


Abstract
Although 131I-iodine (RAI) therapy is a mainstay in the treatment of metastatic thyroid cancer, there is controversy regarding the maximum activity that can safely be administered without dosimetric determination of the maximum tolerable activity (MTA). At most institutions, a fixed empiric dosing strategy is often used, with administered activities ranging from 5.55 to 9.25 GBq (150–250 mCi). In our experience with dosimetry, we have observed that this empiric dosing strategy often results in administered RAI activities exceeding the MTA safety limit of 200 cGy (rads) to the blood or bone marrow in many patients with metastatic thyroid cancer. Methods: We retrospectively analyzed 535 hypothyroid dosimetry studies performed as part of routine clinical care in 328 patients with apparently normal renal function. Results: The MTA was less than 5.18 GBq (140 mCi) in 3%, less than 7.4 GBq (200 mCi) in 8%, and less than 9.25 GBq (250 mCi) in 19%. Analysis of MTA values by age at the time of dosimetry revealed little change in the MTA until the age of 70 y, when a significant decrease occurred. An empiric administered activity of 7.4 GBq (200 mCi) would exceed the MTA in 8%−15% of patients less than 70 y old and 22%−38% of patients 70 y old or older. However, administration of 9.25 GBq (250 mCi) would exceed the MTA in 22% of patients less than 70 y old and 50% of patients 70 y old or older. Factors associated with a lowering of MTA to less than 9.25 GBq (250 mCi) were age at dosimetry greater than 45 y, the female sex, subtotal thyroidectomy, and RAI-avid diffuse bilateral pulmonary metastases. Conclusion: Administered RAI activities of less than 5.18 GBq (140 mCi) rarely exposed blood to more than 200 cGy except in the very elderly. However, administered activities of 7.4–9.25 GBq (200–250 mCi) frequently exceeded the calculated MTA in patients 70 y old or older. Therefore, dosimetry-guided RAI therapy may be preferable to fixed-dose RAI treatment strategies in older patients with thyroid cancer and in patients with RAI-avid diffuse bilateral pulmonary metastases, even when renal function is normal.
Treatment of metastatic thyroid cancer with radioiodine began in the early 1940s (1,2). Although radioactive iodine therapy has significant tumoricidal effects, repeated dosing is associated with clinically apparent bone marrow depression (3). Dosimetry methods were developed in the 1950s to assess the body's retention of radioactive iodine and to estimate the absorbed doses to the blood and bone marrow. These techniques enable clinicians to calculate the maximum tolerable activity (MTA) of 131I-iodine (RAI), or the amount that can be administered without producing toxic effects on the bone marrow. By the late 1950s, a dosimetry-based approach determining the MTA of RAI was routinely used in the management of thyroid cancer patients at Memorial Sloan-Kettering Cancer Center (4). Dosimetry defines important safety parameters that guide the use of multiple large, therapeutic administered activities of RAI (5,6), even though there are yet no data demonstrating the superiority of this practice over the use of repeated smaller doses of RAI.
Current dosimetry protocols are remarkably similar to those described more than 50 y ago (4). After administration of a tracer amount of RAI, serial measurements of retained radioactivity in blood and in the whole body are measured over a 4-d period. These measurements are used to calculate an administered activity that would deliver no more than 200 cGy to the blood or bone marrow (or result in 2.96 GBq [80 mCi] of whole-body retention at 48 h if there was diffuse lung disease) for each patient (7). The theoretic benefit of dosimetry is to maximize the delivered radiation to the tumor without incurring unacceptable adverse consequences. Unfortunately, dosimetry is labor intensive, time consuming, and expensive.
Because the administered activities commonly used in RAI ablation of normal remnants—for example, 1.11−5.55 GBq (30−150 mCi)—are usually well below the MTA predicted by formal dosimetry in healthy patients, most clinicians use empiric dosing strategies to select activities for remnant ablation (8). Most empiric dosing guidelines are similar to those published by Beierwaltes (9), with minor modifications (10–17). In general, administered activities of 1.11−3.7 GBq (30−100 mCi) of 131I are commonly used for ablation of thyroid remnants after total thyroidectomy, whereas metastatic lesions are often treated with empiric administered activities of 5.55−11.1 GBq (150−300 mCi).
The standard of care at our institution is to perform whole-body and blood dosimetry on all patients with metastatic thyroid cancer. This standard is largely based on previous data from our institution demonstrating that administered activities of only 7.4 GBq (200 mCi) would have exceeded the actual measured MTA in 19% of our patients undergoing full dosimetry (18). We observed many cases in which empiric dosing recommendations often exceeded that MTA in older patients and those with large-volume, RAI-avid metastatic disease.
To better understand the distribution of MTAs in our patient population, we retrospectively reviewed all hypothyroid dosimetry procedures at Memorial Sloan-Kettering Cancer Center between 1993 and 1999. We hypothesized that RAI treatment recommendations based on empiric dosing guidelines would exceed the actual measured MTA in a significant proportion of older individuals with metastatic thyroid cancer.
MATERIALS AND METHODS
Study Design
This study was a retrospective review of all hypothyroid dosimetry studies performed at Memorial Sloan-Kettering Cancer Center from March 1993 to January 1999. This study received approval from our Institution Research Board. A dosimetry study was excluded if it involved the use of recombinant human thyroid-stimulating hormone (TSH) or involved patients with a serum creatinine level greater than 2.0 mg/dL at the time of the study.
Sources of clinical data included patient medical records, radioactive iodine scans, and pathology reports. We extracted the following information from each chart: age, sex, histology of tumor, stage of disease, extent of initial surgery (total thyroidectomy vs. lobectomy), results of radiology studies, medications, TSH level, thyroglobulin level, reason for dosimetry (ablation vs. therapy), and serum creatinine level. The data were then masked with regard to the identity of the patient to protect patient confidentiality.
Lesions were considered RAI avid if definite radioactive iodine accumulation was seen within a specific region of interest on the diagnostic 131I scan, including uptake in the neck (thyroid bed or regional metastases) or distant metastases. Pulmonary metastases were classified as either diffuse bilateral uptake or focal nodular uptake in one or more pulmonary lesions based on the diagnostic whole-body scan.
Dosimetry Protocol
In general, levothyroxine was withdrawn 6 wk and triiodothyronine was withdrawn 2 wk before diagnostic testing. All patients were instructed on following a low-iodine diet in preparation for RAI scanning.
Standard hypothyroid blood and whole-body dosimetry was performed as per our standard clinical practice as previously described (7). The MTA—the administered activity that would deliver 200 cGy to the blood (or result in 2.96 GBq [80 mCi] retained at 48 h if there was diffuse lung disease)—was calculated as previously described (4,19). As part of the MTA determination, heparinized whole-blood samples were obtained 4, 24, 72, and 96 h after administration of 37−185 MBq (1−5 mCi) of 131I. Aliquots were counted in an automated scintillation counter to determine activity concentrations. These data were used to determine the locally deposited β-particle dose to the blood. The γ-ray component of dose to blood was determined from whole-body retention measurements taken at similar time points with the addition of 2 early points at 5 min and 2 h. A 131I standard was counted at each time point to monitor the consistency of detector performance. The MTA defines the maximum allowable dose for an individual patient but does not determine the final activity actually administered. The actual dose selected for administration is based on multiple clinical factors including severity of disease, rate of disease progression, prior response to RAI therapy, and willingness to accept the potential side effects of a large administered activity.
Statistical Analysis
All data are presented as the mean ± SEM and medians, with ranges given when appropriate. Continuous variables were compared using the unpaired t test, and categoric variables were compared using χ2 analysis. Repeated measures were analyzed using ANOVA. A P value of less than 0.05 was considered statistically significant.
RESULTS
Between March 1993 and January 1999, 535 hypothyroid dosimetry procedures were performed on the 328 patients. For this article, only the first hypothyroid dosimetry procedure on each patient was selected for analysis.
Table 1 presents the pertinent clinical features of these 328 patients. The mean age at the time of dosimetry was 47 ± 17 y, with a range of 11−88 y.
Clinical Characteristics of Patients
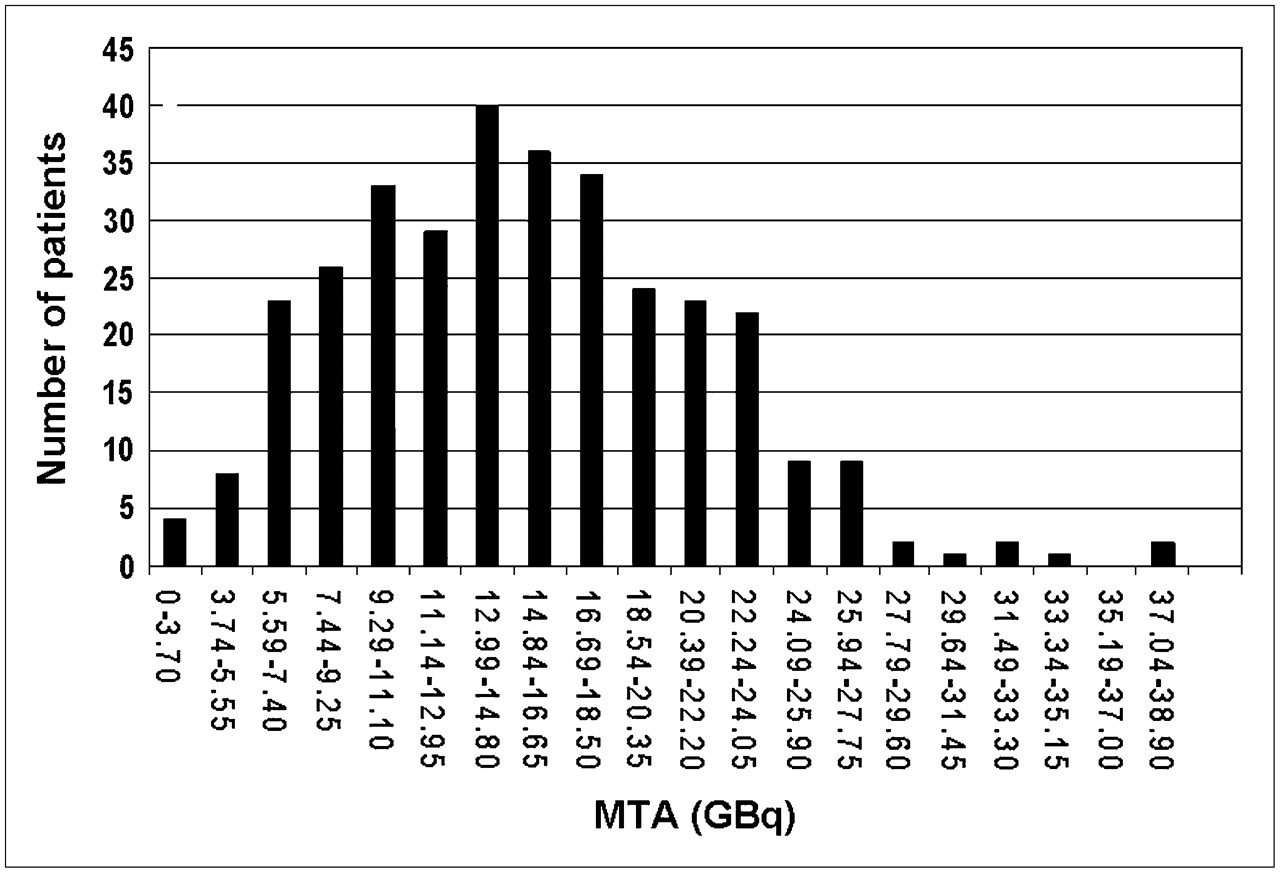
The actual MTA distribution ranged from 2.3 to 37.9 GBq (62−1,024 mCi), with most patients falling within the 7.4- to 24.05-GBq (200−600 mCi) category (Fig. 1). Analysis of the MTAs was based on cutoffs of 5.18, 7.4, and 9.25 GBq (140, 200, and 250 mCi, respectively) to reflect empiric dosing schemes commonly used. Overall, only 3% of patients had an MTA below 5.18 GBq (140 mCi), whereas 8% were below 7.4 GBq (200 mCi) and 19% were below 9.25 GBq (250 mCi) (Fig. 2).

MTA distribution for the 328 patients. Mean MTA is 15.3 ± 6.4 GBq (414 ± 173 mCi).
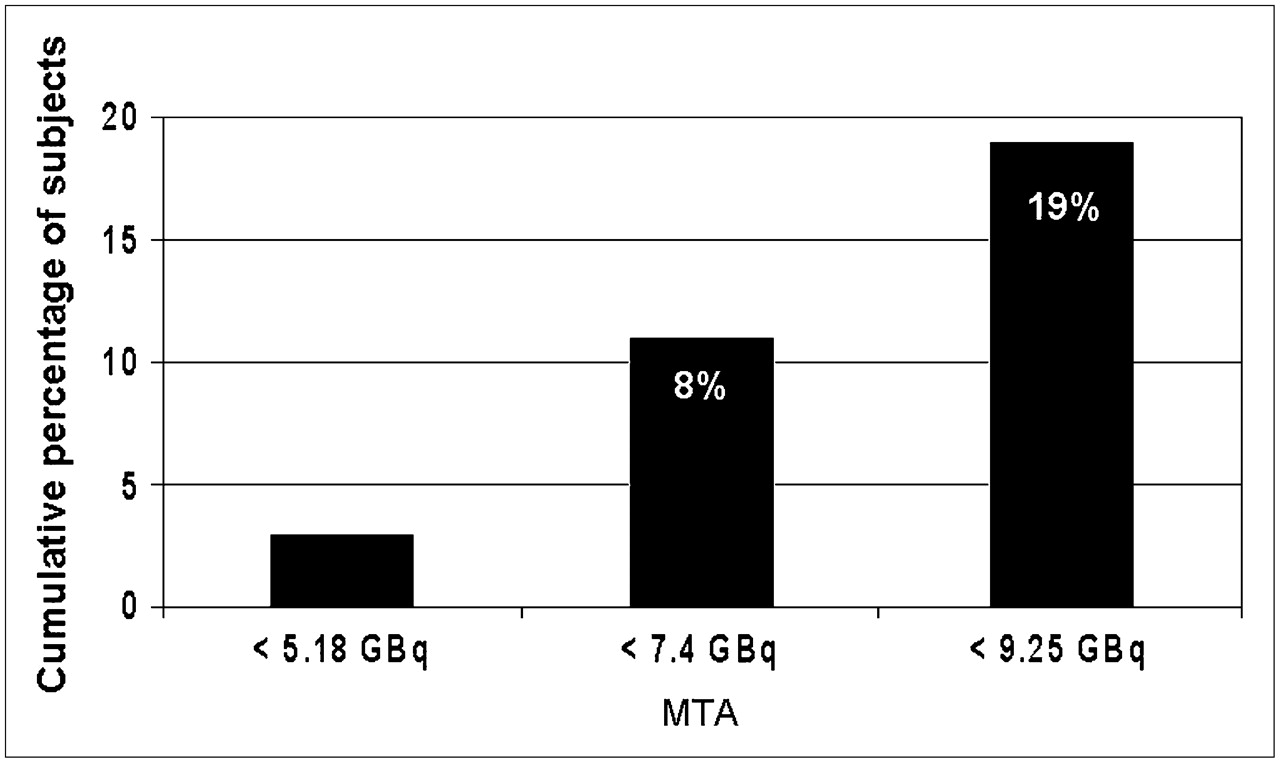
MTA cutoff points on bar graph. Three percent of patients had MTA lower than 5.18 GBq (140 mCi), 8% had MTA lower than 7.4 GBq (200 mCi), and 19% had MTA lower than 9.25 GBq (250 mCi).
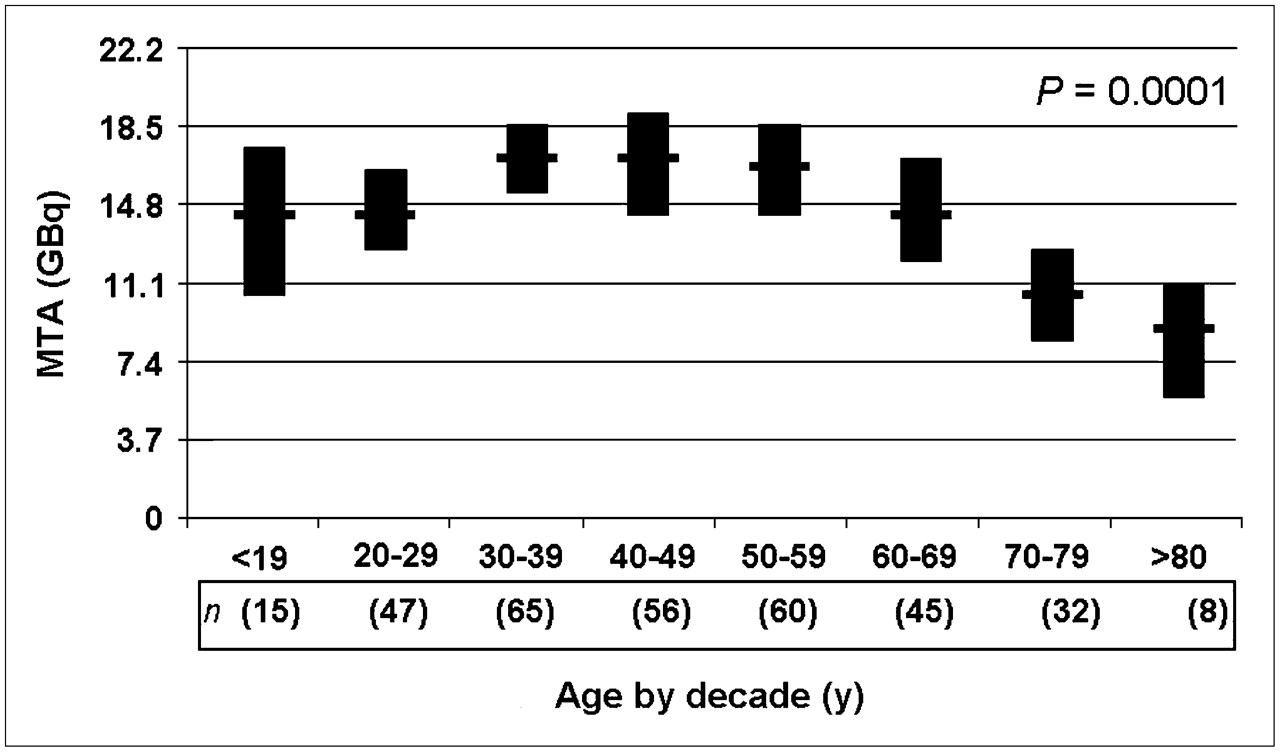
Analysis of mean MTA values with 95% confidence intervals by age at the time of dosimetry revealed little variation in the MTA up until age 70 y, when a significant decrease occurred (Fig. 3).
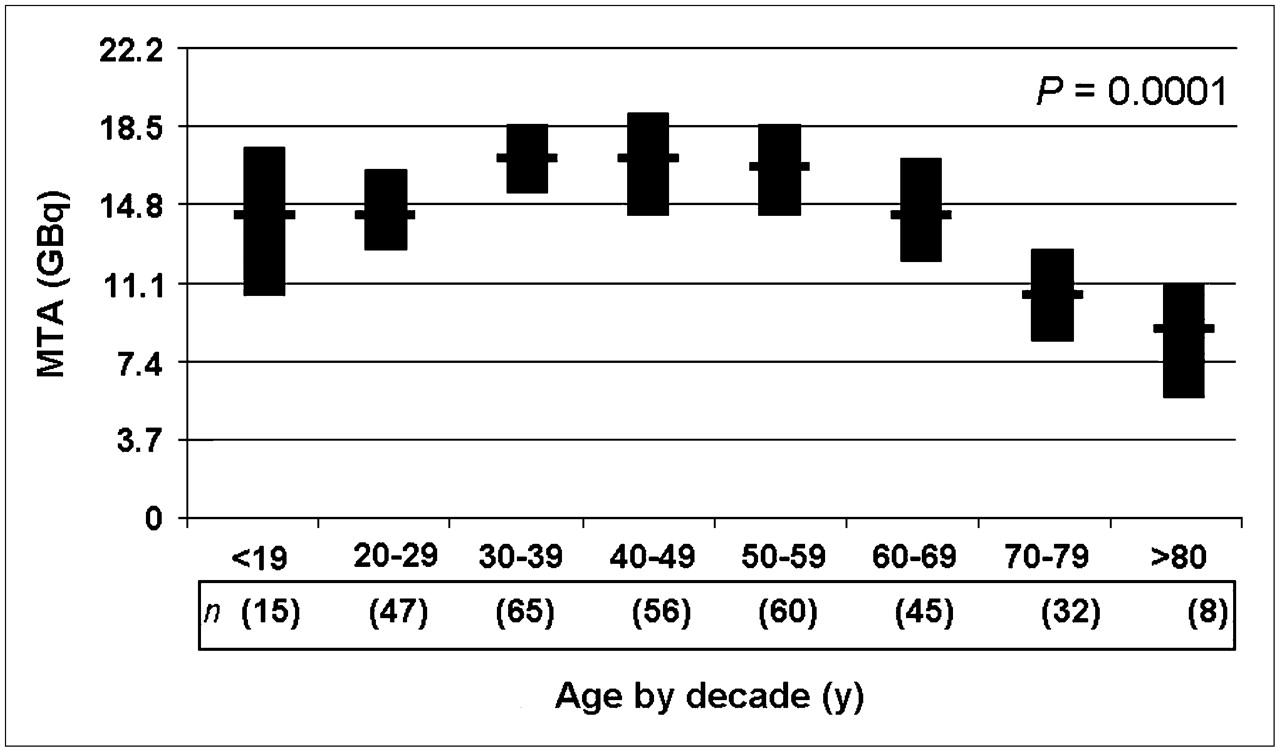
Mean MTA value (horizontal bars) according to age, with 95% confidence intervals (vertical bars). MTA showed no significant change until declining in seventh decade of life.
To better understand the impact of MTA measurements within specific age groups, we analyzed the data to demonstrate the frequency with which empiric dosing would exceed the MTA in each decade of life (Fig. 4). As expected, empiric doses of 5.18 GBq (140 mCi) exceeded the MTA in fewer than 5%−7% of patients less than 70 y old and only 13% of patients 80 y old or older at the time of dosimetry. However, an empiric dose of 7.4 GBq (200 mCi) would exceed the MTA in 8%−15% of patients less than 70 y old, 22% of patients 70–79 y old, and 38% of patients 80 y old or older. Furthermore, an empiric dose of 9.25 GBq (250 mCi) would exceed the MTA in as many as 22% of patients less than 70 y old and 50% of patients 70 y old or older at the time of dosimetry.

Percentage of patients (according to decade of life) in whom MTA exceeded empiric dosing. Empiric dose above 7.4 GBq (200 mCi) exceeded MTA in large proportion of patients more than 60 y old (14% of patients 60–69 y old and 22% of those 70–79 y old). Empiric dose of 9.25 GBq (250 mCi) would exceed MTA in 22% of patients 60–69 y old and in 50% of those 70 y old or older.
Clinical variables associated with an MTA of less than 9.25 GBq (250 mCi) included an age older than 45 y at the time of dosimetry (P = 0.009), the female sex (P = 0.05), lobectomy before dosimetry (P = 0.02), and RAI-avid pulmonary metastases in a diffuse, bilateral pattern (P = 0.03) (Table 2). Other factors analyzed that were not associated with a lower MTA included the histology of the primary tumor, the stage of disease at diagnosis, maximal TSH values, and the stimulated serum thyroglobulin level. Likewise, we did not find an association between MTA and serum creatinine values at the time of dosimetry, but as previously mentioned, patients were excluded from the study if serum creatinine at the time of dosimetry was greater than 2 mg/dL.
Percentage of Subjects with MTA less than 9.25 GBq (250 mCi)
Surprisingly, 10% and 20% of patients less than 30 y old at the time of dosimetry had MTA values of less than 7.4 and 9.25 GBq, respectively (200 and 250 mCi, respectively). A careful analysis failed to reveal any significant differences between these young patients with an MTA lower than expected and young patients with a higher MTA, other than the clinical variables described in Table 2.
DISCUSSION
Although RAI is generally a safe and effective treatment for thyroid cancer when administered at proper activities, it is important to recognize that doses exceeding 5.55−7.4 GBq (150−200 mCi) will often expose bone marrow to more than 200 cGy of radiation in older patients. It is well known that clearance of radioactive iodine is significantly impaired in patients with heart failure or renal insufficiency (20). We now add age to the list of clinical circumstances in which clearance of RAI may be lower than expected. Therefore, on the basis of our data, we would recommend that formal dosimetry studies be performed before administering more than 7.4 GBq (200 mCi) to patients more than 70 y old with RAI-avid metastatic disease, especially when the metastatic thyroid cancer is very RAI avid. Prolonged retention of RAI in large-volume RAI-avid metastatic lesions increases the whole-body exposure rate, often dramatically decreasing the maximum tolerable dose in an individual patient.
Our findings are consistent with the work by Atkins et al., who reviewed hypothyroid dosimetry studies performed on 127 patients with thyroid cancer. Using prescribed RAI activity cutoffs of 5.55 GBq (150 mCi), 7.4 GBq (200 mCi), and 9.25 GBq (250 mCi), they demonstrated that 5%, 11%, and 17%, respectively, of patients would exceed the calculated MTA (21). These results are very similar to our findings in which 3%, 8%, and 19% of patients who were prescribed similar RAI activities (5.18, 7.4, and 9.25 GBq, respectively) would exceed the MTA.
An unexpected finding was the low MTA values seen in the youngest members of our cohort. We could not identify any specific factors that correlated with these low MTAs. The tendency for young patients selected for full dosimetry to have metastatic lesions that were well differentiated and therefore very RAI avid could have resulted in prolonged RAI retention times. The lower calculated MTA for patients with diffuse RAI-avid pulmonary metastases may also have been a factor. Such influences are difficult to quantify objectively in retrospective studies. Although errors in the dosimetry methodology are possible, each patient had 2 independent dosimetry measurements: whole-body counts and blood counts. Methodologic errors would likely affect one or the other of these independent measurements but not both. Additional studies on other cohorts of young patients are needed to better define the safe MTA limits in these patients. Until additional studies are completed, dosimetry should seriously be considered for patients with RAI-avid pulmonary metastases that are visible as bilateral diffuse miliary disease, because this factor was also associated with an MTA that was lower than expected.
Not surprisingly, patients with larger thyroid remnants, such as those few patients treated with lobectomy as primary therapy for thyroid cancer who subsequently required RAI ablation without a completion thyroidectomy, also had lower MTA values than did patients undergoing total thyroidectomy. As with functional metastatic lesions (such as RAI-avid diffuse pulmonary lesions), retention of RAI by normal thyroid tissue results in slower RAI clearance from the body and a lowering of the MTA. Fortunately, relatively small doses of RAI are used in these patients to destroy the thyroid remnant; therefore, exceeding the MTA is rarely an issue.
In our cohort, MTA was not correlated with serum creatinine values of less than 2 mg/dL. Creatinine clearance values were not available in this retrospective analysis, but one would hypothesize that there would be a direct correlation between MTA and creatinine clearance if we had included patients with significant renal failure.
Because radioactive iodine dosing was guided by dosimetry in all patients in this cohort, we cannot evaluate the potential complications of exceeding the MTA in individual patients. However, based on previous studies (3), exceeding the MTA in an individual patient is likely to result in significant bone marrow depression with resultant thrombocytopenia, leukopenia, and anemia. Sialoadenitis and xerostomia are, in general, dose-related complications of RAI therapy but cannot be predicted on the basis of MTA for individual doses (22).
Even though recombinant human TSH has not yet been approved by the Food and Drug Administration for use in the United States as an adjunct to RAI remnant ablation (7,23) and therapy of distant metastases, we have noted that the dosimetry profile obtained during hypothyroid withdrawal is usually significantly different from that seen when recombinant human TSH stimulation is used during thyroid hormone suppression. In general, clearance of RAI is approximately 30% faster after recombinant human TSH preparation than after thyroid hormone withdrawal (24). Therefore, data in this article apply only to patients undergoing RAI treatment after the traditional hypothyroid withdrawal approach. More recently, a newer approach, lesion-based dosimetry, has been evaluated to more specifically quantify radiation doses to individual metastatic lesions (25,26).
CONCLUSION
To our knowledge, this study was the first to investigate the distribution of hypothyroid MTA values in a large cohort of thyroid cancer patients treated at a single institution. Administered activities of 5.18 GBq (140 mCi) or less are generally within a safe range for patients with thyroid cancer. However, administered activities above 7.4 GBq (200 mCi) will exceed the maximal safe level in a substantial number of older patients. Particular caution is needed in patients of all ages with large-volume RAI-avid disease because these patients often require multiple treatments and frequently have MTA values that would be exceeded by routine empiric doses of 7.4 GBq (200 mCi). We therefore recommend formal whole-body and blood dosimetry for patients more than 70 y old and patients with large-volume RAI-avid disease, if administration of radioiodine activity exceeding 7.4 GBq (200 mCi) is contemplated.
Footnotes
-
COPYRIGHT © 2006 by the Society of Nuclear Medicine, Inc.
References
- Received for publication May 4, 2006.
- Accepted for publication July 4, 2006.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Analysis of Residence Time, Effective Half-Life, and Internal Dosimetry Before Radioiodine Therapy
- Dosimetry in Clinical Radiopharmaceutical Therapy of Cancer: Practicality Versus Perfection in Current Practice
- Tumor Response to Radiopharmaceutical Therapies: The Knowns and the Unknowns
- Appropriate Use Criteria for Nuclear Medicine in the Evaluation and Treatment of Differentiated Thyroid Cancer
- Current Treatment Strategies in Metastasized Differentiated Thyroid Cancer
- Alternative Means of Estimating 131I Maximum Permissible Activity to Treat Thyroid Cancer
- Comparison of Empiric Versus Whole-Body/-Blood Clearance Dosimetry-Based Approach to Radioactive Iodine Treatment in Patients with Metastases from Differentiated Thyroid Cancer
- Thyroid nodules and cancer management guidelines: comparisons and controversies
- Assessment of Simplified Blood Dose Protocols for the Estimation of the Maximum Tolerable Activity in Thyroid Cancer Patients Undergoing Radioiodine Therapy Using 124I
- Radioiodine Therapy for Thyroid Cancer in the Era of Risk Stratification and Alternative Targeted Therapies
- The SNMMI Practice Guideline for Therapy of Thyroid Disease with 131I 3.0
- Reply: Differentiated Thyroid Carcinoma: Is There Any Evidence for the Use of Recombinant Human TSH in Thyroid Hormone-Secreting Metastasis?
- Thyroid Carcinoma
- Initial Management and Follow-up of Differentiated Thyroid Cancer in Children
- Complications of Radioactive Iodine Treatment of Thyroid Carcinoma
- Dosimetry and thyroid cancer: the individual dosage of radioiodine
- Blood dosimetry from a single measurement of the whole body radioiodine retention in patients with differentiated thyroid carcinoma
- 131I Effective Half-Life and Dosimetry in Thyroid Cancer Patients
- Role of Radioactive Iodine for Adjuvant Therapy and Treatment of Metastases
- Reply: Stunning Effect