


Abstract
Carvedilol and metoprolol have been reported to be effective in the treatment of patients with chronic heart failure. However, to our knowledge, there have been no studies comparing the effects of the 2 drugs on cardiac function, including cardiac sympathetic nerve activity. Methods: We compared 15 patients with dilated cardiomyopathy (DCM) who were receiving carvedilol (group A) with 15 patients with DCM who were receiving metoprolol (group B). Before and after 1 y of treatment, cardiac 123I-metaiodobenzylguanidine (123I-MIBG) uptake was assessed using the total defect score (TDS) and the heart-to-mediastinum (H/M) activity ratio from the delayed images. The New York Heart Association (NYHA) class and echocardiographic left ventricular ejection fraction (LVEF) also were assessed. Results: In both groups, the TDS decreased (in group A, from 25 ± 14 to 16 ± 14, P < 0.01; in group B, from 27 ± 9 to 19 ± 10, P < 0.01), the H/M increased (in group A, from 1.67 ± 0.31 to 2.01 ± 0.36, P < 0.01; in group B, from 1.68 ± 0.21 to 1.93 ± 0.32, P < 0.01), the LVEF increased (in group A, from 31% ± 10% to 48% ± 10%, P < 0.01; in group B, from 28% ± 9% to 47% ± 15%, P < 0.01), and the NYHA functional class improved (in group A, from 2.9 ± 0.3 to 1.7 ± 0.5, P < 0.01; in group B, from 2.8 ± 0.6 to 1.7 ± 0.6, P < 0.01). The change in LVEF was mildly correlated with the change in the TDS in group A (r = 0.41) as well as in group B (r = 0.53). In the patients with a favorable response in the TDS or H/M, the NYHA class improved more than in the patients without a favorable response (P < 0.05). Conclusion: Carvedilol treatment can improve cardiac function, symptoms, and cardiac sympathetic nerve activity in patients with DCM to a similar extent as metoprolol treatment. The improvement of cardiac function and symptoms is related to the improvement of cardiac sympathetic nerve activity.
The prognosis of patients with idiopathic dilated cardiomyopathy (DCM) remains poor. Activation of the sympathetic nervous system is one of the cardinal pathophysiologic abnormalities in patients with chronic heart failure (1). Studies performed in Sweden in the 1970s suggested that long-term therapy with β-blockers might produce hemodynamic and clinical benefits (2). Subsequent controlled clinical trials have shown that β-blockers produce consistent benefits in patients with chronic heart failure (3–6). Trials using bisoprolol (3), metoprolol (4), and carvedilol (5,6) have demonstrated a decrease in the number of cardiac deaths due to heart failure and improvement of the left ventricular ejection fraction (LVEF) in patients with chronic heart failure (2–6). Only 1 trial using bucindolol has not been able to demonstrate a beneficial effect of β-blockers (7). Recently, comparisons between metoprolol and carvedilol therapy have been reported (8–10). Carvedilol improves cardiac performance to the same (9) or greater (10,11) extent than metoprolol when given to patients with heart failure. However, to our knowledge, there have been no comparison studies between the 2 drugs with respect to their effect on cardiac function, including cardiac sympathetic nerve activity.
123I-Metaiodobenzylguanidine (123I-MIBG) imaging has been used to study cardiac sympathetic nerve activity. Cardiac 123I-MIBG uptake is altered in patients with DCM (12,13). The cardiac uptake of 123I-MIBG and LVEF are correlated (12,13), and 123I-MIBG imaging can be a useful prognostic test in patients with DCM (13). This study was undertaken to determine the effect of carvedilol treatment on cardiac symptoms, function, and sympathetic nerve activity in patients with DCM compared with metoprolol treatment.
MATERIALS AND METHODS
Study Population
Thirty consecutive patients (7 women, 23 men; mean age, 59 ± 12 y; range, 28–79 y) with DCM were placed on treatments with either carvedilol or metoprolol in addition to conventional heart failure therapy, which included digitalis, diuretics, and angiotensin-converting enzyme inhibitors or angiotensin II blockers. All patients had experienced at least 1 episode of heart failure requiring short-term hospitalization. All patients were symptomatic at the start of treatment with carvedilol or metoprolol. Patients were in New York Heart Association (NYHA) functional classes II to IV and had an echocardiographic LVEF of ≤45%. Fifteen patients (3 women, 12 men; mean age, 60 ± 10 y) were treated with carvedilol and 15 patients (4 women, 11 men; mean age, 58 ± 14 y) were treated with metoprolol. Patients were assigned randomly to the groups. All patients gave informed consent in accordance with the guidelines of our hospital’s Human Clinical Study Committee before participation in the study.
Coronary angiography revealed normal coronary arteries in all of the patients. The presence of acute or chronic myocarditis was excluded in all of the patients based on the findings of left ventricular endomyocardial biopsy. None of the patients had abused alcohol. Moreover, none of the patients had congenital heart disease, valvular heart disease, or hypertensive heart disease.
Study Protocol
In patients receiving carvedilol, the initial dose was 1.25–2.5 mg/d. Three to 5 mo later, the dose increased to the maintenance dose of 10–20 mg/d. In patients receiving metoprolol, the initial dose was 2.5–5 mg/d. Three to 5 mo later, the dose increased to the maintenance dose of 30–60 mg/d. We performed a series of examinations before and after 1 y of treatment.
123I-MIBG and 99mTc-MIBI Imaging
The 123I-MIBG and 99mTc-methoxyisobutylisonitrile (99mTc-MIBI) were obtained commercially (Daiichi Radioisotope Laboratories). The patients were injected intravenously with 111 MBq 123I-MIBG while in an upright position. Anterior planar and SPECT images were acquired 15 min after injection and repeated 4 h later. SPECT imaging was performed using a dedicated 3-detector imaging system (PRISM 3000; Picker International). The detectors were constantly corrected for energy, uniformity, and linearity. Projection images were acquired for 55 s in 5° increments over 360° orbits and were recorded at a digital resolution of 64 × 64. Immediately after this acquisition, the patients were injected with 720 MBq 99mTc-MIBI while in an upright position and imaged 30 min later. 99mTc-MIBI SPECT images were acquired for 50 s in 5° increments over 360° orbits. Energy discrimination was provided by a 20% window around the 159-eV photopeak of 123I and a 15% window around the 140-eV photopeak of 99mTc-MIBI.
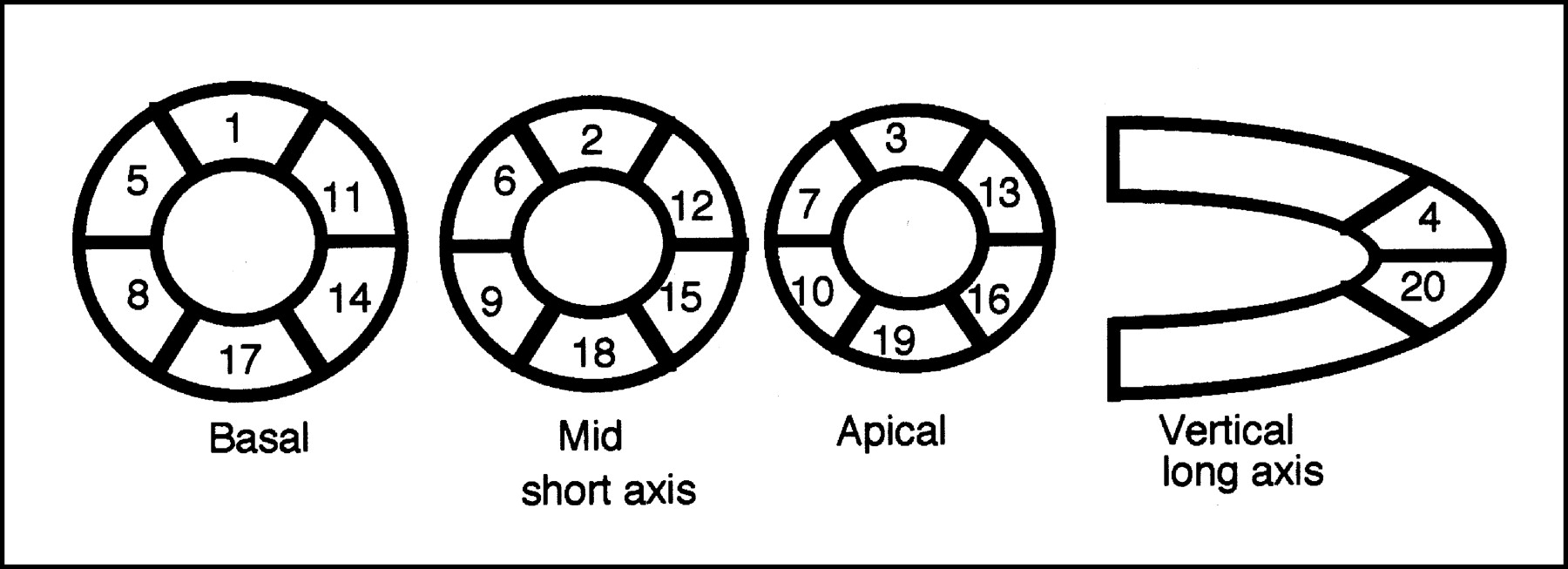
Using the anterior planar delayed 123I-MIBG images, the heart-to-mediastinum (H/M) activity ratio was obtained using regions of interest positioned over the heart (H) and over the upper mediastinum (M). The washout rate was calculated using the formula: (H − M)early − (H − M)delayed/(H − M)early × 100. The myocardial SPECT image set of each patient was divided into 20 segments (Fig. 1). The short-axis images at the basal, middle, and apical ventricular levels were divided into 6 segments each. The apical segment of the vertical long-axis image was divided into 2 segments. Regional tracer uptake was scored semiquantitatively using a 4-point scoring system (0 = normal uptake; 1 = mildly reduced uptake; 2 = moderately reduced uptake; 3 = severely reduced uptake). The total defect score (TDS) was calculated as the sum of the scores for all 20 segments.
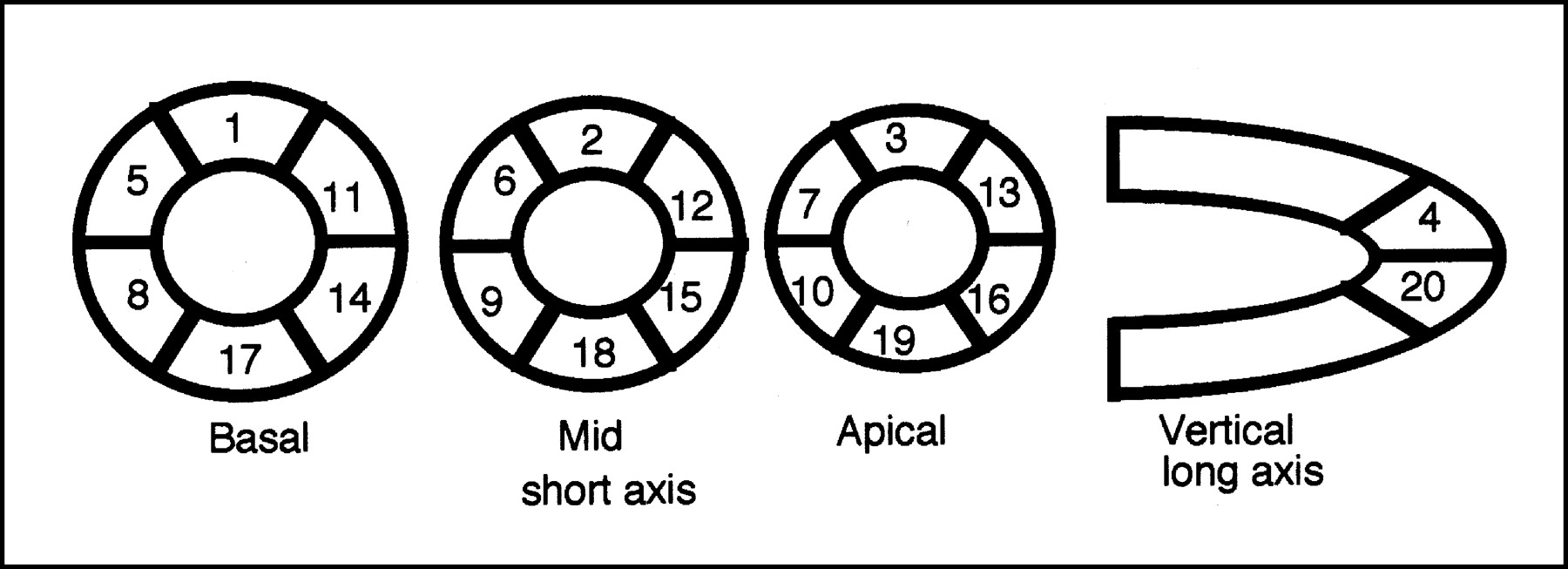
Diagram of segmentation scheme used to assess regional 123I-MIBG and 99mTc-MIBI uptake.
M-Mode Echocardiography
Echocardiographic measurements were performed using standard methods (14). Left ventricular end-diastolic and end-systolic diameters were determined and the LVEF was calculated by the method of Teicholz et al. (15).
Cardiac Symptoms
Cardiac symptoms were scored using the NYHA functional classification.
Data Analysis and Statistics
Statistical analysis was performed with Statview (Hulinks) run on a Macintosh computer (Apple Computers). Specific comparisons of parameters were performed using paired 2-tailed t tests. Unpaired 2-tailed t tests were used to make comparisons between the carvedilol and metoprolol groups and patients with and without a favorable response in the TDS or H/M. All values are expressed as the mean ± SD. Significant differences were defined by P < 0.05.
RESULTS
The TDSs for the delayed 123I-MIBG images are summarized in Table 1. In patients receiving carvedilol, the TDS decreased significantly after 1 y of treatment (16 ± 14) compared with the baseline value (25 ± 14, P < 0.01). In patients receiving metoprolol, the TDS also decreased significantly after 1 y of treatment (19 ± 10) compared with the baseline value (27 ± 9, P < 0.01). The TDS for the 99mTc-MIBI images also changed significantly in both groups. In patients receiving carvedilol treatment, the TDS changed from 6 ± 5 to 3 ± 5 (P < 0.01). In patients receiving metoprolol, the TDS also changed from 9 ± 4 to 5 ± 6 (P < 0.01).
123I-MIBG and 99mTc-MIBI Data
The H/M ratios for the delayed 123I-MIBG images are summarized in Table 1. In patients receiving carvedilol, the H/M increased significantly after 1 y of treatment (2.01 ± 0.36) compared with the baseline value (1.67 ± 0.31, P < 0.01). In patients receiving metoprolol, the H/M also increased significantly after 1 y of treatment (1.93 ± 0.32) compared with the baseline value (1.68 ± 0.21, P < 0.01). In patients receiving carvedilol, the washout rate for the 123I-MIBG image decreased significantly after 1 y of treatment (36% ± 16%) compared with the baseline value (47% ± 15%, P < 0.01). In patients receiving metoprolol, the washout rate also decreased significantly after 1 y of treatment (37% ± 11%) compared with the baseline value (51% ± 10%, P < 0.01; Table 1).
The left ventricular end-diastolic and end-systolic diameters and the LVEF at baseline were compared with the values after 1 y of treatment. In patients receiving carvedilol, the end-diastolic diameter decreased significantly after 1 y of treatment (55 ± 7 mm) compared with the baseline value (64 ± 8 mm, P < 0.01). In patients receiving metoprolol, the end-diastolic diameter also decreased significantly after 1 y of treatment (58 ± 7 mm) compared with the baseline value (65 ± 7 mm, P < 0.01; Table 2). In patients receiving carvedilol, the end-systolic diameter decreased significantly after 1 y of treatment (42 ± 7 mm) compared with the baseline value (54 ± 9 mm, P < 0.01). In patients receiving metoprolol, the end-systolic diameter also decreased significantly after 1 y of treatment (44 ± 10 mm) compared with the baseline value (57 ± 8 mm, P < 0.01; Table 2).
Echocardiographic and NYHA Data
In patients receiving carvedilol, the LVEF increased significantly after 1 y of treatment (48% ± 10%) compared with the baseline value (31% ± 10%, P < 0.01). In patients receiving metoprolol, the LVEF also increased significantly after 1 y of treatment (47% ± 15%) compared with the baseline value (28% ± 9%, P < 0.01; Table 2). The NYHA functional class of the patients is summarized in Table 2. Patients treated with carvedilol showed an improvement of functional class after 1 y of treatment compared with the baseline value (P < 0.01). The functional status of patients receiving metoprolol also improved after 1 y of treatment (P < 0.01).
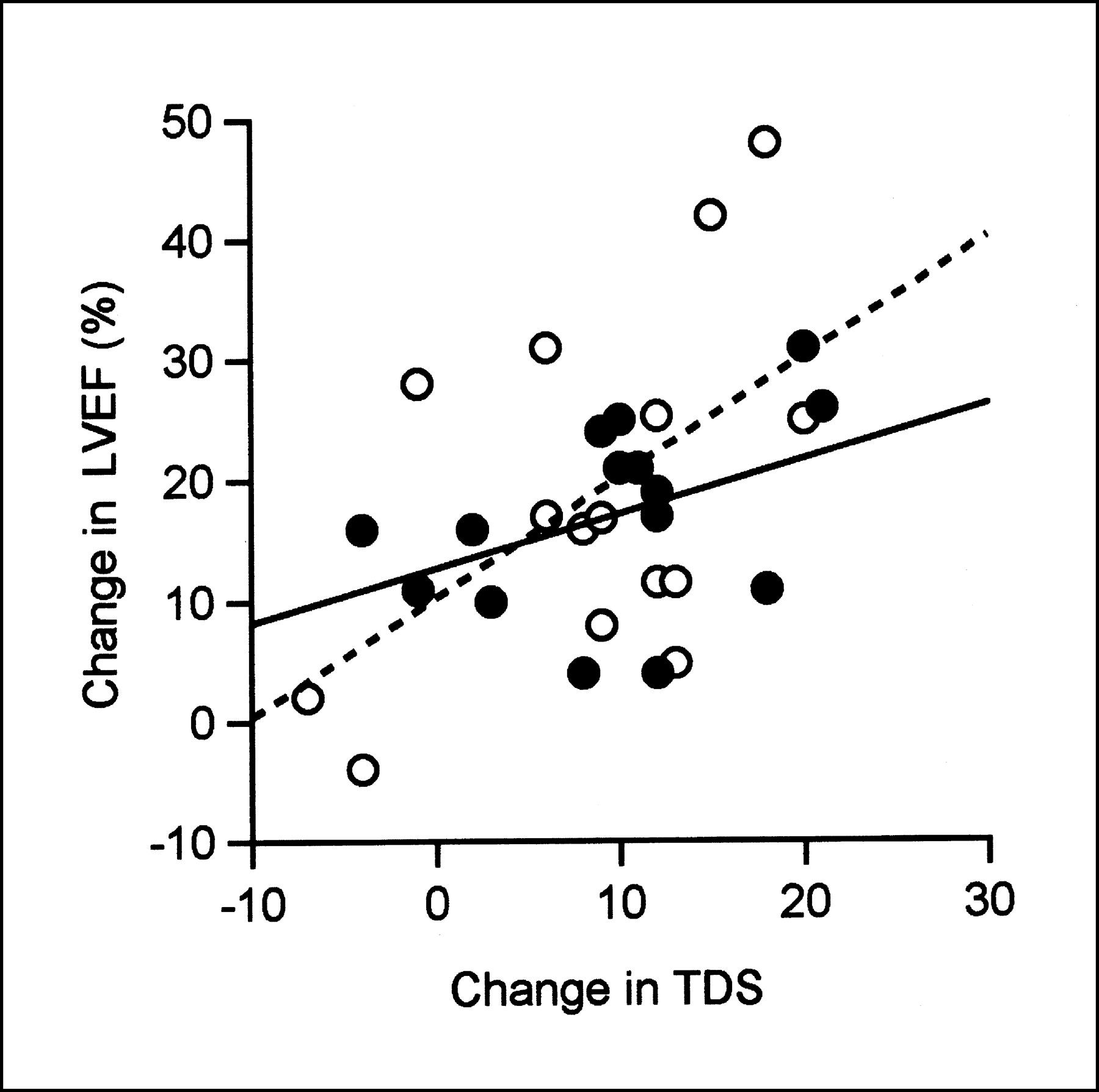
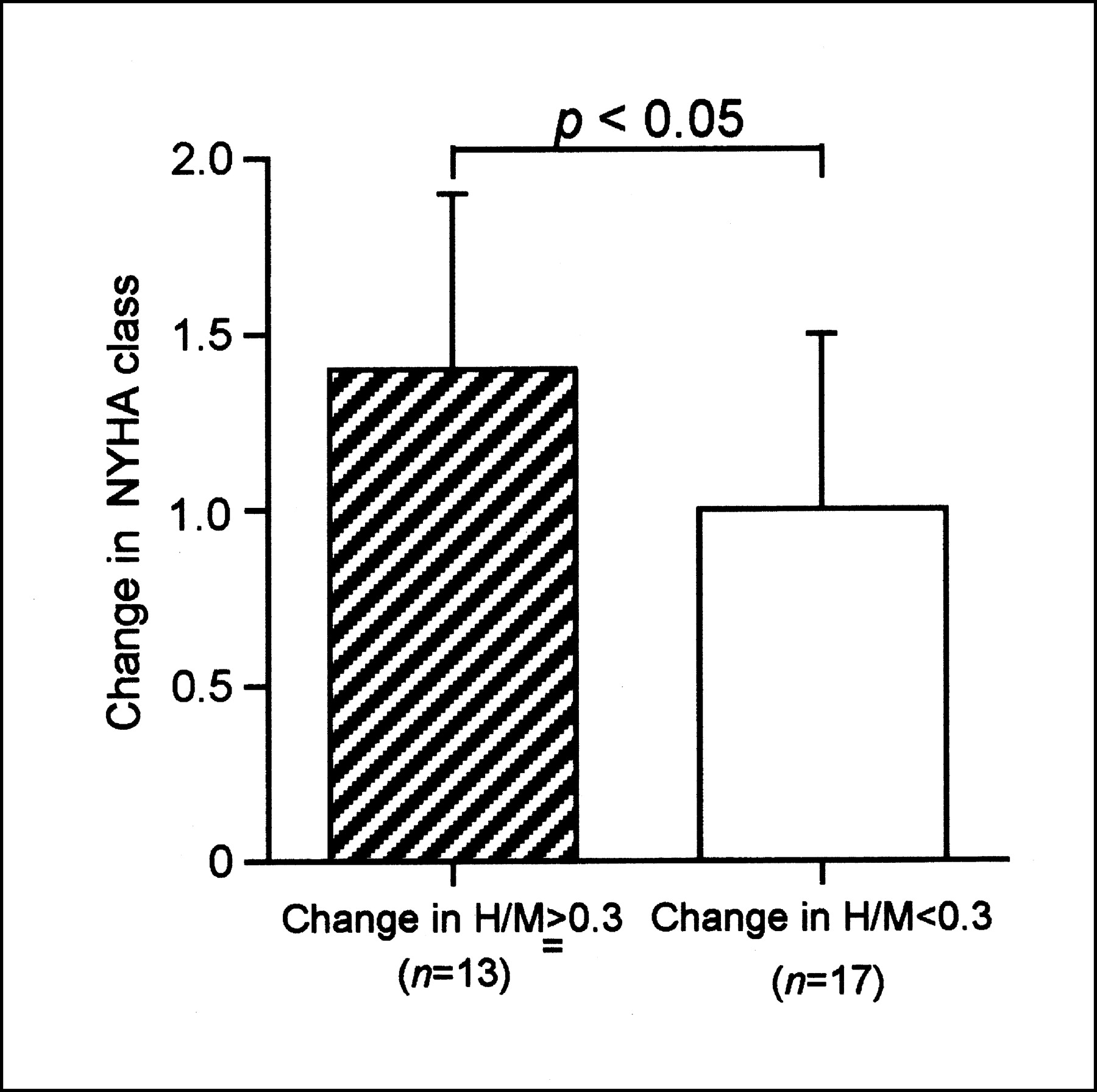
The change in LVEF was mildly correlated with the change in TDS in patients receiving carvedilol (r = 0.41) and in patients receiving metoprolol (r = 0.53; Fig. 2). However, the change in LVEF was not correlated with the change in H/M in both groups (r = 0.06 in patients receiving metoprolol and r = 0.18 in patients receiving carvedilol; Fig. 3). In the patients of the combined group with a favorable response of the TDS that was ≥10, the NYHA functional class improved more than in the patients without a favorable response (P < 0.05; Fig. 4). Moreover, in the patients of the combined group with a favorable response of the H/M that was ≥0.3, the NYHA functional class also improved more (P < 0.05; Fig. 5).

Correlation between change in LVEF and TDS. There were mild correlations in patients receiving metoprolol (r = 0.53) and carvedilol (r = 0.41). ○, Patients receiving metoprolol; •, patients receiving carvedilol.
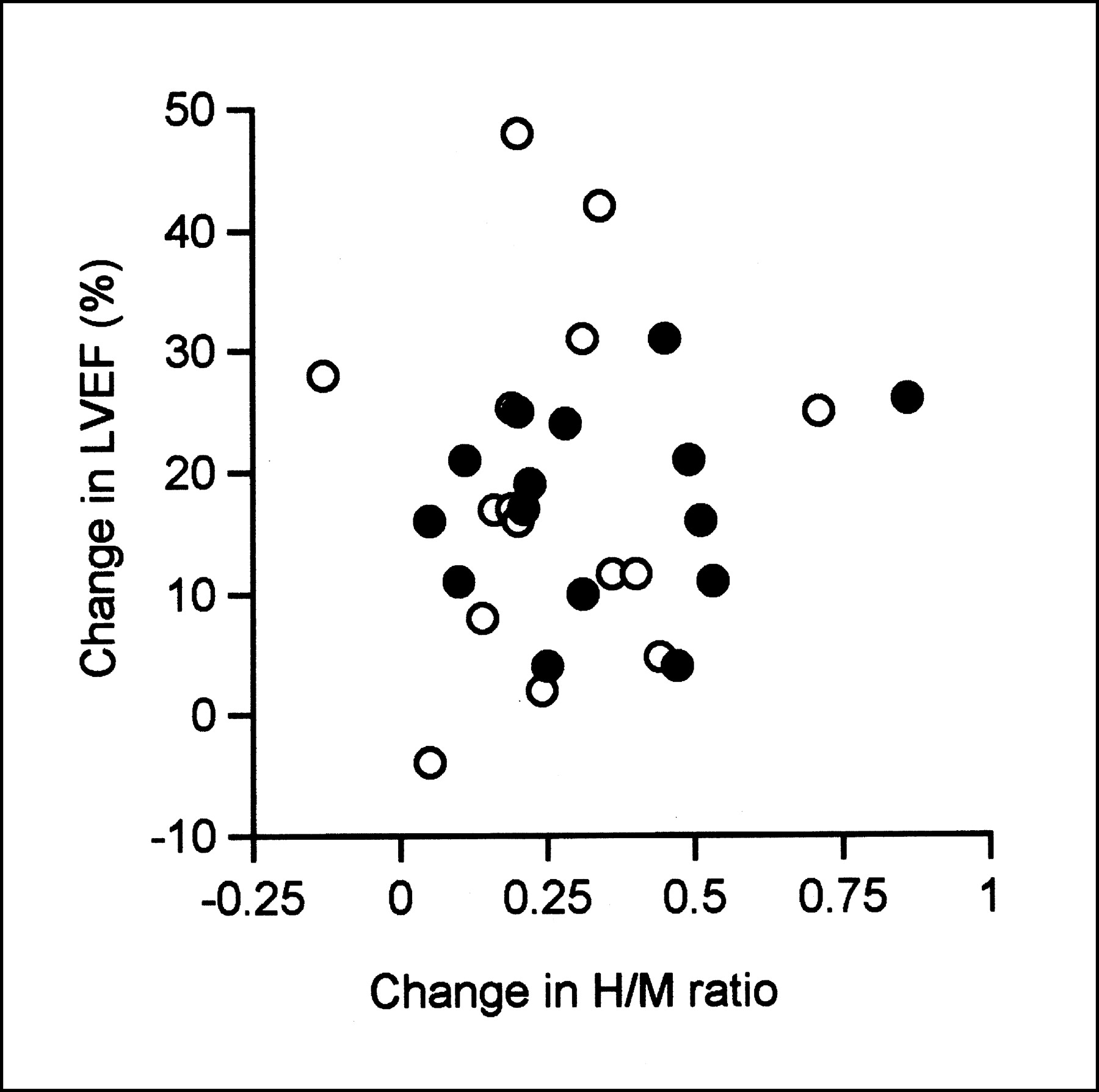
Relationship between change in LVEF and H/M. There were no significant relationships in patients receiving metoprolol and carvedilol. ○, Patients receiving metoprolol; •, patients receiving carvedilol.

Comparison between patients with favorable response and without favorable response in TDS. Favorable response means improvement of TDS ≥10 after β-blocker treatments. Improvement of LVEF in patients with favorable response was higher than that in patients without favorable response (P < 0.05).
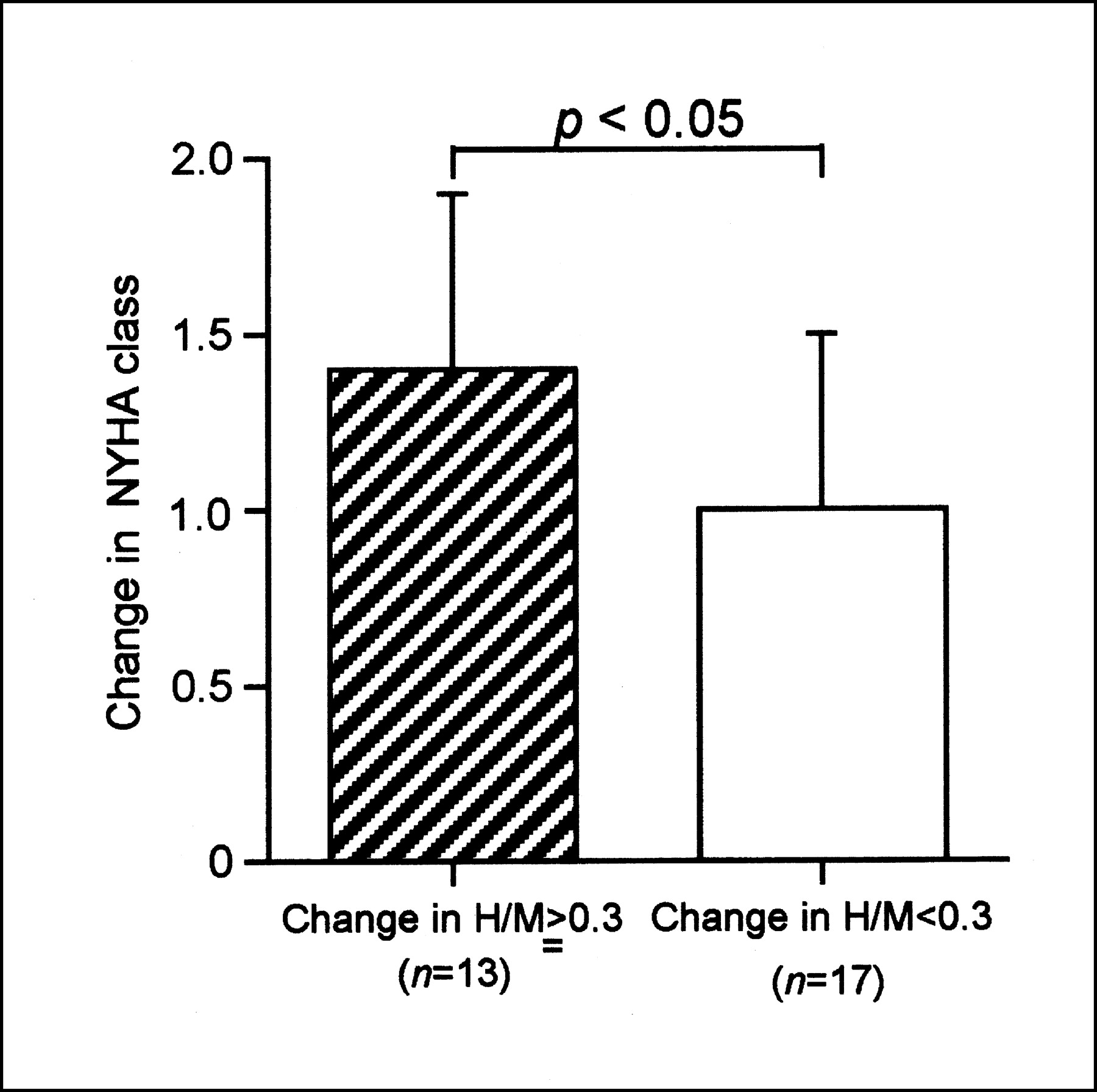
Comparison between patients with favorable response and without favorable response in H/M. Favorable response means improvement of H/M ≥0.3 after β-blocker treatments. Improvement of LVEF in patients with favorable response was higher than that in patients without favorable response (P < 0.05).
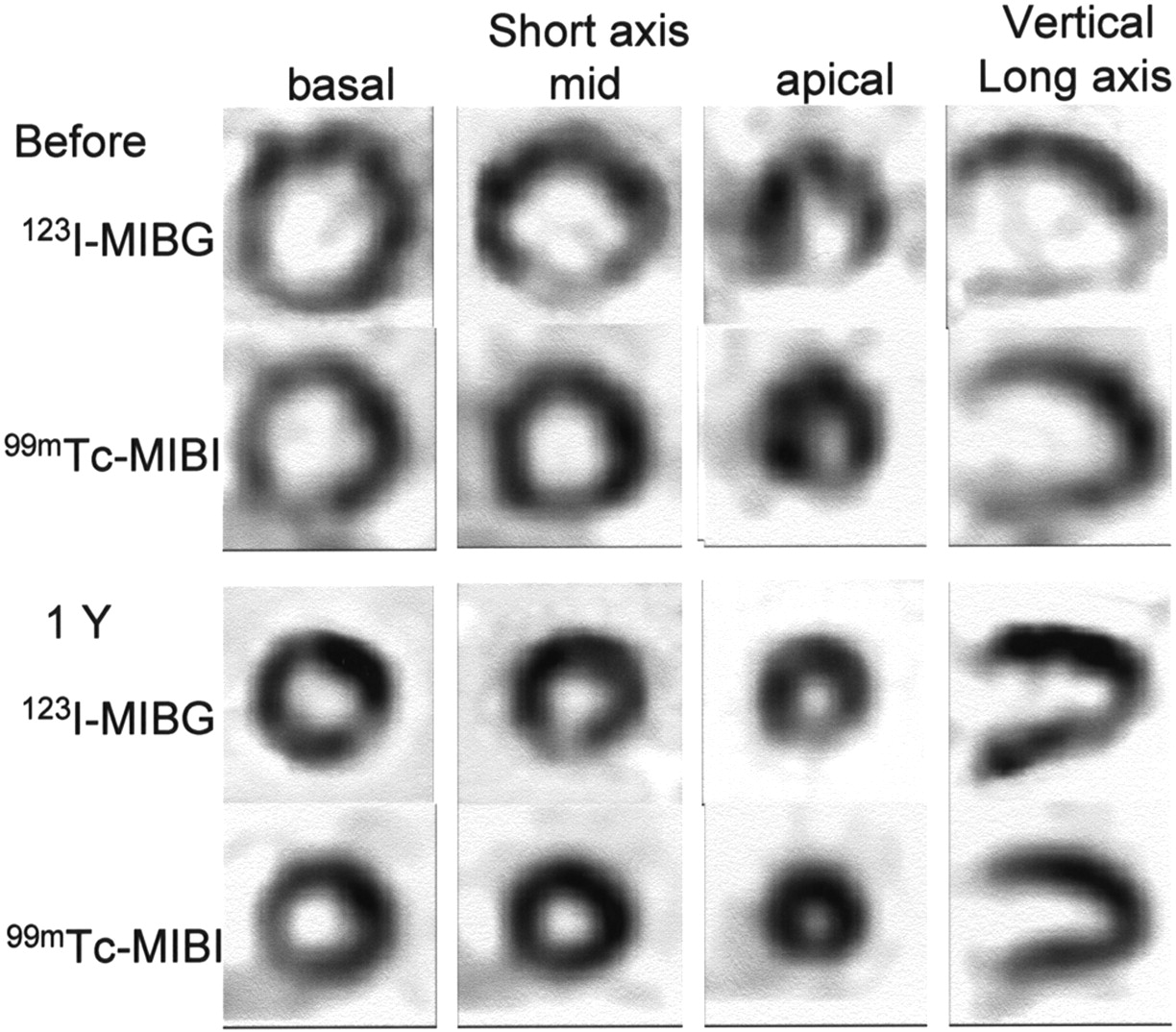
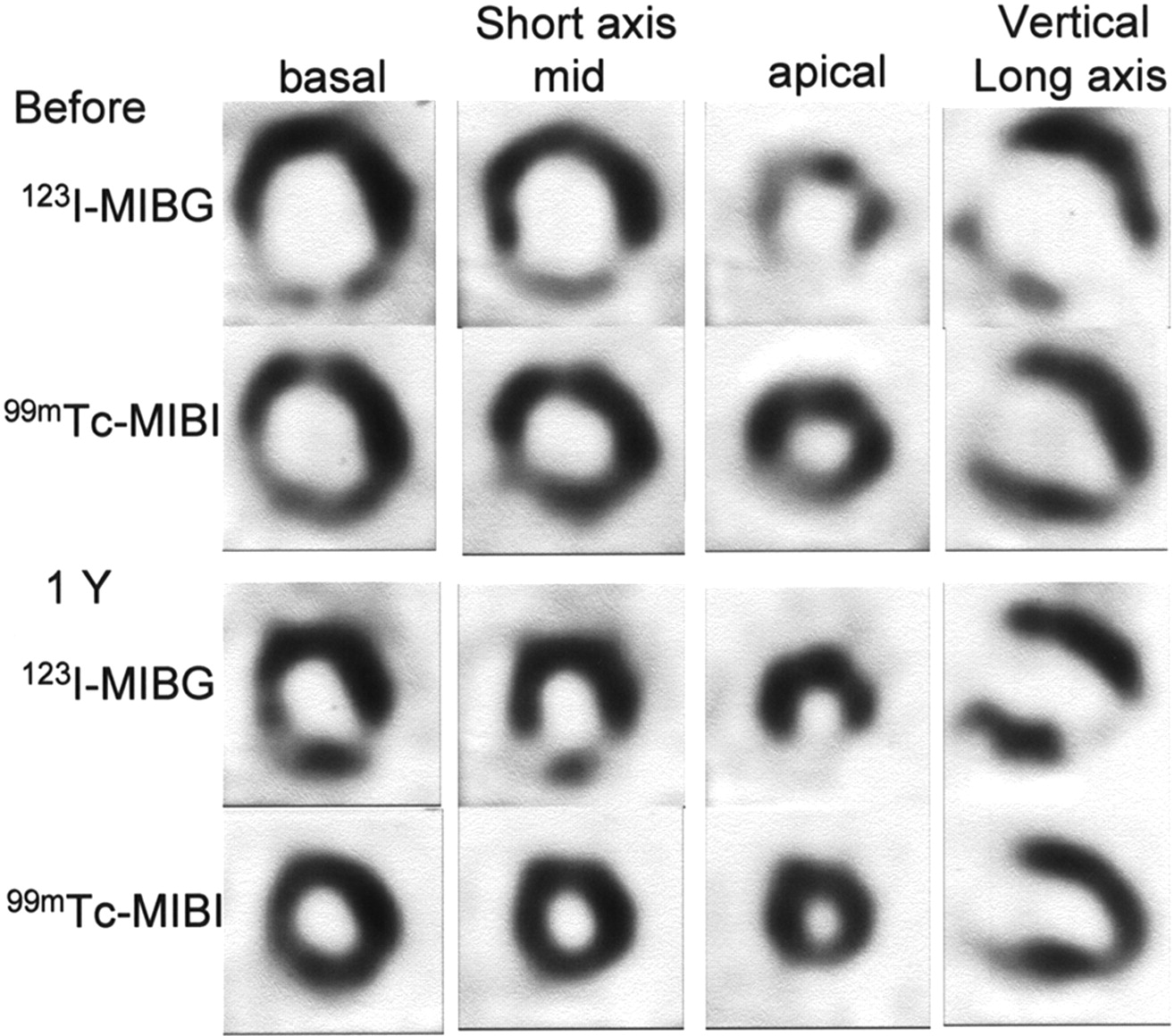
Figure 6 shows an example of the 123I-MIBG and 99mTc-MIBI uptake after metoprolol treatment. The H/M increased from 1.69 to 2.03 and the LVEF increased from 16% to 58% after metoprolol treatment. Figure 7 shows an example of the 123I-MIBG and 99mTc-MIBI uptake after carvedilol treatment. The H/M increased from 1.68 to 2.19 and the LVEF increased from 33% to 60% after carvedilol treatment.

Representative case of metoprolol treatment. 123I-MIBG and 99mTc-MIBI images were obtained from short-axis and vertical long-axis reconstructions.
Representative case of carvedilol treatment. 123I-MIBG and 99mTc-MIBI images were obtained from short-axis and vertical long-axis reconstructions.
DISCUSSION
Myocardial scintigraphy with 123I-MIBG, an analog of norepinephrine, has been reported to provide images that reflect cardiac sympathetic nerve function (12,13). 123I-MIBG uptake is considered to be useful for the evaluation of the severity of heart failure. In addition, the H/M and TDS correlate with the LVEF. 123I-MIBG can also be used to determine prognosis and evaluate therapeutic efficacy (13).
The mechanism of beneficial action of β-blockers in the setting of DCM includes the following: (a) increased myocardial energy that is available for synthetic and reparative processes; (b) improved diastolic relaxation, filling, and compliance; (c) inhibition of sympathetically mediated vasoconstriction via prostaglandin and renin release; (d) protection against catecholamine-induced myocardial damage and necrosis; and (e) upregulation of β-adrenergic receptors, allowing for restoration of catecholamine responsiveness (16–18). Recently, it has been reported that β-blockers enhance the expression of β-adrenergic receptor kinase and reduce the expression of β1-receptors (19). β-Blockers also have hemodynamic and energetic benefits (20) and enhance cell-mediated immunity and improve T-cell function (21).
Several large-scale trials using bisoprolol (3), metoprolol (4), carvedilol (5,6), or bucindolol (7) have been performed in patients with chronic heart failure. Although the bucindolol trial did not demonstrate a favorable effect of treatment on survival, the other trials demonstrated a reduction in the risk of death as well as the risk of hospitalization for cardiovascular causes in patients with chronic heart failure.
The basic biologic action of the third-generation β-blocker carvedilol differs considerably from that of the second-generation β-blocker metoprolol. Compared with metoprolol, which is a β1-selective blocking agent, carvedilol is a relatively nonselective β-blocking agent (22,23), blocks α1-receptors (22,24–26), and has important antioxidant properties (27). Metoprolol treatment increases cardiac β-receptor density, whereas carvedilol does not change cardiac β-receptor expression (11), suggesting that carvedilol allows cardiac function to recover without upregulation of β-adrenergic receptors. Cargnoni et al. showed that the antioxidant activity of carvedilol improves the ratio of reduced glutathione to oxidized glutathione and that the antioxidant effect helps to maintain myocardial viability (28). Rossig et al. reported that carvedilol inhibits endothelial cell apoptosis through its antioxidant effect and that this action might contribute to the beneficial effects of carvedilol in patients with heart failure (29).
On the basis of these pharmacologic differences between carvedilol and metoprolol, there have been comparisons between the 2 drugs in patients with chronic heart failure. Gilbert et al. reported that carvedilol, but not metoprolol, increases the LVEF compared with a placebo (11). However, in that study, the carvedilol placebo did not increase the LVEF, whereas the metoprolol placebo increased the LVEF. Metra et al. also reported that the improvement of the LVEF in the carvedilol group was greater than that in the metoprolol group (10). In contrast, Kukin et al. reported that carvedilol and metoprolol had similar beneficial effects on the LVEF in patients with chronic heart failure (9).
In our study, metoprolol and carvedilol had similar effects on the left ventricular end-diastolic diameter, end-systolic diameter, LVEF, and NYHA functional class. These results are similar to those of Kukin et al. (9). Furthermore, we were able to demonstrate that the improvement of the TDS, H/M, and washout rate in the carvedilol treatment group was the same as that in the metoprolol treatment group 1 y after initiation of treatment. These results suggest that metoprolol improves cardiac sympathetic nerve activity through upregulation of β-adrenergic receptors, whereas carvedilol improves cardiac sympathetic nerve activity without upregulation of β-adrenergic receptors. On the basis of our findings, carvedilol treatment can improve cardiac function, symptoms, and sympathetic nerve activity in patients with DCM. Furthermore, the efficacy of carvedilol treatment for patients with DCM is similar to that of metoprolol treatment.
On the relationship between improvement of cardiac function and cardiac sympathetic nerve activity, the improvement of the LVEF was mildly correlated with the improvement of the TDS in both groups. However, the change in the LVEF was not correlated with the change in the H/M in both groups. The reason may be that the improvement of sympathetic nerve activity after β-blocker treatments might be emphasized on the SPECT images because of the decrease of the left ventricular end-diastolic and end-systolic diameters.
In the patients of the combined group with a favorable response of the TDS or the H/M, the NYHA functional class also was more improved. After β-blocker treatment of either carvedilol or metoprolol, cardiac function, symptoms, and cardiac sympathetic nerve activity estimated by the 123I-MIBG images improved. However, the relationship between the improvement of cardiac function and cardiac sympathetic nerve activity was not always good. These findings means that the improvement of the cardiac sympathetic nerve activity and the improvement of cardiac function and symptoms do not always change in parallel. There are individual differences in these improvement factors. In this study, it seemed to be difficult to see the correlation because the number of patients was few and the number of serious patients of NYHA functional class IV was very few. Gerson et al., in a study of 22 congestive heart failure patients treated with carvedilol, noted no significant relationship between the baseline 123I-MIBG H/M and improvement of the LVEF (30).
On the other hand, myocardial perfusion estimated using 99mTc-MIBI improved after both β-blocker treatments. However, Bennett et al. reported recently that they measured the absolute myocardial blood flow in patients with DCM and found no significant change in the regional blood flow before and after metoprolol treatment (31). Our data that myocardial perfusion improved after β-blocker treatments may be relative improvement on the images due to the decrease of the left ventricular end-diastolic and end-systolic diameters. On the images, the 123I-MIBG uptake improved much more than the 99mTc-MIBI uptake.
Two limitations of our study must be considered. First, because of the small number of patients in this study, it was difficult to identify differences between carvedilol and metoprolol therapy. Second, the dose of both β-blockers was relatively low. In the future, we need to study the long-term effects of these agents and to compare these medicines in a large number of patients.
CONCLUSION
The effects of carvedilol in the treatment of patients with DCM are similar to those of metoprolol treatment with respect to improvements in cardiac function, symptoms, and sympathetic nerve activity. The improvement of cardiac function and symptoms is related to the improvement of cardiac sympathetic nerve activity.
Footnotes
Received Dec. 30, 2002; revision accepted Jun. 13, 2003.
For correspondence or reprints contact: Takuji Toyama, MD, Gunma Prefectural Cardiovascular Center, 3-12, Kameizumi-machi, Maebashi, Gunma, 371-0004, Japan.
E-mail: toyama.t{at}cvc.pref.gunma.jp
REFERENCES
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Comparative effects of long-acting and short-acting loop diuretics on cardiac sympathetic nerve activity in patients with chronic heart failure
- A Pooled Analysis of Multicenter Cohort Studies of 123I-mIBG Imaging of Sympathetic Innervation for Assessment of Long-Term Prognosis in Heart Failure
- {beta}-Adrenoceptor Blockers Increase Cardiac Sympathetic Innervation by Inhibiting Autoreceptor Suppression of Axon Growth
- Prognostic Value of Serial Cardiac 123I-MIBG Imaging in Patients with Stabilized Chronic Heart Failure and Reduced Left Ventricular Ejection Fraction
- Additive Effects of Spironolactone and Candesartan on Cardiac Sympathetic Nerve Activity and Left Ventricular Remodeling in Patients with Congestive Heart Failure
- Effects of torasemide on cardiac sympathetic nerve activity and left ventricular remodelling in patients with congestive heart failure
- Effects of Carvedilol on Myocardial Sympathetic Innervation in Patients with Chronic Heart Failure
- Effects of candesartan on cardiac sympathetic nerve activity in patients with congestive heart failure and preserved left ventricular ejection fraction