


Abstract
We studied the response to F+0 renography and the relative and absolute individual kidney function in neonates and <6-mo-old infants before and after surgery for unilateral ureteropelvic junction obstruction (UJO). Methods: The results obtained at diagnosis and after pyeloplasty for 9 children (8 boys, 1 girl; age range, 0.8–5.9 mo; mean age ± SD, 2.4 ± 1.5 mo) with proven unilateral UJO (i.e., affected kidney [AK]) and an unremarkable contralateral kidney (i.e., normal kidney [NK]) were evaluated and compared with a control group of 10 children (6 boys, 4 girls; age range, 0.8–2.8 mo; mean age, 1.5 ± 0.7 mo) selected because of symmetric renal function, absence of vesicoureteral reflux or infection, and an initially dilated but not obstructed renal pelvis as proven by follow-up. Renography was performed for 20 min after injection of 123I-hippuran (OIH) (0.5–1.0 MBq/kg) immediately followed by furosemide (1 mg/kg). The relative and absolute renal functions and the response to furosemide were measured on background-subtracted and depth-corrected renograms. The response to furosemide was quantified by an elimination index (EI), defined as the ratio of the 3- to 20-min activities: An EI ≥ 3 was considered definitively normal and an EI ≤ 1 definitively abnormal. If EI was equivocal (1 < EI < 3), the response to gravity-assisted drainage was used to differentiate AKs from NKs. Absolute separate renal function was measured by an accumulation index (AI), defined as the percentage of 123I-OIH (%ID) extracted by the kidney 30–90 s after maximal cardiac activity. Results: All AKs had definitively abnormal EIs at diagnosis (mean, 0.56 ± 0.12) and were significantly lower than the EIs of the NKs (mean, 3.24 ± 1.88) and of the 20 control kidneys (mean, 3.81 ± 1.97; P < 0.001). The EIs of the AKs significantly improved (mean, 2.81 ± 0.64; P < 0.05) after pyeloplasty. At diagnosis, the AIs of the AKs were significantly lower (mean, 6.31 ± 2.33 %ID) than the AIs of the NKs (mean, 9.43 ± 1.12 %ID) and of the control kidneys (mean, 9.05 ± 1.17 %ID; P < 0.05). The AIs of the AKs increased at follow-up (mean, 7.81 ± 2.23 %ID) but remained lower than those of the NKs (mean, 10.75 ± 1.35 %ID; P < 0.05). Conclusion: In neonates and infants younger than 6 mo, 123I-OIH renography with early furosemide injection (F+0) allowed us to reliably diagnose AKs and to determine if parenchymal function was normal or impaired and if it improved after surgery.
Since the time that antenatal sonography became widespread, urinary tract abnormalities, often in the form of dilatation, have been detected in approximately 1 of 100 pregnancies (1,2). Between 20% and 50% of prenatally diagnosed dilatation is not evident on postnatal sonograms; of the remainder, 32%–50% is possibly related to ureteropelvic junction obstruction (UJO) (1–6). A final diagnosis of unilateral hydronephrosis caused by UJO will be made in ≤15% (3). The goals of postnatal management of asymptomatic unilateral hydronephrosis are to diagnose severe UJO in terms of restriction of urinary flow and renal parenchymal function so that decisions can be made about further treatment (2,3,6). Accepted protocols for furosemide injection during renography are the F+20 and F−15 methods described by O’Reilly et al. (7); these procedures require an indwelling catheter or at least 2 venous punctures. The recommended well-tempered diuretic renogram (8) and procedure guideline for diuretic renography in children (9) remain fastidious to apply in neonates and young infants because of the need for venous access and bladder catheterization. Sfakianakis et al. (10) were the first to propose another diuretic protocol: simultaneous injection of renal tracer and furosemide. This method is easy, shorter, and avoids unnecessary repeated venous punctures. It is thus particularly convenient for performing diuretic renography on children, and even more so for neonates and young infants. Recently, Wong et al. (11) published encouraging results for use of the F+0 protocol during 99mTc-mercaptoacetyltriglycine (MAG3) renography in children. The protocol could identify the site of obstruction (lower or upper) and distinguish between severe and moderate obstructive patterns. We have already studied the value of early furosemide injection (F+3) during 123I-hippuran (OIH) in children with UJO and obtained concordant results with both the F+3 and the F+20 protocols; identification of severe obstruction was accurate with both methods (12).
The proper management of unilateral UJO in neonates is still debated. Some authors recommend conservative management and close follow-up, whereas others prefer early surgery (2,3). Most authors take into account the function of the affected kidney (AK), as determined by renography, at diagnosis and follow-up. The major problem is that only relative renal function is mentioned. To our knowledge, only 1 publication has dealt with absolute renal function in unilateral UJO in children using 99mTc-dimercaptosuccinic acid (DMSA) (13). We routinely determine absolute renal function during OIH renography under furosemide, and reference values of renal function have been published (14). The aims of this study were, first, to evaluate the accuracy of the F+0 protocol when used in neonates and <6-mo-old infants to investigate persistent unilateral pelvic dilatation suggestive of severe UJO and, second, to compare the absolute and relative renal functions of the AKs and the contralateral NKs. These investigations were performed both at the time of diagnosis and during follow-up.
MATERIALS AND METHODS
Children with a history of urinary tract infection and abnormal findings on voiding cystourethrography were excluded, as were children with bilateral disease. Because, on children, we routinely perform diuretic renography using the F+0 protocol, we selected 2 particular groups of children for study. The first was a control group for whom significant obstructive uropathy could reasonably be excluded on the basis of repeated sonography that showed normal findings and follow-up that showed symmetric renal function (46%–54%). The second was a group with unilateral UJO who underwent surgery of the AK. All children were younger than 6 mo at the first examination and had been receiving antibiotic prophylaxis since birth (amoxicillin, 50 mg/d). The UJO group included only children for whom a postoperative diuretic renogram was available.
The control group consisted of 10 children (6 boys, 4 girls; age range, 0.8–2.8 mo; mean age ± SD, 1.5 ± 0.7 mo) with unilateral or bilateral pelvic dilatation detected during pregnancy. All had moderate or no pelvic dilatation after birth. They were referred to our institution to exclude significant obstruction and to measure tubular function. Radiologic and clinical follow-up until ≤24 mo (mean, 10 mo) excluded significant obstructive uropathy in all (Fig. 1).

Diuretic (F+0) renography was performed on 1.4-mo-old boy in whom bilateral pelvic dilatation detected during pregnancy persisted on left side on postnatal sonograms. (A) One-minute posterior views show symmetric kidneys and rapid, symmetric urinary excretion. (B) Two-minute posterior views obtained 20 min after injection (left) and after prone positioning (right) show no significant urinary flow restriction. (C) Regions of interest and time–activity curve (heart, dark line; bladder, dotted line). Bladder curve shows rapidly increasing activity and micturition. (D) Background-corrected renograms (left kidney, dotted line; right kidney, dark line) show symmetric early 123I-OIH renal uptake (accumulation index: left, 8.39 %ID; right, 9.82 %ID) and normal symmetric response to early furosemide injection (elimination index: left, 4.61; right, 6.26).
The UJO group consisted of 9 children (8 boys, 1 girl; age range, 0.8–5.9 mo; mean age, 2.4 ± 1.5 mo) in whom unilateral UJO was suspected on the grounds of unilateral pelvic dilatation detected during pregnancy and persisting on 2 consecutive sonograms after birth. Twelve diuretic renograms were obtained, 3 children being studied twice. All children had a contralateral kidney determined to be unremarkable (i.e., normal kidney [NK]) on the basis of sonography and voiding cystourethrography. A control diuretic renogram was obtained 6 mo to 2 y after unilateral pyeloplasty (mean, 11 ± 8 mo). Age at surgery ranged from 7 to 35 mo (mean, 17 ± 10 mo). Concomitant sonograms obtained at diagnosis and after surgery were also analyzed.
All children were breast- or bottle-fed during the 30 min preceding tracer injection. No intravenous or bladder catheter was inserted. The children were placed supine in a fixing cushion to minimize movement, with the camera underneath, and the parents were encouraged to stay with their child. 123I-OIH, 0.5–1.0 MBq, was prepared in a 1-mL syringe in a precise volume of 0.10–0.15 mL and was injected as a bolus with a single-use needle. A 2-phase, 20-min dynamic acquisition (30 × 1 s per frame and 117 × 10 s per frame) using a 128 × 128 matrix and a 20% window centered over the 159-keV energy peak of 123I was started immediately after tracer injection. A dose of 1 mg/kg furosemide was slowly injected using the same venous access (F+0). To assess gravity-assisted urinary drainage, a 5-min dynamic acquisition (10 s per frame) was obtained using the same parameters with the child prone. At least 2 posterior static views were acquired with the child supine: at the end of the first dynamic acquisition and after the prone study.
Individual kidney depth was determined on 2 lateral views using a 57Co marker placed under the fixing cushion. The global kidney-to-camera distance was measured in centimeters.
To obtain the injected activity corrected for attenuation, diffusion, and decay in counts per minute, a standard consisting of a 100-mL vial of 0.9% NaCl containing a 0.1-mL aliquot of 123I-OIH was prepared and placed in an acrylic container, which was filled with water, in the fixing cushion. Acrylic plates corresponding to the measured individual kidney depth in centimeters were interposed between the container and the cushion to correct for attenuation. A 1-min static image was acquired in a 128 × 128 matrix (20% window, 159 keV) after the examination. The mean pixel activity for both the vial and the background was obtained by the region-of-interest technique. Because the injected volume was 0.10 or 0.15 mL, the injected activity in counts per minute was obtained by multiplying the background-corrected activity of the standard by 1.0 or 1.5.
Quantitative parameters were calculated on time–activity curves generated for the heart, kidneys, lateral perirenal areas, and bladder using the region-of-interest technique. Background-corrected renal curves were generated to calculate an accumulation index (AI), which was defined as the percentage of injected activity (%ID) extracted by each kidney during 1 min starting 30 s after peak heart activity. The AI of each kidney was calculated using the ratio of the area under the curve of each renogram in counts per minute divided by the injected activity in counts per minute and multiplied by 100. Reference AIs for neonates and young infants have already been established and range from 8 to 12 %ID (14). Relative renal function, expressed as a percentage, represented the contribution of each kidney to the global renal function obtained by adding the left and right AIs.
The response to furosemide was measured by an elimination index (EI), which was defined as the ratio of the 3- to 20-min activities or, when the renal peak occurred at <3 min, the ratio of the peak to 20-min activities. The following patterns of response to F+0 were used to differentiate between AKs and NKs: definitively normal, EI ≥ 3; equivocal, 1 < EI < 3; and definitively abnormal, EI ≤ 1. When the response to F+0 was equivocal, the response to gravity-assisted drainage as determined by a 5-min acquisition with the child prone was visually scored as absent or present by 2 experienced nuclear medicine physicians.
Concomitant sonograms were analyzed, and the results were reported as normal when no pelvic dilatation was observed. When dilatation was observed, the anteroposterior diameter of the dilated renal pelvis was measured in millimeters and graded as follows: grade 0, <10 mm; grade 1, 10–20 mm; or grade 2, >20 mm.
The results of diuretic renography were analyzed for the AKs and contralateral NKs of the UJO group and for the kidneys of the control group in terms of response to furosemide as measured by the EI, response to gravity-assisted drainage in instances of equivocal results, renal function as measured by the AI, and relative function. These parameters were compared between AKs and NKs and with the results of sonography. For children with UJO, results obtained before and after pyeloplasty were compared (Fig. 2).

Diuretic renography was performed on 2.5-mo-old boy in whom grade 2 hydronephrosis on left side was diagnosed during pregnancy and confirmed after birth. (A) One-minute posterior views at diagnosis show parenchymal thinning of left kidney and no response to furosemide, whereas right kidney appears normal. (B) Same views obtained at follow-up show persistent left parenchymal thinning and improvement in left urinary flow under furosemide. (C) Background-corrected renal curves (left kidney, dark line; right kidney, dotted line) at diagnosis show decreased tracer uptake by left kidney (AI, 6.50 %ID) and typical obstructive curve pattern (EI, 0.66). Contralateral kidney was normal (AI, 8.94 %ID; EI, 4.35). (D) After surgery, left kidney improved in function and drainage (AI, 9.43 %ID; EI, 2.15) and right kidney remained normal (AI, 9.40 %ID; EI, 6.43).
Statistical analysis of the AIs and EIs was performed using the Wilcoxon signed rank test to compare results obtained before and after surgery for the same children. The Wilcoxon rank sum test was used to compare unmatched data obtained for the group of children with unilateral AKs and for the group of children with no significant obstruction. Sonographic grading of hydronephrosis was analyzed using the Kruskal–Wallis 1-way equality test. Results were considered significant when P was <0.05.
RESULTS
Response to F+0 and Results of Sonography
In the control group, none of the 20 kidneys had an abnormal response to furosemide (Table 1). EIs ranged from 1.19 to 5.60 (mean, 3.47 ± 1.42) for the left kidneys and from 1.25 to 8.26 (mean, 4.16 ± 2.44) for the right kidneys. If we consider the results for the 20 kidneys together, EIs ranged from 1.19 to 8.26 (mean, 3.81 ± 1.97). Seven kidneys had EIs ranging from 1.19 to 2.81 (mean, 1.94 ± 0.59) and were considered as having an equivocal response to furosemide. A response to gravity-assisted drainage in the prone position was observed in all 7 of these kidneys. In 6 of the 7, anteroposterior renal pelvic diameter was measurable and ranged from 2 to 14 mm (mean, 7.5 ± 5 mm); according to the grade of hydronephrosis, none was considered significantly dilated.
EIs and Sonographic Dilatation Grades for Control Group
Sonography showed a normal (grade 0) renal pelvis in 17 (85%) of the 20 examined kidneys. A moderate, grade 1, dilatation was measured in 3 kidneys (1 kidney of patient 7 and both of patient 9).
In the UJO group, the number of renograms obtained before surgery was 12, because 3 of the 9 children were studied twice (Table 2). In 7 of the 9 children, obstruction was left-sided. At diagnosis, all 9 AKs showed a definitively abnormal response, with EIs ranging from 0.42 to 0.80 (mean, 0.56 ± 0.12); 5 (42%) of the 12 EIs were <0.50. The NKs had EIs ranging from 1.17 to 6.51 (mean, 3.24 ± 1.88); 6 (50%) were >3. An equivocal response to F+0, with EIs ranging from 1.17 to 2.07, was obtained for the other 6 NKs, and all responded to the change in position from supine to prone.
EIs and Sonographic Dilatation Grades for UJO Group Before and After Surgery
A control diuretic renogram was obtained 6 mo to 2 y after unilateral pyeloplasty, when the children ranged in age from 7 mo to 3 y (mean, 1.4 ± 0.8 y). After surgery, all AKs responded better to furosemide: EIs ranged from 1.75 to 3.55 (mean, 2.81 ± 0.64). In 4 children, the response to furosemide remained equivocal, with EIs ranging from 1.75 to 2.78. In all 4, urinary drainage was improved by the change in position. The EIs of the contralateral NKs ranged from 2.40 to 10.05 (mean, 5.68 ± 2.21). The EI remained <3 in only 1 child (patient 1), aged 7 mo, at the time of the follow-up study. Changing the child’s position from supine to prone completed the response to furosemide.
Before surgery, only 11 sonograms were available for analysis, because for 1 child (patient 9) a second sonogram was not obtained before surgery. According to the assigned grade, none of the AKs had a normal pelvis. Pelvis diameters of the AKs ranged from 8 to 45 mm (mean, 24 ± 9 mm). Grade 2 hydronephrosis was observed on 8 (73%) of the 11 available sonograms. All contralateral NKs had grade 0 hydronephrosis at diagnosis.
Postoperative sonography showed resolution of dilatation in 5 patients (56%) and a decrease from grade 2 to grade 1 in 1 patient. Hydronephrosis remained unchanged in 2 AKs (1 with grade 1 and 1 with grade 2). Patient 1 had an increase from grade 0 (8 mm) before surgery to grade 1 (10 mm) 6 mo after pyeloplasty.
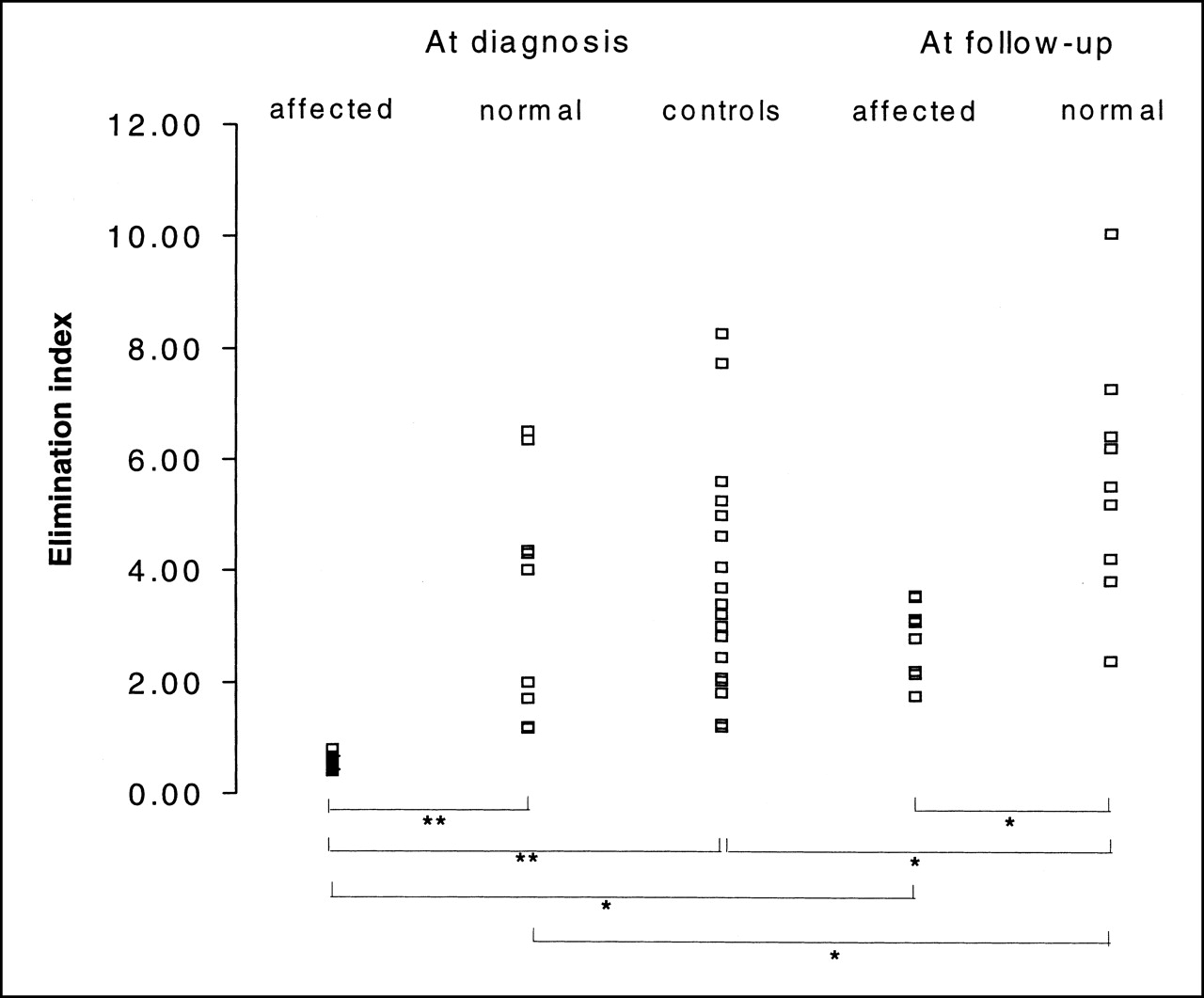
The difference in age between the UJO group before diagnosis and the control group was not statistically significant (P = 0.99). The EIs of the AKs before surgery were significantly lower than the EIs of the contralateral NKs and the control kidneys (P < 0.001) (Fig. 3). No significant difference was found between the NKs of the UJO group and the control kidneys (P = 0.37). After surgery, the EIs in the UJO group remained significantly lower for the AKs than for the NKs (P = 0.002). An increase in EI was observed both for the AKs and for the NKs of the UJO group. Interestingly, the EIs of the NKs at follow-up were superior to the EIs of the control kidneys.

EIs of AKs, contralateral NKs, and control kidneys at diagnosis and of AKs and NKs at follow-up. *P < 0.05; **P < 0.001.
The anteroposterior diameter of the renal pelvis was larger in the AKs than in the NKs of the UJO group or in the control kidneys at diagnosis (P < 0.001). In the AKs, renal pelvic diameter decreased significantly after surgery (P = 0.002).
Individual Renal Function, Global Renal Function, and Relative Renal Function
In the control group, left kidneys had AIs ranging from 7.65 to 10.99 %ID (mean, 8.82 ± 0.99 %ID) and right kidneys, from 8.00 to 12.31 %ID (mean, 9.29 ± 1.23 %ID) (Table 3). When the 20 kidneys were considered together, mean AI was 9.05 ± 1.17 %ID. Global renal function ranged from 15.88 to 23.30 %ID (mean, 18.11 ± 2.06 %ID).
AIs for UJO Group Before and After Surgery and for Control Group
In the UJO group, AIs at diagnosis ranged from 2.88 to 9.97 %ID (mean, 6.31 ± 2.33 %ID) for the AKs, and 6 of 9 were less than reference values (reference range, 8–12 %ID). AIs were markedly decreased (<6 %ID) in 4. All contralateral NKs had normal AIs ranging from 8.23 to 11.92 %ID (mean, 9.43 ± 1.12 %ID). Global function ranged from 11.50 to 22.14 %ID (mean, 15.74 ± 3.00 %ID), and relative function of the AKs ranged from 25% to 50% (mean, 39% ± 9%). Relative function of the AKs was <40% in the 4 patients with the more severely decreased AIs.
After surgery, the AIs of the AKs ranged from 2.61 to 10.38 %ID (mean, 7.81 ± 2.23 %ID). AI improved in 5 of 9 AKs (56%) and remained unchanged in 4: normal in 2 and low in 2 (Fig. 4). The AIs of the contralateral NKs ranged from 9.13 to 13.45 %ID (mean, 10.75 ± 1.35 %ID) at follow-up. Only 1 child (patient 7) had an AI slightly greater than the reference value. Global renal function ranged from 14.34 to 21.72 %ID (mean, 18.55 ± 2.26 %ID) and reached reference values in all but 1 child. Relative function of the AKs ranged from 18% to 50% (mean, 41% ± 10%). It remained <40% in 2 children, staying stable in 1 and decreasing in 1 (Fig. 5).

AIs of AKs (A) and contralateral NKs (B) before and after surgery.
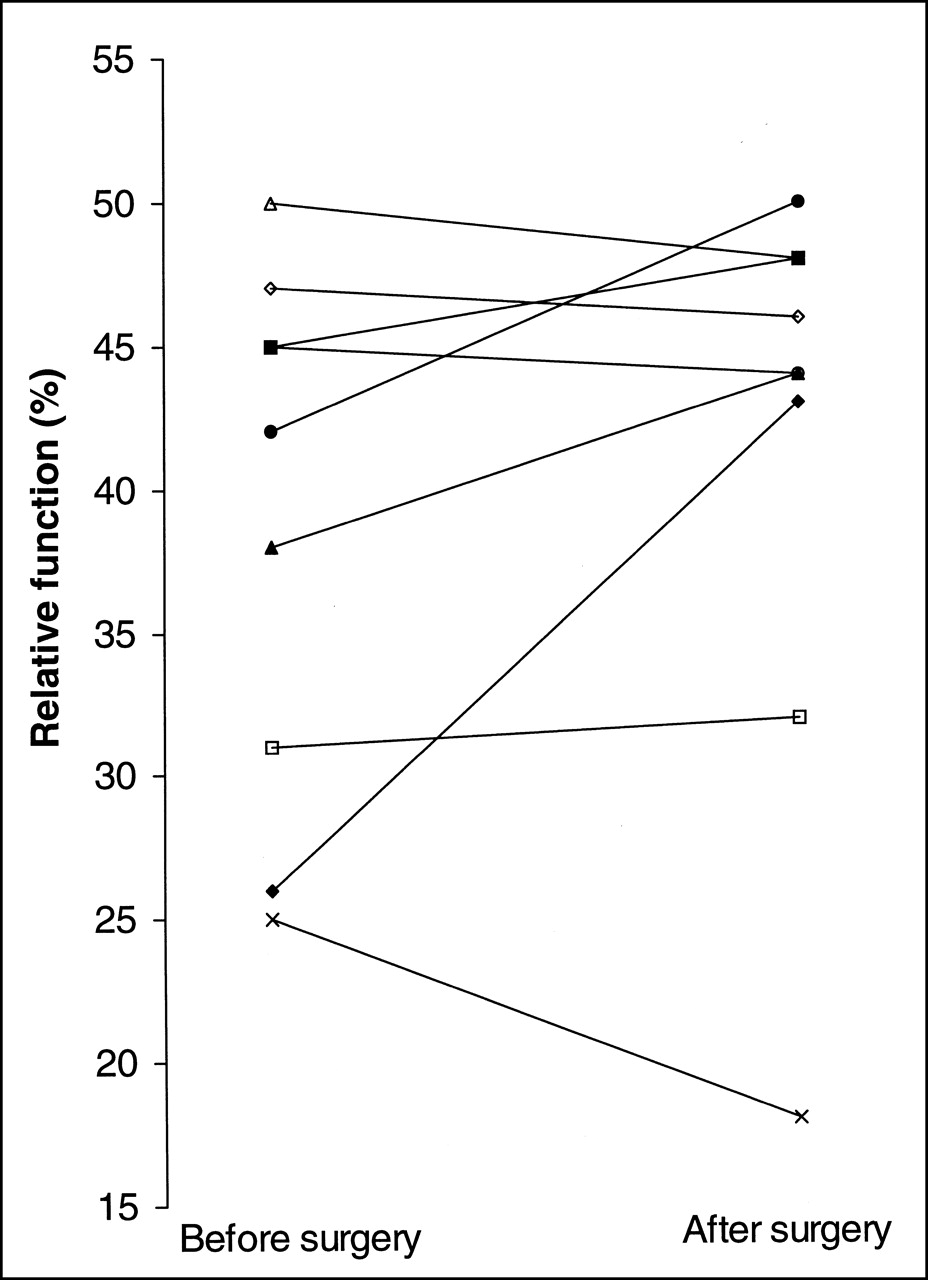
Relative function of AKs before and after surgery.
Statistical analysis showed that in the UJO group, the AIs of the AKs were significantly lower than the AIs of the contralateral NKs and of the control kidneys (P = 0.002) (Fig. 6). No difference was observed between the NKs of the UJO group and the control kidneys (P = 0.16). After surgery, AI did not improve significantly for the AKs (P = 0.05) and remained significantly lower for the AKs than for the NKs (P = 0.007). The AIs of the contralateral NKs of the UJO group were higher than the AIs of the control kidneys (P = 0.006).

AIs of AKs, contralateral NKs, and control kidneys at diagnosis and of AKs and NKs at follow-up. *P < 0.05.
DISCUSSION
Up to 50% of hydronephrosis is caused by UJO (1,2,10,11,15). Because the term obstruction is imprecise, Koff (3) proposed that UJO be defined as “a functional or anatomic obstruction to urine flow from the renal pelvis to the ureter that, left untreated, results in symptoms or renal damage.” From a clinical point of view, the goal of postnatal diagnosis is to distinguish those kidneys whose function will deteriorate because of obstruction and thus possibly benefit from surgery from those whose hydronephrosis will either spontaneously regress or remain stable without impairing parenchymal function.
There is still much debate over how obstruction in neonates is best managed. Until now, evidence that surgery will improve renal function or at least prevent further renal damage has been lacking (1,2,10). In 1994, Koff and Campbell (15) reported a study in which 104 neonates with unilateral UJO were managed conservatively and followed up for ≤5 y: Only 7 (7%) of the children required pyeloplasty because of deterioration in differential function with or without progression of hydronephrosis. Because renal function, especially glomerular filtration, is immature at birth, some authors recommend waiting until at least 4 wk after birth before performing diuretic renography (15,16,17). Using 99mTc-MAG3, which is actively secreted by the renal tubules, Wong et al. (18) obtained reliable results for the diuretic test in neonates and suggested that the previously published unreliable results for diuretic renography in neonates could have been related to the use of 99mTc-diethylenetriaminepentaacetic acid (DTPA), which is a glomerular tracer. Eising et al. (19), using 123I-OIH, also obtained reliable results for diuretic renography, even in neonates.
We lack a gold standard with which to compare the F+0 methods. In their study, Wong et al. (11) considered ≤12 mo of follow-up data to be satisfactory for distinguishing children who require surgery from those who can be managed conservatively. They also pointed out that 53 normal, nondilated kidneys had normal half-time clearance (<10 min), as had been reported for a study using 99mTc-MAG3 (20). In our study of children presenting with proven unilateral UJO, we compared the AK EIs with the NK EIs and found a statistically significant difference. Moreover, the EIs were also compared with those of an age-matched control group with no or moderate renal pelvic dilatation at initial examination and no obstructive uropathy during follow-up. Again, the EIs were significantly lower for the AKs than for the control kidneys. No difference was observed between the contralateral NKs of the UJO group and the control kidneys. These results allowed us to define an EI of <1 as clearly abnormal and highly suggestive of obstruction.
As Rossleigh et al. (21) have emphasized, obtaining an additional view after gravity-assisted drainage is mandatory in neonates and infants to improve the accuracy of the method. We obtained at least 2 additional static views, just before and after a 5-min acquisition with the child prone. Thus, the total study duration was at least 30 min and allowed for proper evaluation of the response to furosemide. The response to a change in position from supine to prone was helpful for EIs of 1–3 and allowed us to exclude equivocal responses in such cases.
It has also been emphasized that use of the F−15 protocol would be better for avoiding false-negative or equivocal results, particularly in cases of intermittent obstruction. Foda et al. (22), in a prospective randomized trial, studied 88 children according to the F−15 or F+20 protocol (44 children in each group) and showed that the number of positive results was significantly higher with the F−15 protocol, although the number of equivocal results was identical for both protocols. In our study, we found no false-positive results in the control group; changing the child’s position from supine allowed us to classify the cases with an equivocal response after F+0. The accuracy of this simple technique is further supported by the results of follow-up studies of the same children after surgery: The urinary drainage of all AKs improved.
In clinical practice, most authors recommend using a 40% threshold for relative function of the AK when deciding whether to treat a patient surgically (17,23–31). In a recent study, Eskild-Jensen at al. (32) monitored renal function in 12 newborn pigs with unilateral induced partial ureteral obstruction and contralateral normal kidneys and in a control group of animals with normal kidneys. Using 99mTc-DTPA, the investigators performed renography at 4, 12, and 24 wk and measured glomerular filtration rate (GFR) by plasma clearance and relative renal function on background-subtracted renal curves. They grouped the AKs according to relative function at first examination. In one group, with relative function > 40%, they observed at 24 wk a marked decrease in relative function to 17% and 22% in 2 pigs, a moderate decrease from 49% to 43% in 1, and stable function in the other 3. In the other group, with relative function < 40%, function improved to >40% at 24 wk for 4 AKs but further decreased from 39% to 32% for 1 AK. In a severely obstructed AK with an initial relative function of 7%, they found a significant increase to 31% at 12 wk. They concluded that initial measurements at 4 wk, including relative renal function, kidney volume, pelvic dilatation, and single-kidney glomerular filtration rate, cannot predict the outcome of renal function at 12 and 24 wk (32). Our observations on the absolute and relative renal functions of the AKs were similar: We saw either stability or improvement of renal function after surgery in the more affected AKs.
In a second publication, Eskild-Jensen at al. (33) found a significant decrease in total GFR at 4 wk in animals with obstruction when compared with control animals. At 12 and 24 wk, the total GFR of the obstructed group did not differ from that of the control group. The investigators observed a significant increase in the GFR of the contralateral NKs when compared with the control kidneys at 12 wk but no difference at 4 and 24 wk. Kidney volume was measured by nuclear magnetic resonance. No difference in volume was found at any time between the contralateral NKs and the control kidneys. Eskild-Jensen at al. concluded that neither function nor size of NKs can predict a decrease in function of AKs in the early phase. In our study, we observed increased absolute function in 2 NKs contralateral to the more obstructed AKs, in which function had not fully recovered at the time of follow-up. Relative function of the AKs remained <40% in these 2 cases, staying stable in one and further decreasing in the other, whereas absolute renal function improved in one and stayed stable in the other. This observation supports the view that measurement of only the relative renal function is insufficient because the decreased function of a single kidney may be counterbalanced by a functional increase in the contralateral kidney.
In another recent study, Groshar et al. (13) performed 99mTc-DMSA SPECT at the time of diagnosis on 13 neonates and infants with unilateral UJO and on a control group of 15 age-matched children with no significant urinary tract abnormalities. The investigators measured renal volume, percentage of tracer uptake per milliliter of renal parenchyma, and absolute renal uptake. They observed a significant decrease in tracer uptake per milliliter of renal parenchyma for the AKs when compared with the contralateral NKs and the control kidneys, but absolute 99mTc-DMSA uptake did not differ between the AKs and the contralateral NKs or the control kidneys. Because the total uptake of the AKs was preserved, no contralateral adaptive changes occurred. Similarly, in our patients, the function of the contralateral NKs remained normal and stable when the AKs had preserved renal function at diagnosis and follow-up.
CONCLUSION
F+0 renography is accurate for diagnosing unilateral UJO in neonates and infants younger than 6 mo. Relative renal function in itself is insufficient for monitoring the function of both AKs and contralateral NKs because of the possibility of adaptive changes. The function of each kidney must be measured separately to assess whether function has improved, remained stable, or decreased at follow-up.
Footnotes
Received Apr. 30, 2001; revision accepted Aug. 7, 2001.
For correspondence or reprints contact: Ariane Boubaker, MD, Nuclear Medicine Department BH07, Centre Hospitalier Universitaire Vaudois, Bugnon 46, 1011 Lausanne, Switzerland.
REFERENCES
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Radionuclide imaging of the renal tract: principles and applications
- Forced Diuresis Improves the Diagnostic Accuracy of 18F-FDG PET in Abdominopelvic Malignancies
- Radionuclide Investigations of the Urinary Tract in the Era of Multimodality Imaging
- The F+0 Protocol for Diuretic Renography Results in Fewer Interrupted Studies Due to Voiding Than the F-15 Protocol