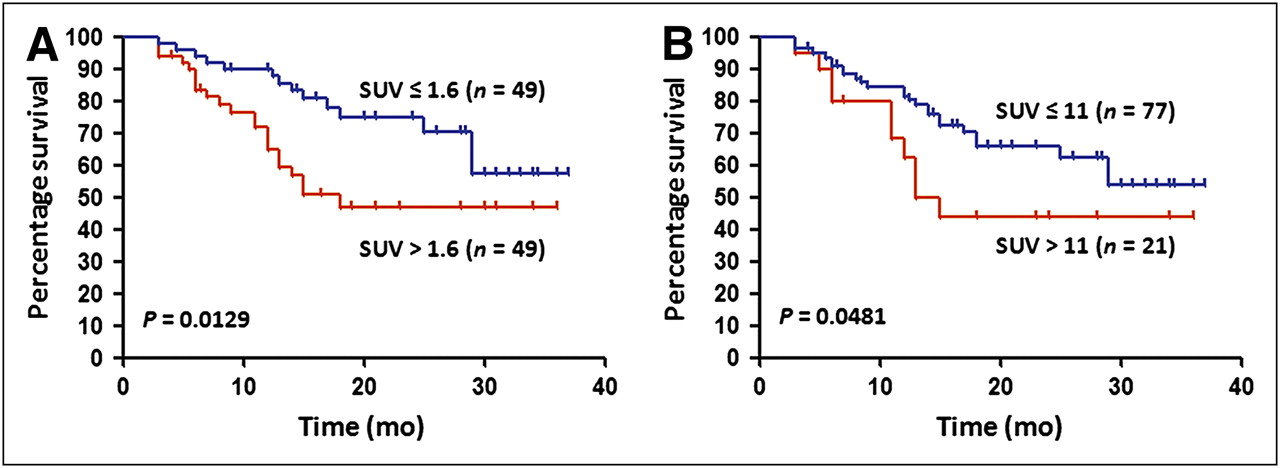
The median survival time was 26.0 mo, and the 2-y OS rate was 54.4%. The 2-y survival rates of patients with a low SUVmax (≤1.6) and those with a high SUVmax (>1.6) on 18F-FMT PET were 75.0% and 46.7%, respectively, demonstrating a significantly poor prognosis for the patients with a high SUV (>1.6) (P = 0.0129; Table 2; Fig. 3A). However, the 2-y OS rates of the patients with a low SUVmax (≤11) and those with a high SUVmax (>11) on 18F-FDG PET were 67.2% and 40.9%, respectively, demonstrating a significantly poor prognosis for the patients with a high SUVmax (>11) (P = 0.0481; Table 2; Fig. 3B). Survival analysis according to histology is listed in Table 2. The adenocarcinoma patients with a high SUVmax on both PET studies demonstrated a significantly poor prognosis, compared with those with a low SUVmax. In the patients without adenocarcinoma, however, no significant difference was observed between high SUVmax and low SUVmax group on either PET study. A survival analysis of prognostic factors is presented in Table 3. Univariate analysis confirmed that advanced stage and high SUVmax on 18F-FDG PET and 18F-FMT PET were significant predictors of a poor prognosis, and multivariate analysis confirmed that only advanced stage was an independent and significant predictor of a poor prognosis.
Two-Year Survival Rate According to Histology and Results of PET Studies in 98 Patients
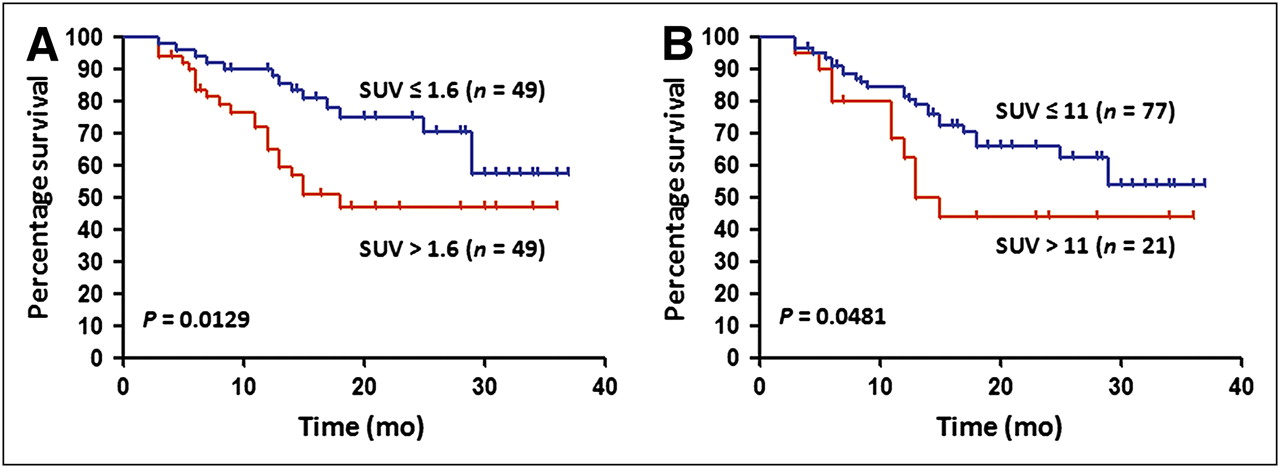
OS of 98 patients with non–small cell cancer according to SUV for primary tumor in 18F-FMT PET (A) and 18F-FDG PET (B).
Univariate and Multivariate Analysis of Prognostic Factors in All Patients (n = 98)
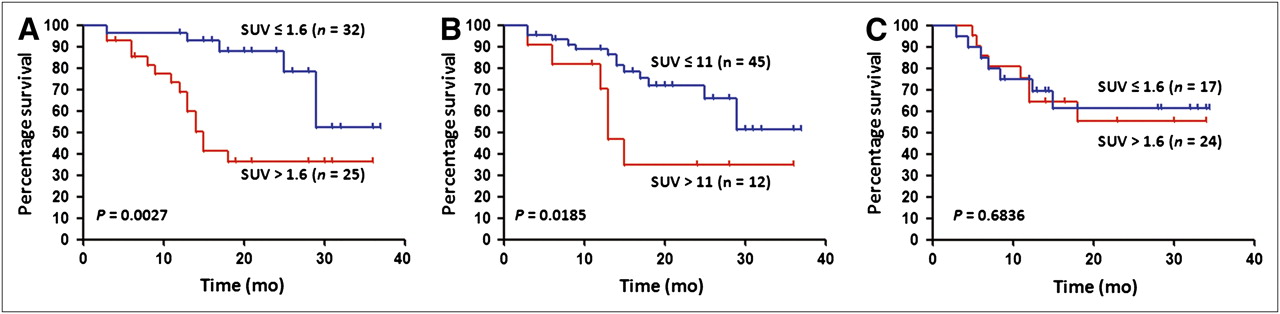
We performed a univariate and multivariate analysis of OS on 57 adenocarcinoma patients. The median survival was 28.5 mo, and the 2-y OS rate was 64.2%. The 2-y survival rates of the patients with a low SUVmax (≤1.6) and those with a high SUVmax (>1.6) on 18F-FMT PET were 81.5% and 37.7%, respectively, and the patients with a high SUVmax (>1.6) showed a significantly poor prognosis (P = 0.0027; Table 2; Fig. 4A). However, the 2-y OS rates of the patients with a low SUVmax (≤11) and those with a high SUVmax (>11) on 18F-FDG PET were 65.8% and 31.7%, respectively, and the patients with a high SUVmax (>11) showed a significantly poor prognosis (P = 0.0185; Table 2; Fig. 4B). Univariate and multivariate analysis confirmed that advanced stage and high SUVmax on 18F-FMT PET were independent and significant predictors of a poor prognosis (Table 4).
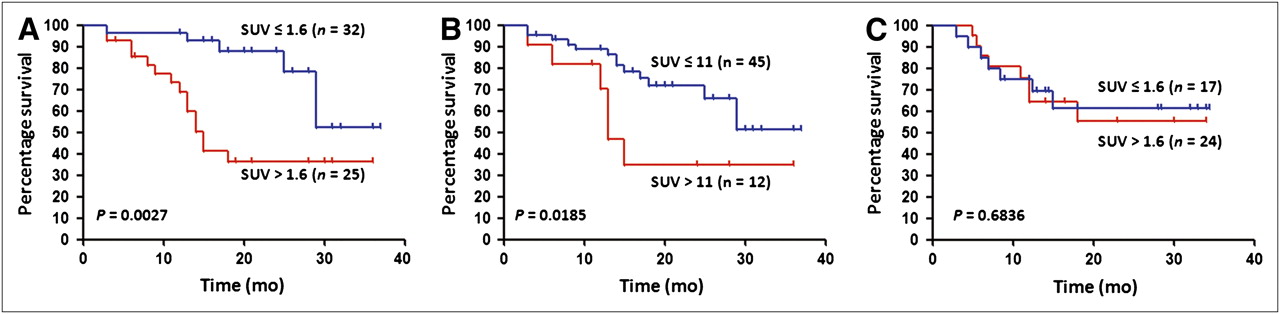
(A and B) OS of 57 patients with adenocarcinoma according to SUV in 18F-FMT PET (A) and 18F-FDG PET (B). (C) OS of 41 patients with nonadenocarcinoma according to SUV in 18F-FMT PET.
Univariate and Multivariate Analysis of Prognostic Factors in Adenocarcinoma Patients (n = 58)
Next, we performed a univariate and multivariate analysis of OS in 41 nonadenocarcinoma patients. The median survival was 25.0 mo, and the 2-y OS rate was 58.6%. No significant difference in OS was observed between high-SUVmax and low-SUVmax groups on 18F-FMT or 18F-FDG PET (Table 2; Fig. 4C).
We examined the association between SUVmax and DFS in 98 patients. The results are listed in Table 2. The patients with a low SUVmax on 18F-FMT PET showed significantly better DFS rates than those with a high SUVmax, whereas those with a low SUVmax on 18F-FDG PET did not show significantly better DFS rates than those with a high SUVmax. In the 98 patients and 57 adenocarcinoma patients, a high SUVmax on 18F-FMT was a significant factor in predicting a poor prognosis in the univariate analysis but not in the multivariate analysis.
DISCUSSION
The present study evaluated the prognostic significance of 18F-FMT PET in patients with NSCLC. The results revealed that 18F-FMT uptake with a cutoff SUVmax of 1.6 for the primary tumor was a significant independent factor in predicting a poor prognosis in patients with adenocarcinoma. On the other hand, 18F-FDG uptake was a significant prognostic factor for OS only in the univariate analysis. These results indicate that, compared with 18F-FDG PET, 18F-FMT PET seems to be the stronger prognostic factor in patients with NSCLC, especially adenocarcinoma. In patients without adenocarcinoma, 18F-FMT uptake in the primary tumor did not have a significant relationship with survival.
Because 18F-FMT did not accumulate in benign lesions and, on the basis of our clinical experience, is relatively specific to malignant tumors (16), we supposed that 18F-FMT uptake would reflect the metabolic viability of the malignant tumor cells. Recently, we found that 18F-FMT uptake correlated with the expression of L-type amino acid transporter 1 (LAT1) and that both LAT1 expression and 18F-FMT uptake were significantly higher in nonadenocarcinomatous disease than in adenocarcinoma (17). In the present study, the mean SUVmax of 18F-FMT differed significantly between adenocarcinoma (mean, 1.6 ± 0.8) and nonadenocarcinomatous disease (mean, 2.1 ± 1.1; P = 0.0031). LAT1 is widely expressed in primary human cancers and several cancer cell lines, where it has been shown to play essential roles in growth and survival (21–25). LAT1 is overexpressed in malignant tumors and is associated with tumor proliferation, angiogenesis, and poor survival. We recently found that positive expression of LAT1 was an independent and significant factor in predicting a poor prognosis in patients with resectable stage I–III NSCLC (26). Our previous studies also showed that overexpression of LAT1 in adenocarcinoma patients was the strongest prognostic factor among patients with NSCLC (27). This background information seems to indicate that the prognostic significance of 18F-FMT uptake in NSCLC is closely correlated with that of LAT1 expression.
The prognostic value of 18F-FDG PET has been evaluated in previous studies (28). Several researchers found that patients with low 18F-FDG uptake in their primary tumor have a significantly longer OS and DFS than patients with high 18F-FDG uptake (8,9,28). The prognostic significance of 18F-FDG uptake is dependent on the histologic cell type of NSCLC, and 18F-FDG uptake by adenocarcinoma correlates with the pathologic tumor stage and tumor invasiveness (29,30). In this study, a high SUVmax of 18F-FDG uptake (>11) was significantly associated with poor prognosis in patients with NSCLC. However, 18F-FDG uptake was not a significant prognostic factor for survival in the multivariate analysis. It is unclear whether 18F-FDG uptake could correlate with the prognosis of patients. In the future, this point should be confirmed by studies having a homogeneous patient cohort.
One limitation of our study is that our population was not homogeneous, with the same tumor stage, the same tumor histology, and the same therapeutic protocol. In this study, tumor stages were various and treatment methods differed among patients. Moreover, the lesions of 40 (40.8%) of the 98 patients were of a nonadenocarcinomatous histology, and the proportion of adenocarcinoma patients (58/98, 59.2%) was lower than in previous studies. Another limitation is that the study did not analyze large numbers of patients with a long follow-up period. A large-scale study with a longer follow-up is warranted. Moreover, the limitation of 18F-FMT PET is that the SUV of 18F-FMT is relatively low, compared with the other PET tracers (31).
CONCLUSION
18F-FMT uptake in the primary tumor was a significant independent predictor of poor prognosis in patients with pulmonary adenocarcinoma. 18F-FMT PET seems to be a stronger prognostic factor than 18F-FDG PET. Further investigations are required to confirm the prognostic significance by a conjugated analysis of the 18F-FMT uptake and LAT1 expression of the primary tumor in patients with NSCLC.
Acknowledgments
We thank Hisao Imai, Takeshi Hisada, Rieko Kaira, and Tetsuya Higuchi for their assistance in data collection and analysis of this study. Our clinical trial registration number at ClinicalTrials.gov is NCT00464282.
Footnotes
-
COPYRIGHT © 2009 by the Society of Nuclear Medicine, Inc.
References





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- First Clinical Results of (D)-18F-Fluoromethyltyrosine (BAY 86-9596) PET/CT in Patients with Non-Small Cell Lung Cancer and Head and Neck Squamous Cell Carcinoma
- Use of Pre-treatment 18F-FAMT PET to Predict Patient Survival in Squamous Cell Carcinoma of the Esophagus Treated by Curative Surgery
- Radiolabeled Amino Acids for Oncologic Imaging
- Comparative Evaluation of 18F-Labeled Glutamic Acid and Glutamine as Tumor Metabolic Imaging Agents
- Transport of 3-Fluoro-L-{alpha}-Methyl-Tyrosine by Tumor-Upregulated L-Type Amino Acid Transporter 1: A Cause of the Tumor Uptake in PET
- Relationship between LAT1 Expression and Response to Platinum-based Chemotherapy in Non-small Cell Lung Cancer Patients with Postoperative Recurrence