


Abstract
Sympathetic nerves play key roles in cardiac physiology and aging-related cardiovascular diseases. This study examined the effects of normal human aging on cardiac sympathetic innervation and function, including the neuronal uptake of catecholamines (uptake 1) via the cell membrane norepinephrine transporter. Methods: Thirty-three healthy volunteers, 17 under 40 and 16 over 50 y old, underwent thoracic PET scanning after injection of the sympathoneural imaging agent 6-18F-fluorodopamine. Myocardial perfusion was estimated by 13NH3 scanning, and arterial blood was sampled for levels of 6-18F-fluorodopamine and 6-18F-fluorodopamine-derived radioactivity. Results: The older group had more myocardial 6-18F-fluorodopamine-derived radioactivity than did the younger group. Myocardial perfusion was also greater in the older group, and arterial blood levels of 6-18F-fluorodopamine were also higher. After adjustment for delivery of the tracer, the estimated level of myocardial extraction of 6-18F-fluorodopamine was lower in the older group (48%) than in the younger group (74%) (P = 0.02). Conclusion: Cardiac uptake 1 activity decreases with normal human aging.
Sympathetic nerves in the heart play key roles in cardiovascular physiology and pathophysiology. Increased entry of the sympathetic neurotransmitter norepinephrine into the venous drainage of the heart (cardiac norepinephrine spillover) occurs during normal aging (1) and also in association with several common disorders, such as hypertension (2), ventricular arrhythmias (3), and congestive heart failure (4), consistent with increased delivery of norepinephrine to adrenoceptors on myocardial cells.
In humans, most of the norepinephrine released from sympathetic nerves in the human heart is inactivated by the neuronal uptake of catecholamines (uptake 1) (5) via the cell membrane norepinephrine transporter. Neurochemical findings have suggested that decreased uptake 1 activity may contribute to the increased cardiac norepinephrine spillover associated with aging (1) as well as that attending hypertension (6) and congestive heart failure (7,8).
The results of studies with 123I-metaiodobenzylguanidine scanning for cardiac sympathetic neuroimaging generally have agreed with the notion of an aging-related decline in cardiac uptake 1 activity (9–11). Although 123I-metaiodobenzylguanidine scanning can provide an anatomic depiction of cardiac sympathetic innervation, this approach has unclear validity for the quantitative evaluation of specific aspects of sympathetic function, such as the vesicular monoamine transporter, vesicular leakage, monoamine oxidase, postganglionic sympathetic nerve traffic, norepinephrine synthesis and turnover, and uptake 1.
Physiologic approaches, such as power spectral analysis of heart rate variability, have no specificity in this regard, and inferences based on such analyses about the effects of normal aging have disagreed with those based on cardiac norepinephrine spillover (1,12).
PET scanning after injection of 6-18F-fluorodopamine can visualize cardiac sympathetic innervation. Neuropharmacologic and physiologic manipulations of different aspects of sympathetic function, including uptake 1 activity, produce characteristic changes in curves relating myocardial 6-18F-fluorodopamine-derived radioactivity to time (time-activity curves) (13–15). In the present study, we tested whether 6-18F-fluorodopamine PET scanning would detect altered cardiac uptake 1 activity associated with normal human aging.
MATERIALS AND METHODS
Subjects
The study protocol was approved by the Clinical Research Subpanel of the National Institute of Neurological Disorders and Stroke. Each subject gave written informed consent. Thirty-three healthy adult volunteers participated in the study. Seventeen were under 40 y old (range, 22 to 38 y; mean ± SEM, 30 ± 1 y; 2 women and 15 men), and 16 were over 50 y old (range, 52 to 86 y; mean ± SEM, 65 ± 3 y; 4 women and 12 men). The group was divided, by the protocol design, into subjects under 40 y old as the younger group and subjects over 50 y old as the older group. All had an unremarkable screening medical history, physical examination, serum chemical testing, complete blood count, and electrocardiogram. They had taken no medication for at least 4 wk before the study. No caffeine-containing beverages, cigarettes, or alcohol was permitted for at least 24 h before the scanning session.
PET Scanning
A brachial arterial catheter was inserted percutaneously after local anesthesia of the overlying skin for arterial blood sampling and hemodynamic monitoring.
Each subject was placed supine, feet first, in an Advance whole-body scanner (General Electric) for thoracic imaging. An 8-min transmission scan with rotating 68Ge/68Ga pin sources was obtained for attenuation correction. 13NH3 (about 185 MBq) was then injected intravenously over 30 s, and dynamic 3-dimensional data acquisition (35 contiguous transaxial slices 4.25 mm apart) was done over 20 min to assess myocardial perfusion. At least 1 h after 13NH3 administration, after a second transmission scan, 6-18F-fluorodopamine (about 37 MBq), synthesized as described previously (16), was infused at a constant rate for 3 min. Dynamic 3-dimensional data acquisition was done in five 1-min, five 5-min, four 15-min, and three 30-min frames, for a total of 3 h of scanning in most subjects.
Data Analysis
Arterial blood samples were assayed for total radioactivity, plasma radioactivity, and 6-18F-fluorodopamine concentrations. Plasma metabolite concentrations were calculated from the total plasma radioactivity minus the plasma 6-18F-fluorodopamine concentrations. The contribution of metabolites to cellular radioactivity was estimated from calculation of a cell plasma partition coefficient as described previously (17).
Dynamic 6-18F-fluorodopamine scanning data were reconstructed after correction for attenuation and for the physical decay of 18F. Cardiac images were analyzed as described previously (17). Briefly, as the data derived from the septum and the lateral wall did not differ significantly from those derived from the entire left ventricular myocardium, circular regions of interest that were approximately half the ventricular wall thickness were placed on images of the septum, lateral wall, and left ventricular chamber by use of time-averaged pictures of a single slice. Left ventricular radioactivity was averaged from 2 regions of interest each in the left ventricular lateral wall and septum. Radioactivity concentrations were standardized by correcting for the dose of radioactive drug per unit of body mass of the subject and are expressed as Bq · kg/mL · MBq (becquerels per volume tissue [mL], corrected by body weight [kg] and injection dose [MBq]). Time-activity curves relating myocardial radioactivity to time were constructed from the dynamic data and compared for the 2 groups.
Dynamic 13NH3 PET images were used to calculate myocardial blood flow with the Procard program (National Institutes of Health). Radioactivity in the left ventricular chamber across time was used as the input function, and 4 continuous short-axis slices of the myocardium were used to determine the concentrations of 13NH3-derived radioactivity in tissues. A 2-compartment model was used to calculate perfusion (in mL/min/g of tissue) on the basis of the average levels of 13NH3-derived radioactivity for the 4 slices.
Cardiac uptake of 6-18F-fluorodopamine was calculated from the peak myocardial level of 6-18F-fluorodopamine-derived radioactivity divided by the area under the curve for 6-18F-fluorodopamine delivered to the heart by coronary perfusion (the integral over time of the plasma 6-18F-fluorodopamine concentration multiplied by the cardiac perfusion rate).
To assess the relationships among aging, arterial 6-18F-fluorodopamine levels, myocardial perfusion, and myocardial 6-18F-fluorodopamine-derived radioactivity, data were analyzed individually. Independent-means t tests were used to compare mean values in the older and younger groups. Statistical significance was defined by a P value of <0.05. Data are reported as mean ± SEM.
RESULTS
The older and younger groups did not differ significantly in terms of systolic and diastolic blood pressures (127 ± 5/67 ± 3 and 120 ± 9/65 ± 3 mm Hg, respectively), heart rate (65 ± 3 and 62 ± 3 bpm, respectively), or body mass (81 ± 4 and 73 ± 5 kg, respectively).
By 5 min after the 3-min infusion of 6-18F-fluorodopamine, the mean left ventricular myocardial concentration of 6-18F-fluorodopamine-derived radioactivity was higher in the older group (9,578 ± 536 Bq · kg/mL · MBq) than in the younger group (7,533 ± 435 Bq · kg/mL · MBq) (P = 0.007) (Fig. 1; Table 1). The mean level of 6-18F-fluorodopamine-derived radioactivity in arterial whole blood at this time was also higher in the older group than in the younger group (2,306 ± 157 and 1,794 ± 118 Bq · kg/mL · MBq, respectively) (P = 0.013), and myocardial perfusion was also greater (0.976 ± 0.008 and 0.661 ± 0.0065 mL/min/g, respectively) (P = 0.03) (Table 1). The plasma metabolite concentration was higher in the older group than in the younger group (1,890 ± 181 and 1,653 ± 156 Bq · kg/mL · MBq, respectively) (P < 0.001).
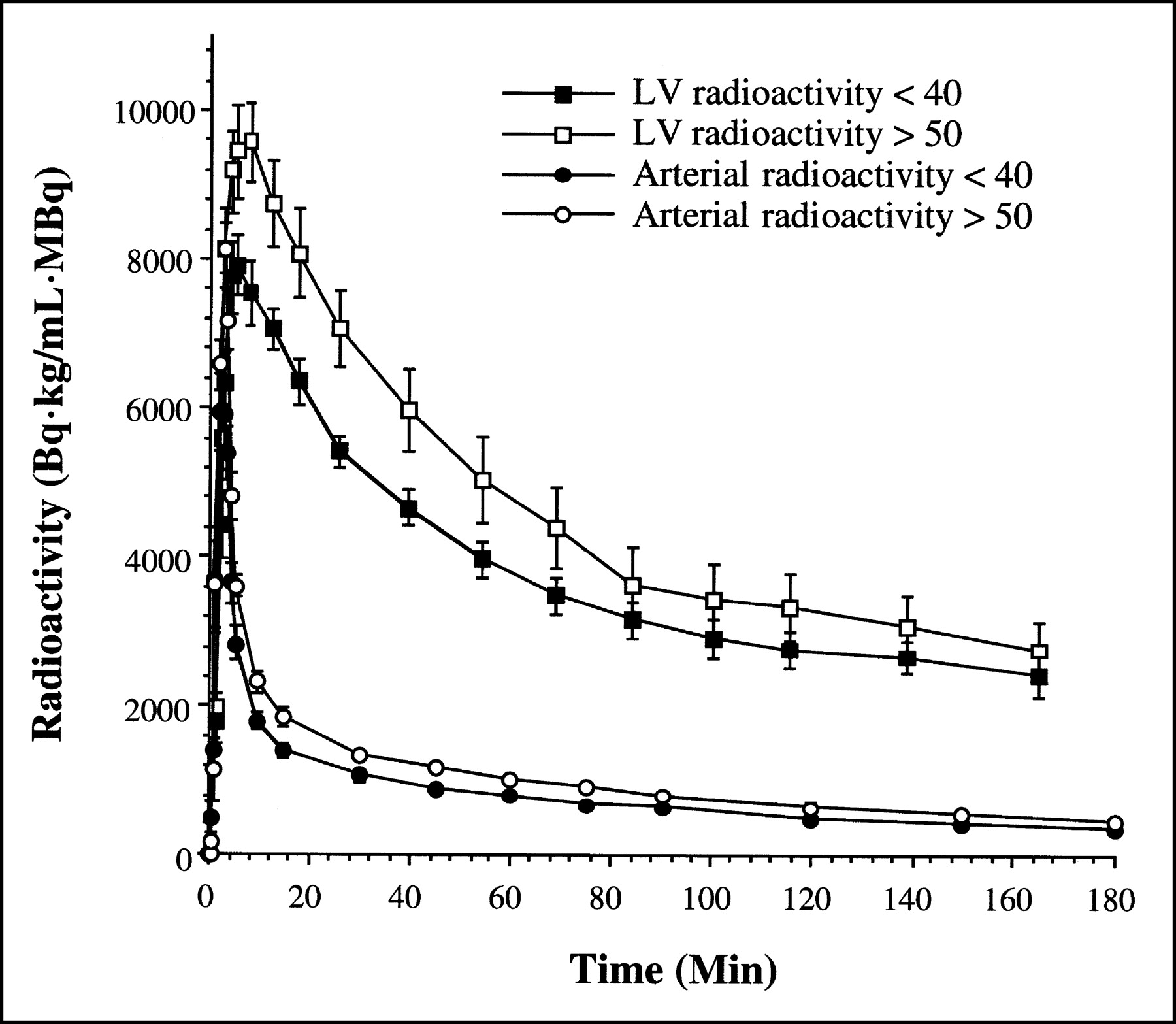
Time-activity curves for myocardial and arterial whole-blood 6-18F-fluorodopamine-derived radioactivity in older (>50 y old) and younger (<40 y old) healthy volunteers. LV = left ventricular myocardium.
Delivered 6-18F-Fluorodopamine and Actual and Predicted Peak Left Ventricular 6-18F-Fluorodopamine-Derived Radioactivity in Young and Old Subjects
The peak myocardial concentration of 6-18F-fluorodopamine (attained at about 10 min), divided by the area under the curve for the delivery of arterial blood 6-18F-fluorodopamine, provided a measure of myocardial extraction of the tracer. Cardiac uptake of 6-18F-fluorodopamine-derived radioactivity averaged 74% in the younger group and 48% in the older group (P = 0.02).
By 5 min after the 3-min infusion of 6-18F-fluorodopamine, 6-18F-fluorodopamine-derived radioactivity levels in the older and younger groups were similar in the liver (6,764 ± 429 and 6,845 ± 497 Bq · kg/mL · MBq, respectively), spleen (6,389 ± 694 and 6,428 ± 834 Bq · kg/mL · MBq, respectively), renal cortex (28,109 ± 2,256 and 28,998 ± 9,148 Bq · kg/mL · MBq, respectively), and renal pelvis (25,126 ± 3,746 and 29,609 ± 9,010 Bq · kg/mL · MBq, respectively). Biliary excretion, reflected by radioactivity in the gallbladder, was substantially greater in the older subjects than in the younger subjects (9,702 ± 206 and 4,591 ± 464 Bq · kg/mL · MBq, respectively) (P = 0.0009). Similarly, after 3 h, the excretion of radioactivity in urine was greater in the older group than in the younger group (23.5 ± 0.9 and 16.3 ± 1.5 ΜΒq, respectively) (P = 0.003), as was the percentage of injected tracer in urine (59% ± 5% and 44% ± 5%, respectively) (P = 0.05).
DISCUSSION
In this study, left ventricular myocardial levels of radioactivity after administration of the sympathoneural imaging agent 6-18F-fluorodopamine were higher in people more than 50 y old than in people less than 40 y old. At first glance, the higher radioactivity levels in the older group would suggest an increased density of cardiac sympathetic innervation or an increased extraction of the tracer via the cell membrane norepinephrine transporter, because uptake 1 is the main means for removing circulating catecholamines in the human heart (5). After adjustment for the delivery of 6-18F-fluorodopamine via coronary perfusion, however, the results actually led to the opposite inference, that cardiac uptake 1 activity decreases as people age.
The older group had increased myocardial perfusion, quantified from 13NH3 scanning (18). The finding of increased myocardial perfusion in older subjects, which might seem counterintuitive, actually agrees with previous reports (19–21). One possible explanation for increased myocardial perfusion in the older group would be increased cardiac work at rest (19). Using 15O-water, Senneff and colleagues did not note a change in myocardial blood flow with increasing subject age (22).
The older group also had higher arterial plasma 6-18F-fluorodopamine concentrations than did the younger group. The combination of greater left ventricular myocardial blood flow and higher 6-18F-fluorodopamine concentrations resulted in a substantially increased calculated delivery of 6-18F-fluorodopamine to the heart. When myocardial extraction of the tracer was quantified from the peak left ventricular myocardial level of 6-18F-fluorodopamine-derived radioactivity divided by the area under the curve for the arterial blood 6-18F-fluorodopamine concentration over time, the cardiac uptake of 6-18F-fluorodopamine averaged 74% in the younger group but only 48% in the older group.
Because the cardiac extraction of 3H-norepinephrine normally averages about 70%–80% in young adult subjects (5,23), the cardiac extraction of 6-18F-fluorodopamine seems about the same as that of norepinephrine (13).
Even during the 3-min infusion of 6-18F-fluorodopamine, myocardial 6-18F-fluorodopamine-derived radioactivity in the older group exceeded that in the younger group. During the initial 5 min, myocardial radioactivity appears to reflect both neuronal uptake of 6-18F-fluorodopamine and extraneuronal cellular uptake of O-methylated metabolites of 6-18F-fluorodopamine (17), which form very rapidly (24). Increased extraneuronal formation of metabolites of 6-18F-fluorodopamine could explain this early differentiation between the groups. Consistent with this explanation, by 5 min after the injection of 6-18F-fluorodopamine, the total concentration of metabolites in plasma was higher in the older group; in addition, the older group had significantly higher levels of 6-18F-fluorodopamine-derived radioactivity in the gallbladder and urine, a result that would be expected if there were more extraneuronal O-methylation and conjugation of the tracer.
Decreased cardiac uptake 1 activity might reflect decreased density of innervation or decreased numbers or function of transporter sites. The present results could not distinguish these possibilities. Because the rates of cardiac production of dihydroxyphenylglycol and dihydroxyphenylalanine, which are indices of the turnover and synthesis of norepinephrine in myocardial sympathetic nerves (25,26), do not change with aging (1), the density of innervation appears to remain unchanged. Right atrial tissue obtained during open-heart surgery from elderly patients without apparent heart failure shows a decreased accumulation of 3H-norepinephrine and a decreased shift of the norepinephrine concentration-response curve by desipramine, compared with tissue from pediatric patients with acyanotic congenital heart disease (27). These findings favor the notion of decreased numbers or function of cell membrane norepinephrine transporter sites on intact sympathetic nerves as a determinant of decreased cardiac uptake 1 activity with aging.
Assaying myocardial tissue norepinephrine concentrations might seem a straightforward way to distinguish the loss of sympathetic nerves from decreased activity of the membrane norepinephrine transporter; however, low norepinephrine concentrations might not necessarily indicate sympathetic denervation in this setting, because conditions in which norepinephrine turnover exceeds synthetic capacity also produce myocardial norepinephrine depletion (28). It has been reported that in cardiac conduction paths from tissue freshly obtained at autopsy, the contents of tyrosine hydroxylase and dopamine-β-hydroxylase decrease with aging (29); this finding does indicate denervation. Aged rats also have evidence of decreased tyrosine hydroxylase activity, on the basis of the responses of tissue norepinephrine contents to treatment with α-methyl-p-tyrosine, an inhibitor of tyrosine hydroxylase (30). As noted above, however, cardiac production of endogenous l-dihydroxyphenylalanine does not appear to change with normal human aging.
Goldstein et al. recently developed a kinetic model for the fate of 6-18F-fluorodopamine in the human heart (17). When a greater input of 6-18F-fluorodopamine was applied to the model, the predicted time-activity curve for myocardial 6-18F-fluorodopamine-derived radioactivity was clearly displaced upward from the empiric curve. That is, the actual amount of myocardial 6-18F-fluorodopamine-derived radioactivity was smaller than predicted, assuming that there were no changes in cardiac sympathetic function in the older group. When assigned values for effective rate constants in the model were varied for uptake 1, a 32% decrease in the value for the effective rate constant for uptake 1 yielded excellent curve fit, in agreement with the finding of decreased peak myocardial 6-18F-fluorodopamine-derived radioactivity for a given amount of delivery by coronary perfusion.
A few PET ligands have been used for sympathetic neuroimaging in the heart in clinical research. 11C-Hydroxyephedrine and 6-18F-fluorometaraminol (31–34) are not substrates for the catecholamine-metabolizing enzymes monoamine oxidase and catechol-O-methyltransferase and therefore have a metabolic fate in sympathetic nerves different from that of endogenous norepinephrine. In contrast, 6-18F-fluorodopamine has a disposition similar to that of endogenous catecholamines. l-11C-Norepinephrine has not been used because of difficulty in synthesizing the stereoisomer.
An aging-related decline in uptake 1 activity would be expected to enhance the delivery of catecholamines to adrenoceptors in the heart for a given amount of neuronally released or circulating catecholamine. This scenario in turn might help explain the well-known aging-related downregulation of β-adrenoceptor-mediated processes.
CONCLUSION
Left ventricular myocardial levels of radioactivity after the administration of 6-18F-fluorodopamine are higher in people more than 50 y old than in people less than 40 y old; however, after adjustment for the delivery of 6-18F-fluorodopamine via coronary perfusion, the evidence indicates decreased cardiac uptake 1 activity as people age.
Footnotes
Received Dec. 4, 2002; revision accepted May 20, 2003.
For correspondence or reprints contact: David S. Goldstein, MD, PhD, NINDS, NIH, Bldg. 10, Room 6N252, 10 Center Dr., MSC-1620, Bethesda, MD 20892-1620.
E-mail: goldsteind{at}ninds.nih.gov
REFERENCES
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.