


Abstract
The molecular imaging and treatment of neuroendocrine tumors (NETs) with radiolabeled somatostatin analogs represent a milestone in the development of theranostic compounds. Whole-body scintigraphy with 111In-pentetreotide has revolutionized the diagnosis and staging of NETs and the evaluation of treatment outcomes. At present, diagnostic accuracy with positron-emitting radionuclides is greater than 90%. Peptide receptor radionuclide therapy (PRRT) has become a well-accepted treatment for patients with well-differentiated inoperable or metastatic NETs and disease progression after first-line treatment. Disease control rates (complete or partial remission or stable disease in patients with formerly progressive disease) of up to 95%, with a low incidence of long-term hematologic and renal toxicity, have been reported. In a recently published randomized trial, compared with intensified treatment of midgut NETs with long-acting and repeatable octreotide, PRRT reduced the hazard of disease progression and death by 79%. Upcoming developments in PRRT include the use of somatostatin receptor antagonists and α-emitting radionuclides, which may further enhance treatment outcomes.
The field of theranostics, comprising the combination of molecular imaging and molecular radiotherapy, exploits the receptor binding and internalization of the same peptides for imaging and therapy. In this field, the development of somatostatin receptor (SSTR)–targeting techniques represents a milestone. The somatostatin analog (SSA) octreotide was developed in the 1980s for its antiproliferative and hormone release–inhibiting effects in neuroendocrine tumors (NETs), such as pituitary tumors or the so-called carcinoids (1,2). Originally used to target a variety of neoplasms, SSTR-targeting theranostic compounds presently are widely used to image and treat well-differentiated gastroenteropancreatic and bronchopulmonary NETs.
RECEPTOR TARGETING
SSTR Expression
In humans, at least 5 subtypes of SSTRs can be found; subtype 2 (SSTR-2) is the predominant receptor in most NETs (3). In the early era of SSTR scintigraphy, it was used for the detection of both primary tumors and previously undetected metastases of NETs and proved valuable in visualizing several other tumors as well as granulomatous diseases (4). The initial targets of 111In-pentetreotide scintigraphy (4) were NETs (carcinoids, endocrine pancreatic tumors, pituitary tumors, paragangliomas, pheochromocytomas, medullary thyroid carcinomas, neuroblastomas, and small cell lung cancer) and other tumors and diseases (meningiomas, breast cancer, Merkel cell tumors, lymphomas, sarcoidosis, and tuberculosis).
There is a distinct correlation between tumor grade according to 2010 World Health Organization criteria and SSTR-2 expression (5). High levels of SSTRs are predominantly found in grade 1 and 2, well-differentiated and moderately differentiated NETs; with the loss of differentiation, the characteristic of SSTR expression is frequently lost, too. Hence, SSTR targeting for imaging or therapy is generally limited to lower-grade disease.
Development of Targeted Compounds
In 1987, the first in vivo SSTR scintigraphy in humans was performed using 123I-Tyr3-octreotide. Cumbersome and expensive, the radioiodine was replaced with chelated 111In in 1989. This radiopharmaceutical was used for imaging and, starting in 1992, for therapy, making it the first SSTR-targeting theranostic compound (6). With the development of the chelator DOTA, SSAs could be stably linked to β-emitting radionuclides, which have favorable physical characteristics for use in therapy (Table 1).
Differences in chemical structure (as in the chelator, radioisotope, or SSA) imply differences in affinity and biodistribution (7–9). In an in vitro comparison, an increase in the affinity for SSTR-2 of up to 12-fold was seen with a single substitution (Table 2; Fig. 1) (10). The choice of the radioisotope is crucial for both diagnosis and therapy; the introduction of 68Ga-labeled SSAs for PET has dramatically changed the diagnostic approach for NETs. From the therapeutic standpoint, despite no clinically demonstrated superiority in the affinity of 90Y- versus 177Lu-labeled SSAs, the greater manageability of the latter—from a dosimetric point of view—has made it the compound of choice for peptide receptor radionuclide therapy (PRRT). Given that 90Y is a pure β-emitter, yttrium-based compounds cannot strictly be regarded as theranostic agents. Posttherapeutic imaging relies on the addition of a small amount of [111In-DOTA0-Tyr3]SSA to the administered therapeutic radiopharmaceutical. SSTR-2–targeting theranostic agents used in clinical practice are 111In-pentetreotide ([111In-DTPA0]octreotide), [177Lu-DOTA0-Tyr3]octreotide, [177Lu-DOTA0-Tyr3]octreotate, [177Lu-DOTA0]lanreotide, [90Y-DOTA0-Tyr3]octreotide, [90Y-DOTA0-Tyr3]octreotate, [90Y-DOTA0]lanreotide, [213Bi-DOTA0-Tyr3]octreotide, and [177Lu-DOTA]JR11.
SSTR-2 Affinity (10)

Structural formulae of DOTA0-Tyr3-octreotate (A), DOTA0-Tyr3-octreotide (B), and DTPA0-octreotide (C), also known as DOTATATE, DOTATOC, and DTPA-OC or pentetreotide, respectively.
SSTR IMAGING
111In-Pentetreotide
Radiolabeled SSAs are used in localization, staging or restaging, and therapy selection; 111In-pentetreotide was the first scintigraphic agent to be approved for NETs and has been the most widely studied (4). Compared with the sensitivity of available morphologic imaging, the sensitivity of 111In-pentetreotide scintigraphy for gastroenteropancreatic and bronchopulmonary NETs and paragangliomas was well documented in the 1990s as being greater than 75% (11). At present, compared with CT or MRI, 111In-pentetreotide is considered suboptimal, with a sensitivity of less than 60% (12). However, with 111In-pentetreotide whole-body scintigraphy, the therapeutic strategy is still modified in up to 50% of cases (13).
68Ga-SSA PET
In the last 15 y, molecular imaging of NETs has been revolutionized by the introduction of 68Ga-SSAs for PET/CT (14). Numerous advantages, such as easy synthesis from a 68Ge/Ga generator, higher spatial resolution (∼4–5 mm), image quantification (SUV), favorable dosimetry, and the possibility of modifying clinical management in 36%–55% of cases, made 68Ga-SSA PET/CT the current technique of choice (15,16). [68Ga-DOTA0-Tyr3]octreotate was recently approved by the U.S. Food and Drug Administration, and [68Ga-DOTA0-Tyr3]octreotide is expected to be approved by the European Medicines Agency soon.
The overall sensitivity of 68Ga-SSA PET/CT for NETs is greater than 90%, whereas specificity ranges from 92%–98%—better than that for CT scanning and 111In-pentetreotide scintigraphy, particularly for small tumors at a nodal or bone level (12,16,17). Unlike 111In-pentetreotide scintigraphy, [68Ga-DOTA0-Tyr3]octreotate PET/CT has a consistent visual and semiquantitative image interpretation among experienced and inexperienced readers. However, its use in theranostics to recommend or exclude PRRT requires practice and training (18).
Receptor Quantification
The estimation of SSTR density is used to assess the viability of cold and radiolabeled SSA therapy as a prediction of the amount of (radio)pharmaceutical that will be concentrated at the tumor site and, hence, the possibility of a response (11). For 111In-pentetreotide, this estimate, expressed on the Krenning scale, is based on the relative uptake of the tumor compared with that of normal organs (liver or kidneys and spleen) on the planar image (11). The same concept can be applied to 68Ga-SSA PET/CT imaging (e.g., on the volumetric image). Furthermore, uptake can be objectively quantified as SUV, which strongly correlates (linearly under a threshold of 25) with the inhibitor constant on dynamic PET and, hence, SSTR levels (19–21). Although criteria have been validated for 111In-pentetreotide with the 4-point Krenning scale, there is no consensus on what should be considered sufficient uptake on 68Ga-SSA PET/CT. The findings of one study have suggested that tumor-to-spleen SUV ratio is superior to SUVmax in the early prediction of response (22).
PRRT
Early Results
Starting in the early 1990s, high doses of 111In-pentetreotide were administered to patients who had high uptake on diagnostic scans to achieve therapeutic results. Doses of up to 18.5 GBq/cycle and, cumulatively, 160 GBq were administered, resulting in partial response rates of up to 7.5%. In addition, improvement of symptoms was reported in up to 62% of cases, and toxicity rates were acceptable (23–25). With the introduction of the chelator DOTA, SSAs could be linked to 177Lu and 90Y, increasing the dose to the tumor and making 111In-pentereotide obsolete for therapeutic purposes. Here we provide an overview of the safety and efficacy of PRRT with β-emitters.
Safety
PRRT is generally very well tolerated. The full treatment is usually administered in 3 or 4 fractions at intervals of 6–12 wk, so as not to exceed single high doses to organs at risk. Acute toxicity, in the form of nausea (with or without vomiting), diarrhea, and abdominal pain, is mild and effectively treated with antiemetics and analgesics.
Because of transient bone marrow suppression, some subacute and usually self-limiting hematologic toxicity can be expected. In large trials, grade 3 or 4 hematologic toxicity has been reported in 3%–14% of the patients (26–28). Long-term myelotoxicity in the form of myelodysplastic syndrome or acute leukemia is a rare and severe adverse event associated with PRRT, occurring in 1%–2% of patients (29). Incidence rates are higher in patients who have been heavily pretreated with alkalizing chemotherapeutics, probably reflecting the myelotoxic properties of these agents (30,31).
Long-term or persistent renal toxicity is considered rare. SSAs are partially reabsorbed in the proximal tubule cells; counteracting this reabsorption with the coinfusion of positively charged amino acids during treatment results in a mean dose reduction in the kidneys of 40% (32). Severe renal toxicity has been reported in 0%–9% of patients; high incidences have been reported in some trials with 90Y because of its biologic and physical properties and treatment in an early era without amino acid renal protection (26,27). With renal protection being the standard of care in international protocols, some radiation nephropathy is still considered normal. In 208 patients, an average annual decrease in creatinine clearance of 3.4% ± 0.4% was observed after [177Lu-DOTA0-Tyr3]octreotate treatment (33).
Dosimetry has been proposed to optimize PRRT. Dose thresholds extrapolated from external-beam radiotherapy were initially proposed for the kidneys and bone marrow. The subsequent introduction of the “biologically effective dose” concept, at least for the kidneys, provided a better dose–effect correlation (34). However, although renal dosimetry is more reliable, bone marrow dosimetry is still in need of fine-tuning. Because threshold doses for renal toxicity are infrequently reached or are largely exceeded with standard 177Lu-based PRRT, and because long-term follow-up of large patient cohorts has indicated a very low risk of severe renal toxicity, routine dosimetry stratification of PRRT candidates is worth exploring in nonstandard treatments, such as retreatments (or salvage treatments) (26,35,36). Given that the bone marrow is the major organ at risk for toxicity after 177Lu-based PRRT, refined dosimetric methods, possibly based on microdosimetry, are warranted.
Efficacy
Objective response rates (complete response plus partial response) ranged from 4% to 45% in available phase 2 trials and might be limited in several trials (Table 3). However, analysis of survival data showed that survival in patients with a partial response might be similar to that in patients with stable disease after PRRT (36–39). With these findings in mind, for the evaluation of a response, one could consider disease control rates (complete response, partial response, and stable disease), which ranged from 62% to 95% in trials including only patients with progressive disease at baseline (38–42). Figure 2 shows the efficacy of PRRT in a patient with rectal NET with metastases to the liver.
Phase 2 Trials with Radiolabeled Somatostatin Analogs for Treatment of Advanced NETs
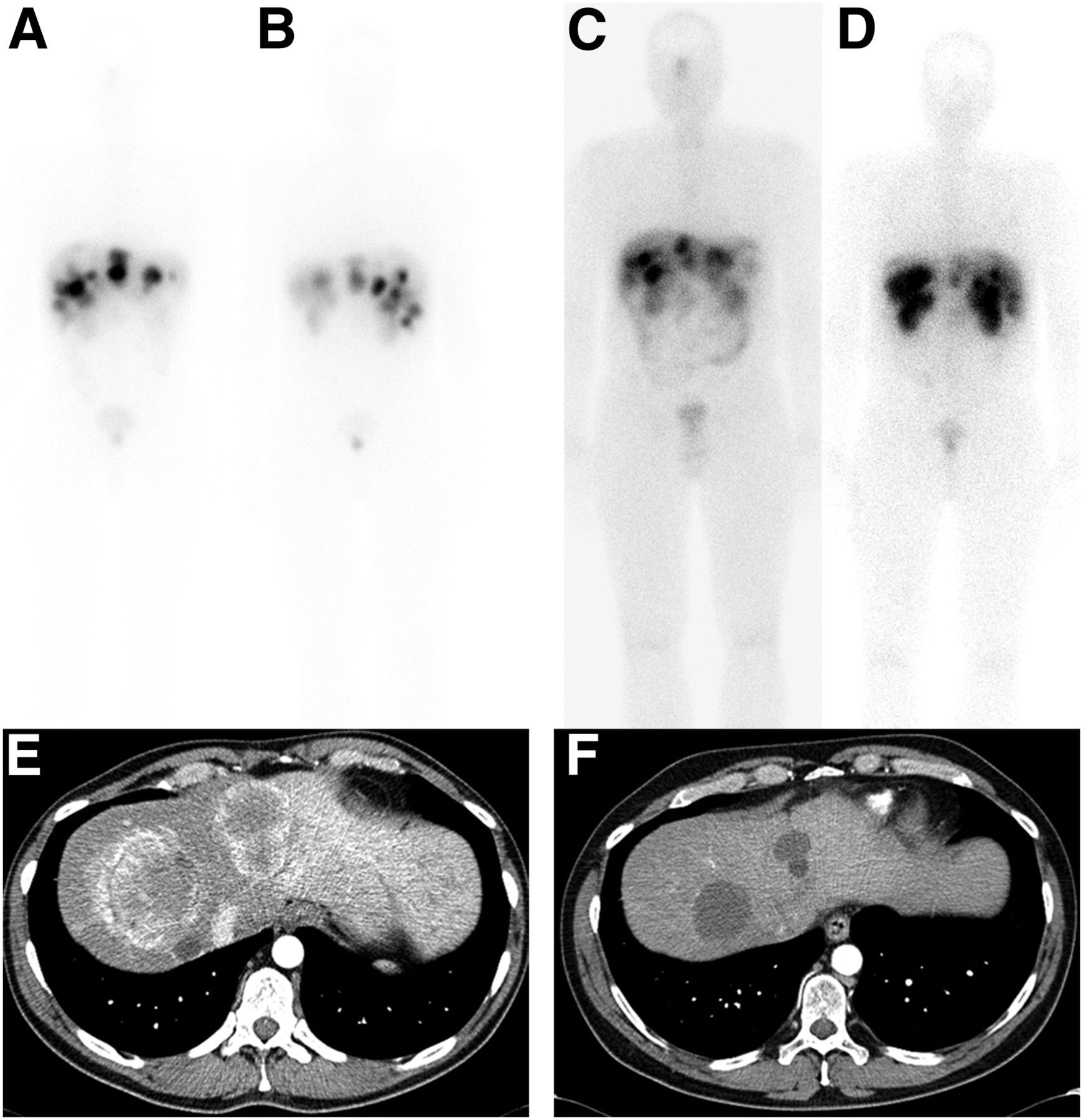
(A–D). Anterior (A and C) and posterior (B and D) planar whole-body scintigrams obtained 24 h after first (A and B) and fourth (C and D) treatments with [177Lu-DOTA0-Tyr3]octreotate in 43-y-old patient with grade 2 (Ki-67, 15%) rectal NET with metastases to liver. After treatment (C and D), physiologic uptake was more pronounced in pituitary gland, kidneys, spleen, and bowels. This decrease in tumor-to-organ ratio may indicate favorable outcome. (E and F) Contrast-enhanced CT of abdomen before (E) and 2 mo after (F) treatment. In addition to decrease in size after treatment, pretherapeutic arterial enhancement was lost and lesions became hypodense, indicating therapeutic efficacy.
Irrespective of radiographic outcome, PRRT can improve patients’ quality of life. The secretion of bioactive hormones by NETs can result in severe symptoms and life-threatening crises. Small intestinal NETs are mainly associated with the carcinoid syndrome, which includes flushing, diarrhea, bronchospasm, tachycardia, and anxiety. PRRT has been shown to improve patients’ quality of life and performance and to decrease a range of symptoms, such as fatigue, nausea, pain, dyspnea, insomnia, and diarrhea (43). In patients with functional pancreatic NETs, PRRT proved very successful in achieving durable control of severe hypoglycemia in insulinomas (44).
In January 2017, numerous phase 2 trials and case series were validated with the publication of the interim analysis of the Neuroendocrine Tumor Therapy (NETTER-1) trial (45). This phase 3 trial included randomization between treatment with [177Lu-DOTA0-Tyr3]octreotate (4 × 7.4 GBq) and treatment with high-dose, long-acting, repeatable octreotide in 229 patients with advanced midgut NETs and disease progression after first-line SSA therapy. The 3 most important findings were that for the PRRT arm, the median progression-free survival was not reached (vs. 8.4 mo for the control arm), the hazard ratio for disease progression or death was 0.21, and the objective tumor response was 18% (vs. 3% for the control arm).
Unlabeled SSAs are the first line of treatment in advanced NETs because of their highly favorable toxicity profile (46). However, after failure of this treatment, therapeutic options are limited. Previous randomized trials demonstrated the efficacy of everolimus and sunitinib (Table 4) and led to the implementation of these targeted drugs. With the publication of the NETTER-1 trial, PRRT has been added to the standard of care. Further randomized trials are needed to compare the efficacy and the toxicity profiles of PRRT and targeted therapies to clarify the best sequencing of the treatment algorithm.
Randomized Controlled Trials for Treatment of Advanced NETs (64)
FUTURE DEVELOPMENTS
Advances in SSTR-2 targeting were obtained with the SSTR antagonist [177Lu-DOTA]JR11. In vitro and in vivo animal studies demonstrated significant increases in (membrane-bound) tumor uptake, tumor radiation dose, and durable double-strand DNA breaks with the SSTR antagonist [177Lu-DOTA]JR11 compared with the SSTR agonist [177Lu-DOTA0-Tyr3]octreotate (47). In 4 patients, [177Lu-DOTA]JR11 resulted in increased residence times, tumor uptake and, hence, tumor dose compared with [177Lu-DOTA0-Tyr3]octreotate (48). Twelve months after treatment, 2 patients showed a partial response, 1 showed stable disease, and 1 showed progressive disease, all without long-term renal or hematologic toxicity.
Studies have been performed with α-emitting [213Bi-DOTA0-Tyr3]octreotide. Theoretically, the high-energy particles can increase double-strand DNA breaks, and the limited tissue range (2 cell diameters) can decrease collateral damage (Table 1). In 7 patients with β-emitting PRRT–refractory NETs, 13.3–20.8 GBq of [213Bi-DOTA0-Tyr3]octreotide was administered in 2–5 dose-escalating cycles (49). The patients had predominantly progressive liver disease, and treatment was administered intraarterially. Treatment was effective in all patients; at the time of analysis, the response in the liver had been maintained for 12–34 mo. Subacute toxicity was limited, but 1 (chemotherapy-naive) patient developed myelodysplastic syndrome 24 mo after treatment. In addition, the γ-emitting capacities of 213Bi decay were used for posttherapeutic scintigraphy.
As changes in disease management are often based on morphologic and molecular imaging, the development of a new PET tracer—[64Cu-DOTA0-Tyr3]octreotate—may further enhance therapeutic decision making. Compared with 68Ga-SSA PET tracers, this tracer has a longer half-life and lower positron decay energy, theoretically leading to a favorable tumor-to-background ratio and better detection of small lesions (50). In a direct comparison, the patient-based sensitivities were equal, but [64Cu-DOTA0-Tyr3]octreotate had a higher lesion detection rate and was superior at identifying affected organs (51).
On a biochemical level, adding the combination of the DNA methyltransferase inhibitor 5-aza-2′-deoxycytidine and the histone deacetylase inhibitor valproic acid may be beneficial. A study of human pancreatic NET cell lines showed epidrug-induced upregulation of SSTR-2 with increased uptake of radiolabeled octreotide, which may be useful in patients with low levels of SSTR-2 expression (52).
CONCLUSION
From the first in vivo SSTR scintigraphy with 123I-Tyr3-octreotide in 1987 to the first phase 3 trial with [177Lu-DOTA0-Tyr3]octreotate, 3 decades of development have inseparably linked SSTR-targeting theranostic agents to NETs. PRRT is on the verge of becoming the standard of care for patients with well-differentiated inoperable or metastatic NETs and disease progression after first-line SSA therapy. Several preclinical and clinical developments, such as the use of SSA antagonists and α-emitting radionuclides, stand to enhance the diagnostic and therapeutic properties of SSTR-targeting theranostic agents and can enter phase 1 or 2 trials. At this time, there is a need for further randomized trials to identify the optimal, multidisciplinary sequencing of long-lasting treatments for these patients.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
Acknowledgments
We thank Wouter A.P. Breeman, radiochemist at Erasmus University Medical Center, for kindly supplying the structural formulae (Fig. 1).
Footnotes
↵† Deceased.
- © 2017 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication January 30, 2017.
- Accepted for publication April 11, 2017.





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- 18F-Labeled Somatostatin Analogs as PET Tracers for the Somatostatin Receptor: Ready for Clinical Use
- 18F-Labeled Somatostatin Analogs as PET Tracers for the Somatostatin Receptor: Ready for Clinical Use
- Peptide Receptor Radionuclide Therapy in Grade 3 Neuroendocrine Neoplasms: Safety and Survival Analysis in 69 Patients
- Theranostic Concepts: More Than Just a Fashion Trend--Introduction and Overview